
Abstract
Expressions of anger within the healthcare context are a common occurrence, particularly in clinical situations where patients can experience emotional distress in the face of illness. The purpose of this study was to examine one aspect of this phenomenon by looking at expressions and causes of anger among Israeli cancer patients and their families from the perspective of oncologists who treat them. Twenty-two Israeli oncologists were interviewed from three oncology centers between March 2013 and June 2014. The grounded theory method was used to collect and analyze the data. Our study revealed that oncologists are exposed to and cope with expressions and acts of anger, aggression, and violence from some of their cancer patients and their families. The causes of this anger include physician blame, unrealistic treatment expectations, perceived errors in communication, and lack of follow up with bereaved families. Our study also revealed that the cultural context affected patient–physician interactions, including anger. This context included a culture that has open interpersonal boundaries and is family-oriented; a multicultural society that includes citizens with different cultural norms and expectations around cancer care; and a strained healthcare system that leaves oncologists limited in time and resources, including limited access to palliative care. Policy implications include reducing oncologist workload by hiring more mental health professionals, having translators available on site to help with language barriers, reducing administrative burdens, and incorporating palliative care widely to help with the psychosocial and physical care of patients and families.
Expressions of anger within the healthcare context are a common occurrence, particularly in clinical situations where patients can experience emotional distress in the face of physical illness. Anger can be described as a constellation of feelings, thoughts, and physiological markers in response to an upsetting internal or external cue (Bond, 2004). Expressions of anger may be verbal, physical, direct and/or indirect (Baty, 2010; Deffenbacher, 2011). Expressions of anger at healthcare professionals are common across nations (Derazon, Nissimian, Yosefy, Peled, & Hay, 1999; D’Urso & Hobbs, 1989; Hobbs, 1991; Hobbs & Keane, 1996; Kuhn, 1999; Ness, House, & Ness, 2000). Anger and violence towards physicians have been reported in Australia (Magin et al., 2011), the United Kingdom (D’Urso & Hobbs, 1989; Hobbs, 1991; Ness et al., 2000), the United States (Gates, Ross, & McQueen, 2006; Kowalenko, Walters, Khare, Compton, & MCEPWVTF, 2005), and Finland (Heponiemi, Kouvonen, Virtanen, Vänskä, & Elovainio, 2014).
Causes of anger within healthcare settings can include reactions to the experience and process of illness including discomfort (e.g. acute or chronic pain, living with a life-threatening illness, etc.); receiving negative information (e.g. bad news about a diagnosis or prognosis, finding out about a complication, etc.); long wait times, institutional depersonalization, bureaucracy, lack of communication, etc.; and negative interactions with healthcare personnel including perceived arrogance, disrespect, bias, humiliation, or feeling dismissed (Lown, 2007).
Anger in the oncology context
Within the oncology context, anger is considered to be a reasonable and expected response to facing one’s mortality, declining health and function, and disease and treatment symptoms (Kissane, 1994; Philip, Gold, Schwarz, & Komesaroff, 2007). Cancer patients and their families can experience anxiety, fear, and sadness among other intense emotions in response to their disease and to poor prognoses that may lead to death (Brintzenhofe-Szoc, Levin, Li, Kissane, & Zabora, 2009).
The Swiss psychiatrist Elizabeth Kübler-Ross suggested that anger is the second out of five stages in coming to terms with impending death caused by a terminal illness (Kübler-Ross, 1969). From a psychodynamic perspective, anger is a normal phase of the grief and mourning process that comes with the many losses associated with receiving a cancer diagnosis regardless of the outcome of the disease. These losses can include body parts, loss of function, loss of control over one’s body, and a sense of loss over one’s future. Feelings of vulnerability and powerlessness that come with a cancer diagnosis can also elicit expressions of anger that can potentially lead to sadness and depression over the disease and its trajectory. In this sense, anger in the oncology context is different to anger in other healthcare contexts that may be caused by impatience at long waiting times, or irritability towards physicians in the emergency room when people are under acute stress and anxiety. Within the oncology context, anger is associated with grief and loss and is considered to be part of an existential process of having to face one’s own vulnerability and mortality.
Observational studies in the oncology context have found that between 9–18% of patients and family members experience anger intense enough to be of clinical concern (Anderson et al., 2008; Kissane, Bloch, Burns, McKenzie, & Posterino, 1994). For example, in one study, morbid levels of anger were found in 9% of patients with advanced cancer, in 13% of their partners, and in 26% of their adult children (Kissane et al., 1994). Another study found that advanced cancer patients were more likely to express anger (53%) as compared to sadness (25%) and fear (21%), and that this anger ranged from moderate to severe (Alexander et al., 2011).
The expression of anger and the cultural context
While anger is a common reaction within the oncology context, the expression of emotions, including anger, is culturally contingent (Bond & Venus, 1991; Fernandez et al., 2014; Matsumoto, Yoo, & Fontaine, 2008). Anthropological examinations of anger across cultures have found that some societies are more likely to express anger than others. For example, while the Kaluli of Papua New Guinea freely express anger (Schieffelin, 1983), the Ukta Eskimos do not seem to feel or express anger at all (Briggs, 1970). Some social psychologists have argued that while anger may be a common human experience, “display rules”, or the social etiquette of expressions of emotion dictate whether anger will be outwardly expressed or not. For example, some studies have found that Japanese and American participants will express disgust and anger when watching a distressing video alone, but that only Japanese participants will hide their expressions of anger when the experimenter enters the room (Ekman, 1971; Friesen, 1972). As such, while anger may be a common occurrence in the oncology context, it is important to consider expressions of anger within the cultural context that they occur.
