
Abstract
Historically, organized violence has been a chronic pervasive problem in Haiti. We set out to elicit Haitians’ views on its effects to guide the development of interventions. In March 2006 we studied a population in the slum area of Cap-Haitien, Haiti’s second largest city, and the nearby towns of Milot and Limbe. A convenience sample of adults was asked to free list all current problems affecting victims of organized violence. Two major categories emerged: psychological problems and financial problems. The psychological problems of “feeling startled and loss of self control,” “sadness/grief,” “continuing to suffer from reliving/reexperiencing past events,” “problems in the head/mental problems,” “deep suffering in the heart,” and “thinking too much” emerged as themes from key-informant interviews. These may correspond to constructs of depression, dysthymia, and anxiety disorders including posttraumatic stress disorder in psychiatric nosology. The development of effective interventions can therefore consider those known to be effective for these problems in other settings. However in selecting interventions, considerations must also include local acceptability, perceived causes of problems, and their social effects.
Introduction
Recent attention on mental health and psychosocial problems in Haiti has understandably focused on the January 2010 earthquake. However organized violence, such as torture or other violence by individuals or groups such as law enforcement and gangs, has historically been the more pervasive problem affecting Haiti. Since the slaves and freed slaves overthrew Napoléon’s army in 1804, Haiti has experienced chronic organized violence including frequent coups d’etat and ongoing civil unrest associated with extreme poverty and lack of infrastructure (Farmer, 2004). These problems are in turn associated with kidnapping, torture, street violence, and domestic violence (Human Rights Watch, 2007; Thompson, Kamber, & Alexandre, 2005). While the political climate has been relatively calm since the elections in 2006, social and political discord have persisted throughout Haiti with ongoing violence and threat of violence by political and social factions (Human Rights Watch, 2007).
Where it occurs this type of violence has been found to be an important determinant of individual and collective health because it can lead to the loss of loved ones, disruption of daily life, food shortages, destruction of local infrastructure, and deterioration in the supply of other basic needs including health care, food, and shelter (Farmer, 2004; Pedersen, 2002). As the country with the lowest GDP in the hemisphere (United Nations Development Programme, 2004), Haiti has limited resources for dealing with these problems. Even before the earthquake, medical, legal and social services were in short supply in Haiti and were difficult to access due to a lack of infrastructure and of trained professionals, leaving most of the population with few health care services (Chatterjee, 2008). An unparalleled exodus of health professionals (Chatterjee, 2008; World Health Organization, 2004) has been temporarily reversed in the aftermath of the earthquake by an influx of expatriates and Haitian nationals assisting in the relief efforts. But this outward migration is likely to resume once the world’s attention and resources are turned elsewhere.
The purpose of our study was to understand how local people affected by the violence view its effects, particularly the resulting mental health and psychosocial problems. We intended for the results to inform future development of mental health services to address these issues in ways that are culturally appropriate and feasible, given Haiti’s limited resources. Therefore, we focused on information of programmatic importance, particularly descriptions of these problems, their severity, their causes, and what victims of violence believe might be effective ways to address these problems.
Given concern with the validity and relevance of mental health instruments used in cultures different from those in which they were developed, we used qualitative interviewing methods to investigate these issues from the local (or emic) viewpoint. We originally began using qualitative methods in this way in 1998 in response to a discussion in the literature on the appropriateness of applying Western mental health concepts to other cultures (Cunningham & Cunningham, 1997; Kirmayer, 1993; Kleinman, 1988). Therefore, while studies have reported posttraumatic stress disorder (PTSD), depression, and/or anxiety in diverse settings and ethnic groups exposed to torture or other forms of violence (Allden, Poole, Chantavanich, & Ohmanr, 1996; Başoğlu et al., 2005; Cunningham and Cunningham, 1997; Holtan, 1999; Lopes Cardoso et al., 2004; Lopes Cardoso et al., 2000; Shrestha et al., 1998; Silove, 1999; Silove, Sinnerbrink, Field, & Manicavasagar, 1997; Silove, Steel, McGorry, Miles, & Drobny, 2002; Thabet, Abed, & Vostanis, 2004; Thabet & Vostanis, 1999), most are based on questionnaires, and the meaning and utility of a checklist of symptoms developed in another culture has been questioned (Kagee, 2004). Such concerns may be justified, given that checklists are a series of closed (and usually leading) questions and most questions involve choosing a fixed response (such as yes/no questions or a Likert scale). These items can be answered even when the question is not understandable to the respondent or reflects concepts with which they are not familiar. Also, one does not have to understand a question to appreciate that choosing the more severe response is more likely to result in financial or other humanitarian aid. We have no scientific data on this issue but our experience is that the receipt of such aid is a common expectation among respondents to research studies in low-resource environments. Therefore, studies based solely on questionnaires that find high levels of symptom severity (among individuals) and prevalence of problems (among populations) do not alone prove that a problem is frequent, is understood, or even exists locally.
Although a large comprehensive study has been done on the nature of violence in Port-au-Prince (Kolbe & Hutson, 2006), little work has been done on the mental health effects among Haitian victims of violence. We were unable to find published studies on how Haitian people themselves perceive the problems resulting from the organized violence, with the exception of a report from Martissant and Port-au-Prince by a physical therapist describing stories of trauma and its effects related in therapy groups (James, 2004). Given the history of recurring organized violence and the likelihood that it would continue to be a major problem in the future, we felt it was important to understand its mental health effects in order to inform future mental health services.
Methods
Study sites
Data collection was conducted over a 2-week period in March, 2006 in a poor section of the city of Cap-Haitien and the nearby towns of Milot and Limbe. Cap-Haitien is Haiti’s second largest city. It is on the northern coast and was the economic and cultural center of Haiti during French Colonial rule. The three sites were chosen to encompass both the urban and town experience of people living in northern Haiti as well as being sites that had clearly experienced the violence that had most recently affected the north. For example, just prior to President Aristide’s departure from Haiti on February 29th, 2004 (Marquis, 2004), the city of Cap-Haitien was attacked and overrun, the airport was looted, warehouses were plundered, and the police station, local radio and TV stations, and many businesses were burned (Bosch & Ridder, 2004; Polgreen, 2004). In Limbe, residents described incidences of torture, rape, and other forms of social violence. Milot experienced several attacks by the rebels in 2004 and the former military in 1994, and respondents have continued to live in an insecure environment. At the time of the study violence was continuing in all three sites.
