
Abstract
The harm reduction policy of Taiwan has been considered a success. However, the HIV incidence among injection drug users declined before the nationwide needle and syringe program and drug substitution treatments were implemented. Thus, other factors in the policy might have contributed to its success. Some authors have suggested that education may have played a pivotal part. In this research, the purported significance of education in the success of the policy is conceptualized by reviewing the studies on harm reduction in Taiwan and reflecting upon my own fieldwork. Moreover, relevant literature is used as reference to reformulate this notion of education. This article shows that harm reduction education may be conducted in numerous forms, most of which are non-formal, improvisational, and contingent. Non-governmental organizations may play a role, but more actors, strategies, infrastructures, and interactions should be considered. This article draws from actor-network theory and refines the current thesis that attributes the policy success to education by utilizing three reflections, namely, appreciating materiality and spatiality, recognizing covert actors in the networking, and treating education as an outcome rather than a means. In conclusion, looking at education as a form of networking offers theoretical insight that increases understanding of its participants, mechanisms, processes, and permutations.
According to the definition given by Rhodes and Hedrich (2010), harm reduction “encompasses the interventions, programmes, and policies that seek to reduce the health, social and economic harms of drug use to individuals, communities and societies” (p. 19). A common target of harm reduction programs is HIV/AIDS. Among existing harm reduction programs, there is sufficient evidence that supports the efficacy of opioid substitution treatments (OSTs) in reducing HIV transmission, but the evidence for the efficacy of needle and syringe programs (NSPs) is more tentative (Kimber et al., 2010). On the other hand, World Health Organization (WHO) and United Nations Educational, Scientific, and Cultural Organization (UNESCO) advocate the combination of information, education, and communication (IEC) as an important way of fighting HIV/AIDS by promulgating appropriate knowledge and promoting desirable behavioral changes (UNESCO, 2001; WHO, 2000). In a systematic review of past literature, Aggleton et al. (2005) find that the combination of IEC and service provision may achieve much more positive and sustainable outcomes than IEC alone. However, it is still unclear how programs that offer education could coordinate with programs that distribute medications and paraphernalia to optimize their intended effects. Both well-designed empirical studies and adequate theoretical frameworks are needed to assess the intricacies of the combination.
Generally, the harm reduction policy of Taiwan has been considered a success (Taiwan Centers for Disease Control (TCDC), 2009). Lyu et al. (2011) speculated in Lancet that the policy success can be mainly attributed to the effects of education. By education, the authors referred to the efforts of non-governmental organizations (NGOs), particularly those of Taiwan’s Society of Preventive Medicine’s Living with Hope Organization in preventing the sharing of needles and solutions among drug users. Owing to the hard work, the likelihood of transmitting HIV and other blood-borne diseases was diminished.
Although practitioners and researchers may disagree on the idea that education is the most significant factor of policy success, nobody has denied its importance. However, the meaning of education has remained elusive, specific to this case. Thus, this research contends that the idea of health education as the key to a successful policy warrants more scrutiny and elaboration. Actor-network theory (ANT), which originated in science and technology studies, is helpful in this respect. The theory was formulated to explain how a finding or an object becomes a truth or reality without resorting to either narrow scientific realism or naïve social constructionism. In other words, ANT does not interpret a scientific truth as “the way it naturally is” or “the way society makes it so.” Instead, the theory traces the networks that undergird the truth and object in the making by following the scientists and other people involved, and examines the processes through which different actors, human and non-human alike, are enrolled and assembled, eventually forming an alliance that sustains the truth (Latour, 1987, 1988). Thus, formation of a scientific truth is at the same time formation of a new social configuration. In other words, what is social and what is scientific constitute each other (Latour, 1993). The longer and stronger a network is, the more credible the finding becomes (Latour, 1988). The idea of network entails an image of an expanding web that is informative, performative, and transformative. Therefore, the authenticity and materiality of truth are relational and indeterminate (Law, 1999), a finding which has been appropriated by the literature on drug use (Vitellone, 2013). This theory is considerably connected with Latour (2005) and Callon (1986), but Law (1999), Mol (2002), and many others have contributed to its current formulations and permutations. The theory has been widely elaborated in social studies of biomedicine ranging from Prout’s (1996) study on metered dose inhalers to Dwyer and Moore’s (2013) research on methamphetamine. Delineating the contour of this theory is beyond the scope of this article. Considering the capacity of ANT to address the work of translation and the non-human actors involved in the networking, which results in the partial existence of scientific truth and objects (Latour, 2005), it has been employed in explaining the process through which education takes form as knowledge practice (Fenwick and Edwards, 2010). Following the path of ANT that extends to education studies, the article puts forward the question, “What can ANT tell us about health education in harm reduction programs?”