Anger in the Israeli healthcare context
Israel is a multicultural society that is home to Sephardi Jews (Asian/North African origin) and Ashkenazi Jews (European/American origin), Muslim and Christian Arabs, and Christians and other religious groups (Severance et al., 2013). Seventy-five percent of Israelis are Jewish, 20% are Arab, and approximately 4.5% are categorized as “other” (Central Bureau of Statistics, 2014). As such, within the healthcare context, Israeli physicians need to negotiate different cultural backgrounds and values, language barriers and challenges in communication (Landau & Bendalak, 2008; Van Londen, Hes, Ameling, & Hengeveld, 1990). Israeli oncologists see patients who come from all three of these ethnic backgrounds. Language barriers are found among patients and caregivers, but also among the healthcare personnel, many of whom are themselves new immigrants and who struggle with the dominant language (Landau & Bendalak, 2008).
While no studies have looked specifically at patient and caregiver anger in the Israeli oncology context, some research has looked at violence towards Israeli healthcare professionals (HCPs) in general (Carmi-Iluz, Peleg, Freud, & Shvartzman, 2005; Landau & Bendalak, 2008; Van Londen et al., 1990). One study that examined 177 Israeli physicians from both hospital and community clinics found that in the last year, more than half (56%) of the physicians reported at least one act of verbal violence and 9% reported exposure to physical violence (Carmi-Iluz et al., 2005). Another study that looked at emergency room medical and administrative staff in a general hospital in Israel found that 74% of the participants had experienced five or more violent incidents in the previous two years (Derazon et al., 1999). Another study that surveyed emergency room doctors in Israel in 25 general hospitals across the country found that 75% of the staff reported experiencing verbal violence in the previous year, 29% were verbally threatened with violence, and 16% had been physically assaulted by a patient or caregiver (Landau, 2004). Finally, a more recent study looking at a sample of 2,356 emergency ward personnel found that some patients engaged in verbal attacks (51%), verbal threats of violence (33%), vandalism in the hospital (22%), and physical attacks (11%). Some accompanying persons (often a family member of the patient) also frequently engaged in violent and aggressive behavior. Doctors reported that caregivers engaged in verbal attacks (55%), verbal threats of violence (36%), vandalism against property (22%), physical attacks (12%), verbal attacks on another staff member (46%), verbal threats against another staff member (41%), and physical attacks on another staff member (24%) (Landau & Bendalak, 2008).
Impact of patient and caregiver anger on healthcare professionals
In healthcare settings, workplace violence has been associated with lower job satisfaction and higher turnover among nurses (Quine, 2001; Sherman et al., 2008). Workplace violence can also affect HCP health (Kivimäki et al., 2003) and increase absences from work (Kivimäki, Elovainio, & Vahtera, 2000). Moreover, physicians have reported that workplace violence reduces job satisfaction and job performance (Heponiemi et al., 2014; Mirza et al., 2012). Other studies have found that workplace aggression and violence can negatively impact patient care (Arnetz & Arnetz, 2001), and reduce quality of life in HCPs (Carmi-Iluz et al., 2005).
In summary, given that anger and aggression are common in the context of oncology, and given the significant negative impact of this anger on healthcare staff, this study set out to examine the types of aggression expressed by patients and families and the root causes of this aggression from the perspective of oncologists. Moreover, we were interested in exploring how the local cultural context may relate to the presence of this anger and aggression.
Methods
Study design and participants
