
Abstract
Autistic individuals without intellectual disabilities show high rates of suicidal thoughts and behaviours (STBs); however, the processes underlying this vulnerability remain still unclear and understudied. This study examined STBs within a multidimensional framework integrating intrapersonal, interpersonal, and environmental factors. Eighty-four autistic adolescents and young adults (aged 12–32 years) were included. Overall, 36.9% of participants reported suicidal ideation, 27.4% reported self-harm, and 42.9% endorsed at least one indicator of STBs. Regression analyses reported that peer victimisation was associated with both suicidal ideation and self-harm, while self-harm also showed a specific association with cognitive emotion regulation strategy. Two canonical correlation analyses were performed, including maladaptive and adaptive cognitive emotion regulation strategies. A positive canonical correlation emerged between maladaptive strategies and the STBs domain, whereas a negative canonical correlation was observed between adaptive strategies and the same outcome. Finally, as a sensitivity analysis, a moderation model examined whether perceived stress reactivity influenced the association between emotion regulation and self-harm, showing that this association varied as a function of stress reactivity. Overall, these findings indicate that STBs in autism reflect a dynamic psychopathological process involving interpersonal, intrapersonal, and stress-related domains, with important implications for clinical assessment and the development of targeted prevention strategies.
Lay abstract
Autistic adolescents and young adults without intellectual disability are at increased risk of suicidal thoughts and self-harm behaviours, but the factors linked to this risk are still not fully understood. This study examined whether peer victimisation, cognitive emotion regulation, and individual stress reactivity were associated with suicidal thoughts and self-harm in 84 autistic people aged 12 to 32 years. Peer victimisation was related to both suicidal thoughts and self-harm behaviours, suggesting that negative experiences with peers may be an important vulnerability factor. Self-harm also showed a more specific association with emotion regulation. In particular, blaming others was negatively associated with self-harm, especially among participants who reported higher stress reactivity. This suggests that, in some contexts, attributing distress to external causes may have a self-protective function rather than being simply maladaptive. Overall, these findings suggest that suicidal thoughts and self-harm behaviours in autistic people may arise from a combination of social adversity, emotion regulation, and stress-related processes. Clinical assessment and prevention should therefore consider peer victimisation and stress reactivity, as well as the specific function of different emotion regulation strategies.
Keywords
Introduction
Autism spectrum disorder (ASD) is a lifelong neurodevelopmental condition characterised by persistent difficulties in social communication and restricted and repetitive patterns of behaviour (Lord et al., 2018). Beyond these core features, autistic individuals frequently report heightened intrapersonal vulnerability, including marked difficulties in emotion regulation and elevated perceived stress reactivity (Cai et al., 2018; Ilen, Feller, & Schneider, 2024). Moreover, they are also disproportionately exposed to adverse interpersonal experiences, such as peer victimisation and social exclusion (Kasari & Sterling, 2013; Sreckovic et al., 2014). These well-documented vulnerabilities are particularly relevant when considering the elevated prevalence of suicidal distress observed in autistic individuals (Blanchard et al., 2021; Hedley & Uljarević, 2018; Richa et al., 2014).
To date, suicidality represents a major public health concern and is commonly conceptualised within the suicidal thoughts and behaviours (STBs) framework, which captures a continuum of suicide-related vulnerability encompassing suicidal ideation and self-harming behaviours (with or without explicit suicidal intent) that fluctuate over time in expression and severity (Brown et al., 2024; Thompson et al., 2020). This clinical framework is consistent with contemporary ideation-to-action theories of suicide, particularly the Three-Step Theory (3ST; Klonsky & May, 2015), which conceptualises suicidal ideation as arising primarily from psychological pain and hopelessness. The later transition to suicidal behaviours is determined by dispositional (i.e. genetic), acquired (i.e. habituation to experiences associated with pain) and practical factors (access to lethal means) (Klonsky & May, 2015). Therefore, within this model, suicidal ideation and behaviours represent distinct but interrelated stages of the same vulnerability process.
In this context, self-harm behaviours have direct consequences for both the individual’s internal state and the surrounding social environment (Moseley et al., 2020). At the interpersonal level, they may serve to influence or interrupt others’ behaviours, or communicate distress when verbal communication is experienced as difficult or insufficient (Moseley et al., 2020). In contrast, intrapersonal functions relate to the regulation of overwhelming emotional or cognitive experiences, including relief from tension, numbness or self-directed negative affect, or the search for sensory stimuli that restore a sense of control (Moseley et al., 2020). Importantly, individuals may engage in self-harm for different reasons depending on the context; moreover, this behaviour may often co-occur with other maladaptive strategies and behaviours (i.e. rumination, self-blame, helplessness, substance use, and eating disorder; Buckholdt et al., 2015; Hooley & Franklin, 2018; Mikolajczak et al., 2009; Nock, 2009).
Converging evidence indicates that autistic individuals are at substantially increased risk for STBs compared with the general population. Meta-analytic data from ASD populations show pooled lifetime prevalence estimates of 37.2% for suicidal ideation and 15.3% for suicide attempts (Huntjens et al., 2024). By contrast, cross-national estimates in the general population indicate lower lifetime prevalences, with suicidal ideation reported at 9.08% and suicide attempts at 2.88% (Castillejos et al., 2021).
Given the increase in the measured prevalence of autism over recent decades (Zeidan et al., 2022), these findings underscore the urgency of identifying the mechanisms underlying this heightened suicidal vulnerability. In this regard, the close link between suicidal thoughts and self-harm behaviours (with or without suicidal intention) observed in the general population is particularly relevant since autistic individuals consistently report higher rates of both STBs, suggesting that similar mechanisms may be involved in their onset. At the same time, the literature on STBs in autistic individuals has expanded substantially in recent years across both youth and adult populations (Mournet et al., 2023; O’halloran et al., 2022). Earlier work, however, often focused on forms of self-injurious behaviour commonly observed in autistic individuals with co-occurring intellectual disability, such as head banging or biting, which were generally conceptualised within the framework of repetitive and stereotyped behaviours rather than within the functional framework typically used to understand self-harm in the general population (Matson & LoVullo, 2008; Mayes et al., 2013; Minshawi et al., 2014).
