
Abstract
Older adults are increasingly living with and managing multiple chronic conditions. The self-management of illness occurs in a social and political context in which the responsibility for health has shifted from the State to the individual, who is expected to be an active consumer of health care. Although there has been extensive investigation of the management of single chronic conditions, the realities of living with multiple morbidities have largely been ignored, particularly among older adults. Addressing this gap, our study entailed in-depth interviews with 35 older Canadian adults, aged 73 to 91, who had between three and 14 chronic conditions. Self-care emerged as a primary means by which our participants managed their illnesses. Specifically, all of our participants were engaged in some form of self-care in order to cope with often debilitating physical symptoms and functional losses. They also utilized self-care because they had reached the limits of available medical treatment options. Finally, our participants argued that self-care was a moral responsibility that was underscored by gendered motivations. Whereas the men tended to emphasize the importance of self-care for the achievement of masculine ideals of control and invulnerability, the women suggested that self-care allowed them to maintain feminine norms of selflessness and sensitivity to the needs of others. In this way, self-care enabled the men and women to reframe their aging, chronically ill bodies as moral, socially valued bodies. We discuss our findings in relation to the extant research and theorizing pertaining to self-care, gender, and healthism.
Introduction
Increasingly, older adults are living with the physical and social realities of multiple chronic conditions as chronic disease has been identified as the leading cause of mortality and disability around the world (World Health Organization, 2011). In Canada, 77 percent of men and 85 percent of women aged 65+ have at least one chronic condition and the average number of chronic conditions increases with age (Statistics Canada, 2006). Although health care providers and formal health care services play a pivotal role in the treatment of chronic conditions, Kerr et al. (2007: 1635) have sagely noted that ‘most of the burden of chronic disease management falls upon patients and their families’. In particular, the management of chronic illnesses requires individuals to monitor their symptoms, adhere to prescribed treatments and medication regimens, cope with physical limitations and emotional consequences of disease, discipline their bodies through diet, exercise, and other lifestyle modifications, and seek expert advice and intervention only where appropriate. In this context, self-care has become a vital and growing necessity for many community dwelling older adults with multiple morbidities.
Self-care has been defined as ‘the activities individuals, families and communities undertake with the intention of enhancing health, preventing disease, limiting illness, and restoring health’ (World Health Organization, 1983: 2). Thus, self-care is both reactive (concerned with the management of symptoms associated with existing acute and chronic health conditions) and proactive (focused on the prevention of illness through healthy lifestyles) (Ziguras, 2009). Although most research has been concerned with the experiences of middle-aged and young adults, there is a growing body of literature that has included or focused solely on older adults’ engagement in self-care. These studies have investigated such practices as the use of assistive devices, complementary and alternative medicine, diet, exercise, prescription medications, over-the-counter medications and/or supplements, modifications to attitudes, behaviors, and/or routines, health and illness education, home remedies, relaxation, meditation and stress relief practices, rest and sleep, social support, and spirituality (Arcury et al., 2006, 2011a, 2011b; Barlow et al., 2005; Cartwright, 2007; Clark et al., 2008; Grzywacz et al., 2011; Leach and Schoenberg, 2008; Leontowitsch et al., 2010; Venn and Arber, 2011).
Collectively, the research on self-care indicates that gender, age, health status, and socio-economic status are important factors shaping and constraining the individual’s engagement in various health practices. For example, women tend to employ self-care more frequently than men, a fact that has been attributed to women’s greater knowledge about health and alternative health practices as well as to their gender socialization which encourages heightened responsiveness to illness (Eisenberg et al., 1998; Grzywacz et al., 2011; MacLennan et al., 2002; Verbrugge, 1985). Within the Canadian context, older adults use alternative therapies less often than their middle-aged counterparts (Park, 2005) although the presence of chronic illness is associated with increased rates of complementary and alternative therapy usage (Millar, 1997; Park, 2005). Additionally, individuals with higher levels of education and income tend to have more health-related knowledge and greater access (via financial resources and extended health care insurance plans) to alternative therapies (Eisenberg et al., 1998; MacLennan et al., 2002; Millar, 1997; Tindle et al., 2005). In Canada, health practices such as acupuncture, chiropractic, counselling and psychotherapy, massage therapy, naturopathy, physiotherapy, and the use of supplements and some assistive devices are not covered by the publically funded health care system, and are, therefore, less accessible to individuals who have lower incomes and/or lack private health care insurance plans. Canadians pay out of pocket for prescription medications up until they reach pre-set deductible limits based on their net incomes, after which point these costs are subsidized by the Government. For individuals aged 73+, deductibles range from 1.25 to 3 percent of a person’s net income, after which the PharmaCare insurance plan covers 75 percent of the costs of both prescription medications and some designated medical supplies (such as diabetes, mastectomy, and ostomy supplies).
Self-care has been shown to be an important means of negotiating ‘biographical disruption’ (Bury, 1982: 168–170) and maintaining continuity of self in chronic illness (Corbin and Strauss, 1988; Lindsay, 2009; Roberto et al., 2005). For example, the women in Roberto et al.’s (2005) study used a variety of self-care strategies in their efforts to cope with the emotional consequences of their physical losses, including reframing the meanings they attributed to themselves or their activities, lowering their personal expectations, relying on spirituality, or comparing themselves with those less fortunate. These self-care efforts enabled the women to establish and maintain a sense of dignity, acceptance, and serenity in the face of emotionally challenging and identity-threatening alterations to cherished activities.
Similarly, individuals have been found to employ self-care practices in order to regain or retain a sense of control over their often unpredictable chronic illness experiences and trajectories (Corbin and Strauss, 1985; Leach and Schoenberg, 2008; Lindsay, 2009). The need for control tends to be especially identified by individuals diagnosed with terminal illnesses such as cancer and HIV/AIDS. These populations often identify self-care practices such as complementary and alternative medicine as an effective means of treating their symptoms and maximizing their quality of life as well as an alternative to western medicine, particularly when conventional treatments have failed (Alder, 1999; Gillett et al., 2002; Lupton, 1997; Pawluch et al., 2000; Thorne et al., 2002; Yates et al., 1993).
