
Abstract
Young people’s experiences of living with a long-term health condition have been largely investigated from the perspective of developing autonomy and optimal self-management of treatment regimens. Little existing research explores how young people adjust to the experience of chronic illness within everyday social contexts. Drawing on sociocultural theories of healthism, in this article, we examine the everyday strategies students employed to manage their health condition at university. Data were drawn from a qualitative study with 16 undergraduate students in Australia. Findings from interviews highlight how participants took up discourses of the (hard-working, diligent) Self to discursively position themselves as ‘health conscious’ and ‘in control’. This positioning was maintained through separating the controlled Self from the (uncontrollable) body. The unpredictability of the body posed a threat to young people’s abilities to maintain control and denied them opportunities to exercise personal agency. Yet, participants also described a number of subversive strategies in order to take back control and resist the experience of ill health. These potential agentic practices often held unintended consequences, including loss of optimal medical control or (self) exclusion from university life – offering new insights into the differing ways young people concomitantly take-up, rework and resist the pursuit of healthism to ‘successfully’ manage their health conditions.
Introduction
The chronic illness literature has offered significant contributions to understanding the lived experiences of long-term health conditions (Bury, 1982; Charmaz, 1995; Williams, 2000). Drawing on Bury’s notion of biographical disruption, much of this research has focused on the difficulties of adjusting to an altered sense of Self and shifts in individuals’ (present and future) biographies (Charmaz, 1995, Larsson and Grassman, 2012) and understanding varying coping, strategies and styles of illness management (Bury, 1991). The experiences of young adults are less well described (some notable exceptions are discussed shortly), despite increasing prevalence of longer-term conditions in young people (Australian Institute of Health and Welfare [AIHW], 2011; Shah et al., 2019). Some literature questions the relevance of ‘disruption’ to young people and considers possibilities for biographical continuity as conditions identified earlier in life become normalised (Williams, 2000; Williams et al., 2009). Other research suggests a more dynamic picture, with possibilities for both continuity and ‘crises’ as young people navigate their (health) identities in ever-changing social conditions (Bray et al., 2014). These fluctuating and less certain experiences of (ill) health shape, and are shaped by, the contexts in which young people live – presenting different life trajectories and forms of illness management (Bray et al., 2014; Spencer et al., 2018).
In this article, we aim to take forward understandings of young people’s experiences of chronic illness, with a particular focus on the university context. Entering university reflects an important transition point for many young people in contemporary society and offers a key site for examining how young people (re)negotiate their health and social identities. However, the experiences of university students with a chronic health condition have been relatively underinvestigated in research to date (exceptions include Balfe, 2007, 2009; Couzens et al., 2015; Grimes et al., 2019; Saunders, 2011) with much of the extant research focusing on the high school context (Gabe et al., 2002) or transitions within the healthcare setting (Fegran et al., 2014). We have reported elsewhere on how chronic illness impacts on university students’ health identities (Spencer et al., 2018). Here, we draw on sociocultural theories of healthism, to advance knowledge of young people’s agency in the management of their conditions. In doing so, we pay particular attention to the differing ways students take up discourses of the body/Self to both accommodate and resist the experiences of ill health and ultimately, find ways to take back control of their health and academic studies.
Young people and the experience of chronic illness
Contemporary literature on young adults and chronic health conditions heavily focuses on the autonomous (responsible) self-management of their illness (Newman et al., 2016). Underpinned by normative developmental frameworks, research and health practice typically prioritise achievement of optimal medical control. Lack of control is often explained by reference to young people’s deficits in knowledge or (wayward) attitudes towards the importance of compliance with medically advised treatment or lifestyle adjustments. Thus, much of the health research focuses on the development of behavioural competencies to optimise adherence to medical regimens within the context of transition from paediatric to adult health services (Newman et al., 2016). However, by locating the ‘problem’ of young people’s (lack of) control over their condition(s) within behavioural frameworks, this individualised approach downplays the profoundly social elements of their transition and health-related experiences, including the differing frames of reference young people draw upon when managing their health (Spencer, 2013).
Research to date highlights the complexities of how young people navigate chronic illness (and its impacts) in everyday life – including impacts on their autonomy, social identities and experiences of stigma. This includes how young people draw on multiple, and sometimes competing, rationalities when seeking to balance optimal medical control of their health conditions, while also upholding authentic and valued personal and social identities. For instance, while there may be normative expectations and logics about ‘good self-management’ (e.g. taking an active role in managing their condition, compliance with treatment regimes and engaging in healthy lifestyle behaviours), young adults may also draw on alternative rationalities to uphold a preferred social identity (Balfe, 2009; Bray et al., 2014; Harries et al., 2019; Monaghan and Gabe, 2015).