Only in recent years has attention shifted to autistic individuals without intellectual disabilities, who appear to be at higher risk for STBs than autistic individuals with intellectual disabilities, according to converging clinical and epidemiological evidence (Richa et al., 2014). Emerging findings indicate that, although the overall presentation of STBs in autistic individuals may appear broadly similar to that observed in non-autistic populations, there are important differences in the underlying factors and motivations (Moseley et al., 2020). Specifically, STBs in autistic individuals are closely associated with loneliness, hopelessness, feelings of worthlessness, and a sense of entrapment, which participants consistently describe as emerging in contexts of stigma, social exclusion, victimisation, and limited access to adequate support (Moseley et al., 2025). In this line, Chikaura et al. (2026) also indicate that, even when accounting for trauma exposure and demographic factors, a diagnosis of autism remains an independent predictor of self-harm, suicide plans and attempts, and clinically significant psychological distress. However, despite growing interest in this area, the literature examining the specific mechanisms and subjective motivations underlying STBs in autistic individuals without intellectual disability remains relatively limited.
Although emotional dysregulation is widely recognised as a key risk factor, the specific contribution of cognitive emotion regulation strategies remains unexplored in ASD in association with STBs. In this sense, cognitive emotion regulation strategies can contribute to the interpretation and processing of emotionally salient experiences over time, potentially influencing the persistence of distress and its association with both suicidal ideation and self-harm (with or without explicit suicidal intent) (Sabzehparvar & Amiri, 2025). At the same time, stress reactivity and peer victimisation, both highly prevalent in autistic individuals and strongly linked to emotional distress (Ilen, Delavari, et al., 2024; Storch et al., 2012), may further exacerbate this vulnerability. The simultaneous study of these dimensions offers a multidimensional perspective that integrates intrapersonal, interpersonal, and environmental factors.
Therefore, this study aims to clarify how these factors are involved in the definition and development of STBs in autistic individuals without intellectual disability. Our hypothesis is that maladaptive cognitive emotion regulation strategies will be associated with higher levels of STBs, while adaptive strategies will show a protective pattern. Greater stress reactivity and greater peer victimisation are expected to be related to increased severity of suicidal ideation and self-harming behaviours (with or without explicit suicidal intent). Finally, we hypothesise that the combined influence of these factors will reflect a multidimensional vulnerability.
Method
Participants
A first power analysis based on a correlational design was conducted using G*Power 3.1 software. Previous research has reported medium-to-large associations between cognitive emotion regulation strategies and STBs (Abdollahpour Ranjbar et al., 2024; Horwitz et al., 2011; Manesh & Kulemarzi, 2024; Mikolajczak et al., 2009). Considering this evidence and aiming for a conservative yet realistic estimate, we adopted an expected effect size of r = .40, reflecting a medium-to-large effect. Given the exploratory nature of the study, a two-tailed model was used to account for potential bidirectional effects. Using a probability level of α = .05 and statistical power of 1 – β = .80, the analysis indicated that 44 participants were required to achieve satisfactory power.
Then, another single power analysis was performed for both regression models predicting self-harming behaviours (with or without explicit suicidal intent) and suicidal ideation. As previously described for the other power analysis, studies have reported medium-to-large associations between cognitive emotion regulation strategies across various clinical and non-clinical populations (Abdollahpour Ranjbar et al., 2024; Horwitz et al., 2011; Manesh & Kulemarzi, 2024; Mikolajczak et al., 2009). Therefore, in accordance with Cohen’s guidelines (Cohen, 2013), a medium effect size of f2 = 0.15 was used.
Given that two primary regression models were tested, and to appropriately control the family-wise error rate, the significance threshold (α = .05) was adjusted using the Bonferroni correction, as recommended in methodological literature on multiple comparisons in power and sample size estimation (Vickerstaff et al., 2019). Accordingly, with an adjusted significance level of α = .025, a power (1 – β) = .80, and nine predictors, the estimated minimum sample size required to achieve adequate power in a two-tailed model was 67 participants.
A total of 113 participants initially consented to take part in the study between October 2020 and March 2025. Following the application of the exclusion criteria and the removal of cases with missing data, the final sample comprised 84 participants with a clinical diagnosis of ASD. This sample partially overlaps with previous studies (Ilen, Delavari, et al., 2024; Ilen, Feller, & Schneider, 2024). The target age range (10–35 years) was selected to encompass adolescence and young adulthood, a developmental period particularly relevant for the emergence of STBs (Goldston et al., 2016; Lewinsohn et al., 2001; Nock et al., 2013).
Autistic individuals were recruited via specialised clinics located in Switzerland and various regions of France, with additional recruitment through professional networks and family associations operating across France and Switzerland. Eligibility criteria required participants to have sufficient verbal abilities and a formal ASD diagnosis. Sufficient verbal abilities were defined functionally as the ability to understand study instructions, engage in the required interactions, and complete the assessment procedures, as evaluated clinically by the specialist in charge of the assessment. Descriptive statistics are reported in Table 1.
Sociodemographic and Clinical Variables.
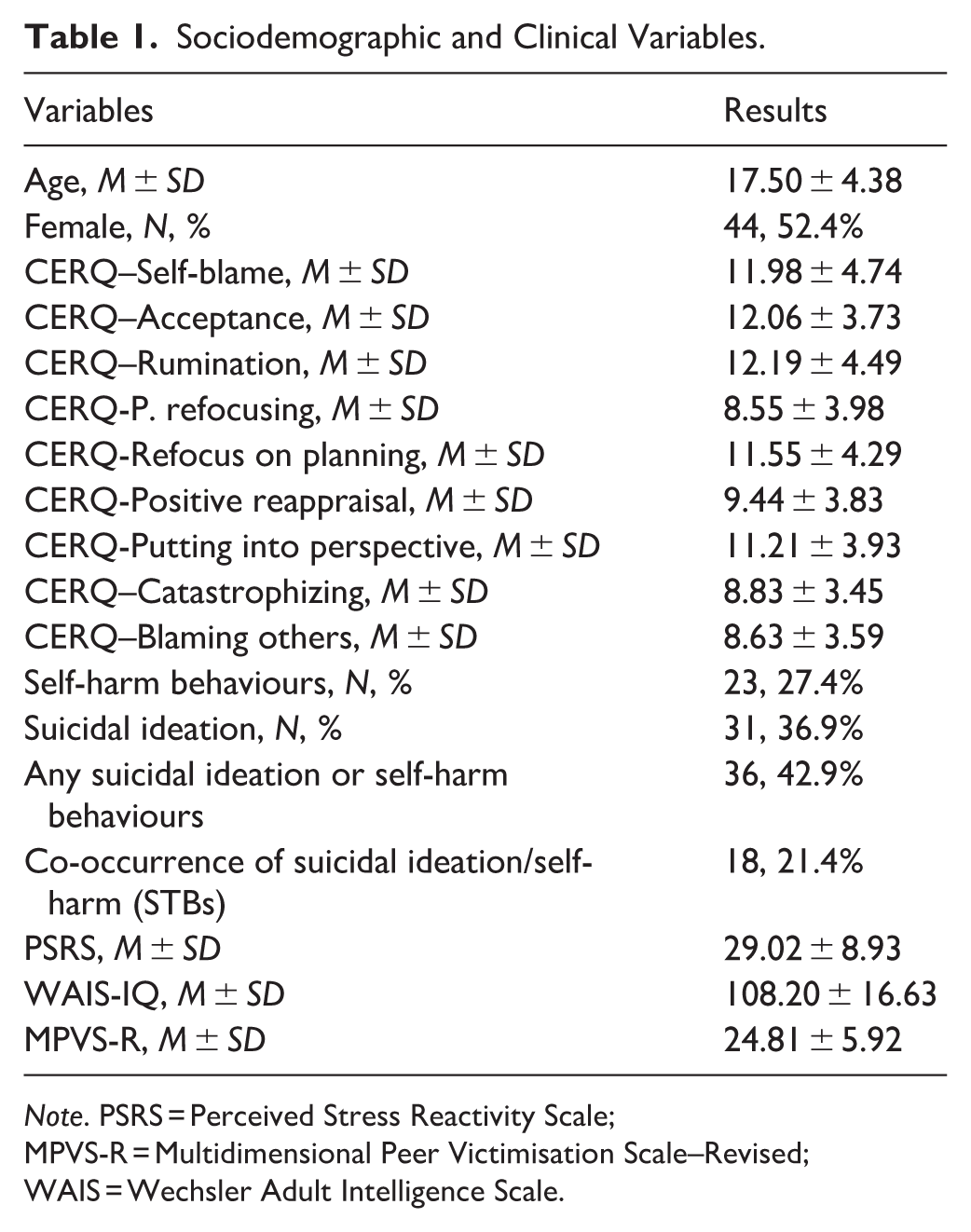
Note. PSRS = Perceived Stress Reactivity Scale; MPVS-R = Multidimensional Peer Victimisation Scale–Revised; WAIS = Wechsler Adult Intelligence Scale.