At the same time, some theorists have argued that the current societal and health policy emphasis on self-care has arisen from shifts in broader political and fiscal agendas (Bunton et al., 1995; Crawford, 1980, 2006; Galvin, 2002; Minkler, 1999; Ziguras, 2009). Indeed, Crawford (1980: 368) has argued that healthism, or the ‘preoccupation with personal health as a primary focus for the definition and achievement of well-being; a goal which is to be attained primarily through the modification of life styles, with or without therapeutic help’, underscores contemporary health policies. Healthism assumes that ‘the problem of [and solutions to] health and disease [are situated] at the level of the individual’ (Crawford, 1980: 365) rather than at the collective or governmental level. This shifting of responsibility for health from the State to the individual has been accompanied by a growing expectation that older adults, like their younger counterparts, will be proactive consumers of health care (Bunton et al., 1995; Crawford, 1980, 2006; Galvin, 2002; Leontowitsch et al., 2010, Minkler, 1999; Ziguras, 2009). Health has been redefined as an active status as well as a commodity that individuals are expected to purchase through their investments in myriad self-care products and services (Crawford, 1980, 2006; Leontowitsch et al., 2010).
Although such a shift in thinking about health has created a greater sense of agency for the individual, it has also been accompanied by the redefining of poor health as a signifier of moral laxity and personal failure (Crawford, 1980, 2006; Dworkin and Wachs, 2009; Higgs, 1998; Lupton, 1995). Having chronic health conditions is now considered to be evidence of one’s culpability (Galvin, 2002). Thus, Becker (1986: 19) asserts that ‘being ill is redefined as being guilty’ and the disabled as well as the elderly who fail to age successfully (Rowe and Kahn, 1987, 1997) are increasingly stigmatized (Higgs et al., 2009; Minkler, 1999; Minkler and Fadem, 2002). In this context, self-care is a socially accepted, if not required, means of demonstrating a sufficient ‘will to health’ (Higgs et al., 2009: 687) even when actual health is no longer a reality, thereby shoring up one’s rights of citizenship. However, rather than fully embracing the societal assumption that their health statuses are a barometer for their morality, thereby often condemning themselves, older adults engage in what Higgs and Rees Jones (2009: 86) refer to as the ‘arc of acquiescence’. Pragmatic about the realities of aging and the ensuing physical changes, older adults experience a ‘gradual withdrawal from successful body maintenance and [a] greater acceptance of bodily limits’ (Higgs and Rees Jones, 2009: 86). The timing of this withdrawal from self-care and other bodily investments is influenced by the individual’s socio-economic status and access to resources, which either facilitate or delimit continued engagement in health promotion and maintenance.
To date, the bulk of the self-care in later life research has investigated the practices that individuals employ in their management of single chronic conditions. The relatively few studies that have investigated how older adults with multiple chronic conditions engage in self-care reveal that the management of the symptoms associated with two or more illnesses is often a complex and dynamic process (Corbin and Strauss, 1985; Leach and Schoenberg, 2008; Lindsay, 2009; Roberto et al., 2005). Nevertheless, our understanding of self-care among especially frail men and women in advanced old age is limited as the existing studies have either focused on individuals under the age of 75 (Lindsay, 2009), have not included men in their older aged samples (Roberto et al., 2005), or have utilized samples in which older men were underrepresented (Leach and Schoenberg, 2008). Additionally, multiple chronic conditions in these studies have typically been operationalized as only two or three health issues (Leach and Schoenberg, 2008), although Lindsay’s (2009) sample participants had a range of two to eight chronic conditions (average of 3.3). Finally, the links between self-care and gender norms and ideals have not been fully explicated. In particular, little is known about how self-care is influenced by and simultaneously shapes masculine norms of control, invulnerability, and physical and social power and prowess and feminine ideals of nurturance, cheerfulness, selflessness, and sensitivity to the needs of others (Prentice and Carranza, 2002).
Building on the existing research and addressing the aforementioned gaps in the extant knowledge, our study focuses on the experiences of elderly, very frail men and women with complex health needs. In light of the physical realities of chronic conditions in later life, the shifting of the responsibility for health from the State to the individual, and the accompanying assumption that older adults will be active consumers of self-care products and services, the purpose of our study was to explore how frail, older adults managed their chronic conditions. Our findings provide important insights into why older adults with multiple chronic conditions utilize self-care and how their health practices are shaped by societal norms pertaining to gender and health promotion.
Methods
Study design
Ethical approval was granted by the University of British Columbia Behavioral Research Ethics Board. The study was conducted in British Columbia, Canada, which has a publically funded health care system that provides highly subsidized health care to all citizens, who are required to pay nominal monthly user fees unless they meet low-income criteria. In-depth interviews were conducted with 35 older Canadian individuals (16 men and 19 women), all of whom were interviewed twice either by the first author or one of two graduate student research assistants (with participants being paired with the same interviewer for both sessions). Multiple interviews were conducted to allow for sufficient time to fully discuss the various ways that individuals experienced and managed their multiple chronic conditions, but also because we were cognizant of our participants’ limitations related to their chronic conditions and did not want overly long interviews to result in further physical suffering or hardship. The first set of interviews lasted an average of 1.1 hours and the second set of interviews lasted an average of 1.4 hours. We spent an average of 2.4 hours with each participant and completed a total of 97 interview hours.
