
Abstract
Health issues now evolve in a global context. Real-time global surveillance, global disease mapping and global risk management characterize what have been termed ‘global public health’. It has generated many programmes and policies, notably through the work of the World Health Organization. This globalized form of public health raises, however, some important issues left unchallenged, including its effectiveness, objectivity and legitimacy. The general objective of this article is to underline the impacts of WHO disease surveillance on the practice and theorization of global public health. By using the surveillance structure established by the World Health Organization and reinforced by the 2005 International Health Regulations as a case study, we argue that the policing of ‘circulating risks’ emerged as a dramatic paradox for global public health policy. This situation severely affects the rationale of health interventions as well as the lives of millions around the world, while travestying the meaning of health, disease and risks. To do so, we use health surveillance data collected by the WHO Disease Outbreak News System in order to map the impacts of global health surveillance on health policy rationale and theory.
Introduction
It is widely asserted that we live today in a mobile world ruled by dense flows, fluidity and mobility (Adey, 2009; Castells, 2011[1996]; Cresswell and Merriman, 2011). In what is usually characterized as globalization, almost everything from ‘goods’ to ‘bads’ are seen as being on the move. This situation has been highly significant for public health. Germs and viruses are considered as mobile threats that flout of territorial demarcations and spread all over the world (Bashford, 2006b), what some have termed ‘globalisation of disease’ (Fidler, 2004b; Lee and McKibbin, 2004; Novotny, 2007). The fear induced by this ‘globalisation of disease’ has generated a tremendous development in global health policies and programmes (Zacher, 2007), notably through the work of the World Health Organization (WHO) and the development of global health surveillance mechanisms (Baker and Fidler, 2006; Calain, 2007). This recent development in global health institutions has led to the emergence of ‘global public health’ (Brown et al., 2006) as a field of practice and theory (Baum, 2003). This article seeks to contribute to both.
However, the global health landscape and its surveillance apparatus 1 has remained largely impervious to critical scrutiny, especially regarding the mutual justification of disease surveillance and global health politics as well as the reproduction of health inequalities through global programmes and practices. The general objective of this article is consequently to critically engage with WHO’s practices and policies regarding infectious disease control by using the surveillance structure established by the WHO and reinforced by the 2005 International Health Regulations (IHR) as a case study. What are the consequences of WHO disease surveillance on the practice of global public health? How does it affect its theorization? The implementation of an epidemic and disease surveillance structure at a global scale by the WHO in the late nineties 2 (Aginam, 2003; Fidler, 2005) is well suited as a case study, as it remains largely unquestioned by scholars (Weir and Mykhalovskiy, 2010: 2) and has been recently criticized by practitioners (Carlowe, 2010; Watson, 2011).
The caricatured representation of viruses and germs crossing borders, circulating through biological and social bodies, and instantly spreading all over the world has been widely accepted and used to rationalize global public health policies (Brown and Bell, 2008; Taylor and Bettcher, 2000). Today, global public health, through the work of the WHO, represents one of the main pillars of public health interventions (Kickbusch, 2003; Weir and Mykhalovskiy, 2010). Health now evolves in a new socio-political space: the globe. Real-time global surveillance, global disease mapping and global risk management are how we currently interact with infectious diseases (Brownstein et al., 2008). Through the problematization of the recent developments in global public health policies and programmes, we argue that the changes introduced by the 2005 IHR (the elaboration of an all-risk approach, the use of unofficial sources of information; the use of information and communication technologies – more details in the next section) tailored a neo-liberal process in which the policing of ‘circulating risks’ emerges as a dramatic paradox for global public health. Rather than being the birth of a revolutionary process associated with post-Westphalianism/supra-sovereignty (Fidler, 2003, 2004a, 2005; Weir and Mykhalovskiy, 2010) or the establishment of legitimate global public health policies (Brown and Bell, 2008; Taylor and Bettcher, 2000), these changes tend to orientate health priorities without effective accountability mechanisms for WHO and other health actors involved.
In order to analyse the tensions of ‘circulating risks’ and their impacts on global health policy, this article begins with a descriptive scrutiny of the politics of global health governance and surveillance at the WHO level, followed by an empirical and quantitative analysis of the practice of global health surveillance from 1996 to 2010, using the data of the WHO Disease Outbreak News System. In a second step, through the examples of the social production of the global microbial space and the social power of contagion, we underline the controversial uses of health as grounds for power relations, adding to the theory of global public health. We conclude with an analysis of the paradoxical transition from dangerousness to risk that, we argue, characterizes contemporary global public health.
WHO and the global public health surveillance apparatus
In what is today represented as a global and fluid world, health surveillance and intelligence are seen as the best ways to control and manage disease proliferation and propagation (Brownstein et al., 2008: 1019). Global health surveillance can be defined as ‘the ongoing systematic collection, analysis, and interpretation of outcome-specific data for use in the planning, implementation, and evaluation of public health practice’ (Thacker, 2000: 1). Health surveillance is based on four types of actions: collecting, interpreting, disseminating and acting on health information (Weir and Mykhalovskiy, 2006: 242). These actions govern the main trends observed in today’s global public health.
The regulation and application of international health surveillance were originally shaped through the International Sanitary Regulations in the 19th century, renamed IHR in 1969 (Baker and Fidler, 2006). The IHR represent the main rules through which global health policies are practised. The main purpose of the IHR is to establish the objects and modalities of disease regulations beyond and between states, using surveillance as the main tool for supra-national health management (Fidler, 2005). Adopted for the first time in 1851, the IHR were amended several times (WHO, 2003: 1). The adoption of a new and highly modified version of the IHR in 2005 completed a complex and deeply political revision process initiated in 1995, which introduced major changes:
The elaboration of an all-risk approach (including human-caused epidemics, such as bioterrorism);
The use of unofficial sources of information for outbreak identification;
The support information and communication technologies for data gathering.
The main goal of this new global health structure of surveillance is identified in Article 2 of the 2005 IHR which aims ‘to prevent, protect against, control and provide a public health response to the international spread of disease [avoiding] unnecessary interference with international traffic and trade’ (WHO, 2005a: 10). It is thus essential to understand that the IHR are integrated into a neo-liberal approach 3 of the world order oriented towards the protection of specific globalization routes (and not the protection of health per se). This includes an all-risk approach, meaning that all types of health emergencies, under the concept of Public Health Emergency of International Concern (PHEIC), are under scrutiny without regard to their sources or origins 4 (Fidler and Gostin, 2006: 86). The concept of PHEIC represents, as shown by the WHO decisional instrument in Appendix 1, the cornerstone of the new IHR.
