
Abstract
Wandering – or leaving a supervised space and/or care of a responsible person – disproportionately affects children with autism and can lead to serious injury. We describe parent-reported wandering in children with autism in early childhood and adolescence and characterize wandering in adolescence. Of 258 teens with autism enrolled in the Study to Explore Early Development, caregivers reported that 45% never wandered, 41% wandered only in early childhood, and 14% wandered at least once in adolescence (including 9% that wandered at both time points). Childhood externalizing behavior problems were positively associated with wandering only in early childhood and at least once in adolescence compared to never wandered (both p < .01). Adolescents who wandered most often left public places (58.3%). To address wandering, caregivers most often added home locks/alarms (30.6%) and least often placed a tracking device (8.3%) on the adolescent. In conclusion, wandering is less common among adolescents than young children with autism but still presents opportunities for intervention. These findings can help partners communicate that childhood externalizing behavior problems are associated with wandering regardless of age and promote awareness of and access to interventions that can improve health and safety.
Lay Abstract
Wandering occurs when a child leaves a safe space. Children with autism wander more than other children. This can lead to serious injury. We describe wandering in children and adolescents with autism. In total, 258 teens with autism were included in the analysis. Caregivers reported that 45% never wandered, 41% wandered only in early childhood, and 14% wandered at least once in adolescence (including 9% that wandered at both time points). Children with behaviors like hyperactivity were more likely to wander in both early childhood and adolescence. Adolescents who wandered most often left public places (58.3%). To address wandering, caregivers most often added home locks/alarms (30.6%) and least often placed a tracking device (8.3%) on the adolescent. In sum, wandering is less common among adolescents than young children with autism. However, we can still help families with adolescents with autism who wander. One way to help these families is to educate people that behavior problems like hyperactivity are associated with wandering regardless of age. Another way to help these families is to increase ways to address wandering away from the home to keep adolescents with autism safe.
Keywords
Introduction
Wandering – or leaving a supervised space and/or care of a responsible person – is common among toddlers who are learning to explore their environment (American Academy of Pediatrics, 2021). It is much less common in older children and can be associated with serious injury, especially among those who cannot independently share their names, addresses, or phone numbers if they get lost. Wandering disproportionately affects children with intellectual and developmental disabilities, with some studies suggesting that a majority of those who wander are diagnosed with autism (A. Anderson et al., 2020; C. Anderson et al., 2012; Barnard-Brak et al., 2016; Kiely et al., 2016; Wiggins et al., 2020). Child factors associated with wandering in early childhood are anxiety, hyperactivity, significant early learning delays, and the severity of autism traits (A. Anderson et al., 2020; C. Anderson et al., 2012; Hong et al., 2018; Rice et al., 2016; T-Pederson et al., 2021; Wiggins et al., 2020).
Wandering among children with autism has been associated with risk for serious injury and premature mortality. In one study, 65% of caregivers reported that their child with autism who wandered was in danger of traffic injury and 24% reported that their child was in danger of drowning (C. Anderson et al., 2012). In another study, 17% of people with autism who were reported missing were found dead (National Autism Association, 2017). Accidental drowning accounted for most of these fatalities (71%) followed by traffic injury (18%). Wandering has also been described as the most commonly reported activity leading to fatal drowning incidents among children with autism 3–14 years of age (Guan & Li, 2017).
Adverse caregiver and family impacts of wandering have also been reported. For instance, 62% of caregivers of children with autism reported they did not attend or enjoy activities outside the home because of child wandering, and 56% said that wandering was one of the most stressful parenting challenges (Pereira-Smith et al., 2019). In addition, wandering concerns may affect up to 73% of caregivers’ decisions to let their child spend time with friends or family in their absence (McLaughlin et al., 2018). Despite these concerns, many parents of children with autism do not receive anticipatory guidance on how to prevent wandering or create emergency response plans (McLaughlin et al., 2018).
There are many available strategies to prevent wandering and intervene when a wandering incident occurs. The most commonly reported prevention and intervention measures implemented by caregivers are physical barriers like gates, fences, and locks; some of the least commonly reported are medical bracelets, tracking devices, and service animals (Andersen et al., 2020; Kiely et al., 2019; Pereira-Smith et al., 2019). Most (96%) caregivers of children with autism have used at least one of these strategies and rate their effectiveness as “good” or “very good” 75% of the time (Andersen et al., 2020). However, a majority (68%) also rate the overall burden of implementing wandering interventions as “high” or “very high” (Andersen et al., 2020). Caregivers identified cost as a major deterrent in using tracking devices to intervene when a wandering incident occurs in one previous study (Kiely et al., 2019).