Participants were recruited through advertisements in local newspapers (25 participants) and posters in public facilities (five participants). We also sent invitational letters of recruitment to 20 potential participants using a database of 200 individuals who had participated in a previous large scale measurement study concerned with chronic conditions and physical activity in which the first author had been a co-investigator. This generated another five participants. We recruited only those individuals who were 70+ and had a minimum of three chronic conditions, at least one of which was arthritis, back problems, cataracts/glaucoma, diabetes, or heart disease. These conditions were utilized as inclusion criteria because they are the most prevalent chronic illnesses reported by older adults in Canada and are frequently linked to increased rates of disability and dependency (Statistics Canada, 2006). All of the individuals who responded to our call for participants and who met our study criteria (related to age and number and types of chronic conditions) were included. No compensation was given to participants, and all interviews took place either in the participants’ homes or in alternative convenient locations.
Our interviews were semi-structured, and although participants were encouraged to speak freely, we used a topic guide to ensure that there was consistency across all the interviews. During the course of the two interviews, participants were asked to give a brief life history, describe their experiences over time with each of their chronic conditions, discuss the medical care they had received in the past and were currently receiving, reflect on how having multiple chronic conditions impacted their daily lives, physical abilities/disabilities, and social interactions, and identify the various strategies and health practices they employed to manage their chronic conditions. Rigor across multiple interviewers was maintained by holding regular team meetings, reviewing transcripts together, and having the first author (who was the principal investigator) provide on-going feedback and mentorship to the two graduate student interviewers.
Sample
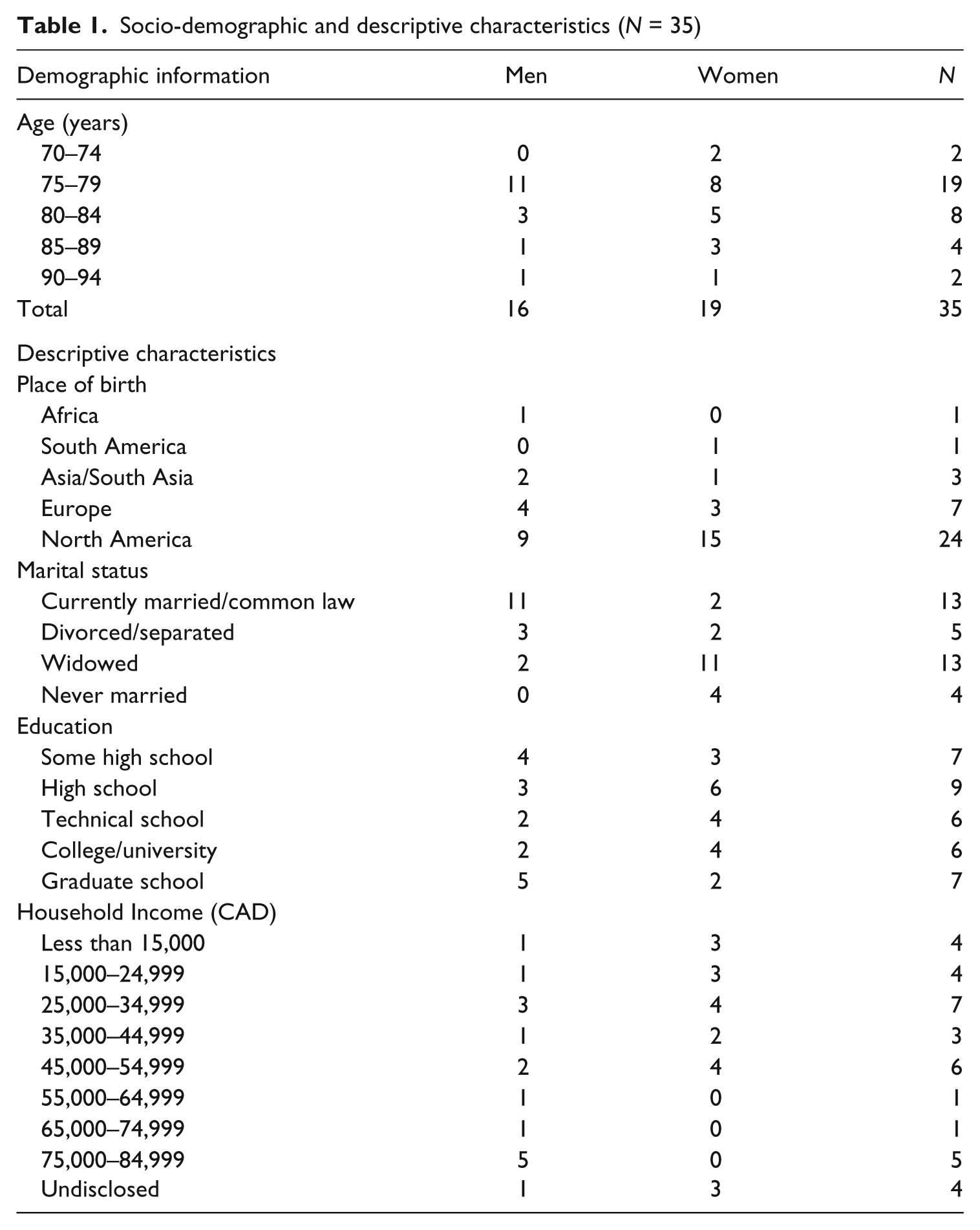
Our sample participants ranged in age from 73 to 91 years, with the average age of the men being 78.6 years and the average age of the women being 80.3 years. Study members had between three and 14 chronic conditions, with most individuals reporting an average of six health problems. Reflecting our recruitment strategy, the most commonly reported chronic conditions included: arthritis (28); back problems (26); heart disease (24); cataracts/glaucoma (14); and cancer (12). Participants reported that their first chronic condition was diagnosed an average of 27.5 years prior to the study and that they had had each of their chronic conditions for a minimum of one year and a maximum of 70 years. Although three participants (two men and one woman) reported having short-term memory loss, none had been diagnosed with Alzheimer’s disease or dementia. All of the participants resided either in their own homes or retirement communities within the greater Vancouver regional district, a large urban center in western Canada. They were diverse with respect to their marital status, incomes, educational attainment, work histories, and countries of origin (see Table 1). Only eight participants (two men and six women) had extended health care insurance.