Data collection
With participation and logistical and technical support from Unité de Recherche et d’Action Médico-Légale (URAMEL, a Haitian NGO based in Port-au-Prince), we conducted a qualitative study to delineate the mental health and psychosocial problems of persons affected by organized violence. Qualitative methods were used to understand these problems from the local (or emic) perspective. Over the period of 2 weeks, 12 trained local interviewers collected and analyzed interview data on the problems resulting from organized violence with particular focus on mental health and psychosocial problems and their effects. Interviews were conducted and recorded verbatim in Haitian Kreyol. Interviewing was done by means of two qualitative methods: free listing followed by key-informant interviews. A detailed description of the way in which we use these methods has been published elsewhere (Bolton, 2001). Briefly, the rationale for this choice of methods is that free listing provides a broad overview of the problems affecting local people. From this broad list, investigators can identify problems which appear to be important (based on how many people mention them and their apparent severity) and that might be amenable to interventions. These problems, once selected, are then explored in more detail using key-informant interviews.
In the present study, free-list interviews began by asking respondents to list all problems of local people (not only mental health or psychosocial problems) resulting from violence. Free-list respondents were a convenience sample chosen to represent the diversity of the poorer part of the adult population in terms of age, gender, and where they lived. Locally respected people (community leaders, healers, and other well-known local people) were contacted through our service partner, URAMEL, who work in the region. They were interviewed and also helped to recruit other local people for interview who were either direct victims of torture and/or other forms of organized violence or were immediate family members of victims. All were asked to list all the current problems only, since our interest was to inform program planning to address ongoing issues. Interviewers were trained to probe for as many problems as possible. For each problem interviewers recorded its name and a short description in the exact words of the respondent. Once the list was completed it was reviewed by the interviewers for potential mental health and psychosocial problems with the respondent still present. For study purposes potential mental health and psychosocial problems were defined as problems related to thinking, feelings, or relationships. For each of these problems interviewers asked the respondent for the names and contact information of local residents knowledgeable about that type of problem. This contact information was recorded separately from the interview. During the analysis all the free lists were condensed into a single composite list including each problem and how many respondents mentioned it. This composite list was reviewed by two of the authors (PB and AG), the URAMEL staff, and by a Haitian staff member from the USAID Haiti Mission who supported the study. We selected a subset of mental health and psychosocial problems for further investigation based on how frequently they were mentioned, apparent severity based on their descriptions, and whether they seemed modifiable using existing interventions and available resources. These problems were then explored in detail using key-informant interviews.
Persons interviewed for the key-informant interviews were community members considered by the community to be particularly knowledgeable about local violence and its effects. Key informants were identified through: (a) local leaders and respected people; (b) the names and contact information of persons said to be knowledgeable about the mental health and psychosocial problems identified in the free lists (as described before); (c) selection of some of the free-list respondents who were clearly very knowledgeable; and (d) “snowball sampling,” that is, referral by one key informant to another key informant. Key informants identified in this way included victims of organized violence and their families, as well as locally respected persons (community leaders, health practitioners, healers, etc.). During the interview they were asked to describe each of the mental health problems selected from the free lists in as much detail as possible with particular reference to how the problem is recognized, its causes, effects, what people have done to address each problem, and what could be done. At least one follow-up interview was sought from all key informants who were found to be knowledgeable, to obtain as much information as possible.
Ethical approval for the study was given by the Institutional Review Board at the Boston University School of Public Health, where PB was a faculty member at the time of the study.
Data analysis
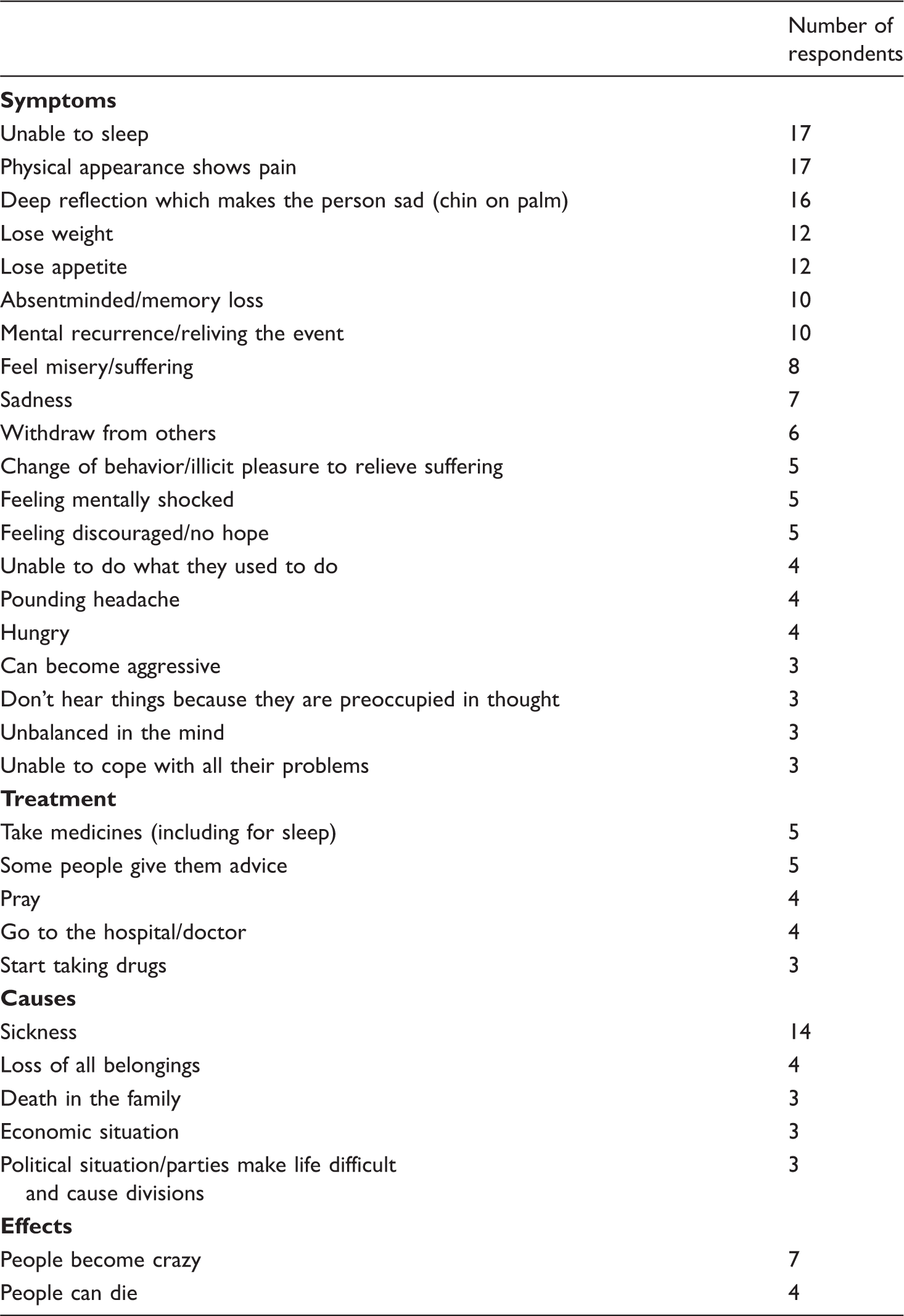
Summary of all problem free-list items mentioned at least three times a

Primary free-list question: “What are all the problems affecting local people that have resulted from torture and organized violence?”