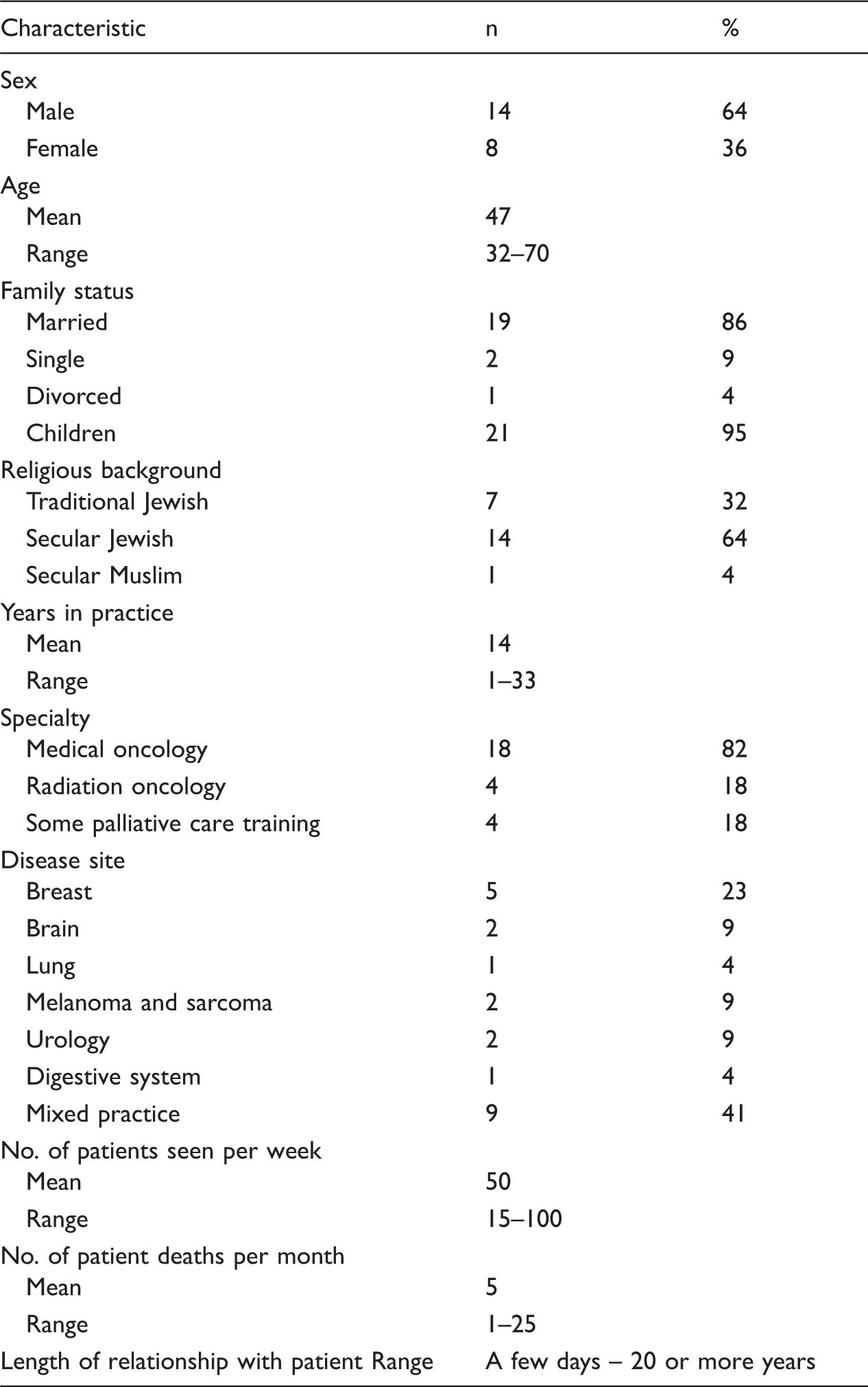
Sociodemographic characteristics of study participants (N=22).
Procedure
Ethics approval was obtained from the Research Ethics Board prior to launching the study. Potential participants were emailed information about the study by the oncologist co-investigators and asked to respond if they wished to be contacted about the research. Twenty-two oncologists responded to the email and none declined to be interviewed. Participants signed a consent form and agreed to the interview being audio-recorded with a digital recorder. A semi-structured interview guide was used and interviews were recorded and transcribed with all identifiable information removed from the transcripts. The analysis presented in this paper emerged from a larger study looking at oncologists’ experiences with patient death (Granek, Ariad, Shapira, Bar-Sela, & Ben-David, 2016; Granek, Ben-David, Shapira, Bar-Sela, & Ariad, 2017; Granek, Krzyzanowska, Tozer, & Mazzotta, 2012). Questions in the interview guide focused on the experience of patient death for the oncologists (i.e. felt experience when patients died, including cognitive, behavioral, and emotional reactions to patient death, etc.), impact of patient death (i.e. ways in which patient death affected oncologists’ personal and professional lives), protocol around patient loss (i.e. what do oncologists do when patients die in terms of follow-up care such as contacting families, etc.), difficult patient loss (i.e. what makes some patient deaths more difficult than others), and communication with patients about the disease and end of life. No specific questions were asked about either patient anger and/or violence towards the staff or about Israeli society. As such, in line with the principles of grounded theory, all data presented in this analysis arose spontaneously from the physician interviews with no specific probes about these topics. The study PI, who is a health psychologist and a trained qualitative researcher, conducted the interviews in the oncologists’ offices at a time and place that was convenient for them.
Data analysis
Data collection and analysis took place concurrently. In order to ensure reliability, the first five transcripts were coded independently by the study PI and the research assistant and later discussed to ensure consensus and agreement about emerging codes. Throughout the process of data collection and analysis, the study team met frequently to discuss emerging findings and to ensure consistency in the emerging coding scheme. Analysis was inductive and involved line-by-line coding with codes and categories emerging from participants’ narratives, and not from pre-conceived categories or codes. Coding was done by reviewing transcripts line-by-line and assigning sections of text to “meaning-units,” or to sections of text that carried a unified meaning (represented by a common theme). For example, whenever oncologists spoke about a lack of palliative care, these sections of text were moved into a created theme we called “lack of palliative care.” This theme eventually moved under the broader category of “Healthcare System” along with other themes that were relevant to this broad concept. In line with best GT practices, all the labels that represented emerging themes remained close to the data in order to provide the most accurate representation of the participants’ experiences and worldviews. Data collection stopped when the team determined that we had reached saturation and no new codes needed to be created. After coding all the interviews, a final coding scheme was developed. When looking at the data, we found that anger was a robust category that emerged in the oncologists’ narratives. As such, analysis for this paper involved extracting and analyzing the codes and categories that reported specifically on patient and/or caregiver anger, physician blame, and Israeli culture. The computer software NVivo 9 was used to store and organize the data.