Socio-demographic and descriptive characteristics (N = 35)
Data analysis
All interviews were digitally recorded and transcribed verbatim by trained research assistants. Following transcription and with the aid of NVivo 8 software, we conducted a thematic analysis (Patton, 2002). In doing so, we drew on the extant literature and theorizing to inform our analysis as well as identifying unique patterns in the data. We began by reading and rereading the transcripts to generate an initial codebook that included (a) types of self-care strategies and (b) reasons for self-care. We subsequently reduced the first category, self-care practices, into specific health behaviors (e.g. such as use of exercise, diet, or prescription medication) and explored the data for gender and social class differences and similarities in terms of rates of usage of particular health strategies. Further analysis of the second broad category, namely reasons for self-care, culminated in the generation of three sub-codes: (a) management of physical symptoms; (b) limits of physician directed care; and (c) healthism. Within each sub-code, we analyzed the data for gender differences. During the multi-staged and complex analytic process, we moved back and forth between the full interview transcripts and the coded data to ensure our interpretations were valid and contextualized in the participants’ broader life histories and experiences. We also continually drew on the extant literature and theorizing about health, gender, aging, and self-care in order to deepen our analysis as well as our understanding of the patterns in our data.
Results
In the sub-sections that follow, we elucidate our participants’ three overarching explanations for their use of self-care: namely, the management of existing physical symptoms and functional losses, compensation for the limits of physician directed care, and adherence to societal norms regarding health.
‘I just try to manage things myself’: self-care to mitigate physical symptoms and suffering
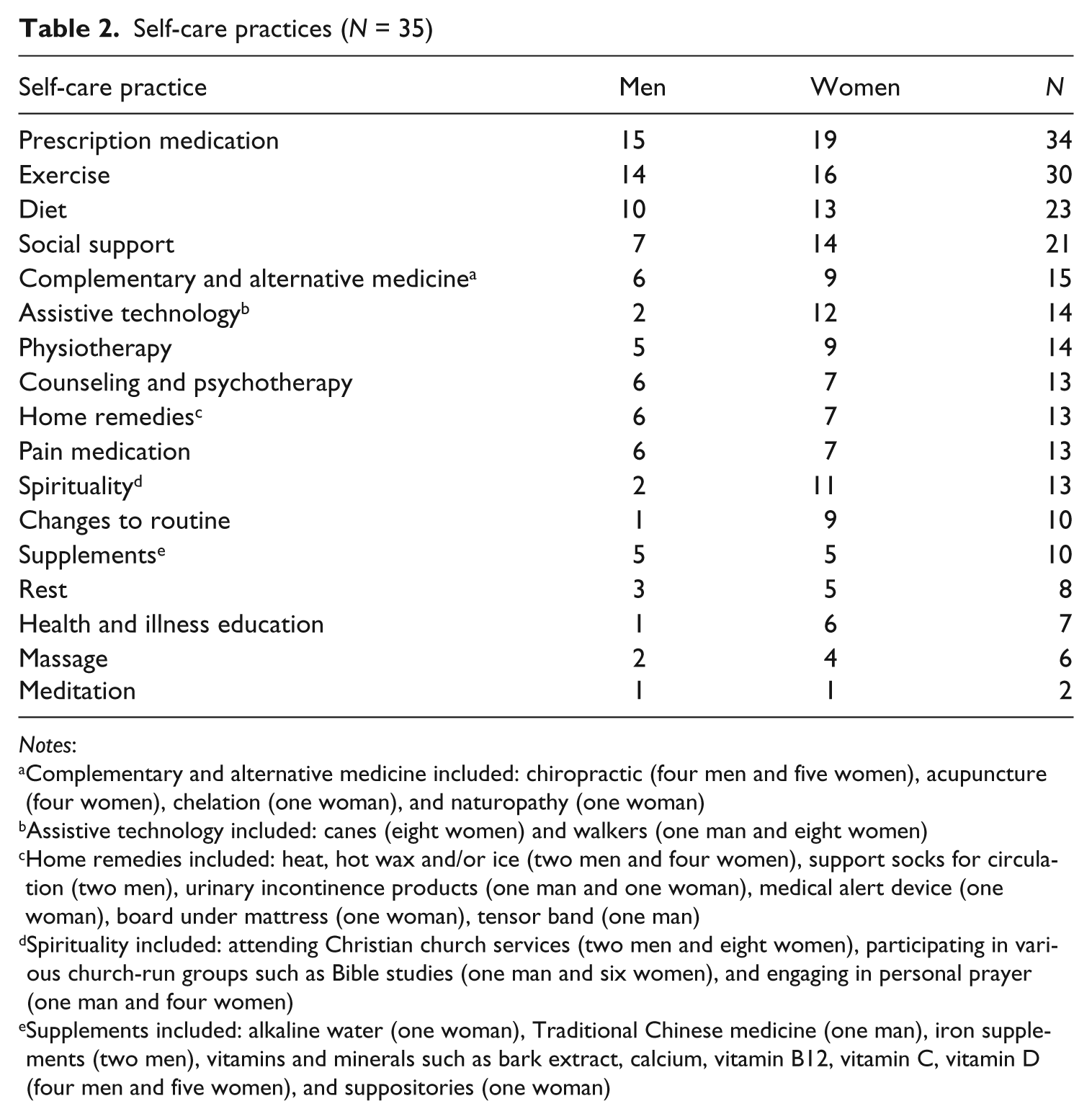
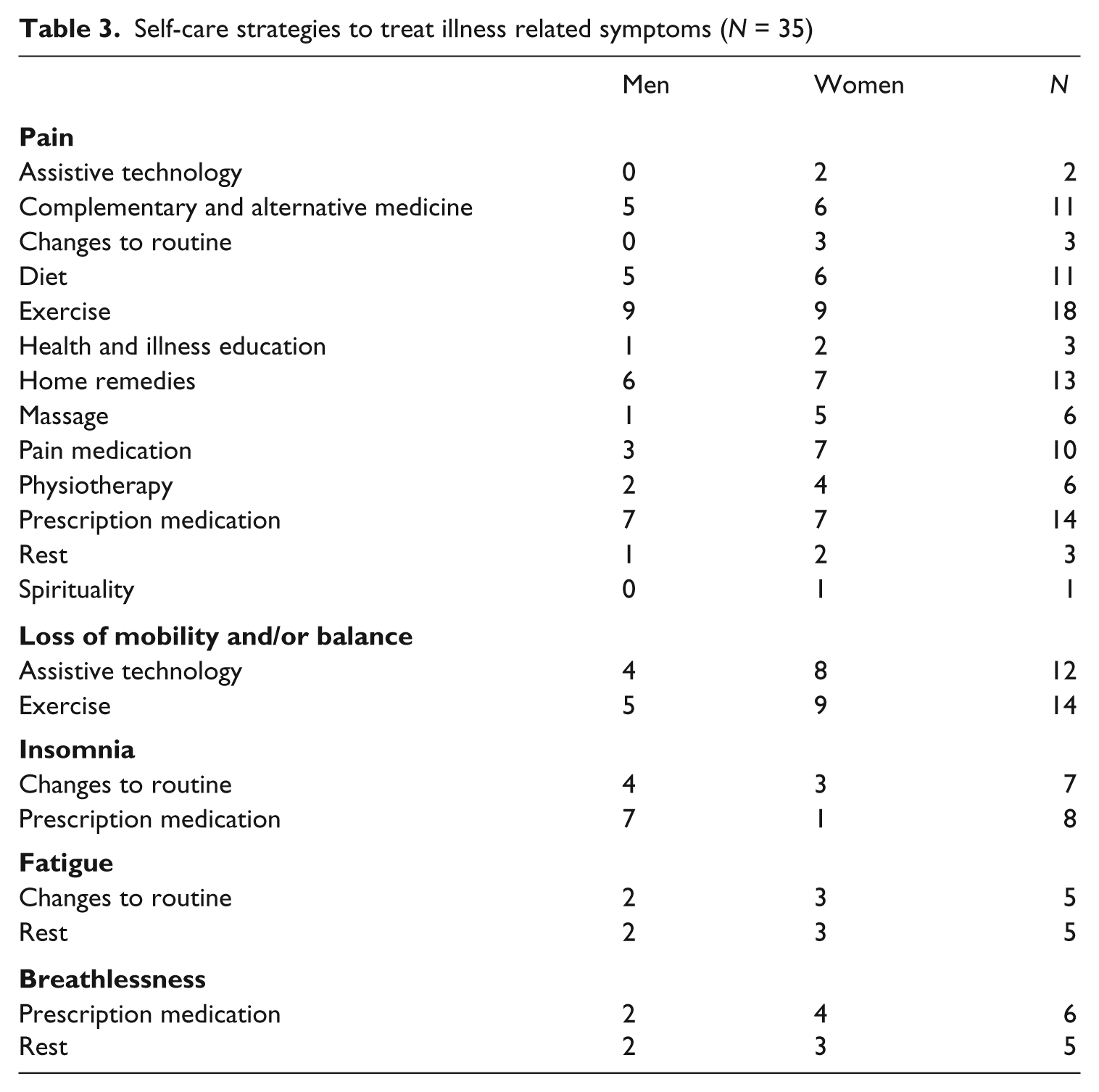
As we have reported elsewhere (Hurd Clarke and Bennett, in press), the majority of our participants were experiencing profound physical suffering, frailty, and loss of functional mobility as a result of their multiple morbidities. Consequently, all of the men and women we spoke with revealed that they were engaging in some form of reactive self-care (Ziguras, 2009), as each person utilized a minimum of two self-care practices and a maximum of 11 (average of six) (see Table 2). While the men used between two and eight (average of five) self-care practices, the women employed between four and 11 (average of seven) health strategies. Our participants framed their reactive self-care efforts primarily as a way to manage symptoms such as pain (13 men and 18 women), loss of mobility and/or balance (nine men and 14 women), insomnia (10 men and four women), fatigue (six men and seven women), and breathlessness (three men and five women) (see Table 3). The most commonly employed health strategies were prescription medication, alterations to diet, exercise, and social support.