According to Article 1.1 of the 2005 IHR, public health emergency of international concern’ (PHEIC) means an extraordinary event which is determined […] (i) to constitute a public health risk to other States through the international spread of disease and (ii) to potentially require a coordinated international response. (WHO, 2005a: 9)
There are four criteria – on a question form to be answered, and called criteria algorithm – for a disease outbreak to be considered as PHEIC (see Appendix 1), and then reported to the WHO and be subject to global surveillance mechanisms, management and alert 5 (WHO, 2005a). These four questions officially account, according to the WHO, for the selection process used by the outbreak verification team based in Geneva (Dry, 2008: 12):
Is the public health impact of the event serious?
Is the event unusual or unexpected?
Is there a significant risk for international spread?
Is there a significant risk for international travel or trade restrictions?
The practical management of global surveillance is made via the Global Outbreak and Alert Response Network (GOARN). Established in 1998 and functional since 2000, the GOARN is self-defined as a technical collaboration of existing institutions and networks which pool human and technical resources for the rapid identification, confirmation and response to outbreaks of international importance. Surveillance data are provided to 900 WHO partners around the world through the Disease Outbreak News System […] in order to keep the international community constantly alert to the threat of outbreaks and ready to respond.
6
Such a system of information exchange and analysis is based on the use of unofficial sources of information (Brownstein et al., 2008: 1020–1021; Dry, 2008: 10; Grein et al., 2000) with a particular emphasis on news and Internet scanning. With the 2005 IHR, states agreed on the use of unofficial sources of information for global epidemiological surveillance, allowing the WHO to potentially declare pandemic alerts without state approvals and confirmations, 7 which can have tremendous impacts on the conduct of national health policies (Blouin Genest, 2013). It is important to mention, as noted by Fidler (2005), that ‘[t]he rapid and effective emergence of GOARN occurred in this 1998–2003 period, however, without an international legal framework to support it’ (p. 349).
As stated at the preparatory conference to the implementation of the GOARN held in Geneva in April 2000, the goal of this global public health apparatus is specifically to anticipate health risks using information technologies and communication mechanisms: [w]hereas traditional approaches to containing outbreaks were defensive, trying to secure borders from the entry of infectious diseases, modern solutions […] are built on a combination of early warning surveillance systems, epidemic preparedness plans, stockpiles of essential materials, speedy communications and information sharing […]. (WHO, 2000: 1)
Mapping global public health: the WHO Disease Outbreak News System 1996–2010
The Disease Outbreak News System of the WHO is a system of global epidemiological communication and information coordinated by the GOARN. Its functional objective is to inform the international community and national health authorities of disease outbreaks and public health emergencies of international concern around the world on a ‘real-time’ basis (Heymann and Rodier, 2001; 2004; Weir and Mykhalovskiy, 2010). The publication of Outbreak News is dependent upon health issues and its interpretation/classification by the WHO outbreak verification team based in Geneva (Dry, 2008: 12), leading sometimes to conflicting interests over what accounts as a legitimate emergency (Carlowe, 2010; Cohen and Carter, 2010; Godlee, 2010; Lowes, 2010; Watson, 2010b, 2010a, 2011).
As stated previously, one of the objectives of this article is to empirically analyse and evaluate the output of WHO surveillance. What and who is under surveillance? Which diseases are seen as irrelevant/relevant? What does the world look like through the eyes of global diseases surveillance? How do they affect national public health policies? In order to address these questions, disease Outbreak News data were gathered for the period of January 1996 to December 2010. These data are accessible online through the WHO website. 8 They were confirmed, completed, and updated 9 through record research in the WHO archive in Geneva in 2011. Quantitative analyses were performed on these data in order to show the overall trends in global health surveillance.
It is important to note that the data used here are limited in scope and details, thus restricting the potential for analysis. A request to access more detailed data (the outbreak verification list – OVL) was addressed to the Alert and Response Operations Department of Global Alert and Response of the WHO. This request was refused by its Medical Officer, DrAngela Merianos (‘Outbreak verification list’, Email communication, 21 Mars, 2011) who argues that [t]he OVL was distributed confidentially to a restricted public health audience for 10 years from ~1998 to 6 June 2007 when it was unsettled to accommodate more stringent communication requirements under the IHR (2005). We have never changed our policy regarding the use of the OVL beyond a confidential operational tool. Unfortunately I am not at liberty to share the database with you for research purposes.
This argument does not appear sustainable as other authors, close to the WHO, have used these data (see, for example, Chan et al. (2010)). The following analysis is thus limited by the available data.
For the 1996–2010 period, 1947 10 disease outbreak news items were analysed, including several cases with multiple countries and/or diseases. Moreover, the dataset consists of two types of cases: new cases and updated cases. Updated cases are used to track the progression of a disease propagation: 38.10 per cent (742 cases) of the dataset consists of new cases, while 61.90 per cent (p. 1205) are updates. Overall, relatively few (p. 742) epidemiological events were tracked around the world for the 1996–2010 period, which represents an average of 49.47 events per year (4.17 by month) for the entire period and the whole planet. For a global surveillance apparatus that scans and analyses tens of thousands of pieces of information on an uninterrupted basis (Weir and Mykhalovskiy, 2010), this appears to be quite a low productivity rate knowing that, based on their own statistics (WHO, 2010), millions of people die every year from infectious diseases. This situation of relatively low coverage raises the questions of the selection process and of ‘an emergency for whom?’ issues that will be analysed later. According to the WHO, this selection process follows their decisional instrument shown in Appendix 1.