This article serves both theoretical and practical purposes by pondering over the education factor in the harm reduction policy of Taiwan through the lens of ANT. The article briefly introduces the policy and presents an overview of the explanations proposed for the decline-before-policy phenomenon. Subsequently, the article juxtaposes existing studies related to health education with my own empirical research. With the inspiration from ANT, the article intends to refine and enrich the current thesis that attributes the policy success to education. Three major findings and reflections are used, namely, appreciating materiality and spatiality, recognizing covert actors, and treating education as an outcome rather than a means.
Harm reduction policy of Taiwan
Injection drug users (IDUs) were not a major constituent of HIV infection in Taiwan until the percentage of IDUs increased drastically from less than 10 percent in 2003 to almost 40 percent in 2004 and 70 percent in 2005 (Yang et al., 2008). This emergent epidemic aroused the concerns of TCDC, which turned to view IDUs as its main policy target. Prior to this epidemic, TCDC mainly dealt with men having sex with men (MSM) and other at-risk groups, including sex workers. Illegal drug users have been defined by law as sick criminals since the Narcotics Hazard Prevention Act of Taiwan was revised in 1998. Owing to the redefinition, drug users became the concern of the legal and medical systems. Specifically, drug users were placed under the supervision of the Ministry of Justice and the Department of Health. In addition, the National Bureau of Controlled Drugs supervised the licensing and regulation of addictive substances, including a wide variety of opiates. 1
From the outset, the need was identified for new strategies and ties of cooperation within the central government. This was particularly true for TCDC, the body tasked to supervise the control of epidemics, such as HIV/AIDS. Under the emergent situation, reductions in supply and demand in the past decades were rendered insufficient. Therefore, TCDC introduced the concept of harm reduction, which led to the implementation of a pilot program that included an NSP offered by cooperative pharmacies and hospitals, an OST that applied methadone in most sites, and an expanded screening and counseling service program (Chen, 2009). The pilot program was implemented in four administrative regions, namely, Taipei City, Taipei County (now New Taipei City), Taoyuan County, and Tainan County. The major milestones of the policy from 2004 to 2008 are listed in Table 1, and the favorable outcome of the pilot program has been reported by Yang et al. (2008). With the initial success in controlling the spread of HIV, the pilot program became a nationwide policy in the following year. The policy effectively controlled the transmission of HIV among IDUs in less than 5 years (Figure 1). The MSM group became the largest at-risk population again in 2008. Public and administrative attention on harm reduction slowly ebbed in 2009. NSP, OST, and screening services subsequently became routinized medical and public health practice.
Milestones of Taiwan’s harm reduction policy, 2004–2008.