Among children with autism, the reported prevalence of wandering is between 33% and 60%, with decreasing prevalence as children age based on cross-sectional data (Kiely et al., 2016; Rice et al., 2016; T-Pederson et al., 2021; Wiggins et al., 2020). However, it is unclear how prevalence estimates differ at each time point (i.e., early childhood and adolescence), and early childhood predictors of adolescent wandering are largely unknown. Factors associated with adolescent wandering, like locations where they wandered, use of words to communicate, and recent intervention measures added by caregivers, are also largely unknown.
The first goal of this analysis was to describe parent-reported wandering in children with autism in early childhood and adolescence and identify early childhood factors associated with wandering only in early childhood and at least once in adolescence. A second goal was to examine, for adolescents who wandered, locations from where they wandered, overall communication abilities, and prevention and intervention measures added by their caregivers in the last 12 months.
It is important to note that the terms “wandering” and “elopement” are sometimes defined separately and other times used interchangeably in the literature. Elopement can sometimes include more intense examples of behavior, like running away from caregivers or bolting into the street. In this article, we used the term “wandering” to characterize leaving a supervised space and/or care of a responsible person to align with the National Autism Association (2022).
Method
Data for this analysis were from the Study to Explore Early Development – Phase 1 (SEED1, 2006–2011) and the SEED Teen Follow-Up Survey (SEED Teen, 2018–2021). SEED1 is a multi-site case-control study of 2- to 5-year-old children ascertained through health and education providers via diagnostic codes/exceptionality criteria and a random sample of state birth certificate records. Caregivers completed the Social Communication Questionnaire (SCQ; Rutter et al., 2003), a screening measure that assessed their child’s likelihood for autism. Children completed the Mullen Scales of Early Learning (MSEL; Mullen, 1995), which assessed their early learning abilities. Children who demonstrated likelihood for autism on the SCQ (scoring 11 or higher, to maximize sensitivity in preschool children in the SEED sample; see Allen et al., 2007; Lee et al., 2007; Wiggins et al., 2007) or had a previous autism diagnosis completed a comprehensive developmental evaluation that included the Autism Diagnostic Interview – Revised (ADI-R; Lord et al., 1994) and the Autism Diagnostic Observation Schedule (ADOS; Gotham et al., 2007; Lord et al., 2000). Study group classifications based on an in-person developmental evaluation were autism, other developmental disabilities, and population comparison. Details on SEED1 can be found in Schendel et al. (2012) and Wiggins et al. (2015).
SEED Teen is a longitudinal follow-up of children who completed SEED1 when they were 12–16 years old. The goals of SEED Teen were to assess the health and healthcare needs of children enrolled in SEED1 as they transitioned into adolescence and to understand early childhood factors related to adolescent health outcomes. SEED Teen participants were recruited from four of the six original SEED1 sites: Georgia, Maryland, North Carolina, and Pennsylvania. The North Carolina site assumed responsibility for collecting survey data from participants in Maryland, North Carolina, and Pennsylvania. This analysis included adolescents who completed SEED1 and whose caregiver reported on the SEED Teen survey a previous diagnosis of autism given by a healthcare provider (n = 269). Of these, 258 (95.9%) had data on wandering at both time points studied and comprised the sample for these analyses. Both SEED1 and SEED Teen were approved by the Institutional Review Boards at each study site.
SEED1 Analytic Variables
Caregiver Telephone Interview
Upon SEED1 enrollment, caregivers completed a telephone interview that collected maternal demographic and pregnancy information and the early developmental history of their child. Demographic variables collected on the telephone interview used in this analysis were family income (above federal poverty threshold no/yes), maternal education (high school or less, some college, college degree, advanced degree), and maternal race/ethnicity (Hispanic, non-Hispanic Black, non-Hispanic Other, non-Hispanic White).
Child Behavior Checklist/1½–5 Years
Caregivers completed the Child Behavior Checklist (CBCL; Achenbach, 2013) to assess wandering and emotional and behavioral problems when their child was 2–5 years old. The CBCL contains 99 behaviors rated as “not true,” “somewhat or sometimes true,” or “very true or often true” in the previous 3 months. Individual items are rated separately by the caregiver, and then some are combined into externalizing (i.e., attention problems and aggression behavior) and internalizing (i.e., emotionally reactive, anxious/depressed, somatic complaints, withdrawn) scales. CBCL externalizing and internalizing t-scores range from 28 to 100, with higher scores representing more behavior problems.
There are no standardized measures of wandering in early childhood. We therefore used an item on the CBCL that asks if the child “wanders away” as a proxy indicator for wandering behavior in the SEED sample. This item was categorized as “no” if the parent answered as “not true” and “yes” if the parent answered as “somewhat or sometimes true” or “very true or often true.” The CBCL wandering item is not included in the items used to derive externalizing or internalizing scales.
MSEL
The MSEL (Mullen, 1995) is a standardized in-person evaluation of the early learning abilities of young children in four areas of functioning: expressive language, receptive language, fine motor, and visual reception skills. Child performance in each of these areas is combined to yield an early learning composite (MSEL ELC) score with a mean of 100 and a standard deviation of 15, with higher scores representing more advanced abilities.
