
Abstract
Our goal in this investigation was to help shed light on the very difficult process of collaboration between family physicians and specialists working at different levels of healthcare delivery. More precisely, and grounded on Giddens’ structuration theory, our investigation aims to understand how medical collaboration emerges and develops around chronic patients. This was a longitudinal interpretive case study, the “case” being a continuum-of-care for patients suffering from diabetes, put in place in an urban health center in the Canadian province of Quebec. The study shows how the application of rules of signification and of legitimation, combined with domination resources, have supported the emergence of new forms of collaborative practices. Our analysis reveals, however, that new collaborative practices at the administrative level do not necessarily entail greater shared decision-making in patient management and the mobilization of knowledge across boundaries. The study also corroborates the mutual recursive influence of practices and structures. Our study’s most important contribution concerns the impact of knowledge dynamics, that is, individual and collective learning, on the development of medical collaboration across levels of care.
Keywords
Introduction
Healthcare reforms in Canada and other Organization for Economic Co-operation and Development (OECD) countries have tried to break down silos between healthcare professionals and organizations in order to improve the quality and efficiency of care delivery. In fact, different Canadian policy commissions (e.g. Clair Commission, 2000;; Sinclair Commission, 2000) have concluded that a functionally integrated healthcare system is essential for strengthening quality of services and for ensuring the sustainability of the healthcare delivery system. Hereafter, there is a need to foster collaboration between healthcare providers. Translating the will to collaborate into effective collaborative practices is however an elusive goal (Addicott et al., 2007).
Analyses from different traditions and disciplines have advanced various explanations for this phenomenon. From a traditional managerial viewpoint, healthcare organizations are seen as professional bureaucracies whose coordination processes rely on qualification standardization and actor autonomy (Mintzberg, 1978); they therefore display considerable resistance to change (Lamothe and Dufour, 2007). From the perspective of the sociology of professions (Abbott, 1988), collaboration is hampered by professional jurisdictional battles because powerful professionals attempt to protect the exclusivity of their scope of practice, which rests on their symbolic power (Oborn and Dawson, 2010). Traditional modes of health professional training and socialization are also said to hinder knowledge integration (Weinholtz, 1991).
Despite the aforementioned institutional obstacles, a number of recent investigations have shown that interprofessional collaboration in healthcare delivery can be effective. For instance, Currie and White (2012) found that, in a multidisciplinary pediatric nephrology unit, fine management of group dynamics fostered the development of a local community of practice and more distributed knowledge brokerage. Formal and informal processes engendered a clinical group identity, centered on the patient’s well-being. These findings corroborate those of an earlier study that highlighted the beneficial role of operational proximity and shared values oriented toward the creation of organizational “citizenship” in knowledge diffusion through professional groups (Tagliaventi and Mattarelli, 2006). Both works emphasize that several mechanisms acting at a micro-level, specifically within an organizational unit, may counterbalance traditional obstacles to interprofessional collaboration.
But what happens when health professionals are expected to collaborate across organizational boundaries? We are interested in this issue particularly as it relates to clinical collaboration between general practitioners (GPs) and medical specialists working in different organizations.
Two sets of arguments—practical and theoretical—support further examination of collaboration among physicians operating at different levels of healthcare delivery. At the practical level, current evidence suggests that physician collaboration is far from optimal. A study conducted among medical residents in four Canadian provinces clearly illustrates this point, underlining the wide gap between existing and desired levels of medical collaboration (Beaulieu et al., 2006). At the theoretical level, Martin et al. (2009) observe: “Rare are studies examining the reconstruction of professional boundaries by actors on the ground in the face of technological, managerial or policy changes. Another, under-researched area is the intra-, rather than inter-, professional boundaries within occupations” (p. 3).
Starting from a conception of collaboration as the process that “occurs when a group of autonomous stakeholders of a problem domain engage in an interactive process, using shared rules, norms and structures, to act or decide on issues related to that domain” (Wood and Gray, 1991: 146), this paper aims to improve understanding of the processes by which medical collaboration emerges and develops across organizational boundaries. We begin by surveying the current state of knowledge on the subject, identifying knowledge gaps and research needs, and defining the research questions. We then set out our analytical framework, drawing upon Giddens’ social structuration theory (1984), and describe the qualitative research methodology that we have adopted. In the following section, we describe the results obtained, and we end up the paper with the discussion of our findings and the contributions of knowledge generated for both theory and practice.
Medical collaboration across levels of healthcare: a literature review
The relatively scant empirical literature on this topic may be divided into two major research streams: the first consists of studies that seek to identify and describe the factors affecting collaboration; the second involves studies that aim to understand the processes through which collaboration emerges.
Factors affecting medical collaboration across levels of care
Individual motivations for physicians to collaborate can influence medical collaboration. GPs wish to develop interpersonal professional relationships with specialists largely to gain better access to specialist services for their patients and acquire new knowledge through collaboration (Berendsen et al., 2006). By contrast, specialists tend to perceive few learning opportunities from GPs (Marshall and Phillips, 1999), seeking rather to use collaboration to regulate the demand for specialized care.
As most studies of medical collaboration concern patients suffering from chronic conditions, they tend to view collaboration as being motivated by patients’ complex healthcare needs over time. However, particular complex cases, for example, serious mental health disorders, may deter GPs from assuming patient care (Fleury and Petitclerc, 2008). Still, regarding mental health, a good relationship with a hospital team may (Horner and Asher, 2005) or may not (Fleury and Petitclerc, 2008) encourage GPs to perform active patient follow-up. Furthermore, when paid on a fee-for-service basis, physicians may feel inadequately remunerated for the time they spend monitoring and caring for depressed patients (Kilbourne et al., 2004).