Findings
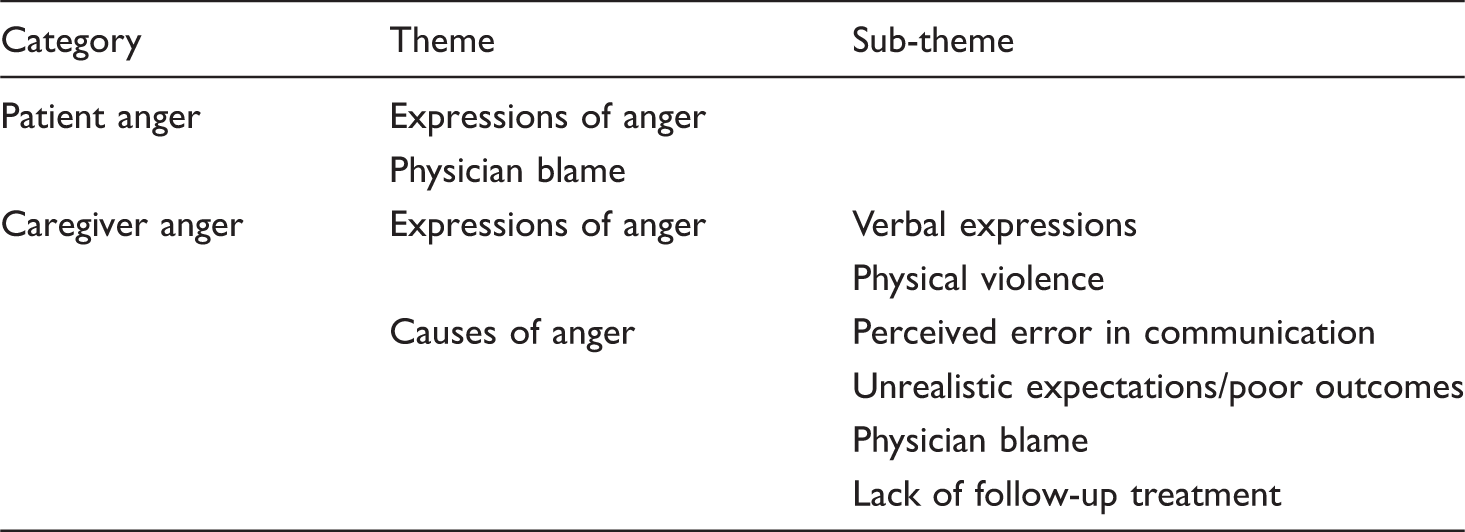
Expressions and causes of anger, violence and aggression in cancer patients and their families.
Patients’ expressions of anger
Expression of anger
Oncologists reported that they found some of their patients to be aggressive and demanding during the treatment trajectory and during end-of-life care. Patient expressions of anger included shouting, cursing, and failing to respect boundaries. On this subject, one oncologist remarked, “There are patients who are more aggressive. For instance, recently this woman came and demanded to see a doctor. I was about to leave already, I had finished my shift, but she demanded to talk with a doctor urgently. She was really aggressive, ran around the ward, and shouted.”
Physician blame
Oncologists reported that patients could get angry because they blamed the physician for their illness or its poor outcome. On this subject, one oncologist explained, “People come in angry and they are scared and they don’t want to die and they are constantly looking for someone to blame.” Another oncologist spoke about this type of anger in the context of deterioration of function in the patient: “When a patient deteriorates, they and I have a feeling that I might have missed something, or something had to be done differently. I think that usually when the disease erupts, it’s no one’s fault. But there’s this unpleasant feeling when the patient thinks—doesn’t matter if it’s true or not—that it’s my fault that the disease came back or progressed.” This sense of anger directed at the oncologist for a poor outcome or the suspicion that something was not done correctly was mentioned in different contexts. For example, another oncologist remarked: If a patient got healthy and now they are metastatic, I’m the one who informs them. Many times there is some denial that can go as far as blame. They wonder, “What went wrong. What would have happened if we had done the CT earlier? Who made a mistake? It can’t be true.” All these sorts of reactions. Sometimes they accept the bad news, and sometimes they direct their fear and stress towards the doctor.
Caregiver anger
When it came to caregivers, oncologists reported a number of different types of expressions of anger and different causes of this affect.
Expressions of anger
Oncologists reported both verbal and physical expressions of anger by family members. Verbal expressions included impatience, rudeness in tone, and aggressive speech. On this dimension, one oncologist remarked: “There are family members that come and immediately demand explanations, sometimes in a violent and aggressive way”; and another doctor explained: “Family members can be very irritated, very impatient and very rude. It happens a lot that the family explodes on me.” Oncologists also reported that while rare, families could become violent towards the staff, and in some instances, it was necessary to call security. While not common, physical violence or the threat of violence by family members was considered to be especially stressful for the staff. For example, one oncologist told the following story: “His daughter shouted at me. He tried to hit me with his cane. I had to call security. It’s rare that I have to call security, like once a year. But it’s very difficult for me.” Another oncologist, who had a similar experience, remarked: Once a patient’s son was very angry with me. I was examining his mother when he exploded on me, so I told him to leave or I’ll call security. He was very aggressive. Another time I had an argument with relatives on the ward. One family member came toward me like he was going to hit me. I was really scared and I did call security. It’s unpleasant.
