
Abstract
Acceptance and Commitment Therapy (ACT) is a psychological intervention that has wide clinical applications with emerging empirical support. It is based on Functional Contextualism and is derived as a clinical application of the Relational Frame Theory, a behavioral account of the development of human thought and cognition. The six core ACT therapeutic processes include: Acceptance, Defusion, Present Moment, Self-as-Context, Values, and Committed Action. In addition to its explicit use of the concept of mindfulness, the therapeutic techniques of ACT implicitly incorporate other aspects of Buddhism. This article describes the basic principles and processes of ACT, explores the similarities and differences between ACT processes and some of the common tenets in Buddhism such as the Four Noble Truths and No-Self, and reports on the experience of running a pilot intervention ACT group for the Cambodian community in Toronto in partnership with the community’s Buddhist Holy Monk. Based on this preliminary exploration in theory and the reflections of the group experience, ACT appears to be consistent with some of the core tenets of Buddhism in the approach towards alleviating suffering, with notable differences in scope reflecting their different aims and objectives. Further development of integrative therapies that can incorporate psychological and spiritual as well as diverse cultural perspectives may help the continued advancement and evolution of more effective psychotherapies that can benefit diverse populations.
Introduction
Acceptance and Commitment Therapy (ACT) is a psychological intervention that is garnering increasing interest and empirical support. It has seen wide application in clinical settings as it proposes a broad functional approach to understanding psychopathology. It has been applied to treat a variety of mental disorders (e.g., schizophrenia, anxiety disorders, mood disorders, addictions) (Ruiz, 2010), improve medical outcomes for physical illnesses (e.g., diabetes, epilepsy) (Ruiz, 2010), promote health (e.g., prevent burnout) (Hayes, Bissett et al., 2004), and shift certain kinds of restricting attitudes (e.g., stigma, self-stigma, racial prejudice) (Hayes, Bissett et al., 2004; Lillis & Hayes, 2007; Luoma, Kohlenberg, Hayes, Bunting, & Rye, 2008; Masuda et al., 2007). ACT is recognized by the U.S. Substance Abuse and Mental Health Services Administration (SAMHSA) as an empirically supported treatment (NREPP, 2011).
Among the core therapeutic processes of ACT, healing and recovery are promoted through the cultivation of acceptance and mindfulness (Hayes & Duckworth, 2006). This is in line with the increasing interest in the application of mindfulness and Eastern traditions for mental health problems. Jon-Kabat Zinn was among the first to import the practice of mindfulness of Zen-Buddhism as a treatment when he developed the Mindfulness-Based Stress Reduction program (Kabat-Zinn & Hanh, 2009). A number of “third-wave” psychotherapies, including ACT, now incorporate the use of mindfulness (Hayes, Follette, & Linehan, 2004). Steven Hayes, the founder of ACT, wrote an early paper on ACT and Buddhism, focusing specifically on their similarities in dealing with the ubiquity of human suffering, the role of attachment, mindfulness, valued actions, and issues of the self (Hayes, 2002). To date, however, there has been no other focused review of ACT and Buddhism in the literature. Kang and Whittingham (2010) compared the narrow concept of mindfulness in current Western psychotherapies to the concept of Buddhist mindfulness practice in historical and religious context, including its broader goals (e.g., enlightenment) and various dimensions (e.g., deliberate cultivation of positive wholesome formations). Hall, Hong, Zane, and Meyer (2011) also remarked on some similarities and differences between ACT and Buddhism in examining the cultural applicability of ACT for Asian Americans, especially in the context of a collectivistic culture, although their analysis was more focused on the technical interpretation of ACT rather than its underlying model and philosophy (Hayes, Muto, & Masuda, 2011).
This article will outline and describe the basic principles and processes of ACT, explore the similarities and differences between ACT and Buddhism, extending previous work by increasing the scope to include more basic tenets in Buddhism, and report on the experience of running a pilot intervention ACT group in partnership with a Buddhist Holy Monk.
Acceptance and Commitment Therapy as a “third-wave psychotherapy”
The “third-wave” psychotherapies include among others: Dialectical Behavioral Therapy (DBT), which has been shown to be effective in the treatment of patients with self-harming behaviors (e.g., Borderline Personality Disorder) (Linehan, 1993); Mindfulness-based Cognitive Therapy (MBTCT), effective in prevention of recurrent Major Depressive Disorder (Segal, Williams, & Teasdale, 2002); and Acceptance and Commitment Therapy (ACT) (Hayes, Strosahl, & Wilson, 1999), which has been applied to a number of mental health problems. Although these therapies were developed in response to different clinical populations, they have in common the therapeutic use of concepts related to mindfulness and acceptance (Hayes, Follette et al., 2004).