Heaton et al. (2016), for example, highlight the ways in which young adults differentially prioritise the (medical) demands of their condition with preferred everyday activities, and through developing a conceptual distinction between (medical) control and (personal) autonomy. From this perspective, young people’s apparent ‘selective’ engagement with medically prescribed regimens can be understood as part of their efforts to retain autonomy over their lives (rather than maintain control over health). Indeed, maintaining optimal medical control may compromise autonomy to navigate a ‘normal’ life (see also Balfe, 2007, 2009; Harries et al., 2019; Saunders, 2011). Other research draws critical attention to the fluctuating nature of ill health and how such uncertainty can challenge opportunities for young people to enact preferred health identities (Barned et al., 2016; Spencer et al., 2018), with impacts on their mental health and emotional well-being (Wilson and Stock, 2019). The unpredictability of the body thus becomes a crucial site for (individual and social) control. Other research shows how young people’s management of their chronic illness may be shaped by their experiences of stigma, and in these contexts negotiating social relationships is critical to how they manage their illness experience. Saunders (2014) draws on Goffman’s stigma to examine how young people with inflammatory bowel disease actively manage the (stigmatising) impacts of their condition on their (personal and social) identities. In this context, establishing and maintaining a preferred (morally sanctioned) identity become priority and the locus for ‘control’.
The body and Self in the everyday management of chronic illness
Healthism has long recognised and reported on the processes through which modern society comes to denote the body as a ‘project to be continually worked on and accomplished as part of an individual’s self-identity’ (Shilling, 2003: 5). Drawing on Foucauldian notions of governmentality and technologies of the Self (Foucault, 1988), critical scholarship exposes the ways in which dominant health discourses come to define and (morally) sanction socially and culturally appropriate bodies, which in turn proscribe the range of preferred (individual) actions on, and over, the body (Crawford, 2006; Lupton, 1995). In the context of neoliberalism, engaging with ‘body-techniques’ (Williams, 2001) is branded as a route to, and evidence of, individual ‘empowerment’ and the successful uptake of (and commitment to) the pursuit of health (Lupton, 1995). Yet, these ‘individualised’ health practices are located within, and endorsed by, social institutions that privilege knowledge from health risk experts – producing powerful social pressures to conform to dominant body ideologies (Higgs, 1998; Lupton, 1995). Deviations from these body norms (and the strategies to achieve these) denote the (lack of) moral character of the individual – ultimately exposing them to blame, shame and stigma for their personal failings to uphold and enact the healthy body ideal (Galvin, 2002; Shilling, 2003).
The chronically ill body suggests non-conformity to these socially proscribed normative body ideals and the individual’s failings to uphold health (Crawford, 2006; Higgs, 1998; Lupton, 1995). Research investigating adults’ experiences of chronic conditions highlights the self-care strategies individuals adopt to circumvent personal culpability for their ill body (Clarke and Bennett, 2012). Careful monitoring of symptoms, compliance with treatment and lifestyle modifications become active strategies of the ‘will to health’ (Higgs et al., 2009: 687). In her examination of medically undiagnosed symptoms, Nettleton (2006) revealed how individuals feel (socially) compelled to explain their illness by drawing attention to the shortcomings of their body (rather than themselves). Referencing biology as the origin of disease and describing the body as foreign, unfamiliar and outside (individual) control enable individuals to (morally) distance themselves from the deviant ill body. Yet the alien, unpredictable body can threaten opportunities for self-care and destabilise the sense of Self. Charmaz’s (1983, 1995) research highlighted how individuals can feel ‘let down’ by their bodies and thus distance themselves from their illness to uphold their preferred (social) identities. Other research reveals individuals’ preference for maintaining control over the ‘normal’ Self, rather than the (largely uncontrollable) body and related symptomatology (Balfe, 2007; Townsend et al., 2006). Preserving the Self thus shapes the forms of self-care used in response to symptoms (Barned et al., 2016). This apparent decoupling of the body from the Self has been challenged in other literature, which suggests a more complex relationship between the body/Self (Bendelow and Williams, 1995; Turner, 1992). In relation to pregnancy, Carter (2010) provided useful insights into how women’s shifting positions of feeling both in and out of control can disrupt their sense of self and opportunities for agency. Charmaz (1983) argued that the body and the Self are always intricately linked as embodied experiences of shame, guilt and blame dictate the affective responses to, and experiences of, ill health (Sointu, 2016).
Despite these significant advances to the scholarship on adults with chronic illness, relatively less is known about how young people respond to, and experience, chronic ill health in everyday social settings, including how these experiences shape health practices and forms of agency. Balfe (2007, 2009) highlighted the tensions young people experience when seeking to balance their public and private self and body. Similarly, Heaton et al. (2016) considered how young people aim to ‘strike a balance’ between control and autonomy. What is less well examined are the ways young adults take up (or not) dominant ideologies of health and the body to manage their health conditions. Drawing on sociocultural theories of the body and healthism, we thus aim to contribute to this less explored terrain and advance knowledge of how students manage their chronic health conditions at university and consider the resultant implications for their agency.
Methodology and methods
This article draws on the findings from a qualitative study examining the experiences of university students’ living with a chronic health condition (Spencer et al., 2018). The study was underpinned by a broadly constructivist framework, which privileges the importance of meanings attached to interaction and the co-construction of knowledge (Denzin and Lincoln, 2017). Data are thus co-produced relationally between the interviewer (a fourth year undergraduate Honours research student) and interviewee, and interpretation reflects the researcher’s own positionality within the narrative (Riessman, 2008). We reflect on this relationship, and its impact on data generated, in our final discussion.