Participation in the study was voluntary, and all participants received compensation in the form of a voucher (i.e. Amazon and FNAC) with a commercial value of 100 euros. The study was approved by the Cantonal Research Ethics Committee of Geneva (CCER) (2018-01117).
Community Involvement Statement
Community members were not formally involved in the development of the research question, study design, selection of measures, data analysis, interpretation of findings, or dissemination planning. Recruitment was facilitated in part through professional networks and family associations; however, these organisations did not contribute to the design, conduct, analysis, interpretation, or reporting of the study.
Questionnaires
All measures included in this study were administered in French.
According to previous research (Dhossche et al., 2002; Herba et al., 2008; Kim et al., 2005), suicidal ideation and self-harm behaviours (with or without explicit suicidal intent) were assessed using two items from the Achenbach System of Empirically Based Assessment (ASEBA) questionnaires: the Youth Self-Report (Achenbach, 1991) for participants aged 11–18 years, and the Adult Self-Report (ASR; Achenbach & Rescorla, 2003) for participants aged 18–59 years. Specifically, Item 18 (“I deliberately try to hurt or kill myself”; self-harm behaviours with or without explicit suicidal intent) and Item 91 (“I think about killing myself”; suicidal ideation) were used. Each item was rated on a 3-point scale (0 = not true, 1 = partly or sometimes true, 2 = very true or often true). For each participant, endorsement was defined as a score of 1 or higher.
Cognitive emotion regulation strategies were measured using the French adaptation (d’Acremont & Van der Linden, 2007) of the Cognitive Emotion Regulation Questionnaire (CERQ; Garnefski & Kraaij, 2007). This self-report instrument evaluates how individuals manage their emotions following negative or stressful experiences. It comprises 36 items rated on a 5-point Likert-type scale (from 1 = almost never to 5 = almost always), covering a range of adaptive and maladaptive cognitive strategies. The adaptive dimension encompasses acceptance, positive refocusing, refocus on planning, positive reappraisal, and putting into perspective, while the maladaptive dimension includes self-blame, rumination, catastrophizing, and blaming others. Reported internal consistency in the original validation ranged from α = .68 to .83 (Garnefski & Kraaij, 2007), and from α = .62 to .82 in the French version (d’Acremont & Van der Linden, 2007). For this study, Cronbach’s alpha ranged between .69 and .88 with a total score of .85.
Stress reactivity was assessed using the Perceived Stress Reactivity Scale (PSRS; Schlotz et al., 2011), a 23-item self-report questionnaire evaluating perceived responses to everyday stress. Items are rated on a 3-point Likert-type scale, with higher scores indicating greater stress reactivity. The PSRS shows good test–retest reliability and validity (Schlotz et al., 2011), and for the current sample, a Cronbach’s alpha of .90 was observed for the total score.
Peer victimisation was measured using the French version of the Multidimensional Peer Victimisation Scale–Revised (MPVS-R; Bates et al., 2015). The MPVS-R consists of 20 items assessing five dimensions of peer victimisation: physical victimisation, verbal victimisation, social manipulation, attacks on property, and electronic victimisation. Participants indicated how often they had experienced each form of victimisation during the past year on a 3-point Likert-type scale (1 = Never, 2 = Once, 3 = More than once). For this study, a total score was computed to provide an overall index of peer victimisation, with higher scores indicating more-frequent experiences of victimisation. The internal consistency for the total score in the current sample was α = .86.
Statistical Analysis
All statistical analyses were performed using SPSS 30.0.0. Data distribution was first examined to verify normality, following the recommendations of Kim (2013). Subsequently, Spearman’s exploratory correlation analyses were carried out between all CERQ subscales, stress reactivity, peer victimisation, suicidal ideation and self-harm behaviours (with or without explicit suicidal intent). To further examine the unique contribution of emotion regulation strategies to these outcomes (i.e. suicidal ideation and self-harm behaviours), two separate multiple regression analyses were performed, including only the CERQ subscales that showed significant values at previous bivariate analyses.
Two separate canonical correlation analyses (CCAs) were conducted as exploratory multivariate analysis to examine associations between maladaptive and adaptive emotion regulation strategies and the STBs dimension. CCA is a multivariate statistical technique designed to assess the relationship between two sets of variables by identifying pairs of linear combinations that maximise their shared variance (Loureiro et al., 2025). This approach is particularly valuable in psychological research for uncovering complex, multidimensional relationships between cognitive-emotional processes and behavioural outcomes (Loureiro et al., 2025). In this study, although the “blaming others” subscale is conventionally classified as a maladaptive strategy, it showed an opposite pattern of association with suicidal thoughts and self-harm behaviours (with or without explicit suicidal intent) both at the bivariate and multivariate levels. For this reason, and to maintain internal coherence within the canonical functions, blaming others was included in the adaptive variable set.