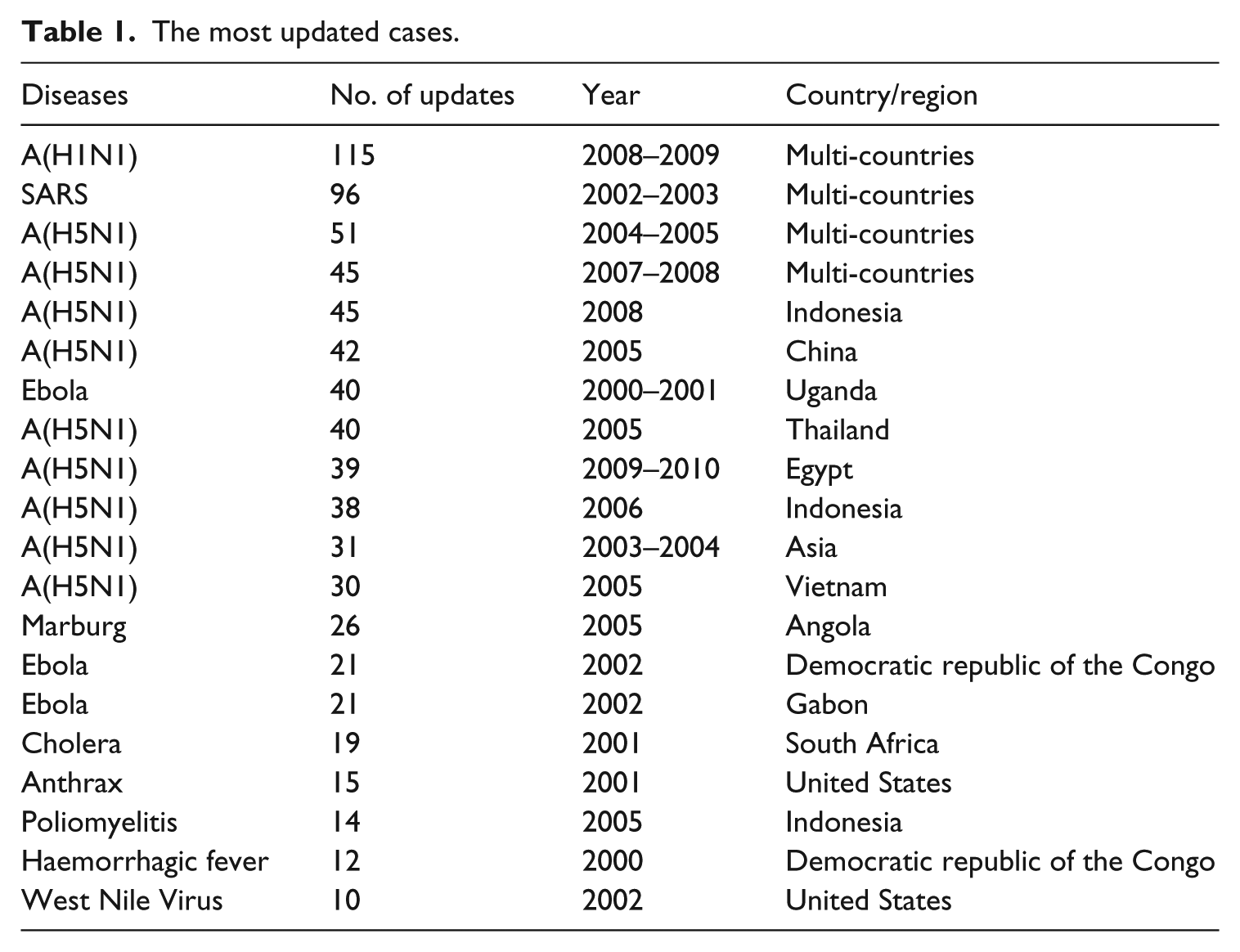
The most updated cases are reported in Table 1. They correspond to the major epidemics tracked by the WHO structure of infectious disease surveillance over the 1996–2010 period. This list contains arguably those most striking infectious diseases from a Western media and popular culture point of view, such as A(H1N1), A(H5N1), Ebola, SARS or Cholera. These diseases generally received a large amount of mainstream attention, reaffirming the argument expressed by Seal (2002) that ‘media presentation of health matters is not neutral, being subject to many determining influences’ (p. 2) such as fear, media exposure, stereotypes, power relations or personal representations of the different actors at stake (a victimization process or search for heroes for example).
The most updated cases.
As showed by Figure 1, when combined by diseases, the range of diseases tracked appears to be limited, with influenza-like diseases accounting for more than 28 per cent, and 71 other health issues 11 representing only 36 per cent. WHO disease surveillance thus puts emphasis on influenza. This finding is intriguing, especially if we keep in mind that a global flu surveillance system operated by the WHO, called FluNet, 12 already exists separately from the 2005 IHR.
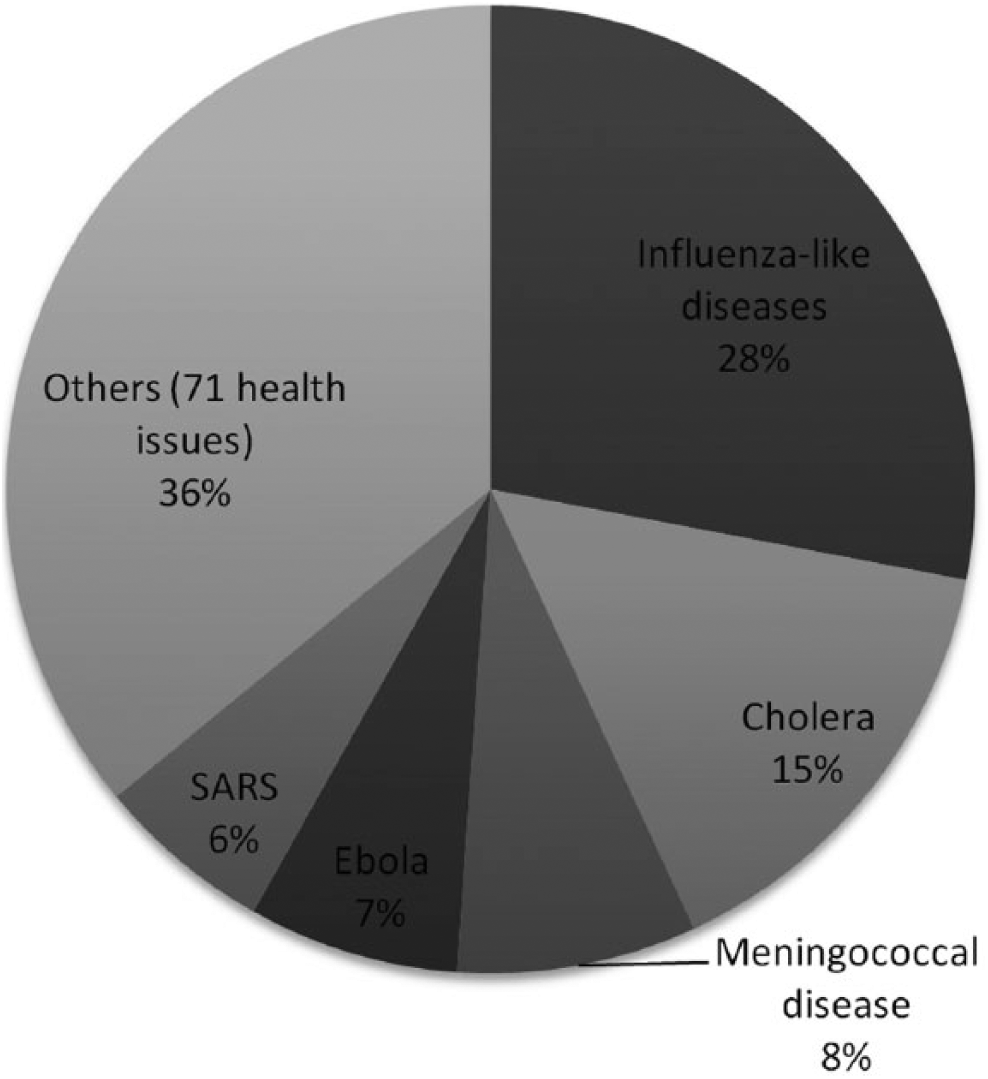
The most tracked diseases.