Included among the 6 problems explored in the subsequent key informant interviews. The remaining two problems were mentioned in the short descriptions free-list informants gave for each problem.
Sezisman pran yo (“They are startled by the sudden shock and have lost control”)

Included under acute loss of control symptoms.
Results
Respondents described acts of brutality by the military and paramilitaries over the previous decade resulting in both collective and individual exposure to organized violence. In the local communities the military were frequently blamed for killing, beating, looting, and raping. Resulting economic stress within the family was also blamed for increased levels of domestic violence, although this was much less emphasized than the violence by the military and political gangs.
Free-listing results
A total of 41 individuals participated in the free-list interviews across all three sites. In the past, we have found that a minimum of 20 interviewees representing both genders and varying ages is necessary to identify the salient issues. In this study, we doubled this number in case there were differences between sites but on analysis we found no clear differences among the major responses. The sample was chosen to include approximately equal numbers of men and women from all three sites, and of varying ages from 18 years to elderly.
Two major themes emerged regarding the results of violence. The first and most commonly mentioned theme was psychological problems. Seven salient psychological problems were identified (in decreasing order of frequency): (a) fear, (b) feeling startled with resulting loss of self control, (c) sadness/grief, (d) continuing to suffer from reliving/reexperiencing past events, (e) loss of dignity, (f) helplessness/discouragement, and (g) problems in the head. Other psychological problems were also mentioned. Of these “mental trouble” was a nonspecific term similar to “problems in the head” while “people lose their heads” and “unable to sleep” were mentioned by fewer than five respondents. The single most commonly stated problem was that people are constantly fearful or afraid, reported by 29 out of 41 people (see Table 1). This was discussed in terms of feeling afraid with associated physical symptoms (such as trembling) as the result of real threats from people still in the area or who may return. But fear was also mentioned in terms of being always watchful and easily startled by nonthreatening events such as barking dogs.
The second (and less commonly mentioned) major theme was financial hardship (see Table 1), for example, “economic problems,” “families suffer because they are hungry,” “unemployment,” “people can’t work,” and “economically people have regressed.” A commonly reported result of violence was loss of possessions or homes due to destruction and pillage. People were often robbed when forced to abandon their homes without their possessions.
To supplement the information in Table 1 we have summarized below in bullet form the common themes that emerged from the descriptions of all the problems:
Victims of violence are subject to discrimination, such as not being able to rent apartments or get work. Loss of dignity results from both stigma as victims of violence and from victims’ inability to care for themselves and family. Others in the community mock or criticize them. Stigma is particularly severe for victims of sexual violence: both family and society tend to reject them. People feel that violence can recur again at any time. Therefore, community members don’t trust each other, resulting in fragmentation and loss of ability of the community to come together to address problems. Perpetrators live openly in communities, which contributes to an ongoing sense of insecurity. People may leave their homes and sleep in the open or in the houses of others, or constantly move about in order to avoid further victimization. They may leave the area resulting in the breakup of families. Because of insecurity and mistrust people no longer feel they can relax or be at ease in their neighborhoods. Unemployment is commonly due to inability to function because of physical and mental disorders, discrimination, and being in hiding. Hence people are unable to provide for themselves or their families or to replace their lost possessions. Victims of violence tend to become violent themselves, resorting to domestic violence and victimizing others in the community.
Key-informant interviews
As described in the Methods section, the topics of the key-informant interviews were selected from the free-list data by an ad hoc group comprising the external researchers, URAMEL staff, and Haitian USAID mission staff based on how frequently each problem was mentioned, apparent severity, and feasibility of addressing these problems. We therefore selected all the more commonly mentioned problems (those mentioned by at least five respondents) with the following exceptions: “People are constantly afraid,” “people are in misery” and “people are discouraged” were largely attributed by respondents to insecurity and poverty and addressing them was considered beyond the scope and resources of NGOs or other humanitarian organizations. “Mental trouble; mental instability” was not selected because this appeared, based on the problem descriptions, to be a cover term that encompassed all the other mental health problems.