The term “third-wave” arises from a perspective on the evolution of psychotherapies that identifies the “first wave” as behavioral therapy, which emerged in the 1950s as a response to traditional psychoanalytic forms of psychotherapy and which added empirical rigor by focusing on behaviors (Hayes, 2004). This approach contributed to and continues to inform learning theories and the treatment and management of a variety of conditions and behavioral problems; indeed, in vivo or clinical exposure remains one of the most effective psychological interventions for many forms of anxiety disorders. The second wave refers to the rise of Cognitive Therapy in the 1960s and 70s, which promoted the primacy and centrality of cognition as a focus for understanding clinical problems and the target for clinical interventions. In practice, treatment manuals and research often combine both Behavioral Therapy and Cognitive Therapy together as Cognitive-Behavioral Therapy (CBT). The term “third-wave” has evoked debate as to whether the new therapies are significantly different from traditional forms of CBT to warrant this distinction (Hofmann & Asmundson, 2008). Regardless, the focus of this paper is on ACT, its underlying philosophy and theory, and its relationship with Buddhism.
Philosophy and theory of ACT
The underlying philosophy of ACT has been described as a specific type of Contextualism, termed “Functional Contextualism” (Hayes et al., 1999). The root metaphor in Contextualism is an “act in context”, emphasizing that any action or event cannot be separated from its historical and current context (Hayes, 1993). Functional Contextualism uses workability as a pragmatic truth criterion, and its explicit analytic goal is to be able to predict and influence events by manipulating variables in context. It rejects traditional anthropic mechanism that many psychological interventions such as CBT can be seen as based upon, as it emphasizes a functional contextualistic approach over a structural mechanical approach (Dougher, 2000; Hayes, Luoma, Bond, Masuda, & Lillis, 2006). From this perspective, “mentalism” is rejected and thoughts are seen not as a special causative independent variable of emotions and behaviors. Instead, both cognitions and emotions are seen as private internal behaviors. Both internal and external behaviors are contextually controlled (Dougher, 2000; Hayes et al., 2006).
Based on this philosophy, Hays and colleagues developed Relational Frame Theory (RFT) as a refinement of the work of B.F. Skinner to account for how human language and cognition develop and become contextually controlled (Hayes, Barnes-Holmes, & Roche, 2001). According to RFT, human language and cognition are unique in their capacity to arbitrarily relate events in a specific way, called Relational Frames. The properties of this kind of relational responding include the derivation of mutual relationships (e.g., if A is greater than B, then B is less than A); relationships arising from combinations (e.g., if A is greater than B, and B is greater than C, then C is less than A); and the change in functions of specific events based on their relations to others (e.g., if A is just like B and you become afraid of B, now you also associate fear with A) in certain contexts. There are different kinds of relational frames—equivalence, greater than, less than, etc. Deictic frames are a specific family of relational frames, such as “you” vs. “I”, “here” vs. “there”, and “then” vs. “now” that describe a relationship with reference to the speaker’s perspective, and are seen as critical for perspective taking.
The core processes of ACT
Acceptance and Commitment Therapy (ACT) is a clinical derivation and application of RFT with its own model of psychopathology and intervention. ACT consists of six core processes: Present Moment, Self-as-Context, Acceptance, Defusion, Values, and Committed Action (Hayes et al., 1999; 2006) (see Figure 1). Present moment refers to the non-judgmental awareness and experience of psychological and environmental events in the present; in essence, it captures many important facets of mindfulness as it is commonly applied in current psychological literature. Self-as-Context refers to the sense of self that arises from perspective taking (as in RFT), so that one is in contact with the “self” as the context in which psychological events occur as opposed to (mis-)taking psychological events such as thoughts, feelings, roles and other conceptual identities as the literal “self.” Acceptance is often clinically operationalized as the willingness to experience in contrast to avoidance. It is distinguished from some common notions associated with acceptance such as defeatism. Defusion contrasts ACT with CBT’s emphasis on cognitive restructuring. Instead of focusing on changing the content of one’s thoughts, in ACT there is an emphasis instead on “deliteralizing” thoughts; that is, training one to see thoughts as merely thoughts, and reverse the tendency to become “fused” with our thoughts or equating thoughts with reality. Values refer to the clarification of and being in touch with personalized values that matter to the individual in various life domains, such as health, family, work, friendship, community, and spirituality. Values are distinguished from goals as a value is likened to a direction (e.g., east) that serves to guide one’s behaviors rather than an endpoint in itself. Even though goals may be pragmatically used in therapy, the process of aligning actions in accordance with one’s values is emphasized rather than focusing on achieving outcomes. Finally, Committed Action refers to developing patterns of behaviors that are consistent with values, as opposed to actions driven by unworkable internalized rules and schemas (where there is “fusion”), avoidance (where there is lack of acceptance); or conceptualized past and future (where there is lack of contact with the present moment).