The chronological development of disease surveillance for the 1996–2010 period is also fashioned by the main pandemics tracked. As can be seen in Figure 2, the progression of disease tracking over time follows a linear pattern, with an average of just over 10 disease outbreak news stories per month, but with a higher reporting rate in time of pandemics. Some of the main historical pandemics of the 1996–2010 period are reported in Figure 2. With the exception of Cerebrospinal meningitis in the Africa Region in 1996 (which occurred separately in a multitude of countries without being analysed as one pandemic by the WHO), they correspond to some of the most updated diseases. While showing that the surveillance structure seems to ‘work’ properly in time of epidemiological crisis, this figure also shows that the surveillance apparatus is potentially prone to bias by being concentrated on diseases affecting mostly industrialized countries (e.g. influenza-like diseases) or culturally feared diseases (e.g. Ebola) rather than those with the most important health impacts (in order: diarrhoeal diseases, HIV/AIDS, tuberculosis, Malaria, etc. – as shown by WHO ranking on mortality rates for infectious diseases (WHO, 2008)). Again, the argument supported by the WHO regarding this selection process is that it corresponds to its decisional instrument (see Appendix 1).
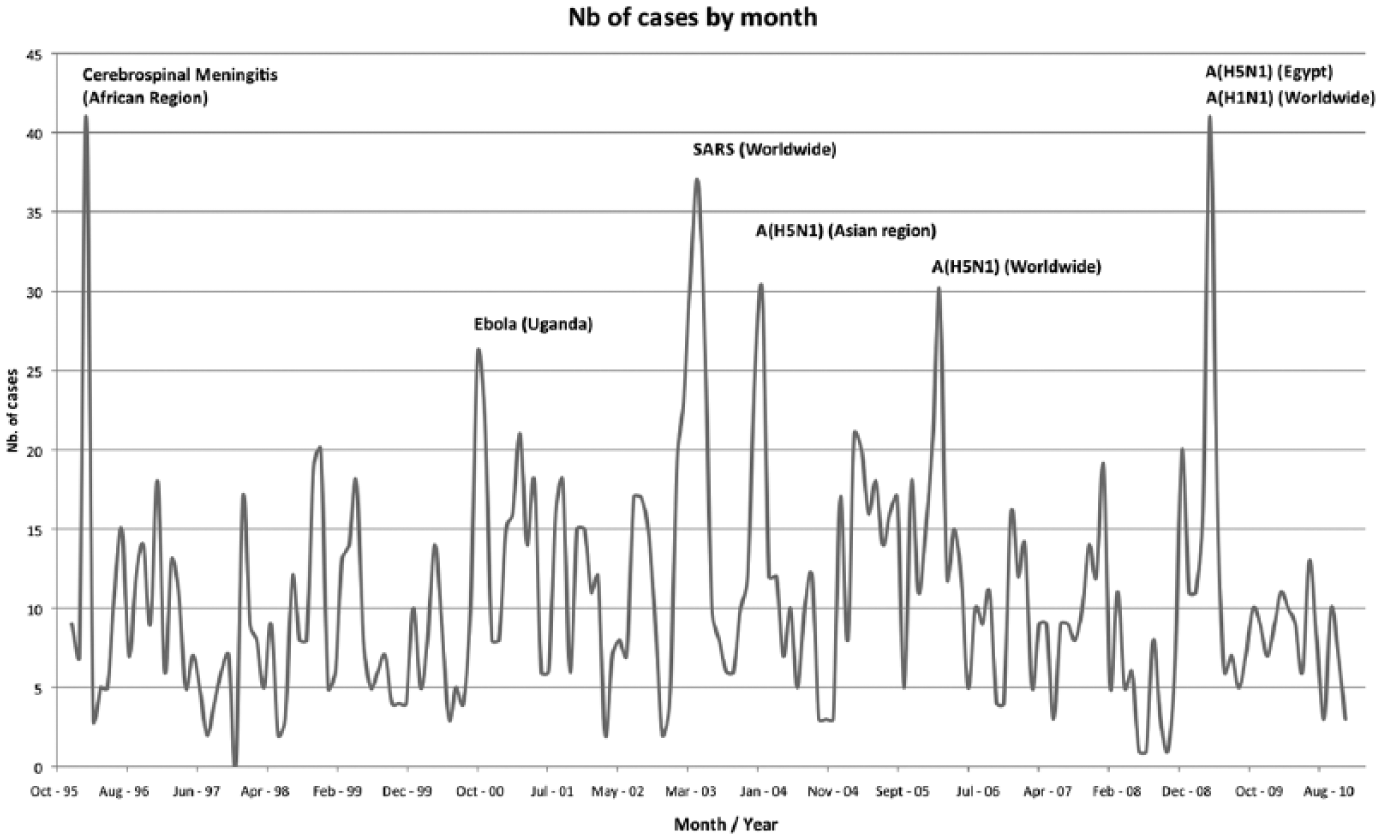
The evolution of disease surveillance over time.