Self-care practices (N = 35)
Notes:
Complementary and alternative medicine included: chiropractic (four men and five women), acupuncture (four women), chelation (one woman), and naturopathy (one woman)
Assistive technology included: canes (eight women) and walkers (one man and eight women)
Home remedies included: heat, hot wax and/or ice (two men and four women), support socks for circulation (two men), urinary incontinence products (one man and one woman), medical alert device (one woman), board under mattress (one woman), tensor band (one man)
Spirituality included: attending Christian church services (two men and eight women), participating in various church-run groups such as Bible studies (one man and six women), and engaging in personal prayer (one man and four women)
Supplements included: alkaline water (one woman), Traditional Chinese medicine (one man), iron supplements (two men), vitamins and minerals such as bark extract, calcium, vitamin B12, vitamin C, vitamin D (four men and five women), and suppositories (one woman)
Self-care strategies to treat illness related symptoms (N = 35)
Four men had relatively simple self-care plans comprised of one to three health practices. For example, an 80-year-old man who had arthritis, back problems, a bowel disorder, cancer, heart disease, mental illness, and urinary incontinence summarized the strategies he employed to manage his chronic conditions and the accompanying physical symptoms he experienced in this way: ‘I do a 20 minute exercise every morning for [the pain] in my knees and my arms … and you have to keep walking’. In contrast, the majority of our participants were engaged in complex systems of self-care designed to address and ameliorate a myriad of physical concerns. For example, a 73-year-old woman who had arthritis, heart disease, kidney disease, polymyalgia, and stomach ulcers, was using a total of five strategies in a variety of ways to treat pain in her back, neck, legs, and hands, loss of mobility, and insomnia. Specifically, she had made changes to her routines, educated herself about her various illnesses, begun to take four prescribed medications, employed various non-prescription drugs, and tried a number of home remedies. With regards to her efforts designed to address the arthritic pain in her hands, she described doing the following: I take Tylenol for arthritis … in my fingers … but I don’t like to take too many. I take enough pills. I don’t want to have [prescription] painkillers for it … I’m going to pick up the paraffin wax today and put the paraffin wax on my hands … You just melt the wax … and brush it on and leave it for about an hour, peel it off and put it back in the pot again … I also have one of those long narrow magic bags and I heat it up and hold onto it and that helps.