Finally, as a supplementary analysis, a moderation model was tested to examine whether stress reactivity influenced the relationship between the CERQ blaming others subscale and self-harm. This analysis was conducted to explore the possibility that attributing blame to others, typically considered a maladaptive coping strategy, might play a different role under conditions of high emotional reactivity. Moderation analysis was performed using the Model 1 of the macro-PROCESS v.5 with a 5,000 bootstrap.
Results
Descriptive statistics for sociodemographic and clinical variables are reported in Table 1 and in Supplementary Table 2. Moreover, as reported in Table 2, self-harm with or without explicit suicidal intent were positively correlated with suicidal ideation (r = .59, p < .001), self-blame (r = .34, p < .001), peer victimisation (r = .26, p < .05), and stress reactivity (r = .45, p < .001). Conversely, a negative correlation also emerged with positive refocusing (r = –.36, p < .001) and other-blame (r = –.24, p < .05).
Spearman Correlations Among Study Variables.
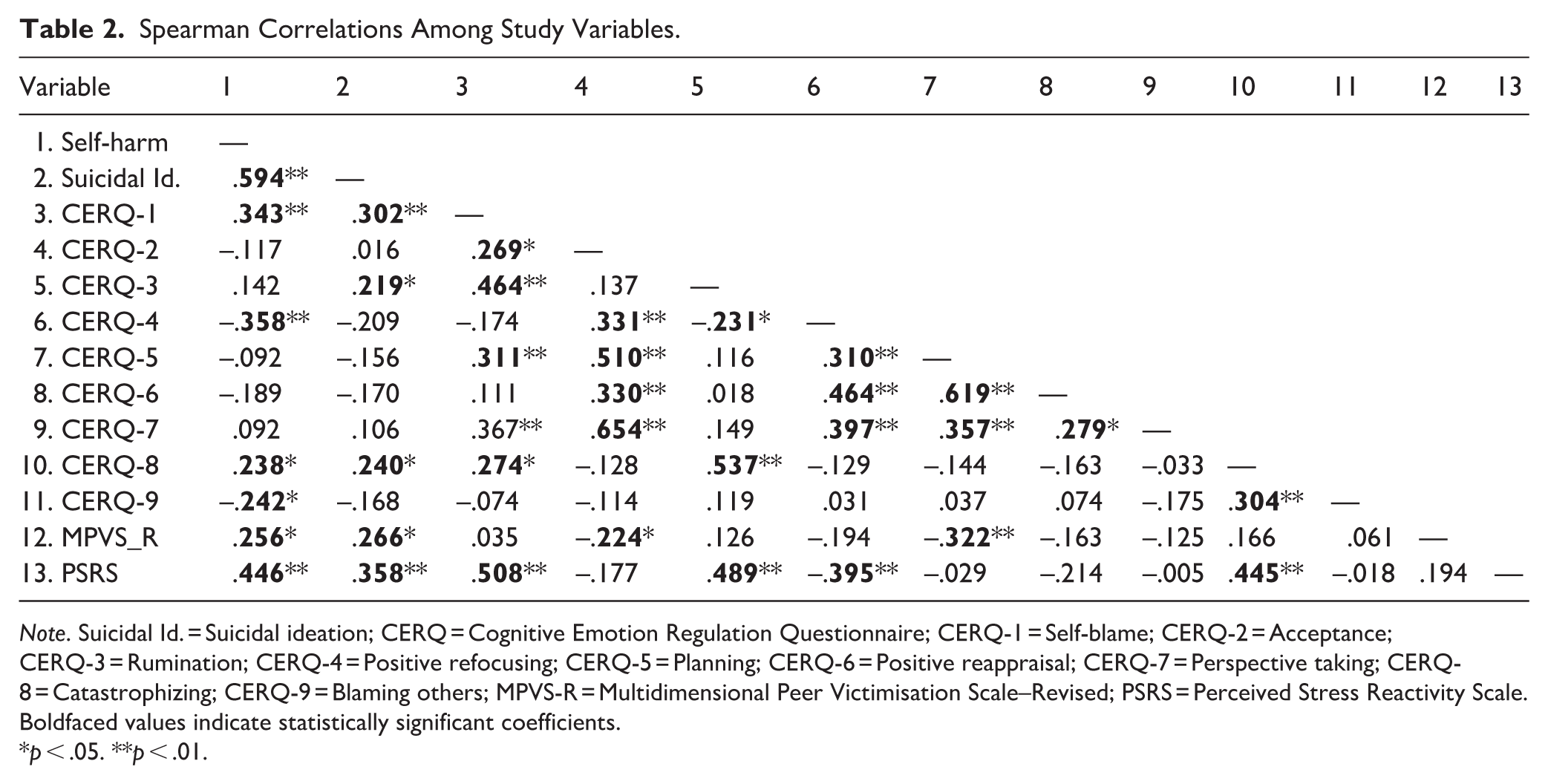
Note. Suicidal Id. = Suicidal ideation; CERQ = Cognitive Emotion Regulation Questionnaire; CERQ-1 = Self-blame; CERQ-2 = Acceptance; CERQ-3 = Rumination; CERQ-4 = Positive refocusing; CERQ-5 = Planning; CERQ-6 = Positive reappraisal; CERQ-7 = Perspective taking; CERQ-8 = Catastrophizing; CERQ-9 = Blaming others; MPVS-R = Multidimensional Peer Victimisation Scale–Revised; PSRS = Perceived Stress Reactivity Scale.
Boldfaced values indicate statistically significant coefficients.
p < .05. **p < .01.
Similarly, self-harming behaviours were also positively correlated with self-blame (r = .30, p < .001), rumination (r = .22, p < .05), catastrophizing (r = .24, p < .05), peer victimisation (r = .27, p < .05), and stress reactivity (r = .36, p < .001) but not with positive refocusing or other-blame, as in case of suicidal ideation, suggesting a slightly different pattern of cognitive, and emotional correlates.
Linear Regressions
At the multivariate level, two separate multiple linear regressions were conducted to examine the contribution of emotion regulation strategies to self-harm behaviours (with or without explicit suicidal intent) and suicidal ideation, respectively, controlling for age, gender, IQ, stress reactivity, and peer victimisation.