Acceptance and Commitment Therapy core processes.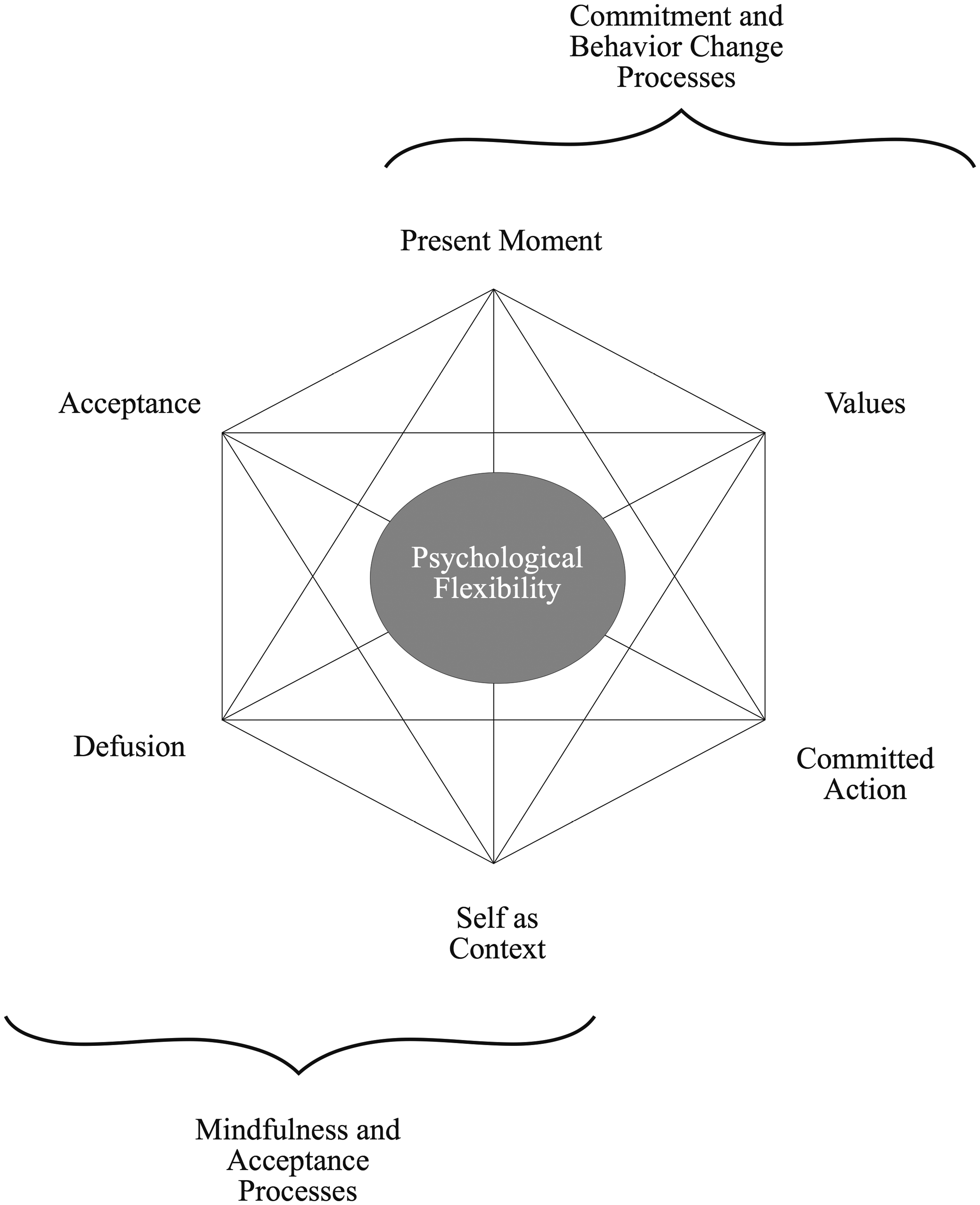
Comparison of ACT and Buddhism
There are a lot of similarities between ACT and some of the common tenets in Buddhism, and yet, there are differences within these correspondences. As the philosophy and beliefs of Buddhism are deep and complex and there are many different branches of Buddhism, we will focus only on a few important common and basic doctrines. The Four Noble Truths is one of the central doctrines underlying Buddhism.