GPs’ referral practices vary widely and do not arise solely from patient needs (Franks et al., 2001). Time pressure and financial incentives seem to have little influence on rates of referral; the physician’s characteristics, such as years of experience and degree of specialization, appear to have greater weight. Physicians’ psychological issues (e.g. risk tolerance) have mixed effects (Franks et al., 2001). The choice of specialist by a generalist is influenced by many factors such as medical skills, ease in obtaining an appointment, prior experience, quality of communication, and the specialist’s efforts to return the patient to frontline care (Kinchen et al., 2004). Furthermore, problems of communication often persist between levels of care. Information technologies can help resolve communication problems but their implementation is highly complex (Sicotte et al., 2006).
The notable difference between the views of specialists and generalists regarding their interest in sharing clinical guidelines for the follow-up of chronic diseases (Kasje et al., 2002, 2004) can help us to understand collaboration motivations and practices. By and large, generalists seem more interested in using common practice guidelines to better harmonize care. Specialists, by contrast, do not feel a pressing need to use guidelines, basically due to their perceived lack of outcome expectancy (Cabana et al., 1999; Pronovost, 2013). Perceptions of the evidence also differ significantly: while both generalists and specialists follow methodological criteria, generalists also consider it important to respect the contextual nature of primary care delivery (Beaulieu et al., 2004).
In sum, empirical research on the factors that may influence medical collaboration across levels of care has identified many plausible determinants of collaboration at individual (physician and patient), organizational, and systemic levels. However, findings are not yet conclusive: psychological factors, physician remuneration modes, information technologies, degree of formalization, and quality of relations between levels of care have diverse and contradictory effects on medical collaboration. Therefore, there is a need to better understand the phenomenon. Process studies can potentially fill this gap.
Process studies of the development of medical collaboration
Process studies aim to understand how and why things emerge, develop, or terminate over time (Langley, 1999). Said differently, such studies are interested in grasping actors’ dynamics. Political and cognitive dynamics are particularly important in professional environments (Dubar and Tripier, 1998) and have significant influence on collaboration practices and structures.
Political dynamics
Work in the sociology of professions has described the battles over professions’ jurisdictional boundaries (Abbott, 1988). These power struggles unfold at both the interprofessional and intraprofessional levels, as Currie et al. (2009) demonstrate. These researchers explore changes in professional relationships—among family physicians and between specialists and family physicians—after policymakers assigned a new role called “General Practitioner(s) with Specialist Interests” (GPSI) to some family physicians. They highlight how professional relationships have been disturbed by “modernisation” of the system through the introduction of new roles, hindering the development of collaboration: specialists protect their professional jurisdiction, claiming to hold the expertise needed to perform the task adequately and thus accepting only subordinate roles for GPSIs. Meanwhile, GPs are alarmed by the introduction of a “specialized” role (i.e. a new hierarchy based on new knowledge) for some of their peers.
While political issues can limit collaboration and knowledge mobilization across boundaries, it has also been proposed that power can be productive. Based on the theory of resource dependency, akin to a political perspective on organizational dynamics, Mur-Veeman et al. (2001) explain the stakes involved in deploying shared-care models. In this view, an organization’s survival depends on its capacity to control indispensable resources. The organization thus establishes inter-organizational links with other organizations in its environment to reinforce its power. Regarding the implementation of shared-care models, the motivation for and dynamics of such collaboration rests largely on a perception of interdependence, notably concerning access to scarce resources, that is, expertise.
Cognitive dynamics
Few empirical studies have explored how changes at the organizational level, intended to improve medical collaboration, effectively influence collaboration practices and knowledge dynamics. In his study of telemedicine projects, Nicolini (2007) traces the dynamics of learning that accompany the introduction of information technologies and prompt temporal and spatial redistribution of medical practices. Videoconferencing in cardiology, for example, leads cardiologists to compensate for the loss of certain diagnostic avenues (visual, clinical examination) by increasing their interaction with family physicians. This interaction catalyzes a learning dynamic: both cardiologists and GPs learn what questions to ask, what elements to attend to, and how to “see” them.
Similarly, Nilsen (2011) has illustrated how videoconferencing reinforces collaborative work and offers opportunities for learning in daily medical practice. Notably, medical talk enables continuity in knowledge-sharing and might close gaps revealed by dilemmas: traditional written referrals typically lead to incomplete information, which affects the quality and comprehensiveness of the communication. Conversely, collaborative real-time work facilitates the immediate resolution of such gaps and dilemmas.
In the same vein, Osmundsen et al. (2015) have shown how, in the context of diabetes management, telemedicine allows a beneficial co-production of healthcare delivery: tripartite consultations may lead to positive outcomes such as patients being empowered to take a more active role in their own care, GPs increase their knowledge and competence exchanging with specialists, and the latter become more aware to adopt a more holistic approach to care.
To conclude, although process research has examined medical collaboration across organizational boundaries and provided insights into political and cognitive dynamics, several shortcomings remain. First, political dynamics have mainly been viewed as obstacles to collaboration. Few process studies have been interested in examining how actors’ dynamics contribute to the emergence and development of collaboration practices. Research on cognitive issues has provided some insights but has mainly focused on the impact of information technologies on collaboration practices. Furthermore, these studies have not examined the evolution and eventual institutionalization of collaboration practices and structures over time. In fact, research generally concentrates on the micro-dynamics of medical collaboration; the analysis does not encompass the “diffusion” of practice changes in the field.
Taking into account these knowledge gaps, we have defined the research questions that guide the present empirical investigation as follows: (1) How do collaboration practices between GPs and specialists working in different organizations emerge and develop? (2) How do these practices become institutionalized?
Relevance of structuration theory for understanding medical collaboration
We have adopted Giddens’ structuration theory (1984) as the broad theoretical framework for this investigation. This meta-theory aims to reconcile two competing visions of actors’ dynamics: primacy of structures and primacy of actors’ agency. For Giddens, structures exist as a property of social practices and should not be conceptualized as given. Practices are seen as recurring and regularized actions which are performed by individuals situated within a social system and which also create and recreate that system. This theory posits that structures are simultaneously empowering and constraining and ensue from previous actions. Said differently, structures are both outcome and resource for action. Structures are sets of rules and resources that individuals use and reconstitute in the course of their actions. More specifically, social agents produce and reproduce practices by drawing on three complementary dimensions of structures: rules of signification (meanings); rules of legitimation (moral rules); and resources of domination, either allocative (e.g. control of materials) or authoritative (control of people). This definition of structures is broader than the usual definition found in the managerial literature and also includes the institutions, that is, cognitive, regulatory, and normative structures, that impact meaning and bring stability to social behaviors (Scott, 1995).