The model examining self-harm behaviours (with or without explicit suicidal intent) was significant, F(9, 74) = 6.32, p < .001, explaining 43% of the variance. As shown in Table 3, higher age (β = .26, p = .014, lower level confidence interval [LLCI] = .009, upper level confidence interval [ULCI] = .075) and more severe peer victimisation (β = .30, p = .003, LLCI = .013, ULCI = .058) were associated with higher self-harm behaviours. Among the CERQ subscales, blaming others was negatively associated with self-harm behaviours (β = –.21, p = .035, LLCI = –.315, ULCI = –.012), suggesting that individuals who tend to attribute blame externally reported lower self-harm behaviours. Moreover, suicidal ideation model was also significant, F(8, 75) = 3.68, p = .001, accounting for 28% of the variance. As reported in Table 4, only peer victimisation was positively and significantly associated with suicidal ideation (β = .24, p = .028, LLCI = .003, ULCI = .050).
Multiple Regression Model Predicting Self-Harm Behaviours With or Without Explicit Suicidal Intent.
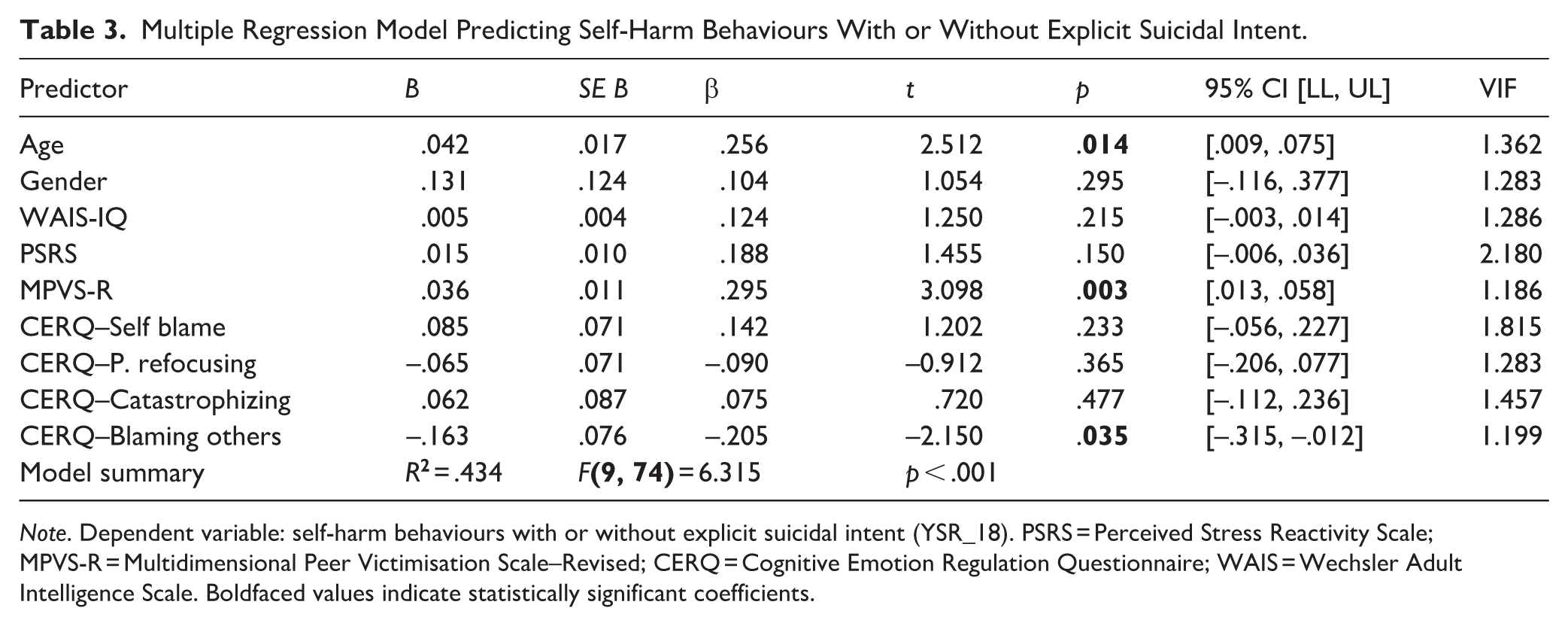
Note. Dependent variable: self-harm behaviours with or without explicit suicidal intent (YSR_18). PSRS = Perceived Stress Reactivity Scale; MPVS-R = Multidimensional Peer Victimisation Scale–Revised; CERQ = Cognitive Emotion Regulation Questionnaire; WAIS = Wechsler Adult Intelligence Scale. Boldfaced values indicate statistically significant coefficients.
Multiple Regression Predicting Suicidal Ideation.
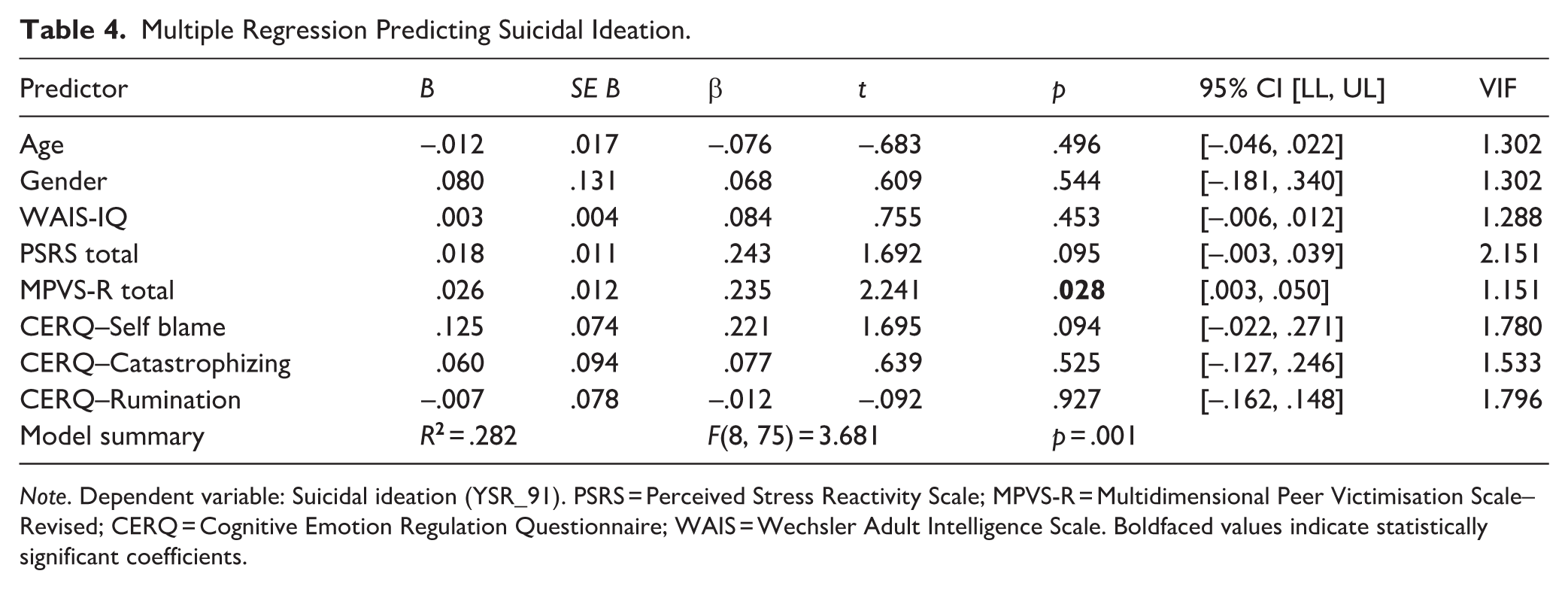
Note. Dependent variable: Suicidal ideation (YSR_91). PSRS = Perceived Stress Reactivity Scale; MPVS-R = Multidimensional Peer Victimisation Scale–Revised; CERQ = Cognitive Emotion Regulation Questionnaire; WAIS = Wechsler Adult Intelligence Scale. Boldfaced values indicate statistically significant coefficients.