Study context and participants
Data were generated through in-depth interviews with students attending a large Australian university. Participants were informed about the study and recruited via posters displayed around campus and electronic advertisements sent via email. Recruitment materials highlighted the specific focus on current university students who have a medically diagnosed physical chronic health condition. Because the study was exploratory in nature, a convenience sampling strategy was used (the limitations of which are considered in the discussion). All students who expressed an interest in the study (via email) and who met the inclusion criteria (e.g. a current university student with a medically diagnosed physical health condition) were subsequently interviewed by M.R. The sample (n = 16) included 13 women and 3 men, aged 19–32 years who self-reported a range of conditions, such as diabetes, thyroid conditions and epilepsy (see Table 1).
Participants.
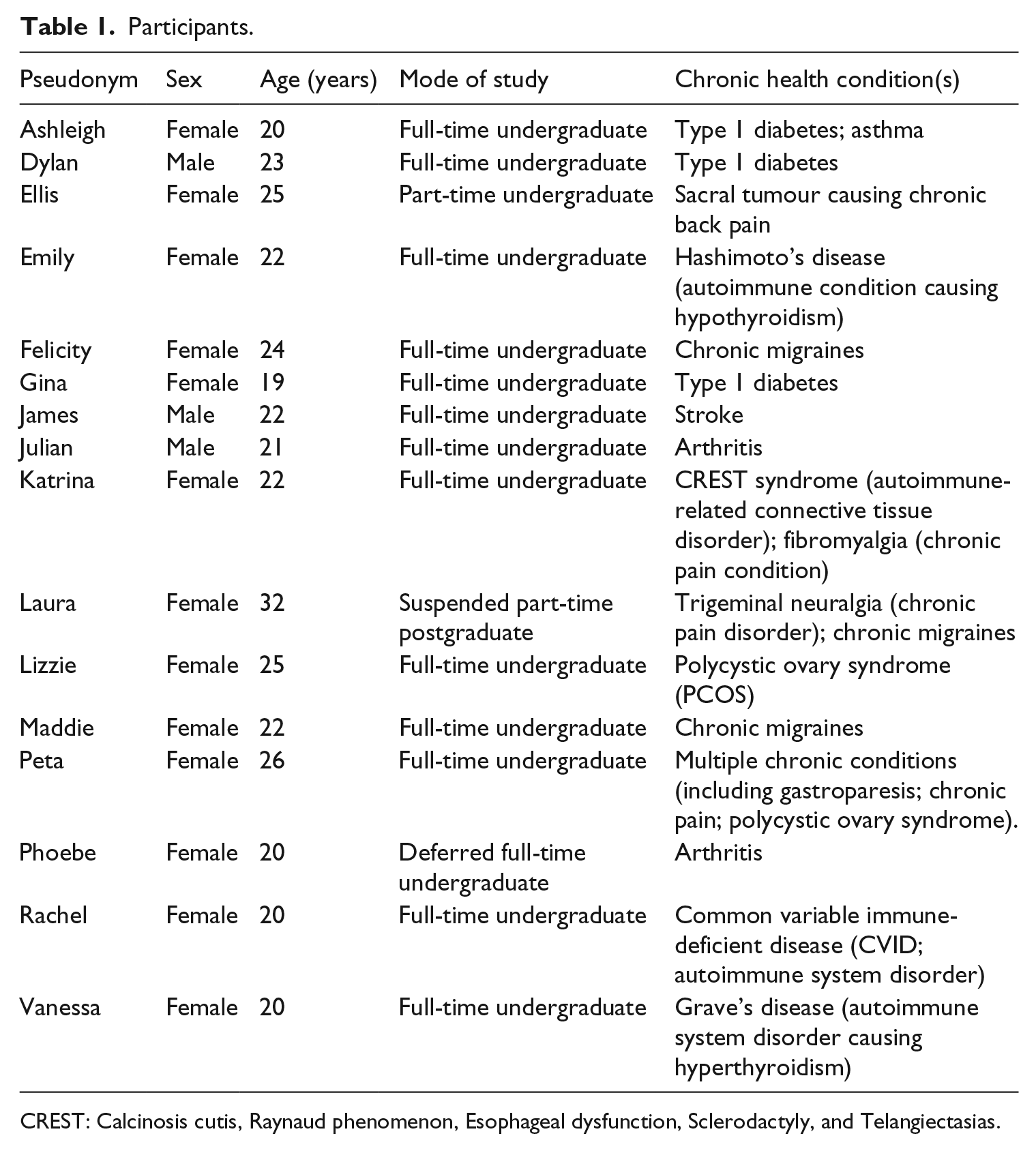
CREST: Calcinosis cutis, Raynaud phenomenon, Esophageal dysfunction, Sclerodactyly, and Telangiectasias.
Ethics approval was granted by the University of Sydney’s Human Research Ethics Committee. Written informed consent was secured at the start of each interview and included a discussion with participants about the study and their involvement. Respondents were advised that participation was entirely voluntary and that they could withdraw at any point.