She went on to describe many other similar regimens for pain in other parts of her body as well as to treat her other physical concerns. Likewise, a 79-year-old man who had back problems, a bowel disorder, diabetes, glaucoma, heart disease, and hemorrhoids used four strategies for managing his various health issues. In particular, he described the importance of diet, exercise, prescription medications, and supplements to his self-care efforts:
I’m very careful about my eating … because I also have a touch of diabetes … I still everyday do bends and I do push-ups … I put on about eight pounds this winter and I’m working at getting it off … I’m trying to play tennis and I do a lot of walking … I did go to the gym last January for a while and I got myself a personal trainer for just one lesson. But I found that I don’t work well in a gym because you’re always waiting to get a machine. So I have a [treadmill] that I use at home … I am going to start going over to the gym and work on the machines to get me bending down here because I’m tight in the back … I take digitalis, aspirin, warfarin, and five grams of morphine every day and three times a week I take another two and a half grams … and now my iron pills.
In this way, most of our participants vigilantly monitored their symptoms and had utilized extensive and time-consuming self-care plans.
Only eight of our participants had extended health care insurance plans and, therefore, the majority of the men and women had to pay the full costs of their various self-care strategies, where applicable. Nevertheless, and perhaps as a result of their relative affluence, the majority of the men and women we interviewed did not report that the costs associated with self-care were a deterrent. Only two women indicated that their self-care choices had been curtailed by a lack of finances and extended health care insurance. An 81-year-old woman who had had back problems, a bowel disorder, cancer, cataracts/glaucoma, chemical sensitivities, chronic obstructive pulmonary disorder, depression, fibromyalgia, osteoarthritis, osteoporosis, and post-polio syndrome had stopped using acupuncture, massage, and physiotherapy when they became financially out of reach: [My] muscles were already tightening because of the post-polio [and fibromyalgia]. So there was absolutely no way in the world I could even let those muscles relax … I went to have some acupuncture to see if I could release some of the pain and get some feeling back into my fingers … I tried massage and physiotherapy of course but I ran out of money.
Similarly, a 76-year-old woman who had arthritis, back problems, colon cancer, cataracts/glaucoma, heart disease, urinary incontinence, and who had had a hip replacement was about to terminate her use of chiropractic treatments for financial reasons, a situation she regretted: ‘I can’t really afford chiro. It’s so expensive … but it helped a lot … It’s too bad it’s not covered [by health care] … it’s difficult accessing some of the medical things’.
‘The doctor can only do so much; the rest is up to you’: self-care in response to the limits of physician directed care
As well as using self-care to treat a broad spectrum of physical symptoms and functional losses, many of the participants indicated that they were engaged in reactive self-care (Ziguras, 2009) because they had reached the limits of the treatment options available from their physicians. Indeed, 15 individuals (six men and nine women), who were particularly frail and had complicated health issues, made comments similar to those of an 87-year-old woman who had Crohn’s disease, effects of stroke, heart disease, Type II diabetes, and urinary incontinence, and who stated: ‘My doctor has done all he can’. Consequently, she had turned to exercise as a means of dealing with her loss of balance and mobility, made changes to her routines to manage her pain, and altered her diet to try and control her incontinence and diabetes as well as to limit the pain associated with having Crohn’s disease. Having seen numerous physicians and specialists, these participants were either fatalistic about or resigned to their prognoses and the inability of medicine to further reduce the impact and severity of their symptoms, let alone cure their various chronic conditions. A 75-year-old man who had arthritis, back problems, chronic fatigue syndrome, heart disease, and sleep apnea put it simply: ‘I’ve been to so many different doctors – and there’s really nothing that can be done’. For him, the use of rest, supplements, assistive devices, chiropractic, physiotherapy, and prescription medicines were all that was left in terms of available, meaningful options for managing the physical realities of his numerous illnesses.
Indeed, our participants often indicated that they no longer sought out extensive medical care, preferring to manage their illnesses at home and on their own. An 86-year-old woman who had back problems, effects of stroke, heart disease, osteoarthritis, and short-term memory loss described how she had carefully changed her routine, begun to use exercises designed to improve her mobility, tried acupuncture, massage and prescription medication for pain management, and utilized various assistive devices as a result of unrelenting fatigue and declining functional mobility. Although she had a complex and comprehensive self-care plan, she was reluctant to seek out additional physician directed care for her chronic conditions for the following reasons: There’s no need for me to see my doctor. There’s nothing she can do – unless I broke my leg or something stupid like that … so I haven’t seen my doctor for over a year. Mind you I don’t really want to. There’s nothing that she can do. My spine is extremely painful but there’s nothing they can do with that … I just have to sit it out … If my doctor calls me and says ‘I want to see you,’ I’ll say to her, ‘Is there anything else you can suggest?’ And if there are, then I will go and see her. I don’t want to be foolish about it, but I mean if she can prescribe something new that’s come on the market that would be better regarding pain, I would certainly go for that. But I’m not going to get cured of anything.