Canonical Correlational Analysis
Then, an exploratory CCA was conducted to examine the multivariate association between maladaptive emotion regulation strategies and the STBs dimension (Figure 1). The analysis yielded one significant canonical function, with a canonical correlation of r = .493, Wilks’ Λ = .736, F(6, 158) = 4.36, p < .001. The second function was nonsignificant and was therefore not interpreted. Within the maladaptive emotion regulation set, the first canonical function showed the strongest structure coefficient for self-blame (–.935), followed by catastrophizing (–.516) and rumination (–.442). The cross-loadings reflected the same pattern, with self-blame (–.461), catastrophizing (–.254), and rumination (–.218) each showing meaningful associations with the canonical function.
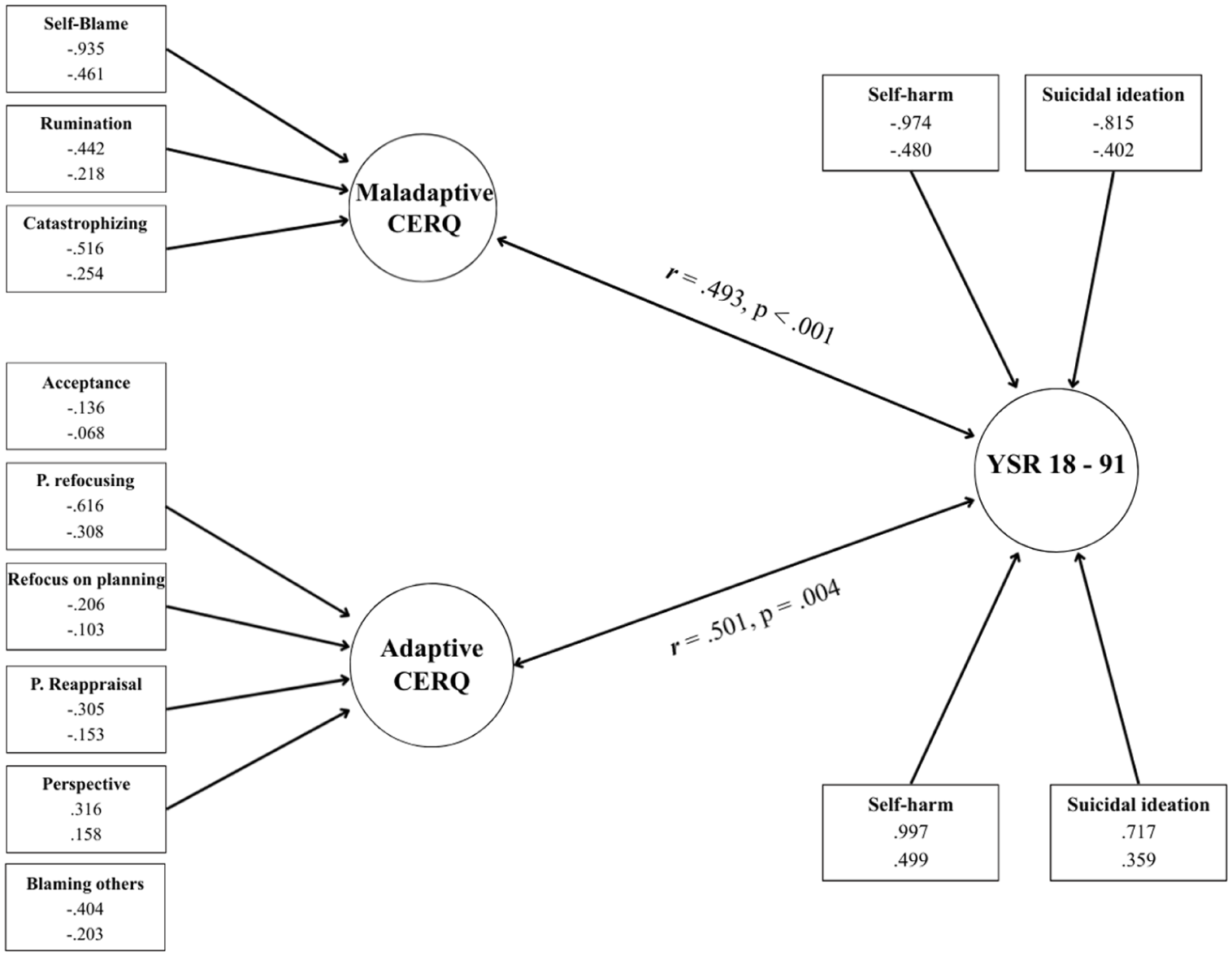
Canonical correlational analysis on adaptive and maladaptive CERQ subscales on STBs dimension.
On the other side, the canonical function representing self-harm behaviours (with or without explicit suicidal intent) and suicidal ideation also demonstrated substantial and coherent contributions from both indicators. Self-harm had the strongest loading (–.974), followed by suicidal ideation (–.815), indicating that both variables aligned closely with the extracted STBs dimension. Cross-loadings confirmed this pattern (–.480, and –.402, respectively), suggesting a strong degree of shared variance between the maladaptive emotion regulation function and the behavioural outcomes.
Consistent with these loading patterns, the canonical function accounted for a notable proportion of variance within both variable sets. For the maladaptive set, the variance extracted was .445, indicating that 44.5% of the variance among self-blame, rumination, and catastrophizing was captured by the canonical function. The redundancy index showed that the STBs dimension shared 10.8% of the variance with the maladaptive strategies. On the other hand, for the STBs set, the variance extracted was .807, meaning that 80.7% of the variance in suicidal ideation and self-harm behaviours was captured by the canonical function. The redundancy value indicated that 19.6% of the STBs variance was shared with the maladaptive emotion regulation function.