Data collection
Individual semi-structured interviews were conducted in a campus meeting room by M.R. Potential participants emailed M.R. to express their interest in the study. At this time, further information was provided to the student and a convenient date and time arranged for the interview. Broad topic discussion areas were identified from the literature and included participants’ experiences of managing their health condition(s); the types of support they seek out or engage with and their experiences of university, with a focus on how this context can aid or hinder management strategies. The discussion guide was piloted prior to use and contained a series of open-ended questions and prompts to facilitate in-depth discussions. The semi-structured nature of the interviews enabled participants to identify and discuss the issues most relevant to them, while maintaining a degree of consistency across interviews to ensure comparisons. Interviews ranged between 20 and 70 minutes and were audiorecorded with participants’ consent and transcribed verbatim by a professional transcription service. All transcripts were fully anonymised by removing any identifiers and using pseudonyms. All data were securely stored in line with ethical and data protection requirements.
Data analysis
Inductive thematic analysis was conducted through a multiple-stage iterative process by the authors (Green et al., 2007). Transcripts were carefully reviewed for accuracy by M.R. and then re-read to enable identification of salient codes emerging. Emergent codes were then scrutinised and synthesised into broader topical categories. Categories highlighted key priorities and concerns for participants, such as upholding a positive health identity, managing the invisibility of symptoms and grappling with university processes. Finally, categories were interrogated to consider patterns, inconsistencies and meanings across and within the data to identify core thematic areas that capture participants’ perspectives and experiences, while acknowledging and attending to the ways in which the interviewer participated in the construction of particular narratives (reflexivity) within the context of an interview (Riessman, 2008). At each stage of the analysis, the authors met to discuss and debate conceptual categories and how these may help to explain the data.
Findings
The analysis revealed some of the distinct challenges participants experienced while managing their health condition at university. Working through such difficulties required diligent and continuous attention by the individual in order to minimise adverse (health, social and academic) outcomes. Respondents described the strategies they used to manage both themselves and their health, with a particular focus on the control of undesirable symptoms. Maintaining control was, however, threatened by the unpredictability and uncertainty of when (and how) ill health could strike. Significant disruption to participants’ everyday lives unfolded during times when their body ‘took over’. In the analysis that follows, we highlight how these young people sought to take back control of their bodies and ultimately resist the experience of ill health.
Managing the Self and (ill) health
When talking about their chronic condition(s), participants placed particular emphasis on their abilities to manage and control their health, frequently presenting themselves as being ‘good self-managers’ (Ellis et al., 2017: 25). Participants described being proactive, organised and ultimately in control of their health.
I’m quite proactive about trying to do the best I can [. . .]. For the most part I have learnt to manage things and take control. (Ellis, Sacral tumour) I’ve always been very in control of my condition. I decided I wanted to do that [. . .]. I’m the person who does primarily manage it. I had to learn how to manage it and what I have to do. (Ashleigh, Diabetes)
Respondents reported a variety of ways they had ‘learnt to manage’ their health conditions. First, they highlighted how they sought to (better) manage themselves through being hyperorganised and prepared for times of ill health. Some participants described how they would plan ahead for assignments or capitalise on ‘good’ (read healthy) days to meet academic requirements. Others reported working during the commute to university or adjusting their routines to accommodate (the limits placed upon them by) their condition(s). Learning to manage themselves was closely tied to knowledge about (the limits of) their bodies.
And then the study and academic side of it?
This semester, now that they’ve dropped me back down I’ve found it more challenging, I just need to be aware of my limitations a bit more. Previously if I had to get my work done I’d stay up and I’d study till 11, 11:30. [B]ut now I just need to manage myself a bit better [. . .] I know I need to go to bed at 10, 10:30 if I want to get up and go to uni the next day, because I know I need that sleep. [I]t has kinda forced me to be a bit more organised with my work. (Emily, Hashimoto’s Disease)
I’ve just gotten used to being ridiculously organised. I try to get my assignments [done] early in case I get sick. . . (Katrina, CREST Syndrome)
Second, participants described the active management of their condition, particularly how they had become more ‘health conscious’. Engaging with conventional forms of health promotion, such as maintaining a healthy diet and regular exercise, was often cited as evidence of their conscientious management of health.
I’ve got insulin resistance but I keep that really rather under control, my blood sugars have been great, hormones have been normal, diet, exercise is immaculate. (Peta, multiple conditions)
Could you tell me a little about your health?
I was diagnosed with diabetes when I was 12 [. . .] I find having diabetes makes me be on the ball about my health and you have to consciously think about what you’re eating [. . .] you’re thinking about your whole meal plan [. . .]. I’m very conscious about what I eat and exercise. (Gina, Diabetes)
These young people’s accounts of their health-enhancing strategies can be understood as part of their uptake of, and commitment to, dominant discourses of self-responsibility. As described, establishing such forms of (positive) self-care and ‘autonomy’ are often the target of critical transition phases in the management of chronic conditions. This proactive (individual) responsibility was well-recognised by participants themselves.