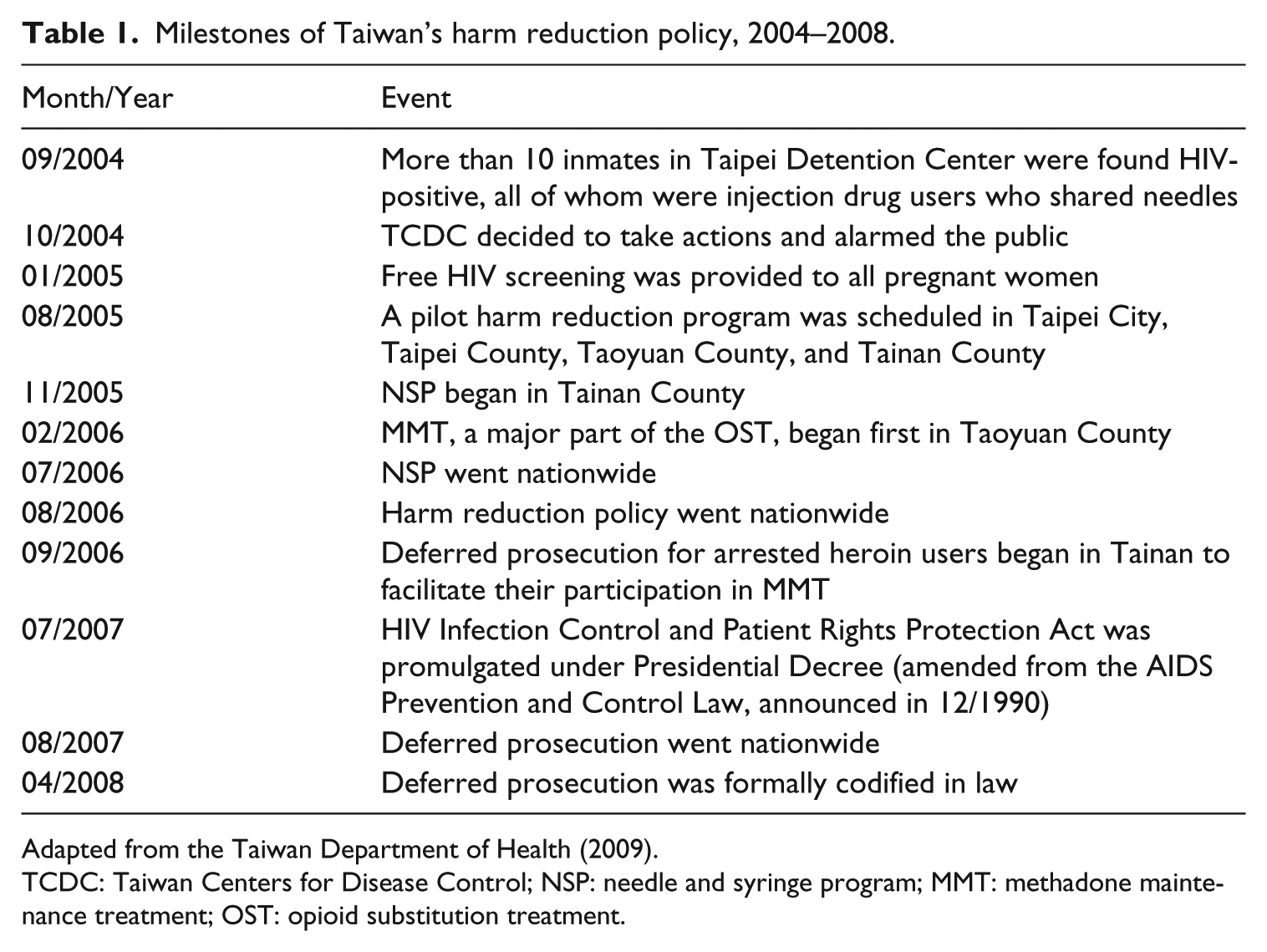
Adapted from the Taiwan Department of Health (2009).
TCDC: Taiwan Centers for Disease Control; NSP: needle and syringe program; MMT: methadone maintenance treatment; OST: opioid substitution treatment.