Another central premise in structuration theory is that social actors are knowledgeable agents, meaning that they are aware of social rules, and possess and apply knowledge in the production and reproduction of everyday encounters (Giddens, 1984: 22). This competence is expressed in words, by means of discursive consciousness, or in routines, by means of practical consciousness. That being said, agents are not necessarily fully aware of all the implications of their actions: there are unacknowledged conditions of their actions as well as unintended consequences. Agents are also reflexive as they have the capacity to observe and understand what they are doing while they are doing it.
Overall, what stands out is that structures and systems do not exist independently of agents but only in the context of their practices; hence, the interest in analyzing them. Giddens (1979) invites us to pay special attention to knowledge and power dynamics arguing that the concept of action is logically tied to that of power. The latter notion is understood as transformative capacity embedded in action.
Methodology
Our stance in the process of knowledge generation is broadly interpretive. As noted by Morgan (1980), this perspective
is based upon the view that the social world has a very precarious ontological status, and that what passes as social reality does not exist in any concrete sense, but is the product of the subjective and inter-subjective experience of individuals. (p. 608)
More specifically, this study has involved critical interpretive research since, as defined by Deetz (1982), we worked with a variety of texts (instigated, pre-existent) and looked at organizational “deep meaning structures” in relation to medical collaboration.
Within this paradigmatic framework, and with the aim to specifically examine the evolution of collaborative practices over time (from emergence to institutionalization), we decided to conduct a longitudinal qualitative case study (Stake, 1995) since a longitudinal design appears necessary to observe how processes unfold over time (Menard, 1991). The research period considered lasted 9 years, from 2006 to 2015, fieldwork having been conducted from August 2012 to May 2015.
The main unit of analysis, that is, the “case,” is the continuum-of-care for diabetic patients conceived and implemented in an urban health center in the Canadian province of Quebec (hereafter referred to as HSSC-A). For a number of years, this health center has been working on improving medical collaboration between levels of care (primary, secondary), notably for a better management of chronic diseases. We chose this continuum-of-care because diabetes is a common chronic medical condition accounting for a significant proportion of frontline medical services. Furthermore, to be effective, the management of diabetes requires a close collaboration among health providers and patients, the aim being to slow down the progression of the disease and prevent subsequent complications through a comprehensive healthcare approach, for example, promoting lifestyle interventions, adopting preventive interventions of cardiovascular risk factors, and maintaining blood glucose levels in the normal range. In addition, current evidence clearly stresses the importance that such patients are cared for by a multiprofessional clinical team (family physician, nurse, pharmacist, dietitian, psychologist, etc.) with specific training in diabetes that operates at the primary healthcare level and with the eventual support of medical specialists (Clement et al., 2013: 22).
Most healthcare services in Quebec are funded by the government through taxpayer contributions and provided by public organizations that offer primary, secondary, and tertiary health services. While this is a publicly funded healthcare system, physicians affiliated with it are independent entrepreneurs who are basically paid on a fee-for-services basis, whether they work in private practice or in public institutions. Governance of the system has been partially decentralized over the years: the organization of health services and the allocation of financial resources has been delegated to Regional Agencies.
The Quebec healthcare delivery system underwent a major reform in 2004 aimed at replacing a producer-oriented logic by a population-based approach. Its main objectives were to (1) maintain public health and address its determinants, (2) manage patients within a given territory, and (3) involve citizens in healthcare decision-making.
The first decision taken by policymakers was to create 95 Health and Social Service Centres (HSSCs) across the province. The new HSSCs were created by merging formerly independent healthcare organizations operating within the same geographical territory, that is, community health centers known as CLSCs, which offer primary health and social services, long-term care institutions, and general acute-care hospitals. Decision-making power concerning health services organization was decentralized to the HSSCs, which were mandated to develop collaborative arrangements with other care providers within their territory and with supra-regional entities. The Regional Agencies were also mandated to support the implementation of health services networks.