As an example, Table 2 underlines how global health prioritization processes regarding the most pressing health issues depend on the measurement mechanisms and techniques used at the WHO level. This table shows, on one hand, the 10 most frequent diseases tracked by the Disease Outbreak News System in 2008 (number of cases tracked). These top 10 diseases account for more than 75 per cent of all diseases tracked by the WHO system of global surveillance for the 1996–2010 period and represent global health priorities according to the Disease Outbreak News System in 2008. Table 2 includes, on the other hand, the 10 leading causes of death (infectious diseases only) worldwide in 2008 13 as provided by the WHO (deaths, annual figures). They represent the overall global health priorities in terms of deaths, as measured by the WHO in 2008. However, and as pointed out previously, the 10 most reported diseases in the Disease Outbreak News System did not account for the most important infectious diseases in terms of death and health impacts, leading to conflicting global health priorities. None of these leading causes of death were actually in the top 10 of diseases tracked by the Diseases Outbreak News System in 2008. This finding shows no correspondence between the negative heath impact of a disease and its occurrence in the Disease Outbreak News System. This situation highlights how global health priorities are highly dependent on the mechanisms/techniques used to evaluate them, creating contesting spaces for resource allocation processes that may result in important gaps between health issues affecting populations and resources granted. However, it is important to note that many causes of death presented on the right side of Table 2 can be symptoms for the 10 diseases most tracked by the Disease Outbreak New system, explaining partly why we do not find them on the left side of Table 2. 14
Global health priorities, 2008.
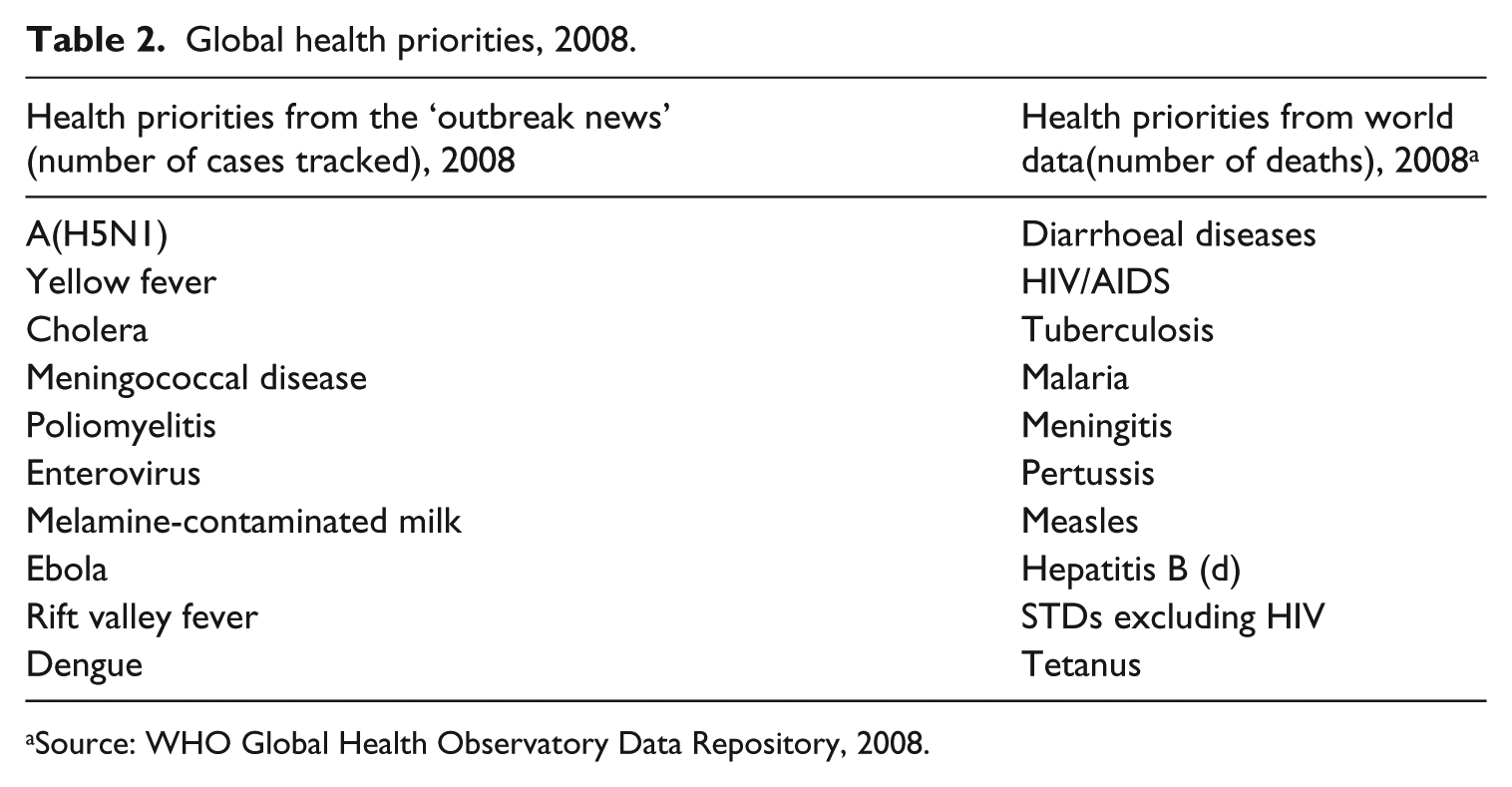
Source: WHO Global Health Observatory Data Repository, 2008.