Although 15 of our participants (six men and nine women) were resigned to their health problems and considered self-care to be a means of mitigating symptoms once the limits of medicine had been reached, they also viewed their various health promotion strategies as a means of staving off further cognitive and physical declines. A 78-year-old woman who had Crohn’s disease, diabetes, heart disease, and osteoporosis indicated that she had changed her routine, regularly used supplements and prescription medication, monitored her diet, and engaged in exercise because of an underlying concern about becoming physically dependent or mentally incompetent: I don’t want to end up in a nursing home. I’ve looked after people you know, and it’s really sad. I don’t want to end up like that. I don’t want to get Alzheimer’s [disease] so I keep my mind active. I’m trying to do everything so that I stay healthy.
Similarly, a 79-year-old man who had back problems, a bowel disorder, diabetes, glaucoma, hemorrhoids, and heart disease explained his reason for exercising, carefully monitoring his diet, and taking prescription medication: ‘I want my body to last as long as I’m here. I’d like it to last so that I don’t have to be creeping around on the floor on my hands and knees’.
‘You control your health’: self-care as a moral imperative
Many of our participants argued that both reactive and proactive self-care (Ziguras, 2009) were an individual’s moral responsibility. For example, 18 individuals (eight men and 10 women) maintained that good health was invariably the result of the personal effort and self-discipline in which individuals were obliged to engage. Comments such as ‘you have to be proactive’, ‘you have to be responsible for yourself’, and ‘your health is up to you’ were relatively commonplace during our conversations with the participants. A 76-year-old man who had arthritis, back problems, bowel disorder, heart disease, and osteopenia considered self-care to be ‘the discipline of trying to make sure that you do the things that are necessary to keep yourself healthy and active’. For him, this entailed the use of chiropractic, exercise, physiotherapy, and prescription medications. Similarly, a 76-year-old woman who had arthritis, back problems, cataracts/glaucoma, colon cancer, heart disease, high blood pressure, and urinary incontinence contended the following: ‘You’ve only got yourself and you have to self-discipline yourself. “Yes, I must have three meals a day. Yes, I have to have salad every day and I have to have my oatmeal” … You’re your own policeman’. In addition to advocating a healthy diet, this woman utilized assistive devices, exercise, and prescription medications.
Although the men and women both emphasized that self-care was a moral responsibility, they spoke about the perceived obligation to engage in various health practices in distinctly gendered ways. For example, half of the men stressed the importance of maintaining control over their lifestyles and their bodies in order to promote health and retain their quality of life. Privileging self-discipline and self-reliance in the face of adversity, the men made comments similar to those of a 79-year-old man who had arthritis, back problems, a bowel disorder, Dupuytren’s syndrome, prostate cancer, and urinary incontinence: I try to keep my life under control … I’m health conscious – always doing one sport or another and mostly having a good diet … if you use your head and try to manage [your health problems] the best possible way, then your quality of life doesn’t have to deteriorate as much as if you didn’t … You cannot let your health problems take over your life. You have to stay in charge. You have to be in control.
In contrast, half of the women stated that they had a moral responsibility to engage in self-care in order to stay as healthy, and therefore independent, as possible and refrain from becoming a burden on their friends and family members. These women described how important it was to their sense of self to not become ‘a bother to anyone’ or ‘put [their health problems] on other people’s shoulders’ as they endorsed feminine norms of altruism and sensitivity to the needs of others. An 81-year-old woman who had back problems, a bowel disorder, cancer, cataracts/glaucoma, chemical sensitivities, chronic obstructive pulmonary disorder, depression, fibromyalgia, osteoarthritis, osteoporosis, and post-polio syndrome asserted: When you have a chronic condition … it’s wonderful to have a neighbor who is close by that you know is more than willing to help. But you know in your heart that they’re not going to stay your good neighbor and good friend if you’re after them every day to do something for you. So you want to be as independent as possible. You want to ask for favors as little as you can … One of the hardest things about being disabled is that you can’t do as much for other people as you’ve always done. You know you become dependent on other people instead of helping other people and it’s an awful hard blow to take.
Someone who had prided herself on her ability to care for others and volunteer in the community, this woman’s growing dependence on others was a profound source of dismay and personal loss.
At the same time, many of our participants frequently judged themselves according to extant health promotion standards and accepted wisdom about healthy living, thereby finding themselves morally wanting or praiseworthy. For example, one-third of our participants (six men and seven women) articulated the sense that their self-care efforts were insufficient and expressed feelings of inadequacy and guilt over their failure to properly discipline their bodies. A 78-year-old woman who had arthritis, asthma, back problems, glaucoma, migraine headaches, and a neurological disorder relayed the following: I need to do more exercise … I’m not doing the exercise I should do … There are people who I know that I could walk with but I haven’t initiated that yet. So that remains to be done. That’s sort of top of my list for personal reform – exercise.
In this way, these participants were well versed in what they should be doing differently so as to achieve a moral sense of self and frequently admitted to the various ways that they did not measure up to accepted standards for healthy living.
In contrast, 10 participants (five men and five women) expressed satisfaction with their self-care efforts and articulated the sense that they were fulfilling their moral obligations by limiting their health risks and subscribing to healthy living ideals. An 87-year-old woman who had Crohn’s disease, effects of stroke, heart disease, Type II diabetes, and urinary incontinence contended: I feel I’m doing all I can for my health. I’m not doing things like smoking or something you know very well is bad for you … I have a swim each day … I have a routine in the morning and if I stick to the same diet … my body functions the way it should … I go to my doctor every month … I keep tabs on my health and all my tests … I have to take care of myself. My health is foremost.