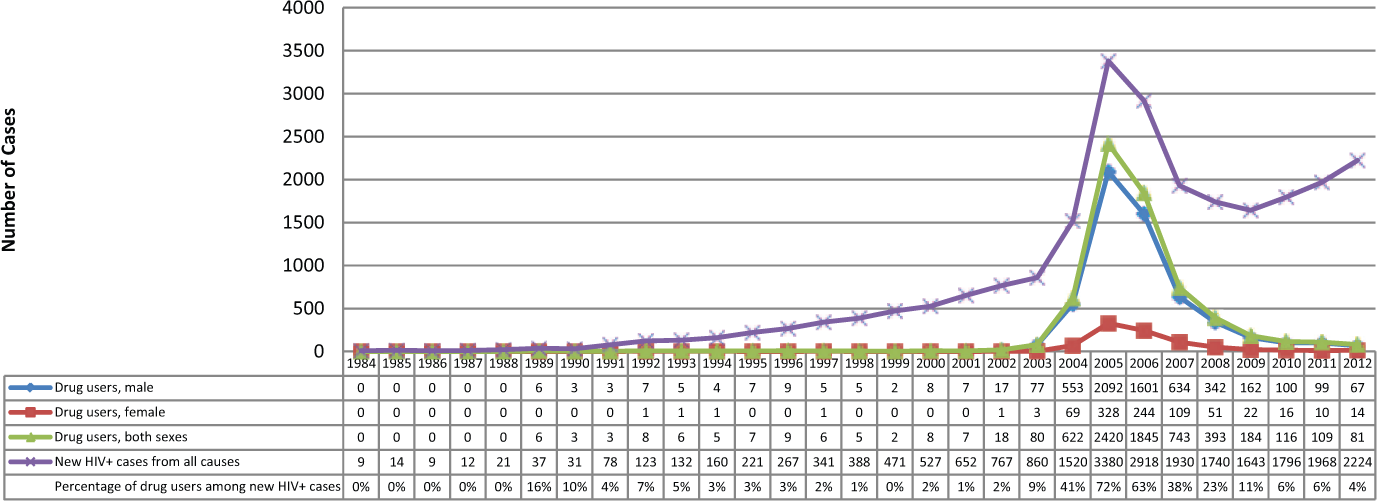
Annual HIV incidence among injection drug users.
Education and the decline-before-policy phenomenon
The harm reduction policy of Taiwan was deemed successful. However, the monthly HIV incidence rate among IDUs was determined to have actually declined before the pilot NSP and OST were implemented in August 2005 (Chen, 2011a; Lyu et al., 2011). Thus, other factors outside of the policy that could have contributed to the success in terms of HIV control were analyzed. Lyu et al. (2011) argued that education by NGOs may be the major factor for the success. By contrast, Lee et al. (2012) suggested that the mandatory screening program that took effect in April 2004 for the violators of drug laws partly accounts for the surge of HIV incidence before the onset of the pilot program. One of my earlier articles summarized three possible explanations for this phenomenon: effects of pre-policy screening, saturation of HIV infection among IDUs, and, most emphatically, disciplinary measures for citizen addicts (Chen, 2011a).
Conceived broadly, education and its accompanying disciplinary measures may account for the sustained effects of harm reduction among IDUs. In Taiwan, health education on HIV/AIDS and drugs is offered through formal and non-formal venues, based on the definition of UNESCO (1997). Formal education, which is conducted in classrooms or other educational institutions, usually has well-organized curricula supervised by the Ministry of Education. In terms of drug education, the implementation of the Chunhuei (春暉, or Spring Sunshine) project is ongoing and a special program called Zizhuihua (紫錐花, or Enchinacea) Campaign characterized by the just-say-no slogan has been introduced. These initiatives aim to reduce demand, rather than harm. Nevertheless, school education was deemed unlikely as the major factor because most confirmed IDUs in Taiwan are not students.
Thus, the effects of health promotion could have occurred through non-formal education, the aim of which is more of intervention than prevention. Non-formal education is defined by UNESCO (1997) as “educational programmes to impart adult literacy, basic education for out-of-school children, life-skills, work-skills, and general culture” (p. 47). Understandably, non-formal education is a diverse field that includes peer education, anti-AIDS clubs, drama, art, youth dialogues, music, and comic books, wherein NGOs play a major role (Morisky et al., 2009). For example, Taiwan AIDS Foundation organized peer educator groups Aixianbang (愛現幫), an abbreviated Chinese phrase which means “people with HIV/AIDS as health educators.”
Education in the context of health promotion is defined conveniently as “a broad and varied set of strategies to influence both individuals and their social environments, to improve health behavior, and to enhance health and quality of life” (Glanz et al., 2002: 10, author’s emphasis). This definition covers a wide variety of existing models. The common presupposition is that health education is a means to an end, an instrument of passing relevant knowledge to targeted populations to achieve desirable changes in a given social setting. However, as I will illustrate below, this definition relies on a predetermined and generally static relationship of targeted groups (society) and educational messages (knowledge), which is the dichotomy that ANT aims to unsettle. From the ANT perspective, this definition of health education fails to appreciate the performativity of delivered knowledge vis-à-vis the targeted subjects, and it lacks focus on the reciprocal and co-constitutive relationship of society and knowledge. Furthermore, based on the present definition of education, it is manifested only when its effects are recognized. In ANT, the authenticity and authority of a fact or idea only come after the network has become longer, wider, and stronger.