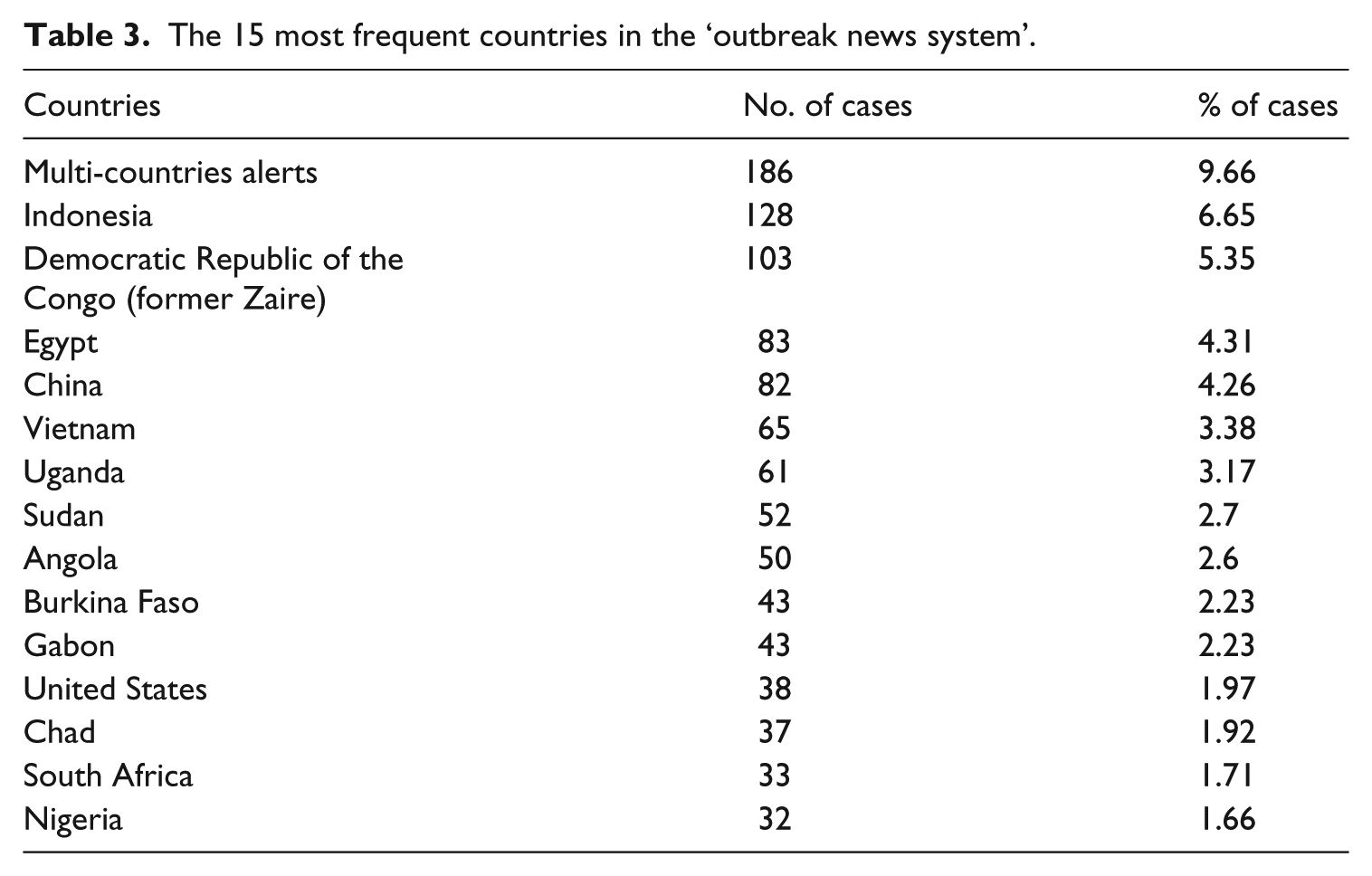
The dataset also shows the stress put on specific countries and regions. Table 3 highlights the top 15 most frequent countries tracked by the WHO surveillance apparatus (for a total of 125 countries). Noteworthy is the importance (more than 9.66%) of multiple countries and worldwide pandemic alerts, as well as the over-representation of Asian and African countries. The importance of worldwide cases underlines the emphasis on the circulation of health risks, rather than health risks themselves (e.g. national health risks). It is also significant to note that the United States ranks at the 12th position, just between Gabon and Chad. The importance put on the United States and North America reveals the higher sensitivity of the global public health apparatus for these countries, which can be partially explained by the fact that a large part of the news analysed by the WHO comes from United States and/or occidental media, 15 and not necessarily by a more problematic epidemiological context. When sorted by regions (Figure 3), the distribution of cases under surveillance is even more oriented towards certain regions, with Africa accounting for more than 43 per cent of all cases. This region is followed distantly by the South East Asian (14%) and Western Pacific regions (11%).
The 15 most frequent countries in the ‘outbreak news system’.
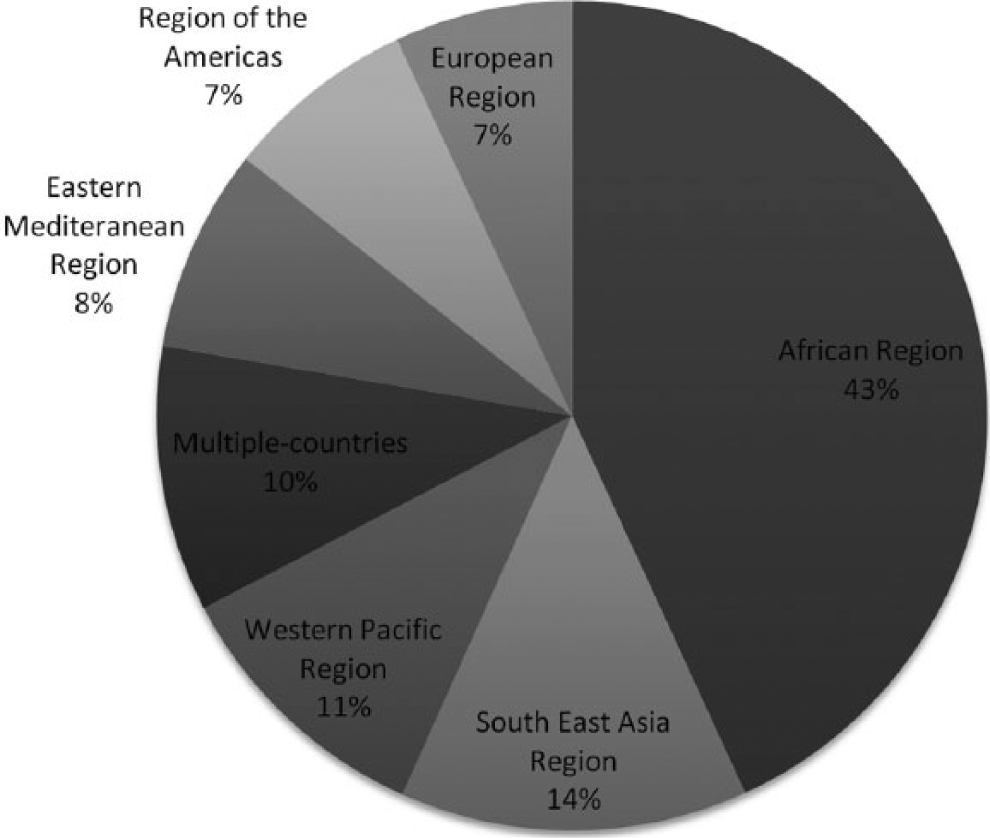
Outbreak news by regions.
The main elements of our empirical analysis can be summarized as follows:
Over the 1996–2010 period, a relatively limited number of new cases (p. 742) were tracked;
There is no equivalency between the prevalence of a disease in the Disease Outbreak News System and its overall health impacts;
The main countries under surveillance are situated in the Asian and African regions, but the United States is among the 15 most important countries tracked;
The emphasis is put on potential multi-country dissemination of disease at the expense of circumscribed and geo-localized health risks;
The circulation of risks, and not health risks themselves, appears to be the main object of surveillance.