Comparing themselves to those they considered less ‘disciplined’ and, therefore, less healthy than themselves, these participants argued that they were, as one 76-year-old man who had arthritis, back problems, a bowel disorder, heart disease, and osteopenia, put it, ‘probably in as good health if not better than most’ of his peers and younger counterparts. Similarly, a 75-year-old woman who had arthritis, back problems, bursitis, fibromyalgia, lupus, osteoporosis, and Tourette’s syndrome stated: I’m better off than some others and I think part of that is due to the fact that I try to take care of myself. I try to eat as healthy as I can … And I don’t sit around and mope about it. You know? I don’t let my health control me.
Whereas most of the participants emphasized that one could and should control their health, a smaller number (six men and six women) articulated the sense that they had little control over their health, particularly given their advanced ages. For example, a 76-year-old man who had asthma, back problems, effects of stroke, and heart disease contended: It’s just age. I’m getting rusty … As people age, you lose some of your acuity. It’s the aging process. Nothing is forever … there will be a beginning and there will be an end … You know there are stars in the sky. They’re born and they’re luminous and they shine brightly and then they die.
Despite his fatalistic attitude toward his health, the above man continued to use a range of self-care strategies, primarily because he wanted to placate his daughter: ‘My daughter tells me that if I do stretching exercises that might help with my pain. So I’m trying that. And it might. But I’m not convinced’. For this man, along with seven of his counterparts (four men and three women), self-care was driven by the desire to please significant others, primarily adult children and spouses, or alleviate their worry rather than from any real conviction that these health behaviors might alter their destinies.
Discussion
In this article, we have examined self-care as a means of managing the physical realities of having multiple chronic conditions in later life. The majority of our participants had developed complex and time-consuming regimens comprised of numerous reactive and proactive self-care practices (Ziguras, 2009). On the one hand, our participants were utilizing reactive self-care to manage a myriad of physical symptoms that had arisen from their chronic conditions and because they had reached the limits of the medical treatments available from their physicians. In this way, the men’s and women’s reasons for using self-care reflected those found in studies on individuals diagnosed with HIV/AIDS and cancer (Alder, 1999; Gillett et al., 2002; Lupton, 1997; Pawluch et al., 2000; Thorne et al., 2002; Yates et al., 1993). Additionally, many of the men and women also endorsed proactive self-care (Ziguras, 2009) as they argued that they had a moral responsibility to prevent additional chronic conditions or functional losses. Thus, our participants had deeply internalized healthist norms and the assumption that they must be active consumers of health care (Bunton et al., 1995; Crawford, 1980, 2006; Galvin, 2002; Leontowitsch et al., 2010; Minkler, 1999; Ziguras, 2009) so as to demonstrate an acceptable ‘will to health’ (Higgs et al., 2009: 687).
That said, some of our participants contended that there was a limit to what they could reasonably hope to achieve through self-care given their advanced ages. Resisting the stigmatization (Higgs et al., 2009; Minkler, 1999; Minkler and Fadem, 2002) associated with the failure to age successfully (Rowe and Kahn, 1987, 1997) and consistent with Higgs and Rees Jones’ (2009) concept of the arc of acquiescence, these individuals were pragmatic about and accepting of their health realities and futures. However, rather than withdrawing from body investments and despite their lack of conviction about the efficacy of various health practices, the men and women continued to utilize self-care primarily to placate significant others. In this context, self-care was a means of attending to the needs of loved ones or of avoiding potential criticisms regarding socially unacceptable capitulation to poor health, if not one’s inevitable demise.
At the same time, our participants spoke of self-care as a moral imperative in distinctly gendered ways. Similar to the research by Corbin and Strauss (1985), Leach and Shoenberg (2008), and Lindsay (2009), both the men and the women described self-care as a vital means of disciplining their unruly, aging bodies. However, the men’s descriptions of the importance of self-care and their emphasis on the need for control reflected masculine ideals of invulnerability and physical power and prowess (Prentice and Carranza, 2002). Like the existing research (Eisenberg et al., 1998; Grzywacz et al., 2011; MacLennan et al., 2002), the women in our study were employing more self-care than the men. As well as perhaps reflecting their greater responsiveness to illness (Verbrugge, 1985), the women’s use of self-care was often driven by a strong desire to limit the burden they placed on others. Specifically, the women hoped to retain their independence as well as their ability to care for others. Thus, the women were striving to achieve and retain feminine ideals of nurturance and sensitivity to the needs of others (Prentice and Carranza, 2002) through their engagement in various health practices. In this way, for both the men and the women, and like the findings of Roberto et al. (2005), the use of self-care enabled our participants to retain a positive, gendered, and moral sense of self.
A potential limitation for this study is its sample size and sampling techniques as well as the fact we did not ask about barriers to and facilitators of self-care. Thus, our ability to reflect on the relationship between socio-economic status and self-care is profoundly limited. Additionally, we did not query our participants about the sources of messages concerning the obligation to engage in self-care. Finally, although the participants had diverse ages, incomes and levels of education, none identified as homosexual and the majority of the men and women we spoke with were of European descent.
Future research should draw on a more diverse sample of frail, elderly individuals about their experiences of self-care and should delve more fully into the factors that promote and delimit older adults’ ability to engage in reactive and proactive self-care. It would also be beneficial to analyze the self-care practices and motivations of rural older adults who lack the same levels of formal health care resources that are available to urban dwelling individuals. Furthermore, it would be very useful to investigate the impact of the media and frail older adults’ interactions with health care professionals on understandings of and engagement in self-care in later life.
Conclusions
The findings from this study suggest that frail older adults are active consumers of health care as a result of the limits of medicine, the internalization of the responsibility of the individual for health, and gendered ideals and behaviors. Given population aging, the increasing prevalence of chronic conditions, and the emphasis on demonstrating one’s morality through healthy lifestyles and body investments, reactive and proactive self-care will become ever more important, if not expected, in later life. Affording individuals an important and socially sanctioned means of mitigating aspersions of their character as a result of their loss of health and increasing dependence, self-care in later life fosters the creation of an agentic, moral, and gendered self.