The final list of topics selected from the free lists (see Table 1) for further investigation were: (a) feeling startled and loss of self control; (b) sadness/grief; (c) continuing to suffer from reliving/reexperiencing past events; (d) problems in the head/mental problems; (e) deep suffering in the heart; and (f) thinking too much. The last two topics were not included in the list of problems reported in the free lists but the ad hoc group decided to include them because they emerged frequently as underlying psychological issues in the short descriptions accompanying each problem.
Thirty-nine people were interviewed as key informants. Tables 2–7 summarize the interview findings for each of the topics investigated:
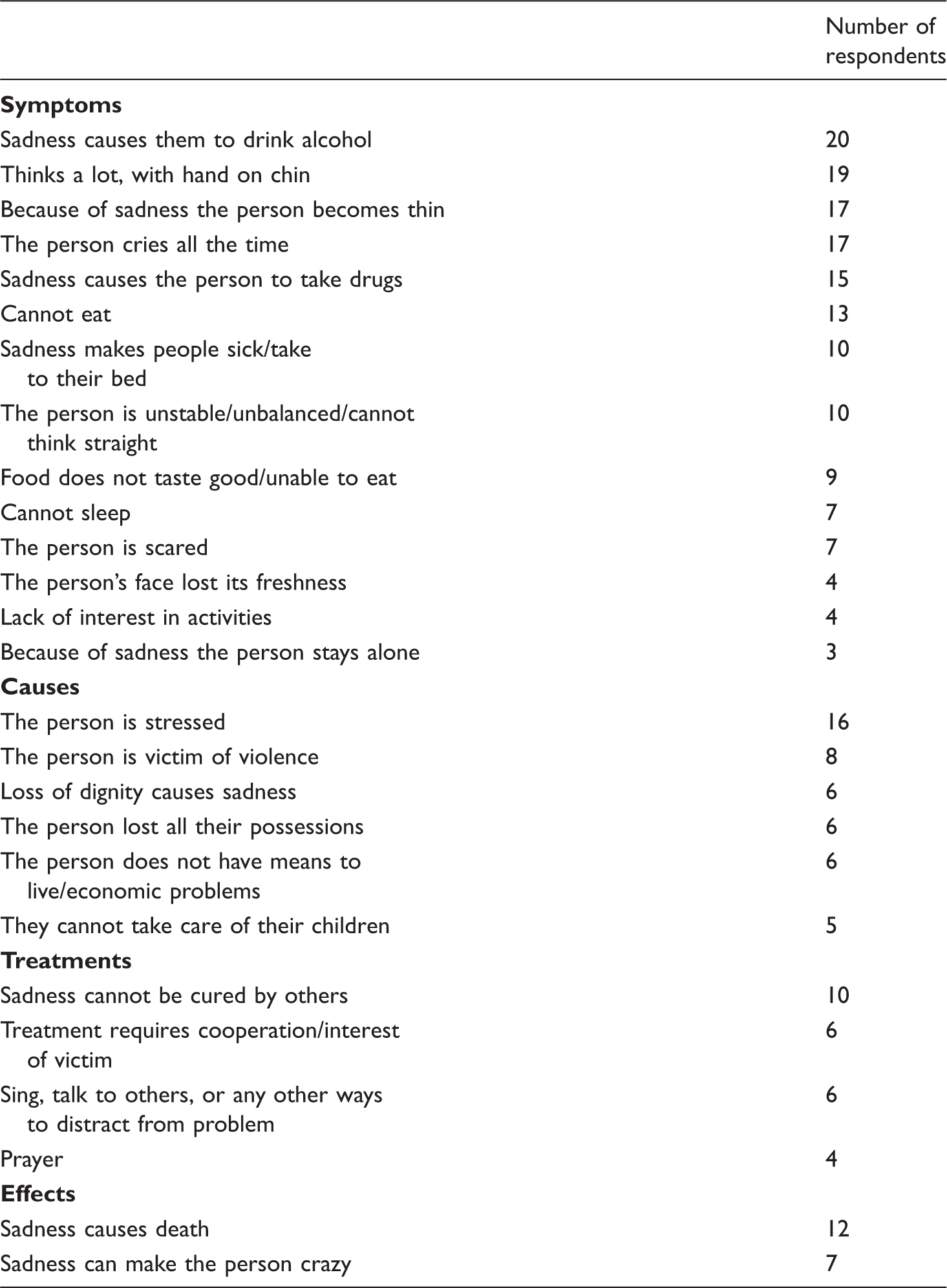
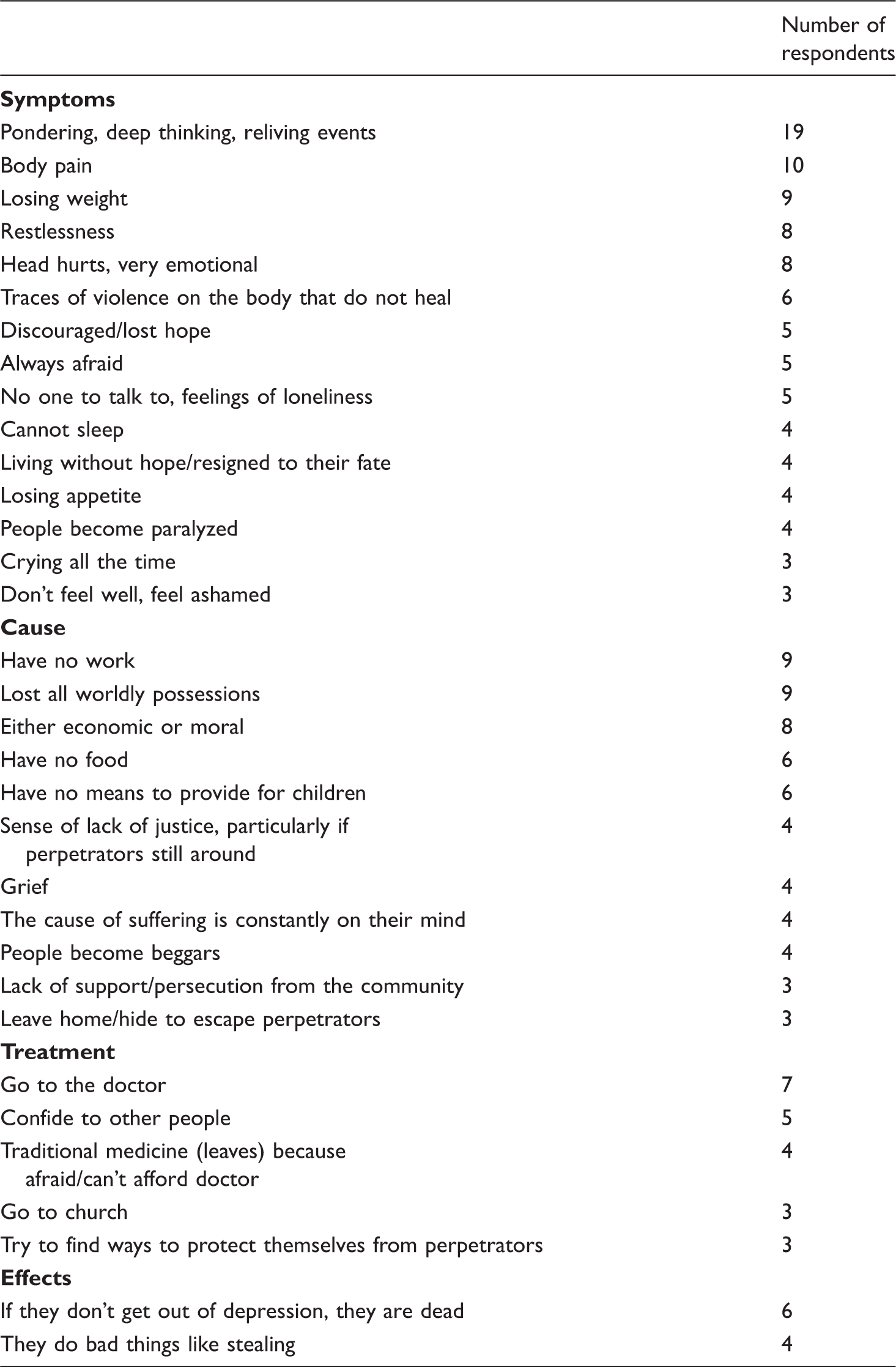
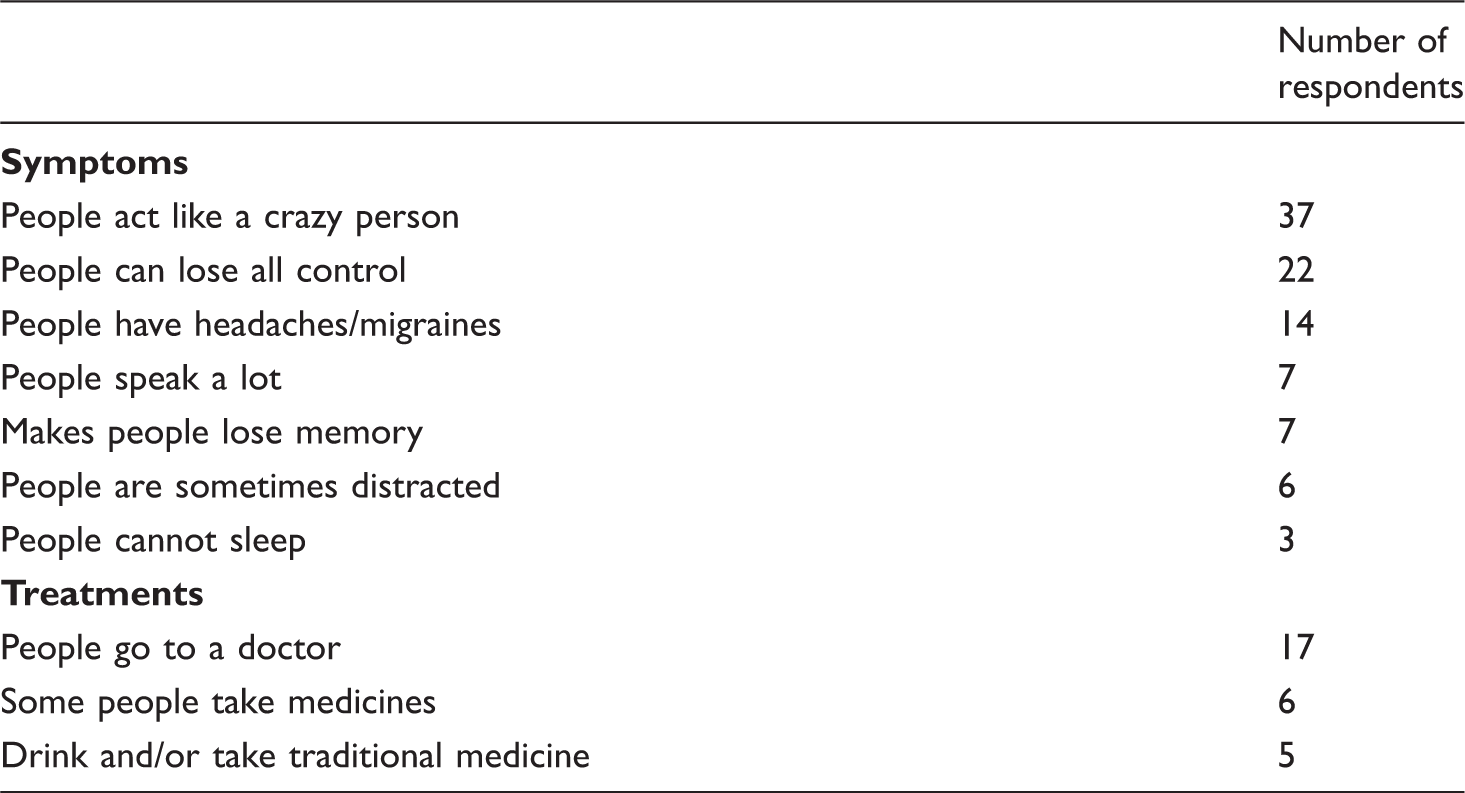
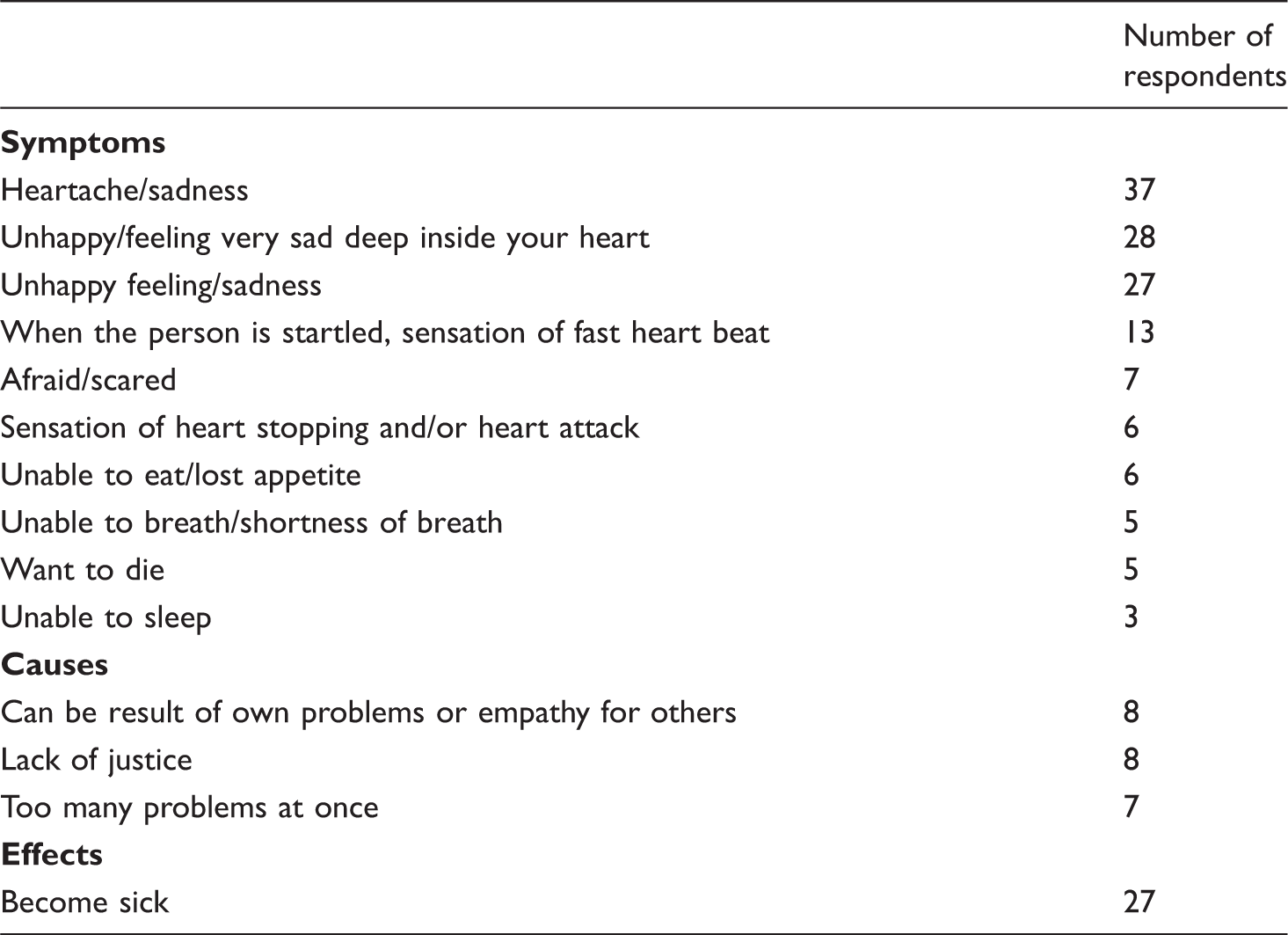
Feeling startled and loss of self control “Sezisman pran yo” (Table 2) was described as a type of mental shock resulting from exposure to traumatic events and traumatic loss, or as suddenly having so many problems to deal with that you think too much. Symptoms occurred immediately after the event and might persist or recur with reminders of the event. In addition to being startled easily and feeling anxious, some of the many symptoms include somatic and mental manifestations such as chills, trembling, diarrhea, high blood pressure, the sensation of having a heart attack, crying, and fear. Being startled and physical trauma to the head were the most frequently reported causes (described by 17 and 15 key informants, respectively). Sadness “Chagren” (Table 3) was due to thinking about loss, both loss of people and loss of a better living situation and resources. Hence it was worse among those who remember when conditions in Haiti were better. Sadness was also severe for those who have children for whom they cannot care. The most common symptom was drinking alcohol. Taking drugs was also frequently mentioned. Other prominent symptoms are thinking a lot, weight loss, crying, and lack of appetite. The most commonly reported causes of sadness were stress, followed by being a victim of violence. Causes less frequently reported were loss of dignity, having lost all one’s possessions, and economic hardship. Continuing to suffer and relive past events “Yo kontinye soufrwi” (Table 4) was commonly described as thinking deeply about these events and/or being preoccupied with them. The next most common symptoms were somatic such as bodily pain, weight loss, restlessness, and headaches. The most frequent causes of suffering were related to economic difficulties, being unable to work, having lost possessions, lacking food, or lacking means to provide for children. Other