A second CCA was conducted to examine the multivariate association between adaptive emotion regulation strategies and the STBs dimension (Figure 1). This analysis also yielded one significant canonical function, with a canonical correlation of r = .501, Wilks’ Λ = .694, F(12, 152) = 2.54, p = .004. The second function was not significant and was therefore not interpreted.
Within the adaptive emotion regulation set, the first canonical function showed the strongest structure coefficients for positive refocusing (–.616) and blaming others (–.404), followed by smaller contributions from putting into perspective (.316), positive reappraisal (–.305) and planning (–.206). Acceptance showed only a minimal loading (–.136). The cross-loadings displayed the same configuration, with positive refocusing (–.308), other-blame (–.203), putting into perspective (.158), and positive reappraisal (–.153) presenting the most meaningful associations with the canonical function, whereas acceptance (–.068) and planning (–.103) showed smaller contributions. Overall, the adaptive canonical function was primarily defined by positive refocusing and other blame, with additional but more modest contributions from perspective taking, positive reappraisal and planning.
On the other side, the canonical function demonstrated strong and coherent contributions from both indicators of the STBs dimension. Self-harm showed an extremely high loading (.997), with suicidal ideation also displaying a substantial loading (.717). Cross-loadings confirmed these associations (.499 and, .359), indicating a robust degree of shared variance between the adaptive emotion regulation function and the STBs.
Consistent with these loading patterns, the canonical function accounted for a more modest proportion of variance within the adaptive strategy set. The variance extracted for this set was .133, indicating that 13.3% of the variance among acceptance, positive refocusing, planning, putting into perspective, and other blame was captured by the canonical function. The redundancy index showed that the behavioural function explained 3.3% of the variance in the adaptive strategies. This lower proportion of variance may reflect the opposite direction of the relationship between putting into perspective and the STBs dimension.
Conversely, for the STBs set, the variance extracted was .754, meaning that 75.4% of the variance in suicidal ideation and self-harming behaviours was accounted for by the adaptive canonical function. The redundancy value indicated that 18.9% of the STBs variance was shared with the adaptive emotion regulation function.
Supplementary Moderation Model
Finally, a supplementary moderation analysis was conducted to further clarify the nature of the association between blaming others and self-harm (with or without explicit suicidal intent) by examining whether this relationship varied as a function of stress reactivity (Supplementary Table 1). The full model was significant, R .670, R2 = .449, F(7, 76) = 8.854, p < .001, and the interaction between blaming others and stress reactivity emerged as a significant predictor of self-harm behaviours (B = -.015, SE = .007, t = –2.227, p = .029). The inclusion of the interaction term accounted for a significant increase in explained variance, ΔR2 = .036, F(1, 76) = 4.958, p = .029.
To probe the nature of this interaction, conditional effects were examined at low (–1SD), mean, and high (+1SD) levels of stress reactivity. At low levels of stress reactivity, blaming others was not significantly associated with self-harm (B = –.042, SE = .087, t = –.475, p = .636). At average levels of stress reactivity, the association was significant (B = –.174, SE = .068, t = –2.560, p = .012). The effect became stronger at high levels of stress reactivity (B = –.321, SE = .098, t = –3.284, p = .002), indicating that higher stress reactivity amplified the negative association between blaming others and self-harm.
This supplementary analysis was conducted to better understand whether the protective association of blaming others observed in the main analyses varied depending on stress reactivity. The significant interaction confirms that the effect of blaming others is conditional on stress levels, becoming more pronounced as stress reactivity increases.
Discussion
The main aim of this study was to clarify how cognitive emotion regulation strategies, stress reactivity, and peer victimisation contribute to STBs in autistic adolescents and young adults without intellectual disability to capture both their specificity and shared dimensionality.
From a bivariate perspective, analyses showed a pattern of associations in which intrapersonal vulnerabilities and interpersonal adversities were related to increase suicidal distress (i.e. ideation and behaviours), and vice versa. However, when examining suicidal ideation and self-harm behaviours separately, the regression models demonstrated both shared mechanisms and distinct psychopathological signatures.
Self-harm was most strongly associated with peer victimisation, followed by age, with blaming others emerging as a strong protective factor. In this regard, the fact that interpersonal difficulties were the strongest associated factor is consistent with contemporary Interpersonal Theory of Suicide (IPTS; Joiner, 2005; Pelton et al., 2020; Van Orden et al., 2012) supporting the idea that recurrent interpersonal experiences of peer victimisation, exclusion, hostility, or social threat may foster feelings of thwarted belongingness and perceived burdensomeness, two processes well known to be strongly implicated in the emergence of STBs in vulnerable populations. In this sense, the results highlight that autistic individuals exposed to hostile contexts or exclusion by their peers may experience more negative self-representations in relation to others, which may be associated with greater suicidal distress (Pelton et al., 2020). On the other hand, the protective association between blaming others and self-harm is consistent with the self-serving attributional bias theory, according to which attributing negative experiences to external causes may serve a self-protective function by preserving self-evaluation and attenuating the internalisation of distress (Mezulis et al., 2004).
In contrast, the model examining suicidal ideation explained a more modest proportion of variance and revealed a less cognitively differentiated profile. Peer victimisation remained the only significant associated factor, whereas no individual cognitive emotion regulation strategy emerged as a unique contributor. This suggests that suicidal ideation in autistic individuals may reflect a broader affective urgency or behavioural coping response, less tightly tied to specific cognitive strategies than self-harm.
Taken together, these findings suggest that although self-harm and suicidal ideation share common characteristics (e.g. peer victimisation), they also exhibit notable differences at the intrapersonal level. This pattern is consistent with evidence indicating that suicidality in autism may be linked to partially distinct profiles that are partly different from those observed in non-autistic populations (Pelton et al., 2020). In line with this view, peer victimisation emerged as a central and recurrent vulnerability factor, remaining the strongest associated factor for STBs even when considered alongside cognitive emotion regulation strategies and stress reactivity (Chang et al., 2024; Holden et al., 2020; Moseley et al., 2022). At the same time, our findings extend the literature by showing that suicidal ideation and self-harm diverge in their intrapersonal architecture. While self-harm was associated with a more cognitively specific pattern, particularly involving attributional processes (Mezulis et al., 2004; Millgram et al., 2024), suicidal ideation appeared to reflect broader affective dysregulation, less tied to distinct cognitive mechanisms (Jenkins & Schmitz, 2012). This distinction is consistent with ideation-to-action frameworks suggesting that autistic individuals may show different emotional patterns of association from distress to ideation and, in some cases, to behavioural action (Moseley et al., 2020). Thus, while our findings confirm the centrality of interpersonal adversity highlighted by Pelton et al. (2020), they also contribute novel insights by delineating how stress reactivity and cognitive emotion regulation intersect with social experiences to shape partially distinct risk profiles for STBs.