The integration of ANT and education research has been done before. Fenwick and Edwards (2010) have offered a brilliant and useful work that introduced ANT into education studies; they claimed that the inclusion of non-human actors and the emphasis on translation and networks of ANT are the major analytic advantages of the theory. Notably, terms such as network may have been used in traditional health education models, but the network in ANT is different from social network. In the latter, network is “the web of social relationships that surround individuals” (Heaney and Israel, 2002: 185). However, network in ANT refers to “an assemblage of materials brought together and linked through processes of translation that perform a particular function” (Fenwick and Edwards, 2010: 12). In other words, the “social” in social network is a pre-given property with a stable ontological status, whereas the social in actor-network is earned through the stabilization of networking.
How ANT enriches the understanding of education
This article does not intend to prioritize any explanation for this decline-before-policy phenomenon. Rather, it aims to refine the idea of education based on the qualitative research I conducted during the peak of harm reduction initiatives in Taiwan, that is, from 2004 to 2009 (Chen, 2009). Using archives, in-depth interviews, and field observation to explore the policy process, the research examined how individuals and governmental units interacted and assembled to contribute to the design and implementation of harm reduction. This assemblage was characterized by heterogeneity and detachability of its components, one of which was NGOs (Chen, 2011b). My research shed light on how harm reduction messages such as protected sex and avoidance of sharing needles and solutions were packaged and forwarded to IDUs as policy targets. This article attempts to weave a wide array of studies on harm reduction in Taiwan with my empirical data to better illustrate how this ANT perspective can enrich our understanding of health education on harm reduction.
Spatiality and materiality
A major feature of ANT is the methodological symmetry in treating human and non-human actors, a symmetry that is particularly important to harm reduction education. Human actors, including governmental and NGO workers, are vital to promulgating health messages, such as the importance of protected sex and the undesirability of sharing needles and solutions. However, non-human actors are undoubtedly indispensable. For example, governmental authorities have purchased syringes of the wrong size and needles of the wrong caliber in the early phase of policy implementation. These syringes and needles were not the ones used by IDUs. Thus, they were discarded right away when distributed among IDUs. The ignorance of the personnel in charge became a target of ridicule.
While Lee et al. (2012) suggested factors other than the NGO-offered education, their quantitative study confirmed the importance of health education. They investigated the role of HIV testing and education by comparing the statistics between the areas that participated in the pilot program and those that did not. They found that educational materials, condoms, dilution water, and alcohol sponges/swabs are protective factors. However, they failed to address how these items function as such. For example, they failed to notice that the diverse packaging of these items make a difference. One of my respondents ridiculed the huge, cumbersome envelopes that other localities used to distribute educational items as follows: “They [IDUs] were scared to death! They said, ‘how could we possibly take it [the envelope]?’ It was so difficult to bring it home, so they simply throw away the stuff.”
Education consists of verbal and non-verbal approaches. Nonverbal approaches are often expressed through actions, settings, and, most commonly, the ways things are presented. Bourgois (2000) demonstrated how methadone dosage sends a message to desperate drug users on how they were supposed to behave. The inadequate dosage given by methadone clinics evidenced a number of presuppositions about the punitive attitude of treatment. In the process of struggling, drug users were ruthlessly triaged, disciplined, and excluded from decision making. The arrangement of treatment revealed the texture of power in the network of education that extended from the clinic to the users. In my case, the opinions of the respondents who noticed the inadequacy of huge packages led to the revision of presenting the educational materials to IDUs. These materials were re-packaged in a smaller box and sold in vending machines because health authorities believed that this could prevent curious kids from obtaining these materials for unintended purposes (Figure 2).

The content of a care package: three syringes with needles, condoms, alcohol wipes, educational materials, and normal saline. Note that care packages can contain different items in different places. Photograph by the author.