causes were more directly related to the violence; for example, lack of justice, or loss of family or friends because of violence. Problems in the head/mental problems “Chók nan tét” (Table 5) were described by almost all key informants: 37 of the key informants reported someone they knew with this problem as acting like a crazy person and 22 reported that a person with this problem can totally lose control. Some respondents stated that victims of violence tend to become violent themselves, resorting to domestic violence and victimizing others in the community. No separate underlying causes were listed for problems in the head. Instead, informants commonly referred to this problem as being a result of the other mental problems including the problems described here: feeling startled and loss of self control, sadness/grief, continuing to suffer from reliving/reexperiencing past events, deep suffering in the heart, and thinking too much. No effects are reported in Table 5 since no single response was given by at least three key informants. Deep suffering in the heart “Ke fe mal” (Table 6) was most commonly described as sadness and heartache. Other symptoms include fear, suicidal thoughts, and loss of appetite. Perceived causes derived directly from one’s own problems, from empathy for others’ problems, or a lack of justice. Because no one answer was given by at least three people, no treatments are reported in Table 6. The most common symptoms described for thinking too much “Moun yo panse anpil” (Table 7) were difficulties sleeping and appearing pained. Key informants suggested that focusing on problems made people sad, taking its toll on the physical body by manifesting itself in loss of weight and loss of appetite. By far the most common cause of thinking too much was illness. Other causes included loss of belongings, their economic situation, and the political situation. Chagren (“Sadness”) Yo kontinye soufrwi (“Continuing to suffer from past events/reliving past events”) Chók nan tét (“Problems in the head”) Ke fe mal (“Deep suffering; the pain is so strong the person feels that his/her heart is hurting”) Moun yo panse anpil (“They are worn out from pondering so much on their problems; they think too much”)
In addition to the six problems which formed the focus of the key informant interviews, loss of dignity “Yo pédi diyte yon an zón nan”—one of the salient problems mentioned in the free lists—again emerged frequently in the key-informant interviews. As in the free-list interviews, the key informants reported that loss of dignity resulted from both the stigma associated with being victims and victims’ inability to care for themselves and their families. Victims described being subject to discrimination, for example, not being able to rent apartments, get work, or being mocked and criticized. Loss of dignity was described as particularly severe for victims of sexual violence who reported being rejected by family and society.