Causes of caregiver anger
Oncologists reported that families got angry for a number of reasons that included perceiving that there was a communication error, blaming the physician for the disease, or for poor outcomes, and for perceived lack of follow up after a patient had died. Perceived errors could include even minor incidences of non-intentionally causing pain or distress, or instances where the oncologist was not sensitive or tactful in their speech. For example, one oncologist reported: “Once I placed a needle in a patient’s hand in the wrong way and it burned her a little. Later I met this patient and her brother when I was at the supermarket with my wife. She started yelling loudly: ‘Here’s the doctor that ruined my hand!’ Her brother wanted to pick a fight with me.” Another oncologist who acknowledged they may have spoken insensitively noted: “Out of complete tactlessness I said to the patient: ‘What was your job?’ Like, the patient was already a was. … From then on, there was terrible anger about everything I did.” As with patients, caregivers also blamed physicians about disease outcomes. They blamed the doctor for the patient’s death, for perceived poor treatment, and for being neglectful of their family members. Oncologists noted that although they recognized this anger was displaced and was a result of the stress of watching their family member struggle, and in some instances die from cancer, it was nonetheless a burden on the oncologist and reduced their quality of life and satisfaction with their work. Oncologists frequently discussed this burden, particularly in the context of families being angry with them for poor outcomes: There was one family that wrote a letter of complaint about me. I put a lot of effort to try and help him, and he just had a very cruel disease. They were always very grateful, and the minute the disease progressed their attitude to me turned and I became the one who killed their relative. There were families that were angry and resentful. They asked, “Why didn't this work? You told us this treatment would work. Why did you keep on with this treatment, and now you say it’s not working?” That’s actually a very common complaint. Anger at a treatment I recommended. They took the treatment, but it didn’t work.
Cultural context
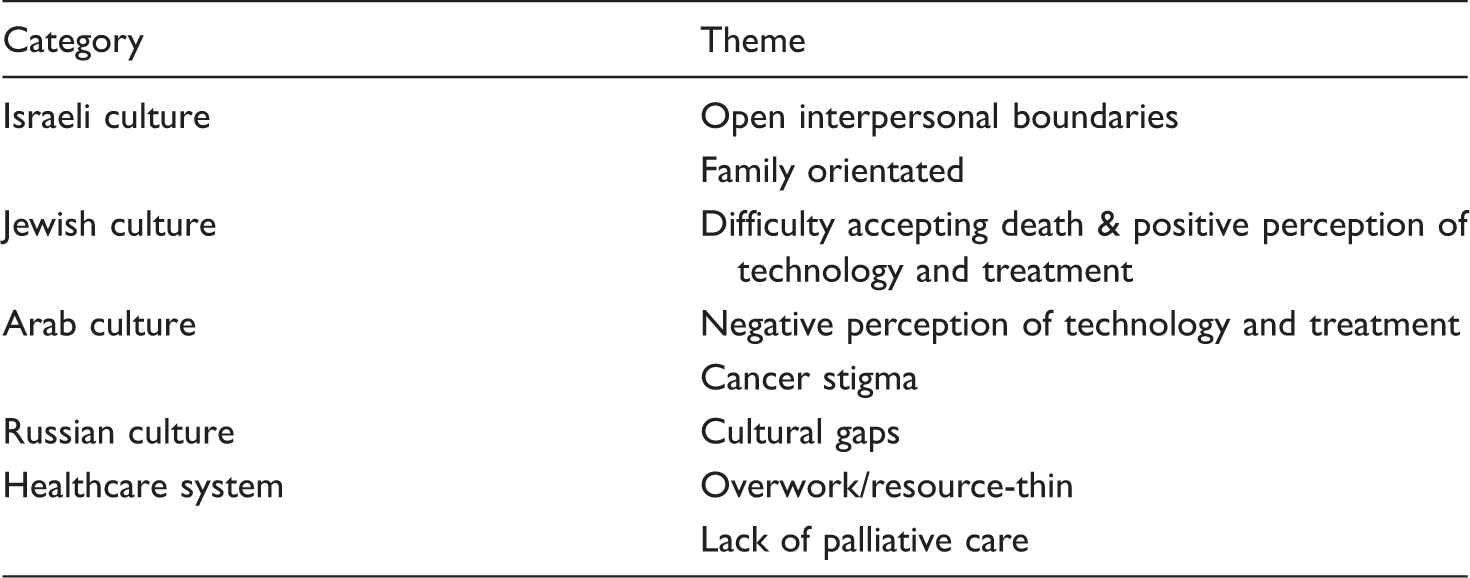
Israeli cultural norms and values.
Israeli culture
Oncologists reported that the two dominant religions in Israel (Judaism and Islam) share two fundamental characteristics that form an integral part of Israeli culture. The first of these common traits is open interpersonal boundaries, which is reported to be particularly prevalent among Israeli Jews; the second, is strong orientation toward the family, or family-orientedness.
Open interpersonal boundaries
Oncologists noted that open interpersonal boundaries among Israelis affected the doctor–patient relationship. Open interpersonal boundaries have to do with social and cultural expectations about psychological and physical distance between people regardless of where they sit on the social hierarchy. The phenomenon of open interpersonal boundaries is one that cuts across professions and disciplines and is common in Israeli society. People feel comfortable with little physical space between them, speak directly, intimately, and without reservation to each other regardless of their age, gender, status, and personal and professional backgrounds. In this sense, Israelis feel familiar and close to one another even when the other may be a stranger, or even in situations that people from other cultures may find inappropriate or intrusive. These open interpersonal boundaries were reported by the oncologists as a factor that made the patient–physician relationship particularly intense, satisfying, and difficult. The theme of open interpersonal boundaries arose with both patients and families. On the positive aspects of this phenomenon, one oncologist explained: There’s really an amazing relationship here between the family and the doctor. In comparison to other countries, here you don’t have clear boundaries in the doctor–patient relationship. There is a sense of familiarity and intimacy. They share things with you. You’re involved, in every detail of the patient’s life and their family. I don’t merely treat the patient, I treat the entire family.