The Four Noble Truths are that: (1) there is suffering (dukkha); (2) the origin of dukkha can be known (and it is caused by ignorance, desire/attachment, and aversion); (3) the cessation of dukkha is possible (by “letting go” of desire and attachment); and (4) the cessation of dukkha is through the Eightfold Path (Bodhi, 1994; Nĥt Hạnh, 1991; Santina, 1984). The Eightfold Path is often grouped into three clusters: Wisdom: (1) Right View and (2) Right Intention; Ethical Conduct: (3) Right speech, (4) Right Action, (5) Right Livelihood; and Concentration of the Mind: (6) Right Effort, (7) Right Mindfulness, and (8) Right Concentration (Bodhi, 1994; Nĥt Hạnh, 1991; Santina, 1984).
It is taught that with ethical conduct and proper concentration and cultivation of the mind, wisdom can be achieved. This leads to joy and happiness in the current life. Further, from the perspective of the ultimate dimension, ignorance, which gives rise to desire and attachment, will be dispelled by wisdom, and hence, the end of suffering, enlightenment, and freedom from Samsara, the cycle of rebirth, will be achieved (Nĥt Hạnh, 2006; Santina, 1984). Related core concepts in Buddhism include the Three Dharma Seals: impermanence—that all phenomena change; non-self—there is no true permanent self-nature in anything and everything is dependent on other conditions to arise; and nirvana—the extinction of ignorance, which includes deep understanding and perception of the true nature of things in the current dimension through the first two seals, enabling contact with the ultimate dimension and the end of suffering (Nĥt Hạnh, 2006). According to Buddhism, enlightenment and the realization of the true nature of things are not attained merely by faith or intellectualized understanding, but rather, through learning and progressing through personal experience, practice, and meditation, supported by a community, the Sangha (Nĥt Hạnh, 2006; Santina, 1984).
Similar to the First Noble Truth, ACT also holds the view that life is suffering, and questions the assumption embedded in most psychotherapies that consider “happiness” as the true state of normal health. For example, the popular self-help book The Feeling Good Handbook (Burns, 1999) in CBT stands in contrast to the ACT self-help book The Happiness Trap (Harris, 2008). In fact, one of the ACT techniques, Creative Hopelessness, often employed at the beginning of therapy, is used to help the patient realize the futility of avoiding the manifest symptom, whether it is depressed mood, anxiety, or pain, which then lays the groundwork for fostering Acceptance (Hayes et al., 1999).
In ACT, unpleasant feeling states like sadness and anxiety are not necessarily seen as inherently abnormal or unusual, nor are their underlying thought patterns and schemas. Rather, somewhat analogous to the Second Noble Truth, ACT posits that psychopathology and many forms of suffering result from our fusion or attachment to our internal experiences including our thoughts, rules, and narratives, confusing them as being real and then avoiding pain and unpleasant feeling states in preference to short-term relief (Hayes et al., 1999). At the psychological level, we are hooked and entangled by our thoughts and mistaking them as the truth.
The “letting go” of our attachment is facilitated by core ACT processes including Defusion—seeing thoughts as thoughts including any evaluative judgments or future worries, Acceptance—the willingness to accept internal and uncontrollable experiences, Present Moment—the presence and awareness of the now, and Self-as-Context—not confusing ideas, concepts, and other internal experiences with a sense of a self (Hayes et al., 1999). These core processes are consistent with the practice of mindfulness as described in the Eightfold Path.
Evidently, there is a parallel between the Four Noble Truths and ACT’s approach to resolving mental health problems. Further, both emphasize the importance of experiential learning rather than intellectualized understanding alone. Compassion and connectedness with others are fostered through the Eightfold Path in Buddhism and often naturally through the core processes in ACT (e.g., increased acceptance of others, decreased fusion with thoughts that lead to anger, increased mindfulness, and increased contact with personal values including relationships with others).
There are a number of notable and important differences between ACT and Buddhism as well. ACT is based on RFT and Functional Contextualism and aims to promote psychological therapeutic outcomes and a meaningful life, while Buddhism has its own philosophy and doctrines to promote spiritual awakening and enlightenment. Thus, the suffering referred to in Buddhism includes Samsara and the cycle of rebirth, while ACT focuses mainly on patients’ target concerns and other difficulties in life from a psychological perspective. The outline of moral conduct in the Eightfold Path is more explicit and prescriptive in Buddhism and differs from the emphasis on personalized values in ACT. In this case, it can be argued that there is an assumption that the personalized values will be inherently “good” (Hayes et al., 1999); the frame of psychotherapy is also setup to avoid the therapist imposing values on patients. In fact, patients are encouraged to ensure that their freely chosen values are individualized values versus collective values. Adhering unreflectively to collective values may be seen as a form of pliance, a kind of inflexible rule-governed behavior. In clinical practice, the relative emphasis on individualized versus collective values is often a source of tension and a potential pitfall in cross-cultural psychotherapy (Hall et al., 2011), although this issue is hardly unique to ACT. Culturally competent practice is needed to facilitate the negotiation of value conflicts (Fung & Lo, 2012; Lo & Fung, 2003). In this instance, freely chosen values can be expanded to include collectivistic values depending on the particular clinical, cultural, and functional context (Hayes et al., 2011; Hayes, Strosahl, & Wilson, 2012).