Data collection and analysis
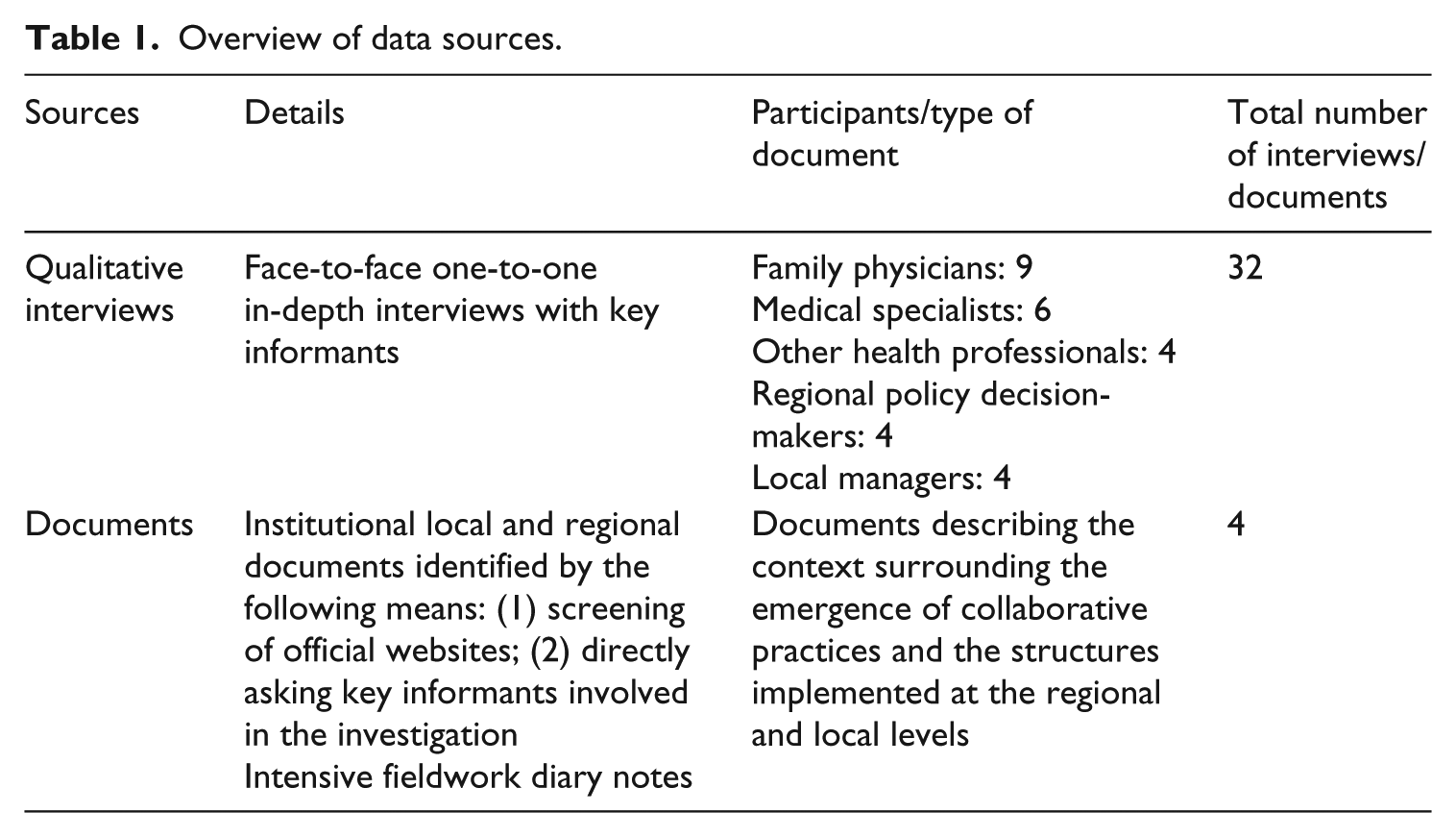
After having obtained ethics certificate from competent institutional review boards, we used multiple sources of data during fieldwork (i.e. August 2012 to May 2015). First, we conducted 32 face-to-face, one-on-one interviews over time with key informants: nine family doctors working in different settings; six medical specialists (three endocrinologists, a cardiologist, two internists); four decision-makers and advisors from the Regional Agency (including three family physicians); four HSSC-A managers; and four other health professionals specializing in diabetes. Three participants, more specifically those most involved in the implementation of collaborative practices, were interviewed twice (at the beginning and at the end of the research project). These participants were very well positioned, both clinically and administratively, to describe in rich details the evolution of collaborative structures and practices. The first and third co-authors conducted these individual interviews in French which lasted 90 minutes on average. Individual interviewing allowed us to gather data about respondents’ perceptions of the issues involved in diabetic patient management, their own professional roles and that of other actors in the healthcare delivery system, their collaborative practices with other levels of care, and learning in the course of these practices, as well as retrospective data concerning the emergence of collaborative practices (events, actors involved, modes of interactions, etc.). All interviews were recorded and then transcribed in full and coded with the support of NVivo-9 software. Coding was performed from the very beginning of data collection on a continuous basis. Based on the conceptual framework of the study, we first elaborated an initial coding book, which was iteratively revised during the coding of new transcribed verbatim. Some interviews were double-coded by two members of the research team to enhance the definitional clarity of codes and the reliability of the process.
Second, we also gathered and analyzed a variety of organizational documents describing the context surrounding the emergence of collaborative practices and the structures implemented at the regional and local levels. This source of qualitative material was very helpful in ascertaining: (1) why and how the regional agency contributed to the emergence of collaborative practices (e.g. putting in place certain new structures to foster collaborative healthcare delivery) and (2) the structures implemented at the local level which aimed at formalizing the collaboration between specialists and family physicians and their evolution. Two strategies helped us to identify and obtain these documents, namely websites screening (e.g. regional agency, HSSC-A), and directly questioning key informants in the field—please see Table 1 for an overview of data sources.
Overview of data sources.
We used a set of intertwined methods and processes to analyze the generated data. We first constructed a global narrative (Langley, 1999) including actors, processes, and events that happened over the period under examination. We specifically focused on the thick description of the processes whereby collaborative practices emerged and developed over time in their situated space/time context. This global narrative set up the second subsequent phase of our data analysis, in which we used a temporal bracketing strategy. Inspired by Giddens’ structuration theory (Langley, 1999), we broke down empirical material into three successive periods (period #1 from 2006 to 2009; period #2 from 2010 to 2011; and period #3 from 2012 to 2015) by pointing out those decisions or events that triggered change, that is, “discontinuity” in the current structure-agency recursive dynamic. Then, driven by the theoretical framework, our third analytical step involved the detailed analysis of collaborative dynamics in each one of the identified periods. We specifically focused on describing current dominant structures and collaborative practices, understanding processes whereby practices instantiated structures, and explaining underlying mechanisms (power relations relationships, knowledge dynamics, etc.). Therefore, periods identified became comparative units of analysis, each one being defined by continuity in context and actions being pursued within them, and discontinuities (change) at their frontiers.
Results
When studying the issue as to how collaborative practices between GPs and specialists working in different organizations emerge and develop in diabetes management, it is possible, as noted above, to break down this structuration process into three subsequent phases corresponding to, respectively: the emergence, the adoption, and the institutionalization of such new collaboration structures and practices. The analysis of the first two phases addresses our first research question whereas the analysis of the third phase concerns the last one. Our results illustrate how structures are both outcome and resource for action, that is, how structures and collaborative practices influence each other.
Period #1 (2006–2009)—emergence of collaborative practices and creation of a diabetes referral center
Following the introduction of a reform, new structures have been implemented that aimed to promote collaboration between levels of governance, and between administrators and clinicians, resulting in the creation of a diabetes reference center. This new structure constituted a leverage for changing medical practices.