Social Responsiveness Scale – Second Edition
The Social Responsiveness Scale – Second Edition (SRS-2; Constantino, 2002) is a standardized 65-item caregiver questionnaire that assesses the distribution of autism traits in the general population. In general, items measure autistic mannerisms, social awareness, social cognition, social communication, and social motivation. SRS-2 t-scores range from 30+, with higher scores representing more autistic traits.
The Vineland Adaptive Behavior Scale – Second Edition
The Vineland Adaptive Behavior Scale – Second Edition (VABS-2; Sparrow et al., 2005) is a standardized semi-structured caregiver interview that assesses sufficiency of skills used on a daily basis in four areas of functioning: communication, daily living, motor, and social skills. The VABS-2 adaptive behavior composite (VABS ABC) has a mean of 100 and a standard deviation of 15, with higher scores representing more advanced abilities.
SEED Teen Analytic Variables
SEED Teen Health and Development Survey
The SEED Teen Health and Development Survey was developed by SEED investigators to assess the health and well-being of SEED1 participants when they were 12–16 years old. Survey topics were chosen by review of the literature and input from people with lived autism spectrum disorder (ASD) experience. Nearly all questions (97%) were selected from existing national surveys or surveillance systems, like the National Survey of Children’s Health (NSCH), because these questions have been extensively tested and were developed by experts who had experience with the topics under investigation. Adolescents were classified as ever having autism if the caregiver endorsed the statement: “Has a doctor or other healthcare provider ever told you that this child has autism, Asperger’s disorder, pervasive developmental disorder, or autism spectrum disorder?” This question was extracted from the NSCH.
The SEED Teen question on wandering, which differs from the proxy CBCL indicator for wandering in SEED1, was also extracted from the NSCH (Pathways follow-up survey of children with special health care needs) (Data Resource Center for Child and Adolescent Health, 2011) and was phrased:
Some children are likely to wander off and become so lost that it is necessary to search for them. Please tell us if this child wandered off or became lost from any of these places DURING THE PAST 12 MONTHS, even if it occurred just once.
Your home?
Someone else’s home such as a relative, friend, neighbor, or babysitter?
School, day care, or summer camp?
A store, restaurant, playground, campsite, or any other public place?
Caregivers were also asked:
DURING THE PAST 12 MONTHS have you done any of the following to prevent this child from wandering off or to find them if they become lost? (Check all that apply).
Added fences or gates to your home
Added locks or alarms to your home
Added other barriers to your home
Placed a tracking device on this child
Used an APP or feature on the child’s cell phone
Finally, caregivers were asked about adolescent communication abilities and current insurance coverage. Caregivers reported that their child “verbally communicates using words easily,” “verbally communicates using words with trouble,” or “does not communicate with words” (i.e., verbally communicates with noises or does not verbally communicate). Current insurance coverage was categorized into any form of private insurance (with or without public insurance) versus public-only insurance.
Statistical Analyses
Descriptive statistics were used to depict the sample and demonstrate the percentage of children who wandered in early childhood and adolescence. Three groups were then created: never wandered, wandered only in early childhood, and wandered at least once in adolescence. Chi-square analyses assessed differences between these three groups in terms of demographic characteristics (i.e., child sex, family income relative to the federal poverty level, insurance status, maternal education, and maternal race/ethnicity), and analysis of variance (ANOVA) assessed differences in early childhood characteristics (i.e., overall scores for CBCL externalizing and internalizing behavior problems, MSEL early learning abilities, SRS autistic traits, and VABS-2 adaptive delays).
Separate Poisson regression analyses identified early childhood factors associated with (1) wandering only in early childhood and (2) wandering at least once in adolescence. For these analyses, never wandered was considered the referent category, and child sex, family income relative to the federal poverty level, insurance status, maternal race/ethnicity, and maternal education were considered covariates. Predictors were continuous CBCL, MSEL, SRS-2, and VABS-2 scores. Missing data were handled via listwise deletion (i.e., complete case analysis); no variables were missing more than 7% of data (see Table 1 footnote).
Characteristics of Adolescents With Autism Who Did and Did Not Wander, Study to Explore Early Development (SEED), 2006–2011, and SEED Teen Survey, 2018–2021.