I’m reasonably proactive about it, or at least I think about it a lot. I mean since I became an adult and phased out of the children’s healthcare system. (Dylan, Diabetes)
Diligent forms of self-management extended to information-seeking and the active investigation of their health conditions. Respondents described how attending university provided an important opportunity to learn more about their health conditions – often reporting to have undertaken their own research on the causes, symptoms and treatments of their condition. This ‘research’ enabled some young people to pursue a range of alternative strategies and lines of treatment.
Is there something about university that has affected your condition?
The education because I did a medical science degree, you learn about some medications, about pharmacology. I also learnt about how the body works; the structure of the spine and the muscles through anatomy. I think that’s actually come to my advantage because I know which muscles I need; for example, if it hurts and you know pain killers. I learn which ones do well for this and suit that. (Julian, Arthritis)
Learning more about their health conditions, however, did not necessarily mean greater compliance with medical advice, but instead aided respondents to engage in a form of ‘experimentation’. Participants described how they worked through a process of ‘trial and error’ to find the best solutions for them, which included manipulating their medications, modifying their diet and exercise (cf. Heaton et al., 2016). Others described seeking out advice from allied health professionals, or the use of complementary forms of therapy.
I’ve seen physio’s and osteo’s [. . .] a naturopath and a nutritionist and I’ve tried to cover everything [. . .] I’m still really trying to figure out what’s causing it and still in the process of seeing different people and, trying different things [. . .] I’ve tried some things but [. . .] there’s nothing I take regularly, occasionally I would take over the counter stuff in the morning [. . .] it’s been like two years of still trying to figure out [. . .]. (Maddie, Grave’s Disease)
Despite positively describing their experimentation with health treatments, opportunities for successful management were severely compromised by the multiple demands placed on participants as a university student with a chronic illness. Respondents talked at length about the intensity of academic workloads and how financial and social commitments exacerbated (and were exacerbated by) their health conditions.
Could you tell me what the hardest thing about uni has been for you?
Hardest thing I think, balancing my health with trying to get my studies done [. . .] [T]rying to balance medication, the attacks, and doing work the way I used to, I used to be able to come home, sit down, work to whenever, and now it’s like if I stay up too late, I know that that could interact with my medication [and] if I forgot to take my medication, I could feel dizzy [. . .] I feel like I’m working extra hard just to try to get to a place where I was at before. (Laura, Trigeminal Neuralgia)
The workload is intense and does get more intense [. . .] I think the hardest thing has been managing the workload with work with social life with chronic illness. (Ashleigh, Diabetes)
Balancing competing academic and health-related demands was a clear struggle for some, particularly during times when (debilitating) symptoms surfaced. Despite their best efforts to ‘stay on top of everything’, participants highlighted times when they had no choice but to be guided by (the limits of) their bodies.
Losing (bodily) control – managing the unpredictability of ill health
While foregrounding their strengths at being hyperorganised, well planned and in control, interviews also revealed how the body could ‘let them down’ and dictated what could be achieved. Loss of control over the body presented everyday struggles and future uncertainties – leaving participants little option but to ‘give in’ to the (unpredictable) demands of their condition.
It got to the point where I was having episodes every day and I just could not function [. . .]. My work is affected, my home life is affected, whether I can go and see friends or not [. . .] It all just snowballed and hit me and my health just plummeted. I was having attacks all the time. I went to the hospital because it lasted up to four days, without break [. . .]. I could barely work; I couldn’t study. (Laura, Trigeminal Neuralgia)
Struggling to function was particularly evident for those with autoimmune conditions, which triggered (unpredictable and debilitating) chronic fatigue and pain. During interviews, these participants discursively disconnected their (uncontrollable, alien) bodies from the Self, reporting how they ultimately had to do (unwanted) things on ‘their body’s terms’.
You feel like your body’s been taken out of your hands. [I]t makes you do things to yourself that you don’t necessarily wanna do. There are some exercises on the foam roller that make me cry because they really, really hurt [. . .] [But] when you have a chronic illness, it needs to be on your own terms, sorry on your body’s own terms because they’re very separate. (Katrina, CREST Syndrome)
This uncertainty about when (and how) the body might dictate required respondents to frequently justify their apparent disengagement in academic and social life and crucially, to ensure friendships were not compromised. Negotiating social relationships and concerns about letting others down featured strongly in participants’ accounts. For some, this included decisions to actively avoid or exclude themselves from social events.
How has living with your health condition affected your experiences at uni, socially?
I didn’t really go out much, I didn’t really leave the house, I just didn’t have the energy to do it [. . .]. I just tell them, I just can’t come, I’m literally too tired to come out. (Emily, Hashimoto’s Disease)
The felt need to continuously explain themselves and their (lack of) engagement extended to their academic studies and participation in university life more broadly. Keeping commitments, submitting assignments on time and attending classes all became tricky when the body was unwilling. Additional (individual) effort to manage both university and their health was needed. However, on many occasions increased effort could not match or overcome what participants described as an inflexible university environment.
