
Abstract
This study examined the relationship between traumatic exposure, host language acquisition and mental health (posttraumatic stress, depressive and anxiety symptoms) in long-term resettled refugees. Participants included a community sample of Bosnian refugees (N = 138, 55% male, mean age of 40 years old) that had resettled in Australia and Austria on average 18 years prior. Two mediation models were tested based on two competing theories. Model A examined whether language acquisition mediates the relationship between traumatic exposure and mental health problems experienced by refugees. Model B examined whether mental health symptoms mediate the relationship between exposure to traumatic events and the acquisition of host language. Model A fit the data well (CFI = 1.00, SRMR = .017, RMSEA < .001, χ2 p = .526), while Model B was rejected as an acceptable model for the data (CFI = .556, SRMR = .136, RMSEA = .352). In Model A, the indirect pathway from trauma to mental health via language acquisition was significant for PTSD (β = .067, p = .028) and anxiety symptoms (β = .063, p = .026) but not depression symptoms (β = .048, p = .071). Intervention strategies aimed at improving host language acquisition may be important not only in successful adaptation to daily living in the host country, but also to improve the mental health of traumatized refugees.
Keywords
Introduction
Research focusing on refugees, asylum seekers and displaced populations has identified high prevalence rates of mental health disorders following exposure to traumatic war events (Fazel, Wheeler, & Danesh, 2005; Kirmayer et al., 2011), especially for those persons exposed to interpersonal and multiple traumas (Steel, Chey, Silove, Marnane, Bryant, & van Ommeren, 2009). In addition, research evidence identified that migratory factors associated with adapting to the host culture occupationally, socially and psychologically can exacerbate the mental health problems associated with exposure to traumatic experiences (Lindencrona, 2008; Porter & Haslam, 2005; Steel, Silove, Phan, & Bauman, 2002). Among migratory factors, host language acquisition is identified as a protective factor, buffering against the stress associated with adapting to the new environment and easing the process of completing daily living tasks (Beiser & Hou, 2001; UNHCR, 2001). On the other hand, inability to acquire the host language exposes refugees to additional stress, which negatively impacts their mental health (Robertson et al., 2006; Söndergaard & Theorell, 2004).
Research investigating host language acquisition has predominantly focused on non-refugee migrant populations. Less is known about the relationship between language acquisition and mental health among refugees and whether findings in non-refugee migrant populations are generalizable to refugees (van Tubergen, 2010). While there is robust evidence that past traumatic experiences commonly experienced by refugees affect mental health (Steel et al., 2009), little is known about the pattern and direction of the causal pathways between traumatic events, host language acquisition and mental health outcomes.
This study investigated two models used to investigate the relationship between traumatic events, host language acquisition and mental health in a sample of Bosnian refugees. The first model (Model A) proposes that while traumatic exposure has a direct impact on mental health, it also indirectly impacts mental health through its relationship with host language acquisition (see Figure 1). While there is no previous research into this proposed model, various studies provide support for the components of this model.
Proposed models explaining the relationship between traumatic exposure, host language acquisition and mental health. Model (a): Language acquisition mediates the relationship between traumatic exposure and mental health; Model (b): Mental health mediates the relationship between traumatic exposure and language acquisition.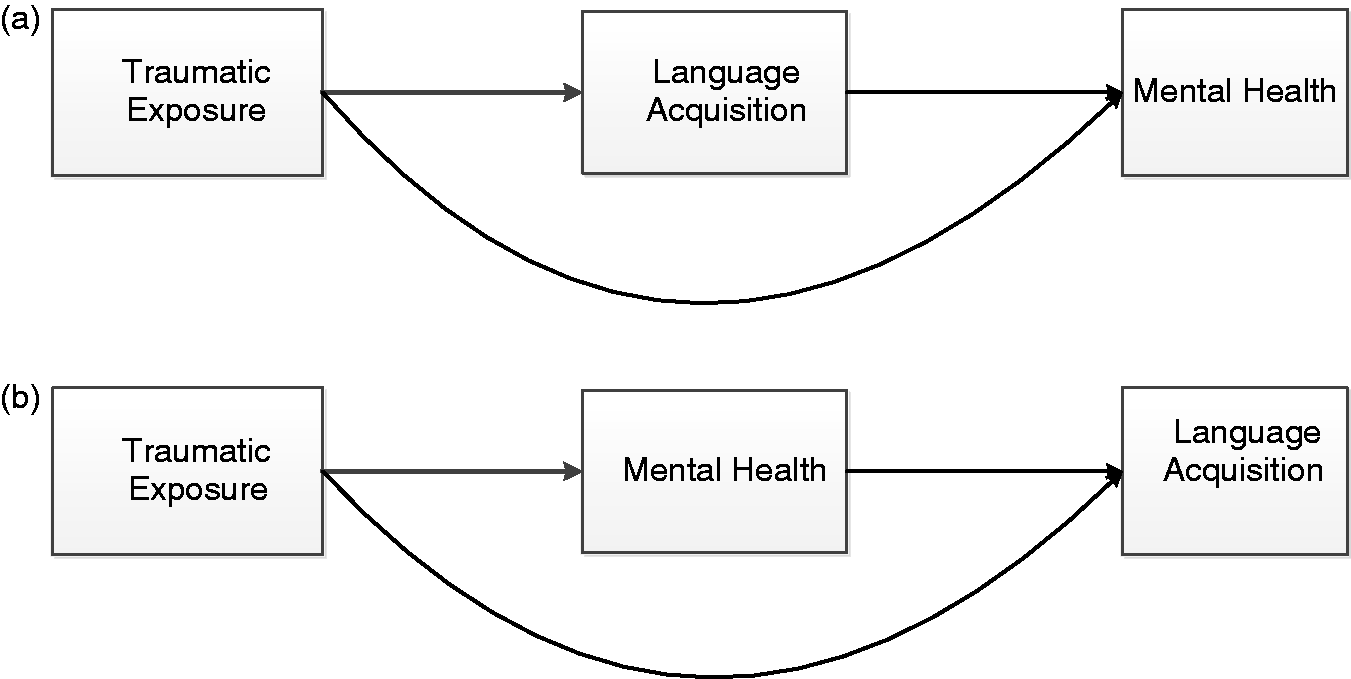