While both Buddhism and ACT undermine the natural attachment to internal experiences including thoughts and feelings, the scope of “letting go” is much wider in Buddhism, including the attachment to a permanent self. In ACT, the notion of Self-as-Context does undermine various kinds of attachments to the self (e.g., thoughts, emotions, memories, roles, and predispositions such as “I am old”, “I am anxious”, “I am unlovable”, etc.). However, ACT does reinforce the experience of an enduring self from the perspective of an observer, clinically termed transcendent self, Self-as-Context or the observer self.
While this may appear to be an incompatibility with Buddhism, it is notable that ACT, similar to other traditional psychotherapies (Aronson, 2004), does not make a specific ontological claim about the existence of a permanent metaphysical self (Hayes, 2005; Hayes et al., 1999). Rather, from an RFT perspective, the observer self arises in language development out of deictic frames, and from the perspective of ACT, it arises out of experiential awareness (Hayes et al., 1999; 2001). In Buddhism, the concept of “no-self” is complex and is often experientially realized at a deeper level of practice (Aronson, 2004). Partly, no-self can be understood through related concepts of impermanence, everything fluctuates and changes, there is no stable permanent self that can be found (Nĥt Hạnh, 2006), and emptiness, nothing can be found as a separate entity that is independent of others (Nĥt Hạnh, 1991). Non-self elements can be found in the self, and the boundaries between self and no-self arise out of misperception and a dualistic way of thinking (Nĥt Hạnh, 2010). Further, the pursuit of whether a self either exists or does not exist can similarly be better understood from a non-dualistic Middle Way, that is, existence and non-existence is also an illusory binary paradigm (Nĥt Hạnh, 2010). This avoids a nihilistic misunderstanding that the self and everything do not exist (Santina, 1984). Thus, the use of a stable observable self is an effective clinical tool psychologically, with a different aim from realizing “no-self” in Buddhism for the purposes of enlightenment.
In Asian and other collectivistic cultures, it has been proposed that an interdependent self that is more inclusive of others (i.e., inclusive of family members or other identified in-groups) may play a more important psychological role than in the West, where an autonomous independent self is emphasized; thus, “we vs. they” rather than “I vs. you” may become an important deictic frame (Hall et al., 2011; Markus & Kitayama, 1991). While this has important cultural value in promoting social harmony, it is conceivable that from a Buddhist ultimate perspective, the “we vs. they” distinction can still be problematic in its dualistic nature, giving rise to undesirable emotions and attachment; hence, the teaching of non-self arising in the Asian collectivistic context. In this instance, from a similar ACT perspective, the rigidity of attachment to a conceptualized (interdependent) self can be just as problematic as a conceptualized (independent) self, resulting in fusion in certain clinical situations: for example, “We Asians are never like this, and can never do that … . ” Defusion in ACT, thus, may serve as countercultural strategies that help patients who struggle with certain rigid cultural scripts (Fung & Lo, 2012; Lo & Fung, 2003).
Therapeutic challenges of ACT in training and therapy
While there are therapeutic challenges in any system of therapy, the apparent or real relationship between ACT and Buddhism can lead to unique challenges and resistance when teaching or applying ACT clinically. For some non-Buddhists, mindfulness meditation may be perceived as a religious practice violating their own religious beliefs. On the other hand, some Buddhists have criticized ACT as not being “true Buddhism.” This is sometimes based on philosophical and theoretical critiques of what ACT promotes in comparison to the underlying Buddhist philosophies (e.g., “no-self” discussed above). Other times, this critique stems from a particular religious perspective based on different branches of Buddhism, common cultural conceptions of Buddhism by non-Buddhists, or personalized belief systems.
In group therapy, it is clear that some patients are able to make rapid gains with the ACT model while others have difficulty making use of it. For instance, some may get stuck on using mindfulness as a tool to directly eliminate suffering, even though this is counter to the therapeutic aim. If there is a correspondence between ACT and wisdom within Buddhism, it is not surprising that it may take time for patients to “get it”, just as it is expected that some Buddhist ideals may take years of reflection and meditative practice to achieve. From the standpoint of ACT, much like Buddhism, a verbal intellectualized understanding is insufficient and can be counterproductive. Metaphors and experiential exercises are used as therapeutic techniques to advance the six core processes. However, given that individuals have different preferred ways of learning, there is great variation in the ways that patients are able to benefit from commonly employed techniques. In addition, because ACT does not make a specific distinction between patients’ struggles and the universal struggles that we all have, similar challenges are commonly observed when running training workshops with therapists.