We would have six hours of straight class, there was no break in between [. . .] and by the end of that day I would always have a migraine. I was feeling very ill, so that just rules out getting anything done for the next night for your lab the next morning, I would be sick on the train home, I couldn’t drive because I’d be vomiting from the pain. (Felicity, Chronic migraines) Your disease doesn’t follow a timetable seems a little bit dumb to have such a rigid structure around something that is completely and utterly unstructured and unexpected. (Peta, multiple conditions)
While (rigid) academic demands highlighted the unaccommodating conditions and effects of the social context, respondents often attributed difficulties to the failings of their own bodies. Indeed, while social commitments with friends reflected the felt pressures not to let others down, during discussions about their academic studies, participants revealed how they sought to not let themselves down. Ellis, for example, described the constant need to justify (to herself) taking time off from university to manage her symptoms.
It’s hard ‘cause there would be two weeks where I’d be out of it, and two weeks where I’d be a lot better [. . .]. I think the hardest thing was that for those two weeks I’d be like, ‘oh I’m fine’ and then the next two weeks I’d be like, ‘I’m dying and it’s the worst thing ever’[. . .]. Like, justifying to myself what I’m doing. (Ellis, Sacral tumour)
Struggling to adjust to the limits of the body and the demands of university revealed how participants were forced to rethink an altered Self and one which was different to their otherwise energised, productive and conscientious ‘normal’ self. James, for example, talked about how he disliked being given additional time during exams and emphasised the importance about finishing on time. The realisation that his body was less capable than how he felt about his (previous) self was difficult.
Because I can’t compete with who I was, now I’ve gotta pace myself. I don’t want the extra time.
is that because you feel you don’t need it or you shouldn’t use it? James: No, it’s because inside I feel more capable, more than my body, like physically I can’t do a lot of things, but mentally, I feel that I’m a lot more capable. (James, Stroke)
These adjustments were not just confined to the present, but required a rethinking of the future. For many, this future Self challenged previously held aspirations and required a realisation (and acceptance) of a different life trajectory. Others described frustrations and disappointments that they would never realise their full academic potential. This is evident when Maddie, a high-performing student with aspirations to study medicine, described the difficulties of trying to maintain good grades during ‘a really bad stage’ of illness. Similarly, Katrina talked about how her future outlook had changed dramatically following her diagnosis and how the restrictions that her illness placed on her meant that she had been forced to consider a different future.
It is frustrating thinking that I haven’t been able to like reach my full potential. I still do reasonable well, but sometimes I wish I could see how well I could do if I didn’t have this pretty major like limitation. (Maddie, Grave’s Disease) [T]hat idea that, your future has been changed. And you’ve had to really adjust to a completely different life. I think that’s the tricky bit because I can remember what I was like [before] when I wasn’t quiet, when I was very loud and very active and able to do all the things that I love. (Katrina, CREST Syndrome)
Yet for other participants, the idea of accepting an altered Self was fiercely contested as they sought to push back against the (limits of) their bodies.
Resisting ill health, taking back control
The idea of taking back control and not letting their bodies and illness dictate their present or future self was a prominent theme. Interviews revealed three inter-connected ways that participants sought to resist the experience of ill health. First, respondents described how they continued to push themselves (sometimes to the extreme) to maintain their normal (health conscious, diligent, hard-working) Self. Second, participants actively downplayed or ignored their symptoms and prioritised other immediate, desirable (social and academic) goals. Third, some young people shared ways they consciously manipulated their condition (to their advantage), but which held potential longer-term health consequences.
Pushing the Self was a recurrent idea in participants’ narratives of how they sought to fight back against the limits of the body. Emily, for example, described pushing through and maintaining a 60-hour working week despite experiencing severe fatigue. Study commitments and maintaining her identity as a hard-working, high-achieving student were priority, often against the advice of her doctor and family. Likewise, Rachel talked about how she pushed herself (and her body) in order to participate in social activities.
I don’t want to say I’m physically incapable of it. My parents and my doctors keep reminding me, no you’re not able to push yourself as hard as you once did, but I still try to do that, which is where I get myself into a bit of trouble, because I’ll push myself so hard and I’ll have that period where I just crash, and that takes me longer to recover than perhaps if I was to just listen to the advice in the first place [. . .]. We had ten weeks of placement and then went straight into nine weeks of semester, and I was also working two jobs [. . .] it was like 60 hours a week and I drove myself into the ground, which is fine, but I was exhausted, it was so bad. I kinda pushed myself. (Emily, Hashimoto’s Disease) Because I’m at college there’s quite a bit of going out and drinking and stuff [. . .]. I do really enjoy that sort of thing and hanging out with my friends, but I’ve actually really pushed myself a lot, so I don’t listen to my body when it tells me when I need to stop [. . .]. I sort of push through even though my body sort of tells me not to. (Rachel, CVID)
Resisting their bodies, however, did not stem from a position of ignorance or lack of awareness of the body’s capabilities. On the contrary, as Rachel’s account illustrates, pushing back against their conditions was often done in full knowledge of the likely health consequences and exacerbation of their symptoms. Pushing the (limits of the) body was thus achieved through actively downplaying or ignoring symptoms and part of a strategy to ‘keep going’ and maintain academic and social engagement. By describing themselves as ‘fine’ and able to cope with the consequences (in the short-term at least), they were able to resist the existence (and effects of) their condition. Indeed, the idea that they were no longer capable of maintaining a full and active life was something fiercely contested.