A common theme of all six problems investigated in the key-informant interviews is that they result in reduced function due to “a lack of interest in anything” or “people don’t want to do anything,” as well as a reported decreased capacity to function secondary to the direct effects on the mind and body (producing hypertension, diabetes, and heart problems). These physical health effects were worse and more frequent in the elderly and could result in death.
All the problems explored in detail in the key-informant interviews were discussed and described by informants as distinct entities. However, this may have been an artifact of the interview process, which asked separately about each problem. Respondents made it clear that most of the problems were closely related to each other in terms of common causes (being the result of violence), their nature, their impact, and the measures people took to deal with them. The problems were also closely interrelated in terms of frequent comorbidity, and each problem could be both a cause and a result of other problems.
Respondent suggestions on how to deal with these problems
Common ways of dealing with mental problems mentioned by respondents were: (a) doctor and medicines (if the person can afford them); (b) traditional healers or medicines; (c) consulting with friends; (d) prayer and church; and (e) distraction with other activities (see Tables 2–5 and 7). For both deep suffering in the heart and sadness respondents considered interventions unhelpful. When asked how sadness can be dealt with the most common response was that it could not be cured (see Table 3). Only two respondents mentioned any strategies for dealing with deep suffering in the heart, with one suggesting resignation to the problem and another suggesting prayer (Table 6, data not shown).
Respondents frequently suggested improving the ability of communities to collectively address mental health and psychosocial issues, both directly and by addressing related issues such as unemployment, lack of security, and lack of justice. Respondents described communities as more united in the past with people more willing to assist each other. They contrasted this with a current breakdown in the sense of community due to political divisions, poverty, and insecurity. This results in fear of neighbors and a general lack of trust which in turn results in increased hardship (with every man for himself) and even in the abuse and marginalization of victims of violence. Some respondents noted that as people become poorer they also become more marginalized in society making it difficult for them to recover, and that communities could better address this problem if they were united.