These findings do not necessarily invalidate the WHO surveillance apparatus, but they underline the fact that a selection process effectively occurs at the WHO level, a process that is not clearly acknowledged by the organization and for which the selection criteria that go well beyond their decisional instrument shown in Appendix 1 are not widely available. We understand that a multitude of factors can affect risk management and surveillance procedures, including national resources and infrastructures, risk for transnational contagion, endemic diseases versus epidemic or specific local context. We absolutely do not deny the importance of these factors, or others. However, its selection criteria must be clearly identified in order to be able to put in place the necessary evaluation and control procedures. As noted previously, detailed and full-scale data are not even accessible for independent research, which clearly restrain the potential of independent evaluation of the WHO surveillance mechanisms. Global public health policies, as any public health policies funded by public money and resources, must be subject to the same and higher accountability mechanisms, including transparency, which is not actually the case. This situation jeopardizes global public health policies, and it stimulates criticism.
Global public health policy and its discontents
These findings echo the main criticisms, by scholars and practitioners, which have been made regarding of the practice and theory of global public health. Dry (2008) pointed out for example that the global health surveillance structure has shifted from ‘long-term demographic measurements and community-led programs [to] rapid-response-oriented early warning systems that feed into a global network of laboratories and control centers overseen by the WHO’ (p. 9). Dry (2008) further proposed that by focusing on the so-called global health risks, we potentially diverge from the systemic roots of health problems by drawing the gaze to the in-between factors such as mobility, immigration or biosecurity (p. 5).
The global public health agenda, mainly focusing on infectious diseases, is also usually critiqued on the grounds that it favours health issues that threaten the industrialized world compared to endemic – but territorially limited – health problems. This is highlighted by our results where the potential circulation of risks, rather than health risks themselves, appears to be the major criteria of disease surveillance. As pointed out by McInnes and Lee (2006), ‘the attention given to the spread of infectious disease speaks more to the concerns of Western foreign (including economic) and security policy than it does for the concerns of global public health’ (p. 12). By concentrating on surveillance and scenario planning as well as on specific diseases (influenza-like diseases), global public health has been dominated by Western fears and interests (Bingham and Hinchliffe, 2008: 173–174).
In this disaster-oriented perspective, ‘[t]errorism, bioterrorism and epidemic disease became conflated’ (Bashford, 2006b: 13), encouraging the linkage of health with security (King, 2002). The intermingling of global public health and security issues also leads to a prioritization process among health issues that risk following military and political interests (McInnes and Lee, 2006). According to Calain (2007), in such context, the ‘core argument over global surveillance has moved from public health concerns toward foreign and security policies, and economic interests’ (pp. 1–3), concluding that it is the ‘impartiality and independence of the WHO Secretariat [that is] at stake’ (Calain, 2007: 2). This was the situation during the 2009–2010 H1N1 pandemic (Blouin Genest, 2013; Cohen and Carter, 2010).
The focus on a narrowly defined conception of what constitutes a valid health risk has furthermore lead to the exclusion of certain diseases from health surveillance and intervention. For example, an outbreak of tuberculosis in South Africa in 2005–2006 was excluded by the WHO (confirmed by our empirical analysis) because it did not succeed the ‘qualification process’ to be considered a relevant issue for international health concerns (Dry, 2008: 9). As commented by Calain (2007), we ‘fail in our duty to protect the most vulnerable populations during a pandemic [and] there is no escaping from the conclusion that the harvest of outbreak intelligence overseas is essentially geared to benefit wealthy nations’ (p. 19).
These criticisms, which are supported by our results, suggest the emergence of a specific space for public health intervention. Especially noteworthy is the juxtaposition and association of two opposite – though highly symbolic – scales: the microbial (germs, virus, molecules) and the global (globalization, networks, flows, trade, etc.). These two scales merge to form what we can call the ‘global microbial space’.
Under the taken for granted global aspect of public health (Dry, 2008: 4) lie major implications regarding the conceptualization of space and the justified (or not) modes of intervention (nationally and globally). Scalar narratives interact and interfere with potential interventions towards diseases, rendering certain forms of intervention (in)coherent depending on scalar representations (Ingram, 2005). Understood primarily as biological and epidemiological phenomena, infectious diseases have also to be apprehended as cultural phenomena as they are limited by ‘the intellectual framing materials available to [them]’ (Farley, 1992: 33).
One of the most important scientific developments regarding the knowledge of diseases that structured the way we currently think and act about global public health is the transition from the miasma theory of diseases to the germ theory in the 19th century (Karamanou et al., 2012). The germ theory of disease opened the possibility to think scientifically about the world as one unified microbial space. At the basis of this theory lies the idea that diseases are caused by microorganisms such as germs, virus, pathogens and so on, which circulate through different vehicles (water, bodies, animals, infected goods). Four elements are central to the germ theory of disease: communicability, causality, vitality and specificity. These four characteristics profoundly changed the spatial understanding of diseases, rendering circulation one of the central elements of the understanding of diseases. These four characteristics structured the recent developments in the work of the WHO through global health surveillance.
Interestingly, the birth of the germ theory corresponds to the establishment of the first international health institutions, which engendered a new scale of action for public health. The first international sanitary conference, held in the mid-19th century, initiated a new scale of (un)collaborative interventions towards diseases for which the new 2005 IHR is the last event of a long historical process. What was at the beginning considered to be a limited inter-national structure, with an emphasis on Europe and a few other countries, underwent rapid growth and changes to now be considered a ‘global structure’ (Brown et al., 2006: 76; King, 2004: 65).
This conceptualization of diseases and health altered the possible and acceptable responses to health risks. As pointed out by King (2002), in such context, [t]he familiar techniques of medical observation are multiplied globally, and the monitoring of individual bodies in specific places augmented (and perhaps replaced?) by the surveillance of the global population in the de-territorialized space of informatics, telemedicine, databases and the internet. (p. 775)
This popular and generalized conception of epidemic and diseases become acknowledged in the 1990s as concerns over the idea that biomedical threats can be linked to a de-territorialized and globalized world (Calain, 2007: 4) where ‘diseases know no border’ (Roemer, 1994).
Diseases, otherness, and places: (dis)locating interventions
Through the identification of whose health is the most valuable, the territory-identity nexus seems to play a major role (see Table 3 and Figure 3). Those results are interesting as they support the well-documented connexion between the causes of diseases and the less valorized identities 16 (Ingram, 2008: 78; Strange, 2006: 234). According to Weir and Mykhalovskiy (2006: 245), in the post-World War II era, the origins of diseases have been associated with what is represented as ‘Third World’ countries, identified as reservoirs of diseases 17 (Aginam, 2004: 298). Narrative techniques, by stimulating the contagious-anxiety culture, supported the linkage between poor or exotic areas to the origin and causes of diseases (Strange, 2006: 220), thus reorienting interventions towards containment and space control, as shown by our results.