I like to be really busy, I’m always studying or with friends, so to actually step back and have to be like, ‘no you need your rest, you can’t do this, you need to take some time out’, is just not in my nature. (Emily, Hashimoto’s Disease) I’ve been, like, yeah, let’s go out. And then it hits, and over the course of about 20 minutes, I have to decide, do I go out and risk not being able to function tomorrow, or do I go home now but disappoint my friends? [. . .]. It gets to the point where I’m nauseous because it hurts so much, but I don’t register that. (Katrina, CREST Syndrome) When it gets really bad I just take pain killers because I can’t be bothered dealing with the pain, but most days I’m okay dealing [with it][. . .] I’m not a big fan of taking pain killers too often so I just avoid that. (Julian, Arthritis)
As Julian’s account alludes to, while participants often sought to ignore their condition and related symptoms, others engaged in the active manipulation of their illness in order to control its impacts. Some respondents reported taking (and omitting) medication in non-prescribed ways, for example. A narrative of ‘trading health’ for other (more desired) gains emerged. By manipulating their health conditions in ways that ran counter to medical advice (or the demands of the body), participants reported ways in which they could still perform well in academic assessments, or go out with friends.
What about study and academically, do you feel there is much of an impact there?
If you’re low [hyoglycaemia] you have impaired cognitive ability, so that’s obviously fiercely detrimental to your exam results [. . .] The way I deal with it is you’ve got a trade-off between frequency of having high blood sugars and frequency of having low blood sugars [. . .]. What I consider doing is pick a different point in that trade-off, and if I’m going into an exam where the consequences of a low are quite serious, I will purposely under-dose so that I will probably go high. (Dylan, Diabetes)
Recently I had an oral presentation in the afternoon. [I] woke up and I could feel [a migraine] so I took medication in the morning. Like if you take it early enough then it can mask it enough. (Maddie, Grave’s Disease)
While evidence of participants’ resistance to their conditions seemed to run counter to medical recommendations, these accounts illustrated how participants utilised their knowledge of their body and condition to negotiate (desirable) trade-offs (cf. Heaton et al., 2016). Indeed, such trading was described as evidence of their expertise and how they (successfully) managed competing demands. In his self-management of his diabetes, Dylan, for example, explained how and when he chooses to selectively engage with medically advised regimens.
[I]t certainly gives you a better trade-off between lifestyle, whether it produces better health outcomes I think is up for debate, but [. . .] I don’t really have a particular routine, and the downside of that is that the management isn’t particularly optimal, but you’ve got a spectrum of how well diabetes is controlled, and while I could definitely be better [. . .] I guess, if I was more routine focused then that would curtail, or limit what I could do, so going out on the weekend and having take away meals would be off the table, but I don’t suffer that detriment, because I’ve expressly not followed that path. But I guess the consequences of the model I have taken is more variable blood sugar levels, which has its down sides, certainly in the long run you’ve got adverse organ effects, but in the short run, you’ve got a trade-off. (Dylan, Diabetes) Not knowing how to manage it, I struggled with that for quite a few months in terms of trying different forms of the pill and then I ended up [on] diabetes medication and [. . .] eventually when I just stood back and was like stop, just stop everything, that made me feel a lot better. (Lizzie, PCOS)
Examples of ‘trading health’ did not emanate from participants’ lack of knowledge about their condition (and associated longer-term risks) but on the contrary, signalled their deep understanding of how their condition and bodies could be (effectively) manipulated to enable personal agency (Balfe, 2009; Heaton et al., 2016). By harnessing their own experiential and ‘research’ knowledge, these young people both ‘successfully’ accommodated and resisted the impacts of ill health and in response to the everyday (academic and social) demands of the context in which they lived.
Discussion
This article has sought to advance understanding of how young people take-up and resist dominant narratives of healthism and the body to support possibilities for agency in their management of a long-term health condition. Students’ narratives of health and their management of a long-term condition reflect shifting, sometimes contradictory, health positions and styles (Bury, 1991; Balfe, 2007, Heaton et al., 2016; Sanderson et al., 2011). Grappling with the (incompatible) demands of university life and a chronic health condition commanded particular expertise, resistance to and agency over the (ailing) body in order to uphold a position of health or normality (Balfe, 2009). Through aligning with, and enacting, the responsible health conscious Self, participants in this study revealed how they were not only successful, educated managers of their condition (Ellis et al., 2017) but also demonstrated their commitment to the pursuit of (ideal) health (Clarke and Bennett, 2012; Higgs, 1998). Findings reported here provide further evidence of the tendency for young people to describe health in more positive ways (Spencer, 2013) and preference for upholding a positive health identity (even during times of severe ill health) (Sanderson et al., 2011; Spencer et al., 2018). Supporting the extant scholarship on chronic illness management of adults (Clarke and Bennett, 2012; Nettleton, 2006; Townsend et al., 2006), these accounts signal that young people also experience pressures to align with social norms about the ideal (read healthy) body, and similarly engage with strategies that minimise any personal culpability for their ill health.