The openness of these interpersonal boundaries also had some negative consequences for the physicians. These included the sense of always being available to patients and their families, their difficulty separating their personal feelings, and the sense of expectation that patients and families could have as a result of this familiarity and/or closeness with the oncologist. On being constantly available, one oncologist remarked, “In other countries, no one will have the doctor’s phone number and they won’t know where the doctor lives.” Another similarly explained: People arrive at any time for visiting hours and it is somewhat of a routine here that if you want to talk to the doctor you can do it at any time, regardless of what the doctor is doing. I remember one time, we were in the middle of CPR and a patient’s family came in and demanded that we talk to them!
These open interpersonal boundaries also led to emotional difficulties for the oncologists, particularly, as this oncologist noted, at end of life: In the Israeli culture, the doctor–patient relationship is more equal, friendlier. Patients give me gifts, send things to my house. Call me to talk about unrelated things. With some I really feel like friends. Then it’s much harder to say, “well, that’s it, we have nothing more to give.”
Family-oriented society
Oncologists reported that Israeli society is one that is family-oriented. As with the open interpersonal boundaries, there were some aspects of this cultural norm that were positive and some that were challenging for the oncologists to deal with. On the one hand, oncologists explained that this gave the patient a lot of support. One remarked: “Most of the patients arrive with their families. It’s something that is very special about Israel—everybody comes. Try entering any random room and you will see large amounts of people. Every day we have talks with many family members. After one talk, the brother comes, then the sister, and then the cousin comes to ask for more information.” Another similarly explained: “It’s Israel, it’s a clan. It’s very odd for us if you cope alone. We live in a state that was built to be very familial.” On the other hand, oncologists noted that this family-oriented society could make their work more challenging. Difficulties included being unable to speak directly to the patient because of the family’s wishes to withhold information, and trying to communicate with, or treat the patient with many people in the room. One oncologist reported: “It’s a stressful situation when 15 people enter the room.”
Jewish culture
Difficulty accepting death and positive perception of technology and treatment
In addition to speaking about Israeli culture as a whole, oncologists also spoke about the different cultural and religious backgrounds of their patients and how it impacted their ability to care for them. Oncologists noted that the Jewish religion emphasizes the sanctity of life and praises technology in the service of this goal; two aspects that make death particularly hard to accept for Jewish patients and their families. One oncologist remarked: Jews have a philosophy of life and death. It’s possible to see that from the attitude to abortions, to end of life, to resuscitations, and organ donations – these transition points into life and out of them are very complex. It’s very common for patients and families to approach this rabbi and that rabbi, and take drugs worth hundreds of thousands of dollars in order to feel that they did everything to fight the cancer. Maybe there’s something in the culture, both as Israelis and Jews, of some sanctity of life that we say that we’ll do everything. Even unreasonable things. We stretch the boundaries. It’s part of our improvisation as Israelis or as Jews. And bending rules is also a part of our culture. It could be that this also contributes to overtreatment. I’ve seen invasive procedures being done on dying patients here. We didn’t do those things in North America. We would be more accepting of the dying process. Here, they’re doing too much of the wrong things for helping people. There are families that don’t want to accept that that’s it, it’s over, and now you only need to support the patient. They bring second opinions. Such families interrupt our work. I see patients receiving fourth line of chemotherapy because the family is pushing for more treatment. I even see patients dying with an infusion of chemotherapy.
Arab culture
Negative perception of technology and treatment
Oncologists remarked that in some religious families from a Muslim background, cancer and its challenges were perceived to be a test from God. In such cases, Muslim families are sometimes reported to choose to forgo certain treatments, including pain medication, particularly at end of life. One Muslim oncologist remarked: “In the Arab sector there are religious families that only believe in religion. They don’t believe in morphine, they don’t believe in radiation. They say this is what God gave.”
Cancer stigma
Oncologists also reported that some of their Arab patients held a stigma around cancer that made it particularly difficult for them to communicate with their patients about their condition. This difficulty was compounded by the uneasy feeling they had that the patient’s family was not accurately translating medical information to their patients. One oncologist reported: “Some Arab families are not willing to tell the patients anything. The patients do not always understand that it’s cancer. The families refuse that we tell them. They translate, they say whatever they want.” Another similarly noted: “If I treat a Bedouin woman, she doesn’t understand any Hebrew, and her family—I don’t know what they translate. So she might not understand her condition.”
Russian culture
In the early 1990s up until recently, approximately 1 million Jews immigrated to Israel from Russia (the former Soviet Union). This massive absorption posed many challenges in cultural integration for this group. Oncologists in our study remarked that these cultural integration challenges were also prevalent in the sphere of cancer care. In particular, oncologists spoke about cultural gaps with Russian patients including unrealistic expectations for the type of care they could receive and communication gaps that had to do with a more formal sense of boundaries between patients and doctors than is the case in Israel. On this, one oncologist explained: “Many times there are very difficult conflicts between the Russian patients and us. Sometimes, the Russian population behaves as if they need to receive exclusive service. Or they get mad at me for not speaking Russian. They get really angry.”
Another oncologist related a different type of cultural gap when they explained: There is a sense of familiarity and intimacy in Israel. Sometimes they overdo it a little. … With patients who come from Russia, you see the difference in the patient’s behavior. Let’s say when a patient comes in … until I say, “sit down”, they won’t sit. Until I ask, “What’s going on? Start at the beginning,” they won’t say a word.