Throughout this process, we face what Ingram (2008) calls the social power of contagion, that is, the tendency to be involved in other-blaming practices regarding the origins and causes of diseases (pp. 78–79). By implying narrative and discursive associations with ‘absorption, invasion, vulnerability, the breaking of a boundary imagined as secure’, infectious diseases themselves are inscribed in a matrix of meanings where mobility, contact, and difference melt in a radical encounter with otherness (Bashford and Hooker, 2001: 2). Fuelled by ‘viral narratives’ (Waldby, 1996), such a distinctive moment seeks to attribute blame and causation. The biological ‘invasion analogy’ where a harmful intruder from outside disrupts the tranquillity of a safe inside thus permeates and infects several social domains (Schell, 1997: 94; Zerner, 2005: 175–176). The virus has in this way become ‘one of the master metaphors of the early twenty-first century’ (Zerner, 2005: 175), stimulated by a ‘contagion-anxiety’ (Bashford and Hooker, 2001: 2), and finding echoes in the media, popular culture and arts (Ingram, 2008).
Contagion metaphors have involved practices of protection that seek to defend the self and the secure from the pathological Other, a social and cultural shelter that relies mostly on containment, quarantine and the establishment of – imagined as – hermetic boundaries (Bashford and Hooker, 2001: 5). According to Schell (1997), ‘[v]irus discourse is retelling old imperialist nightmares that, neutralized under cover of medical common sense, seem to justify exclusionary practices, surveillance, and general prejudice that we would otherwise find inexcusable as well as politically untenable’ (p. 97). Diseases have indeed a fabulous potential to evoke, through their metaphorical functions, the notions of threat and danger (Sontag, 1979), notions that can be ‘use[d] to make moral judgment’ about the diseased (Lupton, 2003: 61).
In this sociocultural and institutional imaginary, the disease is seen to come from outside of a secure self, reducing complex and multifaceted problems to single cause explanations based on space and territory (Convery et al., 2006: 97). This process strongly affects the structure of national health programs by orienting allocation of resources or priorities. The territorial and spatial distinction between the sick and the healthy remains in this sense one of the major determinants of the rationality behind the social interaction with diseases, finding echoes in the current structure of global health surveillance and the 2005 IHR, where it still relies to some degree on the pervasive rationalities of the colonial cordon sanitaire and its territorial distinction between the sick and the healthy, the clean and the dirty.
In such a context that appears to be more imperial than global (Aginam, 2003; Bashford, 2006a; Ingram, 2008: 82–83), the territorial border still gets the function of a ‘line of hygiene’ (Bashford, 2004; Hooker, 2006: 189). Essential to these strategies is the territorial circumscription of the movement and mobility of what is represented as pathological and dangerous. This conception of the pathological threat echoes ‘the long history of the geopolitics of disease [where] people being considered properly in their place, or improperly out of place’ (Bashford, 2006b: 10).
This peculiar process has profoundly shaped the practice and techniques of global public health. As pointed out by King (2002), we are still facing an ‘obsession with boundaries – between races, between classes, and between nation-states – [that] persists, as does the origin narrative that locates the ultimate source, or “reservoir,” of disease in other nations’ (p. 773). This corresponds to the tendency to containment (of circulating risks), rather than prevention based on social determinants of health, that we observed with our results. In this context, it is hard to escape the conclusion that global public health does more than (re)drawing borders through the concept of circulating risks.
Conclusion: being ‘at risk’, or the fraud of global public health policy
Global disease surveillance by WHO is at a crucial time in its existence. It is necessary for effective global public health, as millions of people still suffer from preventable diseases, but it is at the same time highly criticized and exposed to conflicting interests. Our results underlined the bias and selection process that affect disease surveillance, but that it is not transparently divulged by WHO beyond their decisional instrument. This situation jeopardizes the effectiveness of global public health, notably through the introduction and strengthening of a new category: the ‘at risk’. This phenomenon had been previously identified by Castel (1991) as a widespread ‘shift from dangerousness to risk [entailing] a potentially infinite multiplication of the possibilities for intervention’ (p. 289).
According to Castell, through this process, the ‘notion of risk is made autonomous of that of danger’ (p. 287). With risk assessment, the identification and evaluation of danger are not made anymore on the basis of the actual presence of the danger, but rather on its probability of occurrence, what Castell called the ‘statistical correlation of heterogeneous elements’ (p. 288). This implies a new mode of surveillance named systematic pre-detection. In such indirect relationship, ‘[s]urveillance can be practiced without any contact with, or even any immediate representation of, the subjects under scrutiny’ (p. 288). The focus is rather put on the gathering and collecting of information, data and numbers, as we can see with the WHO Disease Outbreak News System.
This conceptualization exemplifies the problematical relationship between risks and surveillance. As pointed out by Clarke et al. (2003), ‘[r]isk and surveillance mutually construct one another’ (p. 172), producing a legitimization process in which risks are used as justification for surveillance, when at the same time these risks are more precisely identified and measured through surveillance (Lupton, 1995, 1999). What is striking with global infectious disease surveillance, as shown with our results, is that it is not only risks that matter, but more importantly the potential circulation of risks.
‘Circulating risks’ appear today to be the main objects of global public health, leaving aside other ‘static’ (e.g. endemic) issues such as inadequate sewer system, resistance to antibiotics or social determinants of health that still cause millions of deaths every year. The potential for circulation is what makes risk a valid argument for being identified as a public health emergency of international concern. Contrary to what is usually said, global public health is not involved in a ‘war against diseases’, but rather in a war against the circulation of specific risks.
This global apparatus rather seeks to align a neo-liberal order. Movement and immobility, embodied by the securitization of circulation, reveal this global public policy where health is conceived in terms of optimization of the neo-liberal collective body. This static/dynamic dichotomy leads us to an interesting paradox. The acceleration of circulation through globalization is seen as causing global health risks, while the main objective of the 2005 IHR is to reduce the potential impact of public health policy on the flows of trade and travel. Circulation and mobility are then understood in global public health as both the cause of health risks and what should be secured from these risks, a paradox that, at least partly, explains the dramatic failure of the current global public health policies.
Footnotes
Appendix
Acknowledgements
The author wants to thank the anonymous reviewers for their valuable comments on previous drafts.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.