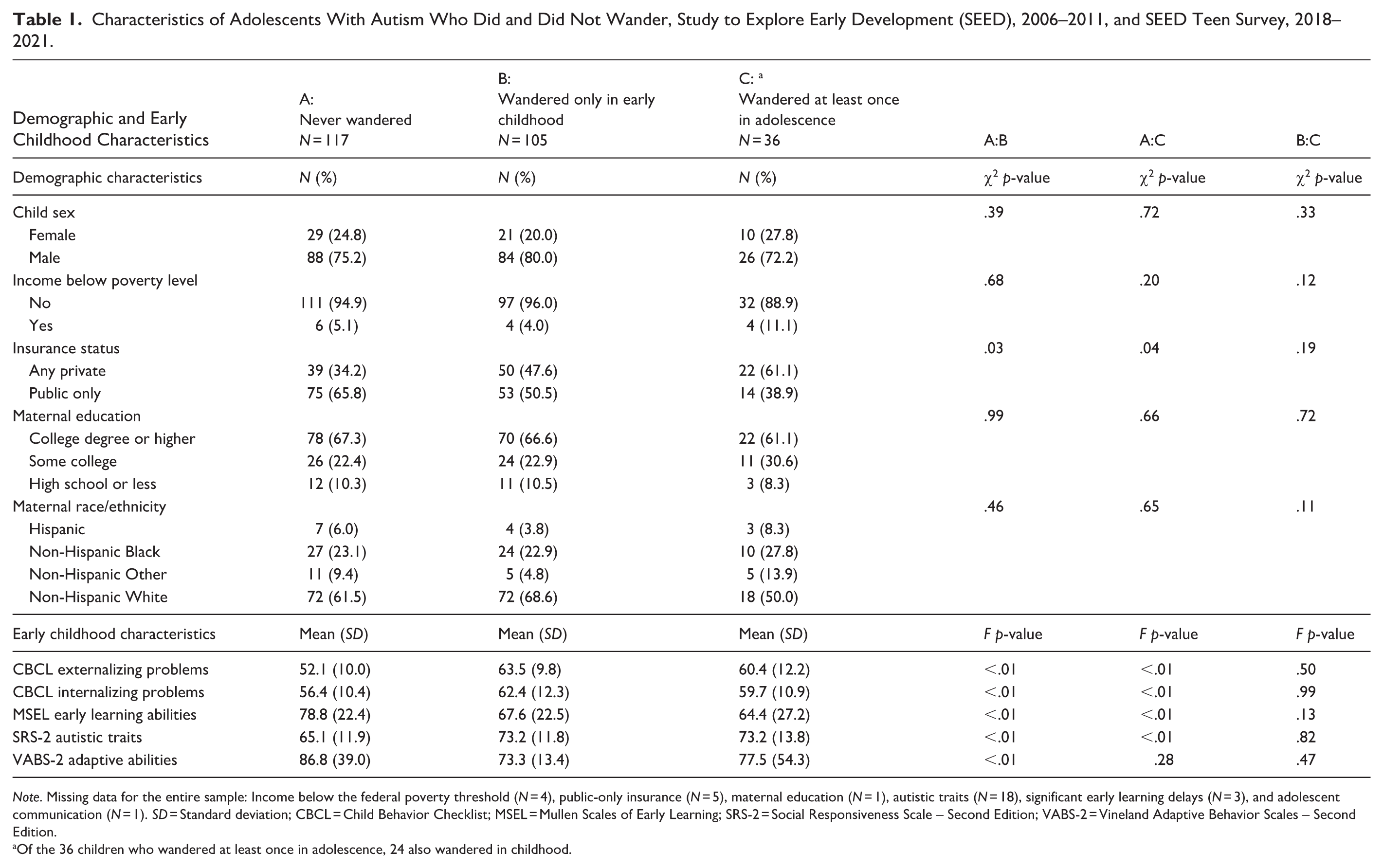
Note. Missing data for the entire sample: Income below the federal poverty threshold (N = 4), public-only insurance (N = 5), maternal education (N = 1), autistic traits (N = 18), significant early learning delays (N = 3), and adolescent communication (N = 1). SD = Standard deviation; CBCL = Child Behavior Checklist; MSEL = Mullen Scales of Early Learning; SRS-2 = Social Responsiveness Scale – Second Edition; VABS-2 = Vineland Adaptive Behavior Scales – Second Edition.
Of the 36 children who wandered at least once in adolescence, 24 also wandered in childhood.
Descriptive statistics were used to examine, for adolescents who wandered, locations from where they wandered, overall communication abilities, and prevention measures added by their caregivers in the last 12 months.
Results
Among 258 SEED participants with autism included in this analysis, 50% (n = 129) wandered between 2 and 5 years of age and 14.0% (n = 36) wandered between 12 and 16 years of age. Characteristics of adolescents who never wandered (N = 117), wandered only in early childhood (N = 105), and wandered at least once in adolescence (N = 36) are reported in Table 1. The groups were similar in terms of demographic characteristics, except those who never wandered were more likely to have public-only insurance than those who wandered only in early childhood and sometime in adolescence. Those who never wandered had lower mean SRS-2 values (indicating fewer autistic traits), lower mean CBCL values (indicating fewer externalizing and internalizing behavior problems), and higher mean MSEL values (indicating more early learning abilities) than those who wandered in early childhood or at least once in adolescence. Adolescents who never wandered had higher mean VABS-2 adaptive skills scores than those who wandered only in childhood.