Health care system
Overwork/resource thinness
Oncologists reported that the workload in Israel is immense both because of the numbers of patients and families and because the healthcare system is resource-thin. This combination of an extremely strained system with a tremendous workload led many oncologists to describe themselves as exhausted, burned out, and at times angry themselves. On this, one oncologist remarked: Many doctors work while distressed because of lack of time, lack of power and so on. A distressed person is an angry person because they want to find someone to blame for their distress, and it’s not like they are going to break the walls at the management office. So they are mad at whoever is near and sometimes at their colleagues.
Lack of palliative care
Compared to North America, palliative care is relatively underdeveloped in Israel and is often practiced by an oncologist rather than a separate palliative care team. The oncologists described the lack of access to palliative care as a challenge of the system that affected their ability to provide the best possible care. The issue of time limitations and lack of expertise in the area put more strain on the already overburdened oncologists. On this topic, one participant remarked: We see so many patients, 15 minutes per patient. When we do palliative care, it’s an hour per patient. People say: “You talked with me, you were there for me. Where was this type of care until now?” It’s amazing to see this response anew every time. Palliative care is not that kind of assembly line.
Discussion
Our study revealed that Israeli oncologists are exposed to and must cope with expressions and acts of anger, aggression, and violence from some of their cancer patients and their families. The causes of this anger include physician blame, unrealistic treatment expectations, perceived errors in communication, and lack of follow up with bereaved families. Our study also revealed that the Israeli context deeply affected patient–physician interactions. This context includes a culture that has open interpersonal boundaries and is family-oriented; a multicultural society that includes Jewish and Arab citizens with different cultural norms and values around cancer care; and a strained healthcare system that leaves oncologists exhausted and limited in time and resources. All of these factors affected patient and family care. In the discussion that follows, we weave together these two sets of findings to provide a contextualized and culturally sensitive explanation for the presence of anger, aggression, and violence in the Israeli oncology context.
On the whole, oncologists perceived that their patients and families were angry because they either felt they had experienced poor care or had unrealistic expectations about their disease. The oncologists corroborated these points when they talked spontaneously about Israeli societal norms. For example, while it is understandable that patients and families might have unrealistic expectations of their physicians in all cultural contexts, it is more likely that patients and families will verbally and physically express this anger in a society that has more open interpersonal boundaries. The multiculturalism that oncologists reported on also provides a good cultural explanation for instances of anger and frustration on the part of patients and families. Oncologists reported struggling with the chronic negotiation of their patients’ and families’ cultural needs as it pertained to communication, treatment, and follow-up care. As a society that includes a variety of religious and ethnic groups, the Israeli context presents a challenge to oncologists, who are exposed to a tremendous variance in beliefs and values about care. Patients and families also experience these challenges as they struggle to communicate across language and cultural barriers, potentially leading to displaced frustration and anger towards the oncologist. Finally, in addition to cultural challenges, oncologists also reported being constrained by time and energy, and often feeling drained by an overburdened healthcare system. Many acknowledged in their interviews that overwork within these systemic constraints did not allow them to give their patients the kind of care they wished they could provide. These observations from oncologists thus seem to corroborate the reported causes of anger and aggression from the patients and families.
While the local cultural context provides one explanation for expressions of anger, our findings indicate that there is a strong relationship between overburdened healthcare systems, stressed oncologists, and the quality of care that patients and families receive, all of which may lead to anger and aggression towards oncologists. This anger and aggression, in turn, compromises the quality of life of the oncologists, and thus the quality of care for patients and their families. This dynamic presents a dangerous loop that may become self-fulfilling without institutional intervention. Other research has corroborated these links. In the oncology context, the literature indicates that patient and caregiver expressions of anger have a negative impact on oncologists including job dissatisfaction and burnout (Blanchard et al., 2010; Eelen et al., 2014; Philip et al., 2007).
Conclusion
Our research could inform policy first and foremost by suggesting a reduction of oncologists’ workload. This goal could be achieved by hiring more staff, including psychologists, psychiatrists, and other mental health professionals who can help with the emotional aspects of coping with cancer and its outcomes. Israeli oncology departments normally have one psychologist on staff working either part- or full-time, as well as a handful of clinical social workers to cope with the emotional needs of all their cancer patients and their families. These are insufficient resources to deal with the number of patients who require support in their emotional care. Trained psychologists can use empirically validated psychotherapeutic methods with patients and their families to address anger as a normal and expected reaction to the death and dying process (O’Grady, Dempsey, & Fabby, 2012).
In addition to hiring more support staff, as the oncologists in this study articulated in their interviews, the integration of palliative care in the oncology context is urgently needed in order to improve quality of life of the patients, their families and their physicians. The integration of palliative care can significantly reduce and potentially eliminate some of the patient and caregiver causes of anger noted in our study findings.