As previously stated, harm reduction education takes place outside of classrooms, that is, in hospitals, prisons, or counseling rooms, where NGO workers offer individual assistance or group discussions. People learn differently in different places and thus space matters. Minimal literature on harm reduction in Taiwan has touched on the spatiality of education. Research has shown that HIV education in prison, even a 1-hour lecture that offers skill building and prevention messages, may improve the knowledge of inmates on AIDS as well as their self-efficacy to reduce risky behavior and increase readiness to change. However, the improvement does not necessarily translate into the minimization of risk of drug use among inmates (Ko et al., 2009). In reality, the effects of education, if any, are sketchy because the prison is always underfunded and understaffed in Taiwan. Based on my empirical observation, I put forward the idea that hospitals are not a good source of education, either, although some of my respondents believe that hospitals can be a good platform for education because they integrate methadone provision with health educational messages. However, even if hospitals were a good platform for education, the key factor might not be the medical staff. An investigative study (Taoyuan Psychiatric Center, 2008) that interviewed 85 OST workers (i.e. psychiatrists and nurses) reveals the ambivalence of service providers. These OST workers agreed on the significance of providing methadone to heroin injectors based on the principle of harm reduction, but their concerns about staff safety or possible violence often took precedence over the need for adequate education. This ambivalence was best revealed by the spatial arrangement of OST clinics. These clinics were usually far away from the main hospital building, aptly reflecting the moral and social distance between ordinary patients and criminals-turned-patients. There was one time when I observed the place providing OST in a psychiatric hospital, and I found it was in fact a shabby container house by the main gate. Thus, the intention and ability of the clinic to deliver adequate education was dubious.
The situatedness of education gains more evidence in the research of Tsai et al. (2010). They collected questionnaires from 414 NSP providers, who were divided into community-based respondents (mostly community pharmacists) and clinic-based respondents (mostly medical personnel in hospitals). Results show that the community group is more actively involved in introducing equipment provision and health education services than the clinical group, although the latter appeared more knowledgeable about HIV/AIDS and blood-borne infections and focused on medically oriented interventions, such as screening, diagnosis, and provision of substitution treatment. The different service schemes of the two groups were explained largely by organization characteristics, professional training, and ethical considerations.
Effective education may happen in the capillaries of the periphery, not at the center. It takes form in every trivial exchange of information, probably accompanied by exchange of either clean needles or newly purchased heroin. For the sake of illustration, I offer a part of my field observation wherein the practice of an enthusiastic community pharmacist is highlighted. The practice demonstrates the central status of spatiality and materiality in harm reduction education even though these are often neglected.
Ms X delivers health information to whoever comes to her pharmacy for free needles. She treats them as if they were her relatives. However, winning the trust of drug users is very difficult during the first few encounters. The users just come in, take the needles, and leave. Distributing needles and syringes is useless, she thinks, if she could not use this to offer adequate information and education. Therefore, she placed clean needles and syringes at the end of an aisle in her pharmacy rather than by the front door, which many other pharmacists would do. This way, visiting drug users have to walk through the door and pass by the cashier. The longer walk buys her more time to say what she wants to tell them. Space translates into time, which in turn translates into opportunities for education. She even improvises so as to optimize the “take-out” of a drug user. She keeps 5–10 clean syringes with needles in the box, probably for 1–3 days’ use. Thus, when a drug user comes in and takes a “grip,” the optimal amount of needles is attained. Like an ethnographer, she learned this trick by observing these drug users coming in and out of her pharmacy.
Generally, 10–30 drug-using visitors come in every day. Most of them are young men, but the demographics gradually moved toward middle-aged men and women. “Business” is usually bad in winter because of the forthcoming Chinese New Year, when drug users hide from policemen who want to improve their arrest records for the annual reviews.
All this learning and service comes with a price. Her shop was burglarized and robbed twice in the past 2 months before my interview. The recently installed monitoring cameras attest to the lesson learned.