The analysis reported here further suggests that conforming to such health ideals and positions is not static and, indeed, can be seen to reflect a range of ‘shifting normalities’ (Sanderson et al., 2011) through which young people seek out ways to negotiate a ‘normal’ (academic and social) life within ever-changing bodily experiences (cf. Balfe, 2009; Harries et al., 2019; Heaton et al., 2016). In a study with young adults with inflammatory bowel disease (IBD), Sargeant et al. (2005) examined the body/Self separation as being part of the tensions between the public and private self and body (p. 149), with the latter not reflecting the ‘true’ self. In this study, and through discursively disconnecting their healthy Self from the unhealthy, alien body, these students could effectively explain their (lack of) academic performance and social engagement at university – distancing themselves from any individual ‘failings’. While these examples may reflect Bury’s (1991) notion of coping or the privileging of different body projects (Balfe, 2007, 2009), this ‘detachment’ from the body could not be achieved without reconciling the tensions of an altered present and future Self. Readjustment to a new Self is a well-documented feature within the biographical experience of chronic illness (Bury, 1982; Charmaz, 1995; Lowton and Gabe, 2003). Heaton et al. (2016) described such adjustments as part of the complexities of maintaining a balance between control and autonomy. Our findings also indicate that young people did not accept such adjustments in straightforward ways, yet may offer novel examples of contestation and resistance to an altered Self, rather than adjustment. Here, by resisting their conditions, participants were better able to conform to dominant norms about what it means to be a healthy ‘normal’ student (Balfe, 2009). Indeed, participants described how they sought to take back control over their bodies and manage their health condition in particular ways to reduce its impacts on their ability to ‘live a normal life’.
Crucially, in this study these forms of resistance were not a product of ignorance about their health condition (as some health literature would suggest), but on the contrary, were deliberate strategies employed by participants and informed by their tacit and academic knowledge of the body/Self and further shaped by the contexts and dominant health discourses in which experiences of ill health were lived. Pursuit of normality triggered particular forms of agency, but this came with ‘trade-offs’ for longer-term health. The idea of trading health for other valued social and academic goals signal how everyday experiences of chronic illness are not wholly bound by the (patho)physiology of the body, but instead draw on other important frames of reference for young people, which are contextually and relationally contingent (Lowton and Gabe, 2003; Sargeant et al., 2005; Spencer, 2013). The active manipulation of their conditions, or pushing themselves to the ‘extreme’, offered opportunities for personal agency in order to take back control and achieve a preferred sense of normality within an abnormal body. Our findings add a novel contribution to the chronic illness scholarship by revealing the ways students’ sought to resist the complex tensions between the body/Self, while seeking ways to uphold dominant social norms about being healthy.
Despite these important advances, some caution is needed with suggesting the broader relevance and transferability of findings based on a relatively small sample of self-selecting university students recruited from one university. In particular, the influences of varying health and social conditions may prompt different ‘normalities’ and forms of management for different groups. The sample included young adults up to the age of 32 and only three young men. A more thorough engagement with the different life stages at university is thus needed, along with a deeper examination of the gendered aspects of young people’s experiences of chronic ill health and university life. Furthermore, the sample included participants with a diverse range of health conditions – each with their own health implications and forms of treatment. This heterogeneity requires some caution when drawing comparisons across the and to avoid suggesting homogeneity. Yet, despite such short-comings, our findings did suggest that students with long-term health conditions face similar challenges at university and thus signal some important recommendations for universities. In particular, our findings suggest the relevance of developing tailored support for students with long-term conditions, along with an examination of how existing academic processes and systems may contribute to the difficulties these young adults frequently experience. Indeed, paying attention to the latter may prove crucial in supporting students to maintain their academic engagement and achieve their potential. Identifying ways to support these students with their health at university is thus a much needed next step in order to enable their full participation in university life.
As previously suggested, participants’ accounts may reflect the important features of their health and particular management style they wish to present (Bury, 1991: 462) and the co-construction and performance of particular identities, within the context of an interview (Riessman, 2008). In this study, the student interviewer may have been perceived by participants as one of their peers – thereby supporting a more comfortable interview dynamic, and our data seem to suggest that participants did not feel unduly inhibited in their responses. However, while the interviewer was unknown to the participants, this similar positioning may have resulted in data that reflected accounts of shared experiences of university – possibly at the expense of downplaying divergent experiences. To guard against this, all authors were involved in the analysis of the data and offered different perspectives on how data were generated and the narratives produced. Indeed, the narrative performances revealed important insights and differences into the varying ways young people may concomitantly take-up, rework and resist the pursuit of healthism within the context of chronicity to ‘successfully’ manage their health conditions in order to fit their everyday university lives. It is within this space that further theorisation and investigation of young people’s lived (ill) health experiences are warranted.
Footnotes
Acknowledgements
We would like to thank all the study participants for their time and contribution to the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Sophie Lewis is supported by funding from an Australia Research Council Fellowship (DE170100440).