Respondents were vague on recommendations of how to rebuild communities. Only two approaches were mentioned: (a) Mistrust and fragmentation within communities have resulted in reduced communication, which further reduces the sense of cohesion and ability to respond to problems. Interventions could focus on improving communication among factions and groups; (b) Addressing the breakdown of friendships and families. Intervening to improve social interactions and providing assistance to families directly could help to rebuild communities.
Discussion
The purpose of this study was to describe the mental health and psychosocial effects of organized violence among a Haitian sample from their own (emic) perspective. This information was intended to inform subsequent quantitative studies of the prevalence of mental health problems among this population and development of interventions to address these issues. However, these later activities never took place due to our inability to secure subsequent funding.
Comparison of our qualitative data with the DSM-IV, (American Psychiatric Association, 1994) demonstrates that many of the symptoms described by our informants correspond to established criteria for major depression, dysthymia, and anxiety disorders including PTSD. Symptoms reflecting the major DSM-IV PTSD criteria (reexperiencing past events, avoidance, and increased arousal) were described by many respondents. Distrust and alienation from others (features of more complex PTSD) were articulated in the respondents’ descriptions of fear and hidden violence (Ebert & Dyck, 2004). Many features of sadness/grief and deep suffering in the heart overlap with the DSM-IV criteria for major depressive disorder and/or dysthymia including lack of appetite, insomnia, diminished interests in activities and suicidal thoughts. Victims also described thinking too much, a concept which shares characteristics with anxiety and major depression and which has been associated with depression-like illness in other non-Western contexts, such as in Zimbabwe (Patel, Abas, Broadhead, Todd, & Reeler, 2001) and Uganda (Wilk & Bolton, 2002). “Sezisman” has been described at length in the literature and can result from an unexpected event, including a traumatic event (Nicolas, DeSilva, Grey, & Gonzalez-Eastep, 2006). The DSM-IV diagnostic criteria for a panic attack and the symptoms attributed to feeling startled and loss of self control are very similar. Almost all the common symptoms of a panic attack were described by our participants (e.g., palpitations, trembling, abdominal distress, chills, and feeling faint).