In this vignette, spatiality (the end-of-aisle arrangement) and materiality (the number of needles and syringes in the box) are skillfully interwoven into the message that goes beyond the health information offered by words or pamphlets. Education does not take place without appreciating spatiality and materiality; it constitutes and is constituted by this intended entanglement of spatiality and materiality. Human and non-human actors (i.e. needles, syringes, and space) coordinate and team up to strengthen and broaden the effects of education as a network.
Covert actors in networking
The previous section involves where and with what, whereas this section focuses on who and whom. In understanding education, a simple yet central question pops up: Who educates whom? This question complicates the ranges and definitions of educators and educatees. Lyu et al. (2011) attributed the success of harm reduction to the alleged effects of education, and implicitly referred to NGOs as educators and IDUs as the educatees. However, this definition is narrow. Extensive interviews in my fieldwork indicate two major findings that aptly expand the definition.
First, ANT rejects a predetermined role and prestige assigned to a certain actor. In the beginning, Pasteur did not possess the power to make farmers believe in his lab findings as the answer to their problem. Such power was attained after he enrolled more participants and witnesses through earning more allies and transposing his lab results into knowledge applicable to farms. In short, Pasteur was seen as the great scientist who saved the farmers only after a strong and stable network was established around him (Latour, 1988). A network that is changeable means the role and prestige bestowed to a certain actor are indeterminate. In the case of harm reduction education, this perspective implies the existence of more educators than we ordinarily define.
Some respondents in my fieldwork surprisingly demonstrated their efforts on education in their encounters with IDUs. A parole officer talked about his initial role in the system of deferred prosecution, in which an arrested IDU promised to attend an OST regularly for a certain period of time in exchange for withholding prosecutorial processes: “Medical staff takes a caring role, we, parole officers act as a bridge, and prosecutors exert pressure.” As time went by, he noticed the transformation of his role and stated,
In the past, we, parole officers mostly took a surveillance role, but now … they [hospital workers] inform us who is absent, and we are obliged to contact relatives to know the reasons. We are becoming more and more like social workers.
Eventually, the parole officer found himself repeatedly relaying to the IDUs under his watch information about HIV/AIDS, safety issues about drug use, and the danger of unprotected sex. Generally, parole officers are not considered a member of the group of educators, but in effect, their efforts adhere to the process of education. I call these actors covert actors in the context of education as networking, who either participate in or facilitate the conditions of education. Opposed to those who are easily identified or overt actors, covert actors warrant more analytic attention as they are not only implicated in but also actively contribute to the network. To the surprise of many people, I have identified some, if not most, prosecutors as covert actors because they contributed to the system of deferred prosecution as a force that compels drug users to receive medical treatment.
Second, from the perspective of ANT, a network is a living assemblage of interested actors forming alliances and reciprocal relationships. This ANT-inspired analytic is closer to the community-building model in health education, where health propagation is tied to the establishment or consolidation of a community in which the boundary between teaching and learning is as thin as a gossamer, if not absent.
A devoted NGO worker described her initial recognition of HIV/AIDS problems among incarcerated IDUs. She has been visiting prisoners with HIV/AIDS since the association was established in 1997. The increase of HIV-positive inmates around 2003 compelled her to ask for educational materials from the Venereal Disease Control Institution (VDCI), but no materials were available because drug use was not yet identified as a risk factor. Eventually, the director of VDCI made the educational pamphlets herself and requested the NGO worker to bring the pamphlets to incarcerated IDUs and ask for their feedback. In another case, public health workers regarded IDUs as experts and consulted them in a focus group, which helped considerably in serving the target population and facilitating policy implementation.
In these examples, who is educating whom? What we have witnessed is a case of mutually enrolling practice among overt and covert actors, who may even be the recipients of the knowledge or information. This practice fostered an acceptable way of understanding, leading to desirable behavioral changes manifested by health statistics.
Education is an outcome, not a means
When education was cited as a main contributor to the success of the harm reduction policy of Taiwan, it was implicitly presumed to be an independent variable to policy outcome, which is a dependent variable. However, education from the ANT perspective is not an independent variable. It constitutes and is constituted by the policy outcome to which it aims to contribute. In other words, education is not a means to an end (policy success in this case), but an outcome.