Compared to youth who never wandered, CBCL scores for childhood externalizing behavior problems were significantly higher for youth who wandered only in early childhood (adjusted prevalence ratio = 1.04; 95% confidence interval = [1.02, 1.06]; p < .01) as well as youth who wandered at least once in adolescence (adjusted prevalence ratio = 1.05; 95% confidence interval = [1.01, 1.08]; p < .01). This means that for every unit increase in CBCL externalizing symptoms (i.e., t-score), the likelihood of wandering increased by 4% in early childhood and increased by 5% in adolescence. Other early childhood characteristics were not associated with wandering at either developmental period (Table 2).
Early Childhood Factors Associated With Wandering Only in Early Childhood and Sometime in Adolescence Compared to Never Wandered, Study to Explore Early Development (SEED), 2006–2011, and SEED Teen Survey, 2018–2021.
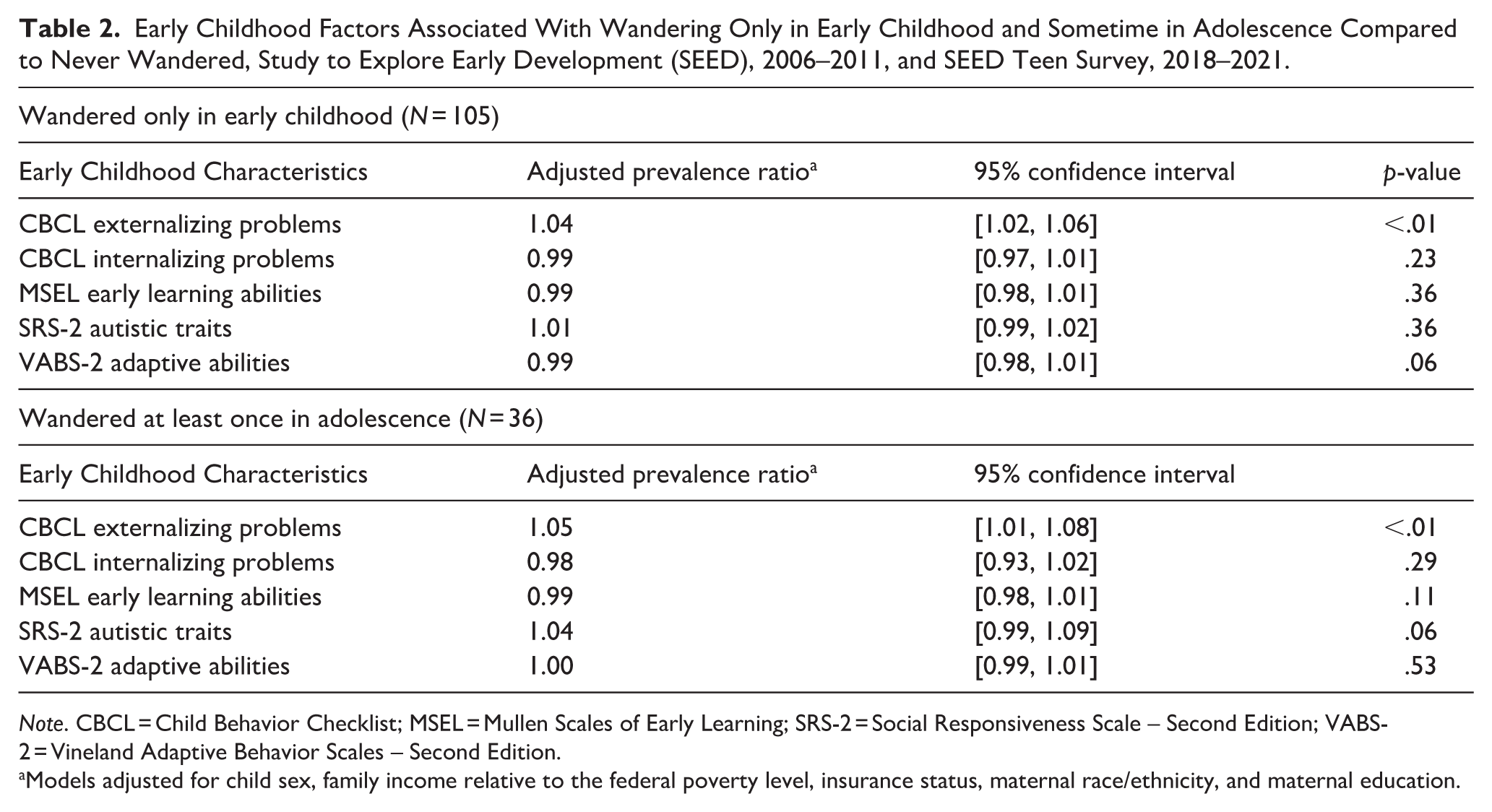
Note. CBCL = Child Behavior Checklist; MSEL = Mullen Scales of Early Learning; SRS-2 = Social Responsiveness Scale – Second Edition; VABS-2 = Vineland Adaptive Behavior Scales – Second Edition.