How did structures at the field level trigger new collaborative practices between the regional authority and health centers aimed to support family physicians in the management of patients suffering from chronic diseases?
As noted above, the reform assigned the Regional Agencies new roles, allowing them significant influence over the development of a continuum of care and services at the local level. Structures to support collaboration between the Regional Agency’s managers and those of the region’s new HSSCs were created, including the “Consortium montréalais en gestion des maladies chroniques (2006)”, which took note of the high prevalence of chronic diseases in the region. The creation of that Consortium, aimed at “developing a preventive approach to frontline care, improving the healthcare network, integrating and harmonizing resources, and developing a coordinated regional program”, enabled the emergence of new consultative practices between managers at the local and regional levels and gave rise to the development and implementation of a series of pilot projects for the management of chronic diseases, selected through a tendering process.
The Chronic Care Model (CCM) is a patient management model that was widely used in the healthcare system at the time (Wagner et al., 1996). The CCM strives to optimize the management of chronic diseases through, among other things, integrated resource management, monitoring of outcomes, and the deployment of fluid, clear, harmonized processes and care continuums known to all actors. As an institution, the CCM provided a template for the shape of the pilot projects and the project approval criteria:
And this, it’s recognized in the literature, is the Wagner model for treating the patient, and it’s also the American model for patient management of the chronically ill, which basically says that we will manage all this with the general practitioner; we will only look for a specialist occasionally. (Manager, HSSC-A)
In addition to overall compliance with the CCM, it was mentioned that proposed projects had to target frontline services (meet the needs of family physicians), include a clinical program, and provide for clinical (health impact) and administrative assessment metrics. It was also stipulated that funded projects had to involve knowledge transfer activities in order to disseminate the tested model.
How did regional demands favor the emergence of collaborative practices at the local level, resulting in the proposition of a new structure whose objective is to support medical collaborative practices between levels of care?
To respond to the call for tenders, HSSC-A assembled a team of specialists (endocrinologists and internists), family physicians, and other healthcare professionals to assess the needs (of the family physicians) and develop the outlines of a diabetes management program. The new collaborative practices between the HSSC’s clinicians and administrators grew out of the health system’s new structure, specifically the creation of merged institutions which made it possible for specialists to work in frontline institutions and enabled a population-based approach. Being responsible for the health of a given population, administrators and some clinicians became aware of the scope of the challenges involved in diabetes management within their territory:
The crowning achievement that came out of the creation of the HSSC was to say, we have one mission, which is the HSSC’s mission, not three facilities’ missions. And the objective is to take our patient through those three missions without the patient noticing it, so it is a whole, an organized continuum of care. (Manager, HSSC-A)
For example, they realized that lack of resources to support management of diabetic patients by family physicians was a factor in creating longer waiting lists to see specialists. Therefore, they proposed a solution based on the creation of a diabetes referral center (henceforth the Center), a new structure whose primary mission would be to provide family physicians with the professional and specialized support they needed for management of this patient population. Responsibility for administering the project was assigned to an internist who had shown enthusiasm for the initiative. However, the endocrinologists involved were disinclined to apply the proposed approach:
In principle, the patient should be managed by us, the endocrinologists. But here the responsibility was given to the internists, who didn’t necessarily have specialized training in diabetes. On the other hand, they may have been more available. So, this created a real problem, you know, because as a specialist, an endocrinologist, I don’t feel I’m, how should I say, in a position where I should be working under the command of other colleagues who are not specialists such as myself. (Endocrinologist)
How did the implementation of a new structure at the local level favor the emergence of medical collaborative practices, perceived as innovative?
As the proposed Center was deemed to be consistent with the Consortium’s requirements, the Regional Agency granted the required funding to implement the project and supported program development. The new clinical/administrative collaborative practices across the local and regional levels therefore led to the installation of the Center at a CLSC. Its main mission is to support family physicians by managing, for a specified time, the diabetic patients they refer to the Center either for lifestyle change (education and follow-up by a team of professionals) or for education and treatment of unstable diabetes (with intervention and specialized medical follow-up by the internists for 2 years).
In the view of the professionals involved in designing the project, this approach allows for optimization of professional roles:
So, specialists see what has to be seen. Not only, for example, to inject insulin. In my opinion, general practitioners can do that. But because doctors were trained, they were able to start a treatment, and modify it up to the point where they say, “no, personally, I can’t do that; I need an expert opinion to pull things together, to combine the medications and then the insulin.” This means that, ultimately, specialists see what has to be seen, and family doctors do what has to be done well for patient management. (Medical advisor, Regional Agency)
The new clinical structure supported the development of innovative clinical practices in several ways. First, it led specialists (in this case internists) to practice in a setting typically reserved for frontline practitioners (CLSCs), in direct collaboration with a team of non-physician professionals:
Well, the interesting thing is that we have secondary and primary care in one place, the CLSC. So the team of specialists has been moved to the CLSC, which is a frontline environment. I think that is something quite new, you know, that specialists should leave the hospital and go really close to the field, to a CLSC. (Manager, Regional Agency)
It would appear that, for many family physicians, bringing all these types of expertise together in one place represents not only an innovative approach but a significant improvement over consulting a specialist:
For us, it’s more than a consultation with a specialist. They get the patients back on their feet, stabilize them, and adjust the insulin, so that we can continue following them afterwards. So it’s a different sort of patient management, it’s not just referral to a specialist, it’s an entire program. (Manager, HSSC-A)
The family physicians therefore developed new referral practices by sending their patients to a center rather than simply to consult a specialist:
… [I]t is a change. I rarely refer patients to the endocrinologists now. I am more likely to send them to the CLSC. Because I find that they are better equipped, they have an interdisciplinary team at the CLSC rather than one specialist. Because the specialists don’t necessarily have more resources than a regular physician if they’re not working in a specialized diabetes program. (Family physician)
The development of these referral practices on the part of family physicians is also related to the Center’s administrative structure, particularly the creation of an operational follow-up committee with an explicit mandate to promote and develop relationships with local medical clinics (outreach).