Adapting ACT for a Cambodian women’s group
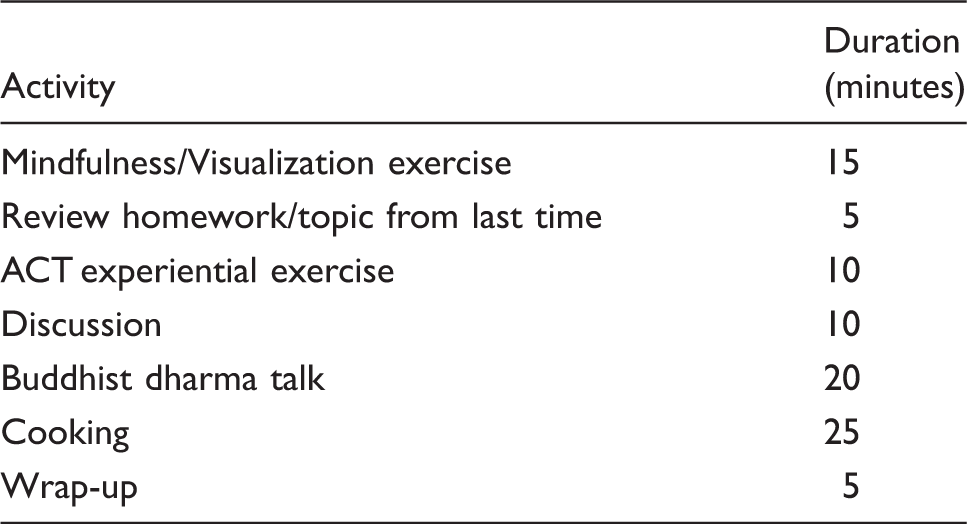
Format of Cambodian ACT-Buddhism group.
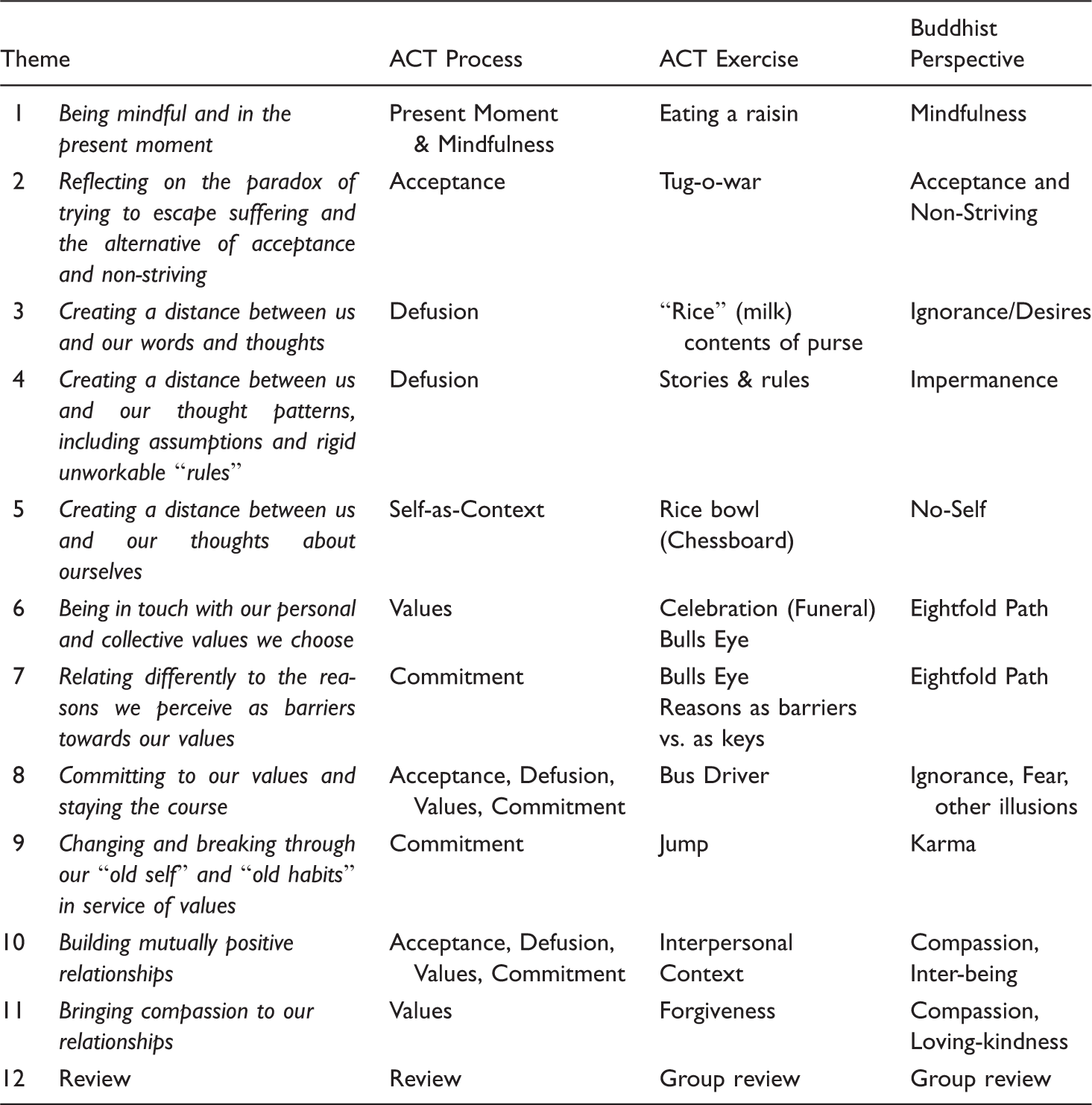
Outline of Cambodian ACT-Buddhism group.