Let us go back to the thesis that science and society constitute each other. If education is seen as knowledge practice and policy outcome is its resultant social configuration, then the notions of co-constitution can apply to their relationship. Similar to considering the findings of Pasteur as true when other actors, such as hygienists and farmers, were enrolled and believed in his claims, education is considered useful and conducive to the desired health improvement as more policy participants are recruited, rendering the policy outcome as successful and desirable.
Education and policy are co-constituted for a purpose, such as controlling the spread of HIV/AIDS, but sometimes, these fail to achieve the intended goals. Contingencies abound. Actors may bump into unintended events that eventually lead to unfavorable outcomes. For example, public health authorities and workers have always feared that the distributed needles, once discarded randomly by reckless drug users, may infect innocent people, especially kids. My respondent in the TCDC informed me that this tragic event occurred in Australia and produced serious setback in policy implementation. Initially, the TCDC planned to print its mark on the distributed syringes to advertise a good policy such as harm reduction, but this plan was eventually called off. The respondent in TCDC said, “A mark like this will be solid evidence [that we contributed to this tragedy].” Accidents happen, and achievements are fragile.
The instability and indeterminacy inherent in the ANT framework can be explained by its conceptual kinship with assemblages, which I used in another article to address the ways that the office, a loose aggregate of policymakers, advocates, and experts, organizes and implements the harm reduction policy of Taiwan (Chen, 2011b). ANT is conceptually related to the idea of assemblages of Deleuze and Guattari (Harman, 2007; Law, 1999). However, the two concepts are often used for different, though overlapping, purposes. In terms of their emphasis on things, Harman (2007) argued that both concepts aim to revive an object-oriented philosophy. The nuanced comparison of the two concepts is beyond the scope of this article. However, suffice it to say that assemblages are often used to explain the ontological complexity of social organization (DeLanda, 2006), whereas ANT is regularly applied to explicate the emergence of scientific truth, objects, and the social therein (Latour, 2005).
Some researchers believe that assemblages imply more theoretical fluidity than ANT (Marcus and Saka, 2006), but the two concepts share a picture of heterogeneous and often detachable humans and things, contingent and fragile associations, and an unstable socio-technical aggregate maintained through collective efforts. More importantly, the two concepts do not take structure as a given condition of action, but cast the causality as the question to be addressed. In ANT, a fact is a fact because more actors are enrolled and interested in making the fact as truth. Thus, education is as dependent as the policy outcome on the collective mobilization and lurking contingency involved in networking. It is an outcome, not a means.
Conclusion: understanding education as networking
In conclusion, this article hopes to address two issues in relation to policy practice and theory reflection. On the practical side, most harm reduction practitioners and policymakers in Taiwan are satisfied with the effects of the policy on HIV control among IDUs. At present, however, they are asking about the mechanism that underlies the policy success. This question is important because it concerns why, how, and where future governmental support is to be allocated. Appropriate education certainly matters because it has been shown to work effectively through networks of people with HIV/AIDS (UNESCO, 2001), but this article replaces the idea of networks with networking to emphasize the active, constructive, and reciprocal aspects of education. This approach calls for a new theoretical framing of how education is understood in Taiwan and elsewhere. By viewing education as a form of networking, researchers may follow and appreciate sophisticated participants, mechanisms, processes, and permutations that constitute educational activities, amorphous and heterogeneous as they may seem. NGOs are definitely vital in education, but these are not everything.
On the theoretical side, ANT has not yet been adequately applied to examine educational efforts specifically involved in harm reduction, even though it has been employed in analyzing tobacco-free programs (Young et al., 2010) and educational studies in general (Fenwick and Edwards, 2010). This article has addressed three theoretical insights that can be gleaned from the ANT perspective. Hopefully, more theoretically informed research will illuminate the various aspects of harm reduction policy and elicit stimulating dialogues on the present theories on health education.
Footnotes
Acknowledgements
The author is thankful to Dr Sheng-Chang Wang from the National Health Research Institute (Taiwan) for the inspiration and assistance he provided that made this article the way it is. Great gratitude also goes to the anonymous reviewers whose comments greatly improved the article.
Funding
This writing was supported by Taiwan’s National Science Council (currently, the Ministry of Science and Technology) through Grant Number NSC 102-2410-H-010-006-MY2.