Models adjusted for child sex, family income relative to the federal poverty level, insurance status, maternal race/ethnicity, and maternal education.
Among those who wandered at least once in adolescence (N = 36), more than half had wandered from a store, restaurant, playground, campsite, or other public place; about a third wandered from their own home and from school, daycare, or summer camp, respectively; and about a fifth wandered from someone else’s home. These categories were not mutually exclusive (Figure 1).
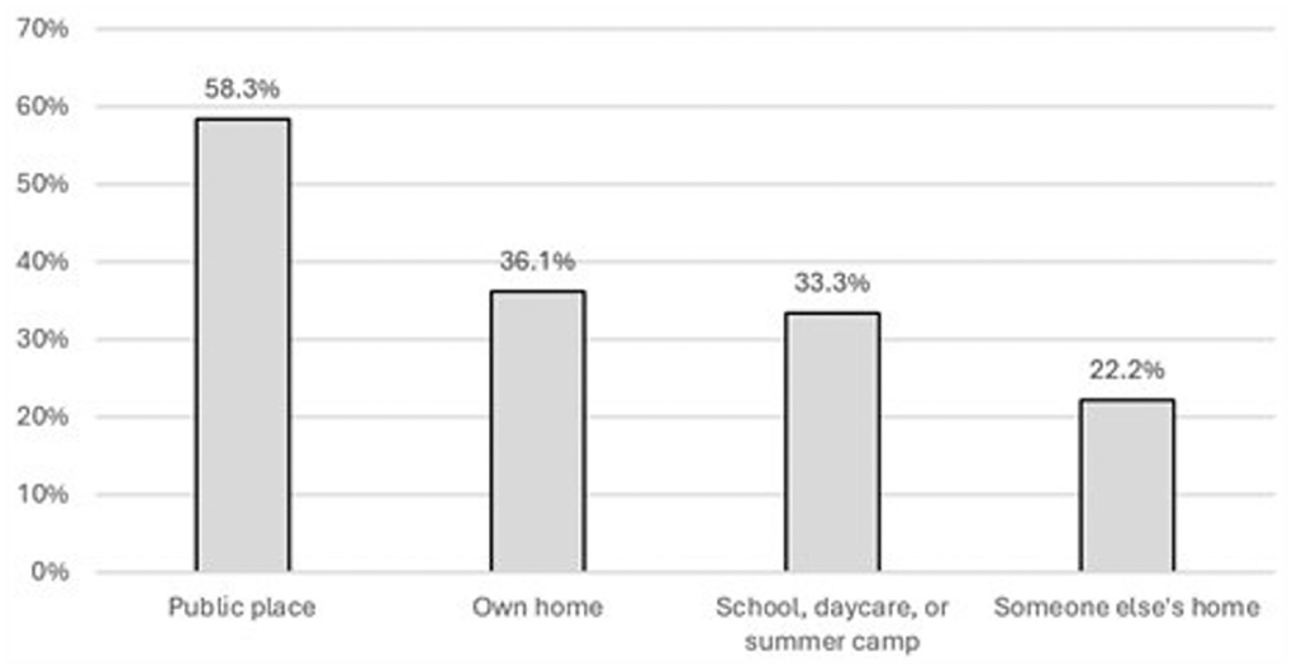
Locations where adolescents with autism were reported to wander,a study to explore the development of the SEED teen survey, 2018–2021.
Among those who wandered at least once in adolescence (N = 36), 13 (36.1%) communicated using words easily, 15 (41.7%) communicated using words with trouble, and 8 (22.2%) did not communicate with words (compared to 76.9%, 20.5%, and 2.6%, respectively, among those who never wandered). The most commonly reported prevention/intervention measures added in the last 12 months in this group of adolescents were locks or alarms, followed by other barriers, an app or other phone feature, fences or gates, and tracking devices (Figure 2). These categories also were not mutually exclusive.