The patients had chronic major mood and anxiety disorders, with limited or modest responses to medication treatment and most had considerable difficulty with individual therapy sessions. They all experienced trauma through the Khmer Rouge regime and had personal difficulties, such as marital and medical problems. The group also had a very low level of literacy and an attempt to use validated translated scales quickly proved invalid because they had a difficult time understanding the items even after interpretation and lengthy explanation, and resorted to consulting with each other communally for the “correct” answers.
In practice, because of logistic challenges, the attendance by the group members was irregular. It also became clear that homework assignments were mostly not completed. It was noted, however, that the participants enjoyed the group when they attended, often behaving in ways that were not seen in the one-to-one psychiatric follow-up sessions. For example, one of the members when seen individually had a difficult time opening up. When silence was used or when she was asked to close her eyes to do meditation, she seemed to comply in the session but appeared unable to focus or access her emotions. She later related to our mental health worker that she experienced these therapeutic techniques as similar to torture. However, she was able to participate more actively in the group including eyes closed meditation even though she encountered the usual challenges in meditation itself. Another elderly woman in the group, who had experienced both the trauma of Khmer Rouge as well as domestic violence from her husband, also opened up much more in the group than in individual sessions. As the oldest member of the group and the most religious, she showed deep reverence toward the Holy Monk and actively participated in the dharma discussion. When the group was cooking as a team, a hierarchy was quickly established based on age, and she was transformed from the role of a helpless traumatized frail old woman to a respected leader of the group, delegating responsibilities to complete cooking tasks.
Although similar messages were delivered through ACT and from the teachings of the Holy Monk, there were some significant differences. The ACT metaphors in some ways carried a similar message and played the same role as the teachings and stories told by the Monk. They both enhanced group members’ reflection and were followed by debriefing and discussion about their meanings and relevance to the patients’ struggles. However, the Monk’s stories carried rich cultural and religious meanings, and appealed to these references as strong rationale and motivation for change. For instance, a story about how the Buddha helped a bereaved widow to finally let go of her attachment when she realized the multiple past lives and relationships she had had drew on the concept of karma and rebirth. The belief in karma was a strong rationale for accepting current suffering and motivating change in behavior.
In addition, due to his position, the Monk was expected to be explicit in giving direct advice and teaching about the correct and incorrect ways of behaving and coping, drawing from Buddhist teachings and his past experiences of helping others in the community. For example, a group member who was angry and had a fight with her husband after feeling neglected significantly changed her interaction with her husband after hearing the Holy Monk discuss the common difficulties in marriage, the correct way of enhancing relationships, and his past interventions with other couples. This direct instruction extended to the teaching of mindfulness meditation. Compared to the clinician’s usual approach, the Holy Monk’s instructions were simple, made less use of imageries, included minimal use of facilitating verbal prompts, but included more direct and strict emphasis on the correct approach to strive for through the hard work of discipline and practice.
In terms of therapeutic relationship, the patients demonstrated tremendous respect to both the monk and the clinician. With the presence of the Holy Monk, this was elevated and even more apparently demonstrated through verbal and non-verbal means, including gestures in greeting and deep bowing. When cooking was involved, the session time was adjusted earlier as the Holy Monk was only to eat a single meal before noon. The patients would wait for us to start eating first before proceeding with their meals. They expressed gratitude and honor that we ate the food they prepared, and some even expressed astonishment that I as their psychiatrist would eat with them. In principle, ACT encourages a more egalitarian relationship between the patient and therapist to reinforce that we are involved with the same struggles, while acknowledging there are inevitable power differences. This was seemingly more difficult given the religious and cultural context in the presence of the Holy Monk.