Palliative care focuses on the relief of symptoms, pain, and stress caused by a serious illness or its treatment, combining symptom control with provision of timely, accurate information and support in decision making (Field & Behrman, 2003). Although palliative care is often mistakenly viewed as end of life (EOL) care, the integration of palliative care should ideally be introduced early in the treatment trajectory to assist patients, families, and healthcare teams regardless of the eventual disease outcome (Waldman & Wolfe, 2013). Early integration of palliative care has been associated with better symptom management, better quality of life, fewer emergency room visits, and fewer hospitalizations in the intensive care unit (Dickens, 2010; Feudtner et al., 2011; Gans et al., 2012; Groh et al., 2013; Postier, Chrastek, Nugent, Osenga, & Friedrichsdorf, 2014). Moreover, the evidence indicates that cancer patients and their families report higher quality of life when patient and family suffering is reduced during the treatment of their disease and during EOL (Friedrichsdorf et al., 2015). Suffering can be reduced through the integration of palliative care which can include, but is not limited to: honest, open, and compassionate communication with families and patients, symptom alleviation, and the availability of psychosocial services such as psychologists or social workers to assist with the emotional difficulties associated with the disease and its treatment (Jones, 2006; Kassam, Skiadaresis, Alexander, & Wolfe, 2015; Wolfe et al., 2008).
Research indicates that adults who are referred early to palliative care live a greater number of days and have a better quality of life than those who do not receive palliative care (Temel et al., 2010; Zimmermann et al., 2014). Despite the importance of these services, and although palliative care and hospice services are covered under the socialized national health insurance law in Israel, only 10–15% of adult Israeli patients who could benefit from hospital and community-based palliative services have access to such services (Bentur, Emanuel, & Cherney, 2012). Moreover, existing services are extremely limited, and the majority of the 15 cancer centers that treat adults in Israel have limited or no physicians trained in the provision of palliative care. In addition to these structural barriers, as our study findings indicated, Israeli physicians face cultural barriers in providing palliative care to patients. A recent report noted that health providers in Israel face the challenge of respecting personal autonomy and providing quality EOL care, while also taking traditional values into account. This situation is further complicated by a lack of widespread familiarity with palliative care precepts among many healthcare professionals. Indeed, among the public, many fear that, in the terminal stages of their lives, they will receive more medical care and less pain relief than they want (Bentur et al., 2012, p. 41). With the exception of a few institutions, hospitals in Israel do not have formal palliative care teams that specialize in treating patients throughout their disease trajectory and at EOL. Instead, the primary oncologist is typically responsible for the majority of EOL physical and psychosocial care, a scenario which, as illustrated in our study findings, can emotionally and physically overburden doctors.
We recognize that this recommendation to increase staff and integrate widespread palliative care is difficult to implement. When compared to other OECD countries, however, Israelis spend significantly less on healthcare, and the budget for oncology services is reduced yearly (OECD, 2011)—a trend that can be reversed with the provision of evidence that this is harmful to patient outcomes. Moreover, in recent years, the Israeli Ministry of Health has set a mandate to improve access to palliative care services for its citizens. Freely available palliative care is especially important in the oncology context. While all citizens have socialized healthcare, some medical services in Israel are available privately. Oncology, however, is one of the few specialties where privatized medicine is not available, and as such, the workload for physicians is immense. The available research indicates that there is a strong link between oncologists’ work demands and quality of patient care. Several studies have found that job stress has a negative impact on communication with patients (Neumann et al., 2010; Neumann et al., 2007). For example, Neumann and colleagues found that job stress decreased physician empathy towards their patients and affected how patients and physicians communicated with one another (Neumann et al., 2007). Similarly, Groß et al. (2014) found that oncologists’ work stress led to impatience and irritability with patients. Finally, another study that surveyed 60 oncology personnel on an inpatient and palliative care unit found that 63% reported a “great deal of stress.” More than half (52%) reported that this workload “negatively impacted patient care.” Eighty-three percent reported that their workload “affected their ability to provide emotional support for patients,” and 89% reported that their workload “affected their ability to provide compassionate end-of-life care” (Dougherty et al., 2009, p. 107). This research demonstrates that oncologist workload negatively impacts patient care, that in turn may lead to patient anger and aggression.
Our findings also suggests that the language barriers and other issues resulting from cross-cultural miscommunication need to be addressed. Cultural and language translators, thus, should be on call at all the major hospitals in order to avoid facing the frustrations that come with being unable to communicate with the oncologist and the healthcare team. Finally, in addition to addressing healthcare infrastructure issues, it is important to take the cultural context into account. The question of aggression in Israeli society has been examined by other theoreticians in diverse fields and may illuminate some other factors that can explain the presence of anger and aggression in the oncology context. Some cross-cultural studies have looked at expressions of anger in Israeli society in general and found that Israelis express their anger more directly and openly than North American cultures, believing that this approach is more trustworthy (Hazleton, 1977; Schoenbrun et al., 1973). For example, in a cross-cultural study comparing Israelis and Americans, Margalit and Mauger (1984) found that Israeli students lost their tempers more easily and expressed their anger more forcefully than American students. In addition to the cultural acceptability of anger and the potential room for misunderstandings due to cultural and language barriers, other explanations for increased expressions of anger in Israeli society include the hot weather, shortages of healthcare staff, and the low status of the medical professional (Van Londen et al., 1990). These varied factors likely contribute to increased tension and irritability among HCPs, patients, and families. Moreover, the insecure political situation and the constant exposure to violence in Israel has also been offered as an explanation for the increased irritability and expressions of anger and violence among the population (Landau, 2003).
Limitations
Although the goal of qualitative research is to gain an in-depth understanding of a phenomenon rather than its breadth, our study is limited to a relatively small sample size. Further quantitative research is necessary to understand the breadth of this problem across the nation. Further research might also examine more psychologically-oriented factors related to anger and aggression in the healthcare context. For example, one line of inquiry may look at how different family structures facilitate different expressions of emotion in the oncology context.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.