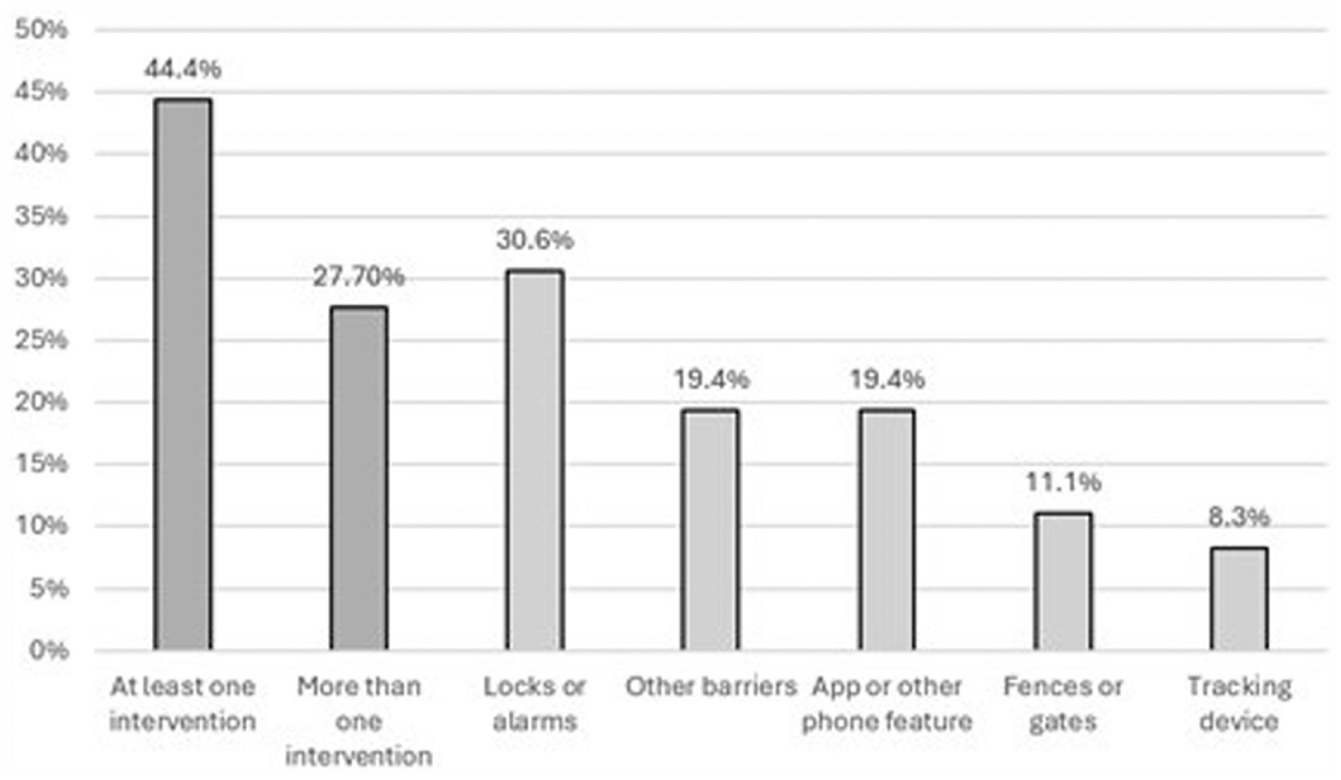
Percentage of caregiversa with adolescents who wandered that added a prevention measure in the last 12 months, study to explore the development of the SEED teen survey, 2018–2021.
Discussion
There are several key findings from this longitudinal analysis. First, we observed that half of caregivers reported that their child with autism wandered in early childhood, and 14% (one in seven) reported that they wandered in adolescence. Childhood externalizing behavior problems were significantly associated with wandering regardless of age. Public places were the most common locations from which adolescents wandered, and almost one quarter of these adolescents did not use words to communicate. Although adolescents most often wandered from public places, fewer caregivers recently implemented safety strategies away rather than near the home, like apps or other phone features or tracking devices. These findings offer important information for families, providers, and community leaders to identify children and adolescents with autism who may be at risk for wandering and implement measures to keep them safe. The following sections relay this information to be translated into pediatric and/or public health practice.
Identifying Factors Associated With Wandering
The mechanism behind the observed association between externalizing behaviors and wandering cannot be ascertained through these cross-sectional data. However, knowledge of these associations can inform pediatric practice. Childhood externalizing behavior problems were defined as attention problems and aggressive behavior in these analyses. Other studies found that a diagnosis of attention-deficit/hyperactivity disorder (ADHD) was associated with wandering in early childhood (Andersen et al., 2020; McLaughlin et al., 2018). Our study extends upon this previous work and suggests that symptoms of ADHD are also associated with wandering in adolescence. Pediatricians and other providers can educate families about this association, provide anticipatory guidance, and help develop emergency response plans to prevent and respond to wandering incidents (McLaughlin et al., 2018; T-Pederson et al., 2021). Moreover, providers may be able to address potential upstream factors that can lead to wandering; for example, identifying antecedents to wandering and providing strategies or referrals to specialists who can help alleviate their consequences (Hotez & Onaiwu, 2023). The most common evidence-based treatments for wandering after functional analysis are targeted support to increase youth communication abilities, proactively providing desirable behavioral alternatives to wandering, and caregiver coaching (Boyle & Adamson, 2017).