While it was not possible to gather a quantitative evaluation of the group, qualitative feedback was obtained by our Cambodian mental health worker. The results were extremely positive about the group. They felt that they increased their knowledge of Buddhism from the Holy Monk’s teaching, including the correct Buddhist method of meditation and appreciation of the impermanence of life. They also felt helped by ACT and remembered several useful ACT exercises. In particular, many remembered the “rice bowl” metaphor, which I used to discuss the idea of Self-as-Context: just as a bowl which may hold rice and different kinds of food depending on the meal, their experience of their continuous observer self persisted in spite of the trauma, hardships, and suffering they experienced. This analogy added to their sense of psychological resilience. They also recalled the “bulls-eye exercise” which focused on the discussion of their values in their different life domains, including family, friends, health, and spirituality, which are mapped on a diagram of concentric circles like a target as a handout.
The participants also gave some ideas about their hopes for future therapeutic groups. They requested that more groups be run in this hybrid format. They thought that the group could continue to expand on interactive activities and have more cooking activities. They expressed the wish that there would be further development of “new models of therapy” that incorporate spiritual, medical, and psychosocial approaches to care.
Since the group ended, I have continued to follow most of the members in individual treatment. It is apparent that there was a positive change in the therapeutic relationship with the members, and we often make references to ACT or Buddhist ideas first discussed in the group. Most reported an increase in their own meditation or participation in Buddhism, such as through listening to dharma talks on the radio or the internet. The more religious as well as the more intellectual members of the group appeared to gain the most, while almost all had some degree of improvement. For example, one participant had voluntarily given up her children to child protection services due to her severe depression and hopelessness and later regretted this action. She was the most educated member of the group and was the only one who completed “homework” consistently, and she frequently helped others with the ACT concepts in the group. Her symptoms completely remitted with medication treatment, the ACT-Buddhism group, and our engagement with her husband and the family was able to get their children back.
Discussion
Further studies are needed to evaluate the efficacy of ACT in various Asian cultural groups, as there is limited clinical data in this area (Hall et al., 2011; Hayes et al., 2011). The potential enhancement of adding an explicit spiritual component in Buddhism to psychotherapy group treatment also warrants further study. Nevertheless, this pilot group experience has highlighted the potential power and importance of cultural and religious metaphors and their capacity for enhancing psychotherapeutic goals. Religion and philosophy traditionally play an important role in facilitating the process of healing and making meaning out of one’s life struggles (Frank & Frank, 1991). Psychotherapy, religion, and philosophy each may have distinct as well as overlapping contributions to helping patients with their problems. In clinical practice, therapists may find the use of cultural and religious metaphors helps patients grasp abstract concepts that are otherwise difficult to understand. Different models of collaboration between mental health practitioners and faith leaders, as explored in this group, can be further developed. This has implications beyond the specific application of ACT or the specific religion of Buddhism as discussed in this paper. Indeed, ACT itself can be adapted to other religious contexts. For example, there is notable overlap between ACT and Christian beliefs. The story of the Garden of Eden can be interpreted as a metaphor for the power and problem of thoughts causing suffering that ACT addresses in therapy (Hayes et al., 2012). While a detailed comparison is beyond the scope of this paper, there is an interest group within the ACT community exploring this overlap.
Conclusion
With the continued search for better approaches to treat mental health problems, there is increasing openness to borrowing from the wisdom traditions, philosophies, and practices of other cultures, including Eastern philosophy and Buddhism. In this initial exploration in theory and experience, ACT appears to be consistent with some of the teachings of Buddhism. Although each is based on different theories with different objectives, there is resonance and similarity in their approach towards alleviating suffering in a way which is somewhat counterintuitive to a more conventional Western approach. As articulated by members of the Cambodian therapy group I worked with, the challenge for the mental health profession is to continue the refinement of our therapeutic methods and develop models that incorporate diverse approaches to care, the psychological and the spiritual, the West and the East. Perhaps this is reflective of the Buddhist Middle Way as divisions are erased. However, this can only occur if we are open to different approaches while thoughtfully studying and incorporating practices and ideas in their deeper cultural context. The strength of science as a progressive discipline is that it is open to challenges that drive its evolution. Open, deliberate, and thoughtful cross-pollination between psychotherapy and other cultural and religious practices, even when there are apparent differences, may ultimately facilitate advances in psychology and psychotherapy.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Acknowledgment
I would like to acknowledge and thank Master Thích Nĥt Hạnh and Brother Phap Linh’s dharma teachings and Dr. Josephine Wong’s input, which clarified some of the Buddhist concepts discussed in the paper, as well as Venerable Nil Choeurn and Mony Mok for co-leading the Cambodian ACT-Buddhism Group with me.
Biography
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.