In addition to the follow-up committee, the HSSC set up management and coordination committees to ensure the Center’s smooth operation. These local bodies all involve, to varying degrees, HSSC managers and physicians. Officials from the Regional Agency also actively participate in some of them (e.g. the evaluation committee).
Period #2 (2010–2011)—adoption of collaborative practices
From the outset, the process of setting up the Center was informed by a vision of frontline practitioners, and particularly family physicians, as central players in the management of chronic diseases and diabetes, supported by a secondary care team managed by an internist. This process ended up in the development of a number of changes in clinical collaborative practices between family physicians and specialists. Through time, structures supporting these new collaborative practices evolved, as a result to the physicians’ needs and demands.
How did medical practices evolve following the introduction of a new structure (reference center)?
The reorganization of health services did not have a major impact on clinical decision-making practices since each doctor remained autonomous. In other words, medical collaboration in the management of diabetic patients took the form of sequential rather than collective coordination:
They refer the patient to us, but that’s all by fax. Then we send them a summary. So we don’t actually talk to them; we rarely do. There isn’t a lot of telephone contact or personal contact. It’s mostly through the diabetes centre. The diabetes centre is the platform. So we receive the requests, we see the patients, we return a consultation report or a course completion report. (Specialist)
In fact, structures have greatly influenced medical clinical practices: while the creation of multidisciplinary teams for a diabetes program led by internists has enhanced the clinical support offered to GPs, it seems to have had deleterious effects on decision-sharing by physicians. The internists, who can draw on wide-ranging professional expertise and are therefore able to perform a comprehensive evaluation of the patient’s state of health, do not always see the usefulness of GPs’ involvement in clinical decision-making:
We are autonomous, due to the fact that we have a really good profile of the patient. (Specialist)
These practices were also consistent with the actors’ perception of the degree of complexity involved in diabetic patient management. When questioned on issues of patient management, most physicians stressed problems such as patients’ compliance with treatments, changes in daily habits, and risks of complication, which require systematic follow-up. Therefore, the juxtaposition of different types of medical expertise at the point of decision-making was not perceived as problematic by physicians. GPs generally conceive this sequential coordination with specialists as the optimal utilization of all available medical expertise for the sake of the diabetic patient.
How did the perception of medical collaborative practices influence the structures at the local level?
Ultimately, however, the scant information provided by the Center led to dissatisfaction on the part of the family physicians about the quality of communication. The family physicians also found that the two programs originally offered by the Center were not a good fit for all of their patients; for some, a simple referral to a specialist might have been be more suitable. Therefore, they asked for, and obtained, changes to the Center’s operating methods (structures) with respect to the transmission of information (systematic forwarding of patients’ progress notes to the referring physician) and the available services (possibility of medical consultation only: “à la carte” services). At the same time, the outreach efforts by the Center’s physicians led to the realization that very few of the diabetic patients seen at hospital emergency rooms were being referred to the Center. New mechanisms for liaising with emergency rooms (through the nurses, a change in structure) and stepped-up awareness-raising efforts directed at emergency room physicians were therefore proposed. This initiative therefore helped changing the practices of family physicians working in the emergency room, increasing referrals from that source:
At the end of 6 months, we didn’t have any patients from the emergency room … after a year, just as many diabetic patients were going to the hospital. So I asked to make a presentation at an ER meeting, I went to see them and I said … many people said, what’s that? What’s the Diabetes Centre? Well, I said, we’ve been around for a year. I said, you have to fill out the yellow sheet. What yellow sheet? So we realized they didn’t know about it in the emergency room. So we did more education, reinforced it. We involved the liaison nurse in the emergency room. (Internist responsible for the Center)
Period #3 (2011–2015)—capitalizing on learning and institutionalization of medical collaboration models
As they engaged in collaborative practices at the organizational, inter-organizational, and clinical levels, physicians as well as medical heads of the Center gained considerable insight into managing diabetes patients, in addition to organizing and managing integrated care programs. Such a learning process had a great impact on subsequent structuration processes, leading to the extension of the Center clinical activities and responsibilities. Similarly, collaboration practices at the inter-organizational level, initially stemming from regional structures, also resulted in several diffusion and consolidation initiatives which contributed to institutionalizing the new model of medical collaboration.
How did the evolution of practices reinforce capacities which yielded to the development of new structures at the local level supporting medical collaborative practices (2011–2015)?
The improvements to communication mechanisms helped the referring family physicians develop their expertise in diabetes treatment and management:
I ask a question and I get an answer. “OK, great, that makes sense.” I see the patient doing well, and the next time I get something similar, maybe I won’t ask the question. I’ll try to apply what I learned from the other consultation. (Family physician)
As this process gave them greater independence, the family physicians ended up referring slightly fewer patients to the Center (a change in practices), freeing up resources for the management of other chronic diseases:
You know, before, there were training courses every week … Now, there are fewer courses … I think that was necessary because we wanted to include COPD, and we wanted to include osteoporosis, without having much more money. (Internist responsible for the Center)
At the same time, the fact that the Center’s specialists were involved in the various management and coordination bodies created in conjunction with the program helped them develop skills and expertise in the organization of service delivery:
So, it got me interested and gave me the know-how to develop other similar projects. I have lots of them in mind. Honestly, I think this care model should be applied to many other chronic diseases … Clearly, where I learned the most was at the organizational level. I know which doors to knock on now, and you know, when you’ve never done this type of project, it’s hard to imagine. (Internist responsible for the Center)
The new capabilities and resources enabled the Center’s local coordinators to propose a hypertension follow-up project. Based on the same criteria as those applied when the original pilot project was approved, the Regional Agency granted funding for the hypertension project and worked closely with local actors to establish the program’s precise characteristics, thereby strengthening clinical/administrative collaborative practices. The process yielded changes in HSSC-A’s range of services (structures). The addition of health services also produced changes in clinical practices.