In this regard, the moderation analysis added further shades to the findings showing that the effect of blaming others on self-harm depends on the level of stress reactivity. At low levels of stress reactivity, blaming others had no significant association with self-harm; however, at moderate and especially high levels of stress reactivity, blaming others became increasingly protective. This finding is consistent with stress-diathesis models, which argue that vulnerabilities become more relevant under conditions of high stress (Van Heeringen, 2012). In this case, it is possible that attributing blame externally may mitigate the intensification of self-critical cognitions when stress overwhelms regulatory resources (Mezulis et al., 2004). This model illustrates that the adaptability of cognitive strategies is context-sensitive and that individuals with high stress reactivity may rely on compensatory mechanisms that are not necessarily consistent with traditional classifications of adaptive and maladaptive regulation.
Finally, the CCAs offered an exploratory integrative perspective by revealing how the sets of cognitive strategies relate to STBs. The maladaptive CCA showed that self-blame, rumination, and catastrophizing formed a coherent latent dimension strongly associated with the STBs domain, suggesting a shared underlying pattern of maladaptive intrapersonal regulation processes. This supports dimensional conceptualisations in which STBs reflect different expressions of a broader dysregulation-related distress construct (Tørmoen et al., 2013). On the other hand, the adaptive CCA, although accounting for a smaller proportion of variance, was primary defined by positive refocusing and blaming others, with a more complex contribution from positive reappraisal, which may reflect cognitive styles characteristic of autism, such as over-analysis or circular reappraisal. Taken together, these exploratory multivariate findings suggest that suicidal ideation and self-harm are characterised by partially overlapping patterns of association with cognitive emotion regulation strategies, although their individual correlates differ when examined separately.
However, some limitations temper the interpretation of the results. Suicidal ideation and self-harm were assessed through two individual ASEBA items, which limited the depth and specificity of measurement. This approach did not permit a clear distinction between non-suicidal self-injury and suicidal behaviour. Therefore, the findings should be interpreted with caution when drawing conclusions about suicidality, although these items still provide clinically meaningful information on suicide-related distress and self-harm phenomena. The cross-sectional design does not allow for causal inferences, and the clinical nature of the sample may limit its generalisability. In addition, the broad developmental span of the sample may have introduced further heterogeneity, as adolescents and young adults may differ in emotion regulation, social experiences, and suicide-related vulnerability. Likewise, co-occurring psychiatric conditions were not used as exclusion criteria and may also have influenced the observed associations. Furthermore, factors such as impulsivity, camouflaging, alexithymia, and sensory sensitivities, which may influence cognitive and emotional processes in autism, could not be included in this study. Future research would benefit from longitudinal and multimodal designs, including physiological markers of stress or behavioural measures of emotion regulation, and from examining whether specific profiles of cognitive and interpersonal risk can guide personalised prevention strategies for suicidal distress in autistic individuals.
Taken together, these findings highlight a multidimensional configuration of STBs in autistic individuals, where intrapersonal (e.g. cognitive emotion regulation strategies), interpersonal (e.g. peer victimisation), and stress-reactive processes interact in dynamic and mutually reinforcing pathways. From a clinical perspective, this suggests that interventions should not focus on a single dimension but should address the relational contexts in which autistic individuals develop and express distress. Victimisation by peers has emerged as a consistent risk factor, underscoring the urgency of targeted prevention efforts in schools and community settings. Furthermore, the context-dependent function of strategies such as blaming others underscores the need for flexible, tailored approaches to emotion regulation work, rather than assuming the universal adaptiveness or maladaptiveness of cognitive responses. In this regard, specific interventions such as dialectical behaviour therapy (DBT) may be especially relevant, as emerging evidence suggests that reductions in suicidal symptoms among autistic individuals are achieved partly through emotion-regulation processes (Huntjens et al., 2025).
Supplemental Material
sj-docx-1-aut-10.1177_13623613261458864 – Supplemental material for Cognitive Emotion Regulation, Peer Victimisation, and Stress Reactivity as Multidimensional Pathways to Suicidality and Self-Harm in Autistic Individuals Without Intellectual Disability
Supplemental material, sj-docx-1-aut-10.1177_13623613261458864 for Cognitive Emotion Regulation, Peer Victimisation, and Stress Reactivity as Multidimensional Pathways to Suicidality and Self-Harm in Autistic Individuals Without Intellectual Disability by Giuseppe Alessio Carbone, Laura Nigro, Laura Ilen, Clémence Feller, Julie Husmann and Maude Schneider in Autism
Supplemental Material
sj-docx-2-aut-10.1177_13623613261458864 – Supplemental material for Cognitive Emotion Regulation, Peer Victimisation, and Stress Reactivity as Multidimensional Pathways to Suicidality and Self-Harm in Autistic Individuals Without Intellectual Disability
Supplemental material, sj-docx-2-aut-10.1177_13623613261458864 for Cognitive Emotion Regulation, Peer Victimisation, and Stress Reactivity as Multidimensional Pathways to Suicidality and Self-Harm in Autistic Individuals Without Intellectual Disability by Giuseppe Alessio Carbone, Laura Nigro, Laura Ilen, Clémence Feller, Julie Husmann and Maude Schneider in Autism
Supplemental Material
sj-png-1-aut-10.1177_13623613261458864 – Supplemental material for Cognitive Emotion Regulation, Peer Victimisation, and Stress Reactivity as Multidimensional Pathways to Suicidality and Self-Harm in Autistic Individuals Without Intellectual Disability
Supplemental material, sj-png-1-aut-10.1177_13623613261458864 for Cognitive Emotion Regulation, Peer Victimisation, and Stress Reactivity as Multidimensional Pathways to Suicidality and Self-Harm in Autistic Individuals Without Intellectual Disability by Giuseppe Alessio Carbone, Laura Nigro, Laura Ilen, Clémence Feller, Julie Husmann and Maude Schneider in Autism
Footnotes
Ethical Considerations
The study was approved by the Cantonal Research Ethics Committee of Geneva (CCER; 2018-01117) and conducted in accordance with the Declaration of Helsinki.
Author Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Swiss National Science Foundation (Grant number: 10002308) to Maude Schneider
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.