In addition to the psychiatric and psychological perspective, it is useful to consider how Haiti’s rich cosmological, cultural and spiritual perspective and history influence the understanding of both problems and healing. Haitian views of mental health have been influenced by West African, French, Spanish, and Native American cultures (Gustafson, 1989; Desrosiers & St. Fleurose, 2002). The legacy of the revolution and subsequent episodes of violence integral to Haiti’s history parallel the development of a cosmology known as Vodou in Kreyol that describes and explains health (Pierre et al., 2010). Vodou flourished between 1804 and 1858 (the period following the Haitian revolution) and again during the last half of the 20th century during the regime of François “Papa-Doc” Duvalier (Miller, 2000). While often hidden, Vodou is practiced by many Haitians to varying degrees (Desrosiers & St. Fleurose 2002; Gray, 2008; Pierre et al., 2010).
In Vodou common physical illnesses can be cured by Western-trained practitioners or the more traditional “Doktè Fèy” (traditional healer). More complex illnesses including emotional, psychic (i.e., psychological), mental, or spiritual problems may indicate a rupture of the deeply valued relationships with the natural, spirit, and ancestral worlds (Pierre et al., 2010) and therefore must be tended to by an Oungan or Mambo (roughly translated in English as a Voodoo Priest or Priestess). The healing process, described simplistically here, involves various practices that are relational, social, and communal in nature, including ceremonies infused with rhythm-based practices such as dance and drumming (Gray, 2008), plant medicine, prayer to spirits residing in the natural and ancestral realms, and feeding the spirits or ancestors to appease and nourish them (Pierre et al., 2010). Healing ceremonies and rituals are conducted for all types of health issues—physical, mental, and emotional—since all are considered to be connected to the spiritual realm, as well as for issues of conflict, justice, economic challenge, and practical issues like employment, food, and personal or collective protection.
One result is that there are not the clear distinctions made in the West between different types of health issues (such as physical health versus mental health) or even between health and other life issues when it comes to causation and treatment (Nicolas et al., 2007). The distinctions drawn by our informants between the various problems were likely of more interest to us than to the informants themselves. This was confirmed for the topics that we explored in more depth: key informants emphasized that the different problems were highly interconnected in terms of co-occurrence, causation, and what people did to deal with them.
Limitations
The Cap-Haitien region was chosen because of its history of relative stability even during recent periods of unrest. It therefore offered the greatest likelihood that the assessment could be followed up by an intervention that could be completed as planned. However, because the local culture and situation are different in other regions of Haiti, we are unsure of the extent to which the findings can be generalized to elsewhere in Haiti.
Since this was a qualitative study using a convenience and a purposive sample, the absolute and relative frequency of responses cannot be assumed to represent opinions in the wider population. Therefore, we do not place very much weight on these numbers except in that they indicate that a response was given by “many” versus “few” respondents and that this probably represents the relative importance or at least salience of these items in the minds of the respondents rather than a measure of their absolute importance or frequency.
The design of this study (and of previous similar studies), particularly the use of broad interviewing methods, the limited number of interviews per respondent, and the use of a convenience sample, preclude a detailed understanding of the problems of this group. Instead, the data are suitable for identifying programmatically relevant information about some of the more salient issues affecting this population. A truly detailed understanding would require more intensive interviews with a larger number of respondents and a wider range of qualitative methods.
Nevertheless, the data suggest that the issues identified and explored in the key-informant interviews are priorities for those affected by organized violence. The next step in program planning would be to develop instruments to quantitatively measure severity and prevalence of these problems and to triage people into these interventions. While at the time of writing, attention is being focused on the aftermath of the January 2010 earthquake, past experience suggests that in the following months and years the chronic effects of structural violence will reassert themselves as priorities for local people. Keeping this in mind, efforts to rebuild Haiti should include an expansion of efforts to further understand and address these effects, including those problems we have described here.
Conclusion
The similarity of symptoms reported to some Western mental disorders suggests that existing instruments based on those constructs could be adapted and used in this part of Haiti (subject to translation and validity/reliability testing). It also suggests that specific therapies found to be effective for these disorders in Western countries (such as cognitive behavioral therapy or interpersonal psychotherapy) could be adapted and tried locally.
Based on the community’s own suggestions, and the published literature, community-level interventions should also be considered. The application of principles from conflict resolution, community building, and peace-building models might form a useful basis for community-wide interventions to reduce mistrust and restore community cohesion. Interventions focused on promoting social capital, including those related to community connectedness and cooperative action in a neighborhood, are believed to contribute to resilience (Landau, 2007; Mowbray et al., 2007). Inadequate social support after trauma is considered an important risk factor for PTSD and so expanding such support may be helpful in subsequent healing (Brewin, Andrews, & Valentine, 2000; De Zulueta, 2007; Ozer, Best, Lipsey, & Weiss, 2003). Since stigma is an important problem for survivors, any of these or other interventions to improve community understanding and acceptance of survivors and to reintegrate them into social networks and employment could improve the quality of life of survivors and their families. Given the historical and cultural context discussed previously, a combination of clinical (individual) and communal approaches may be highly acceptable. Inclusion of Voudou practitioners and other traditional providers may facilitate this type of approach and make it more acceptable and accessible to local people.
Footnotes
Acknowledgements
Special thanks go to four people for making this assessment possible: Nettie Jannini of USAID Haiti and Danuta Lockett of the Victims of Torture Fund, Washington, DC. Without their unflagging support which overcame repeated setbacks this work would never have been done. Also thanks to Marjorie Joseph of URAMEL. In addition to the logistic support which they and URAMEL provided, they also gave invaluable field-based technical support and advice. We also thank Elvire Eugene of AFASDA who helped with logistics in Cap-Haitien.
Funding
This study was funded by the Victims of Torture Fund at the United States Agency for International Development (USAID).