Around 2012, the Center’s medical head started the development of a pilot project for osteoporosis management which likewise drew on what had been learned. To handle the expansion of clinical activities, the head of the Center decided to recruit more endocrinologists. This provided an opportunity to review the division of responsibilities among the Center’s physicians. Henceforth, the internists would be less involved in following diabetes patients; that task was assigned more to the endocrinologists. As a result of the change, there was an increase in medical monitoring of patients with the greatest needs:
Well, in fact, as soon as we arrived, we realized when we gave 3-day course at the diabetes centre—we had a clinic on Tuesday, it was just when we gave the course and that’s what the other internists did—so the internists would see their patients about once every six months because they didn’t do so many courses and clinics. But we said, why can’t we do this clinic every week, the waiting lists are terrible. So we said, we have all the resources here, so if you agree we could each do a clinic. (Endocrinologist 2)
How did diffusion activities, and the role played by the regional agency, shape the institutionalization of the tested collaborative models (2012–2014)?
Shortly after this addition to the Center’s activities, the Regional Agency set about disseminating, in collaboration with the HSSCs, the models produced by the pilot projects that were deemed “successful,” as had been agreed at the outset.
In the specific case of the Center, the dissemination requirement led its staff to take a series of actions to publicize the Center outside the HSSC:
My teams went all over to make presentations at various HSSCs. We invited people from different HSSCs to come and visit us. So, there really was mutual collaboration, because the mandate we were given was: OK, yes, we’re giving you money but it comes with a responsibility to transfer knowledge within the Montreal area. (Manager, HSSC-A)
By virtue of its presence on HSSC-A’s local evaluation committee, the Regional Agency was aware of the improvement in the diabetic clients’ state of health shown by the monitoring indicators:
Any program that is implemented must be evaluated. So, for example, we defined indicators at the beginning. A study is a study. So, if you transfer it to real life, to the real world, basically … to a natural context, will it still give us the expected clinical results? So from the beginning, we set up evaluation methods … (Manager, Regional Agency)
The Regional Agency then decided to make the locally tested model a regional standard (institutionalization of the model). The model was incorporated into the regional action plan for the management of chronic diseases (structure). The Agency played an active role in the dissemination and implementation of the model in the various HSSCs by adjusting the model’s parameters to conditions in each setting and supporting its implementation with financial contributions:
All of our HSSCs have a diabetes project, on the same model as HSSC-A. So, the life habits program is being developed everywhere. The difference is that the life habits program is not necessarily offered at the HSSC. Sometimes it is offered at the primary care hospital. Because there is no structure. They don’t have a specialist at their HSSC … because certainly, ideally, we would just have a coordinating role, making sure it’s more or less the same thing at HSSC-A and HSSC-C. But they don’t have the time, they don’t have the resources, so we’re not just coordinating anymore. We work hand-in-hand, we have meetings, joint working sessions. (Consulting professional, Regional Agency)
Each HSSC on the Island of Montreal adopted the model. The Regional Agency then decided to create communities of practice, new structures that include representatives from the various HSSCs. These new structures in turn fostered clinical/administrative collaboration among HSSCs, which contributed also to the institutionalization of medical collaborative practices:
So we set up professional committees: nutritionists, nurses, kinesiologists, precisely to harmonize tools throughout Montreal. For example, harmonizing the referral form. So now we have a single referral form, everyone has the same one. For the general practitioner, the form is always the same no matter where he is … (Manager, Regional Agency)
Discussion and conclusion
The ultimate goal of this investigation was to help shed light on the very difficult process of collaboration between family physicians and specialists working at different levels of healthcare delivery. Medical professional logics clearly emphasize clinical expertise and professional autonomy. To trigger change toward collaboration of any kind in such an institutional context, powerful jolts appear necessary (Meyer et al., 1990). In the case here reported, and due to the publicly funded healthcare context in which it was conducted, this external jolt was provided by a health reform that sparked important structural changes at the provincial, regional, and local levels. In collaboration with administrators, entrepreneur physicians turned these changes in the environment into an opportunity to improve practices and gradually introduce new forms of clinical/administrative collaboration between GPs and specialists. Given the prevailing situation before the change—two “solitudes” in coexistence—these new practices were perceived as innovative by many actors in the field.
This being said, our analysis of these new forms of collaboration reveals—and this is an important finding of our empirical investigation—that the intensification of collaborative practices at the administrative level does not necessarily entail greater shared decision-making in patient management. The medical collaboration examined here basically consisted in the clarification and complementarity of physicians’ perceived respective clinical roles.
From a political perspective, the forms of collaboration that were adopted appear to represent a win-win strategy for physicians. In the context of resource scarcity, the existence of a new diabetes referral center encouraged collaboration among primary and secondary levels of healthcare, offering diabetic patients a series of new services delivered by an educational nurse, a nutritionist, and other professionals, and allowing physicians to focus on their role as medical experts without losing control over their respective practices. This approach also seems to have been based on the fact that the degree of complexity of the clinical activity, as perceived by the physicians, did not warrant more extensive collaboration in their view. Said differently, it seems that the forms of collaborative practices developed in the context of our study rest on a limited perception of resources dependency. The theory of situatedness of action (Suchman, 1987), which argues that an action’s course depends on contextual circumstances and is influenced by actors’ interpretations, is also consistent with the concept of actors’ reflexivity in Giddens’ structuration theory and further contributes to the validity of our interpretations in this regard.
A political reading also helps explain why the endocrinologists were originally opposed to the proposed collaborative model and did not buy into the change. As we have seen, the endocrinologists associated with the HSSC disapproved the proposed structure, according to which the Center was managed by an internist, because they perceived it threatened their power position. This finding further corroborates that battles over professional jurisdictional boundaries can hamper the development of collaborative practices in particular contexts. It is interesting to note that endocrinologists did play an important role in the collaboration consolidation phase—in Giddens’ terms, this shift can be understood as an unexpected consequence of the action.