Implementing Measures to Keep Children/Adolescents Safe
Taking proactive measures against wandering may be one way to safeguard children and adolescents with autism from preventable injury. The Be REDy Booklet for Caregivers provided by the National Autism Association (2022) provides a variety of wandering resources for families, including a prevention checklist that recommends alerting neighbors, creating an emergency response plan, identifying triggers, teaching coping skills, and securing the home. Adding physical barriers like home locks and alarms has been a particularly common prevention strategy found in several different studies (Kiely et al., 2016; Pereira-Smith et al., 2019; Rice et al., 2016; Wiggins et al., 2020). A multi-layered approach that considers these strategies along with language prompts, swimming lessons, and social stories is recognized in the Be REDy resources as the best way to achieve optimal safety. Although wandering among children with autism decreases with age, use of these and other prevention resources beyond early childhood may help prevent future wandering behavior in adolescence.
Adolescents with autism most often wandered from public places in ours and a few other studies (Kiely et al., 2016; Rice et al., 2016). Wandering interventions implemented away from the home are not included in the Be REDy Booklet for Caregivers and may therefore be an important component of family and community emergency response plans. For family plans, tracking devices may help locate missing children or adolescents (McLaughlin et al., 2020), although they were the least common intervention added in the last 12 months in these analyses. Other wandering interventions that may be useful away from the home are GPS phone features, medical bracelets or shoe tags, and temporary tattoos with identification (Andersen et al., 2020; Pereira-Smith et al., 2019). Providing financial support for these interventions, as well as access to caregiver-mediated behavioral supports through autism waivers, insurance coverage, and low-intensity support services, may increase use, thereby potentially decreasing the risk for preventable injury.
For community plans, mandatory training of law enforcement officers (LEOs) can increase their confidence when working with people with autism (Kenney et al., 2024; Love et al., 2022). Incorporating ways to interact with minimally verbal individuals can be a critical part of this training since 22.2% of the adolescents who wandered in our sample did not use words to communicate, and another 41.7% communicated using words with trouble, similar to other studies (Gardner et al., 2022; Pereira-Smith et al., 2019). Increasing contact with people with autism in the community is another strategy to help LEOs and other first responders increase confidence and better understand people with autism they may encounter (Love et al., 2022).
We observed that children who never wandered were more likely to have public-only insurance than those who wandered only in early childhood or at least once in adolescence. One study found that private insurance was positively associated with use of wandering alerts (Pereira-Smith et al., 2019), which could lead to reporting bias among caregivers who do not have these alerts in place. Wandering alerts like home security systems are some of the most effective wandering prevention measures with the highest financial burden (Andersen et al., 2020). Funding for wandering alerts by public programs like Medicaid may therefore help bring awareness of wandering to caregivers of all children, regardless of insurance status.
Limitations and Strengths of These Analyses
There are limitations to these analyses. We did not use the same measure of wandering at both time points studied. The adolescent measure required higher severity (i.e., becoming lost and requiring a search), whereas the early childhood item captured any wandering behavior. Therefore, the observed differences over time may reflect measurement differences rather than true developmental change. The CBCL item used to assess wandering in early childhood has not been validated and was used as a proxy indicator since standardized measures of wandering are not available for this age group. The item used to assess the addition of prevention measures in adolescence did not exhaustively query possible approaches; moreover, families may have implemented some of the prevention approaches in the SEED Teen Survey before the specified 12-month period. The number of adolescents who wandered was small (N = 36) and could have contributed to the lack of precision in estimates. Finally, our sample was primarily non-Hispanic White, and caregivers were primarily college-educated, which may limit generalizability.
There are also strengths to the analyses. We examined longitudinal changes in wandering from early childhood to adolescence. In addition, we examined factors associated with adolescent wandering based on research-reliable implementation of standardized instruments in early childhood. We characterized certain aspects of wandering in adolescence (e.g., locations where adolescents wandered) that can guide strategies to keep people with autism safe throughout development.
In conclusion, wandering is a common and potentially harmful behavior among young children with autism, and while the prevalence of wandering decreased with age in our sample, one in seven wandered in adolescence. Pediatricians and others can use findings from these analyses to help communicate that childhood externalizing behavior problems are associated with wandering regardless of age and promote awareness of and access to wandering interventions – both near and away from the home – that can improve health and safety. Future research could evaluate the effectiveness of these interventions and how to best support families of children who wander.
Footnotes
ORCID iDs
Ethical Considerations
All phases of this study were approved by the Institutional Review Boards at the Centers for Disease Control and Prevention (CDC) and each study site.
Consent to Participate
Participants engaged in verbal and written informed consent processes.
Author Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: All phases of this study were funded by the CDC.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
Data used in these analyses are protected under a federal Certificate of Confidentiality to protect the privacy of research participants.