Furthermore, drawing upon Giddens’ concept of duality of structures, our analysis allowed us to shed light on the processes involved in the development of medical collaboration. We therefore were able to elucidate how the application of rules of signification (population-based approach, CCM model) and rules of legitimation (e.g. assignment of new roles to the Regional Agency and the HSSCs), combined with domination resources (e.g. physician remuneration methods, Agency funding, new modes of decision-sharing through the creation of clinical/administrative committees and multidisciplinary healthcare teams), have affected collaborative practices.
Moreover, in accordance with Giddens’ theory, our analysis showed how the reflexivity of actors is an essential transformative element of social processes. In fact, the actors’ self-reflection on their own practices made them aware of the limits of the developed collaborative structures. In the first instance, this led them to review the Center’s operating methods and then to expand its services. Therefore, we argue that one of the most original findings of this investigation relates to the impact of knowledge dynamics, that is, individual and collective learning on the development of medical collaboration across levels of care. It appears that the nature of the structures that were created—such as the use of indicators to evaluate the pilot projects and the creation of clinical/administrative committees combining different types of expertise—promoted collective learning, confirming once again that such learning requires structures that can coordinate the learning of interdependent actors (Håland et al., 2015). Furthermore, as suggested by some (e.g. Nonaka et al., 2001; Nonaka and Takeuchi, 1995), the creation of knowledge has been favored by some conditions such as (1) autonomy, which has increased the chance of introducing unexpected opportunities and motivated organizational members to create new knowledge; (2) creative chaos, that is, interaction between organizations and their environment that has encouraged breakdown of routines; and (3) requisite variety, by providing equal access to information through the system which has helped to cope with many contingencies. It should be noted here that collective learning was not limited to local actors. In effect, as a result of its participation in various local initiatives, the Regional Agency was able to draw lessons from experiments in different territories and then impart the benefit of such learnings to all health centers of the region.
Prior work has not adequately explained how medical collaborative practices become institutionalized. Once again, we find that political processes are at the heart of the institutionalization processes. The Regional Agency, which played a major role in disseminating the model, relied on domination resources (incentives) to encourage all the health centers on the Island of Montreal to change their diabetes management practices. In its dissemination activities, it also used the results of the pilot project as a domination resource to delegitimize the old ways of doing things and legitimate the new ones. It would appear that learning dynamics also contributed to the institutionalization of the new medical collaboration model: as a result of the learning by the regional communities of practice, the HSSCs gradually adopted the same work tools, which encouraged the family physicians to take ownership of the tools. As they work in different territories on the Island of Montreal, they were particularly pleased by the harmonization of working methods.
We should also stress another factor that contributed to the institutionalization of the medical collaboration model developed by the health center under study: the adaptation of the model to conditions in each territory. In short, the Regional Agency can be said to have played the role of a “linking organization” (Heinze et al., 2016):
Linking organizations purposefully, rather than inadvertently, connect actors within the community around a particular issue, interface between the broader field and the community levels. Linking organizations not only create local networks, they translate field level changes to the community and thus shape local organizations’ responses to institutional demands. (p. 5)
We consider this role to be essential for the development of medical collaboration between different levels of care insofar as it supports physicians who are heavily invested in their micro-clinical work and therefore need additional resources (expertise, time, etc.) in order to renew their practices.
The results of this study make a number of important contributions. At a theoretical level, it stresses the key role played by actors’ cognitive dynamics in the development of medical collaborative practices, supported by several structures involving multiple actors. As highlighted by our review of the literature, these dynamics have received scant attention. What is more, our work has also shed light on an understudied phenomenon, namely the institutionalization of these collaborative practices at the field level. Future research should however further examine how the clinical context (i.e. complexity of patients’ health needs) influence intra-medical collaboration.
At a more practical level, our work suggests that the development of medical collaborative practices requires a close relationship between regulatory agencies (regional authority) and local health organizations, as well as between clinicians and administrators. Furthermore, it appears that actors should need to renew their ways of doing to support collective learning. For instance, regulatory agencies could go beyond their traditional role of formal authority and also behave as change support agents, denoted here as “linking organization.” Some physicians could also assume more important leadership roles and further get involved in services organization. What is more, the coordination of these interdependent actors’ learnings asks for the mobilization of “tools,” such as evaluation devices, the implementation of clinico-administrative committees, and the development of knowledge transfer activities that support actors’ reflexivity.
As any empirical investigation, this work presents some limitations. Having been conducted in a publicly funded Canadian healthcare context, where provincial jurisdictions have control over health services organization and management, and where physicians are nonetheless autonomous entrepreneurs, caution should be recommended in regard to the extrapolation of its results to very different healthcare delivery environments. What is more, the study was carried out in a local territory with a high reputation of creativity and innovativeness in the implementation of new modes of healthcare delivery at the provincial level—whereas this feature was fruitful concerning the richness of data gathered, the application of knowledge generated in less resourceful contexts should be made with prudence. All that said, the way in which we conducted our analysis enabled us to provide a sound understanding of collaborative practices, and how they reproduce or change structures over time. The validity of the study basically relied on the methodological coherence we reached between research questions and the selected methods, the triangulation of data sources, member check, a continuous process of data collection and analysis, and the involvement of all the members of the research team in the interpretation of findings (Morse et al., 2002).
In conclusion, our work provides an empirical understanding of the emergence and development of new professionalism models, notably organizing professionalism, which considers that organizing is an integral part of professional action (Noordegraaf, 2015). While we agree with Noordegraaf that evolution towards this new professionalism model demands upstream actions such as physician training and socialization, our investigation also shows that the transformation of medical practices can also be affected through the introduction into the system of new structures which, over time, alter power relationships between the actors and enrich knowledge and practice. On the basis of the strong theoretical underpinnings adopted over our whole research period (Morse et al., 2002), the transferability of knowledge that we have generated will be particularly suited to publicly funded and managed institutional healthcare delivery systems where physicians enjoy a great deal of professional and managerial autonomy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research has been funded by the Canadian Institutes of Health Research.