Trauma diminishes the capacity to deal with additional stress (Lindencrona, 2008), which indirectly increases vulnerability to stress related psychopathology (Matheson, Jorden, & Anisman, 2008; Schweitzer, Melville, Steel, & Lacherez, 2006; Steel, Silove, Bird, McGorry, & Mohan, 1999). Research indicates that language acquisition is an important stressor associated with the migratory process. Knowledge and familiarity with the host language is a major domain underpinning the process of acculturation that refugees go through during migration as they negotiate their participation in the new culture and maintenance of the origin culture and identity (Berry, 1997). The stress arising from this process associated with acquisition of host language is identified as a significant risk factor (Berry, 1997; Bogic et al., 2012; Ellis, MacDonald, Lincoln, & Cabral, 2008; Knipscheer & Kleber, 2006) predicting increased general distress, anxiety symptoms and even posttraumatic stress disorder (PTSD) symptoms (Beiser & Hou, 2001, 2006; Kartal & Kiropoulos, 2016; Schweitzer, Brough, Vromans, & Asic-Kobe, 2011; Silove, Steel, McGorry, & Mohan, 1998; Söndergaard & Theorell, 2004).
The second model (Model B) proposes that mental health symptoms associated with traumatic exposure affect the capacity to acquire the host language (see Figure 1). In this model, trauma exposure has an indirect relationship with host language acquisition, due to the direct relationship between trauma and mental health, and the subsequent relationship between mental health and language acquisition. Model B is supported by neurobiological research that finds that traumatic exposure alters the neural pathways in the brain that are associated with cognitive domains and executive functioning (Etkin, Gyurak, & O’Hara, 2013), with the largest effects on working and verbal memory, attention, learning and information processing (Bremner et al., 1993; Gilbertson, Gurvits, Lasko, Orr, & Pitman, 2001; Polak, Witteveen, Reitsma, & Olff, 2012; Scott et al., 2015; Shaw, Strother, McFarlane, Morris, Anderson, Clark, & Egan, 2002). These cognitive domains consequently play a role in second language acquisition. This proposition, however, has not been empirically tested. In addition, research in this area is predominantly conducted with veterans and the serving military, and hardly any studies have examined the impact of PTSD, depression or anxiety symptoms on executive functioning and language acquisition in refugees. Limited evidence suggested that traumatized refugees presenting with more severe PTSD symptoms acquire the host language at a significantly slower rate (Söndergaard & Theorell, 2004). This indicates that PTSD symptoms related to automatic processing problems, impairment in executive memory (Kanagaratnam & Asbjørnsen, 2007) and cognitive difficulties (Söndergaard & Theorell, 2004) may partially explain difficulties with acquisition of the host language.
To better understand the relationship between trauma, mental health symptoms and host language acquisition, this study examined which of the two above-mentioned models better explained the relationship between these variables. In particular, we firstly examined if host language acquisition mediates the relationship between traumatic exposure and mental health problems experienced by Bosnian refugees (Model A). Secondly, we examined if mental health symptoms mediate the relationship between exposure to traumatic events and acquisition of the host language (Model B). Furthermore, because there is evidence to indicate that language acquisition is predicted by age (Flege, Yeni-Komshian, & Liu, 1999) and length of residence (Beiser & Hou, 2001) and that gender is a significant predictor of PTSD (Armour, Elhai, Layne, Shevlin, Duraković-Belko, Djapo, & Pynoos, 2011), we considered the potential confounding effects of these variables. Finally, we also tested if the models differed between Bosnian refugees resettled in two different countries.
War and resettlement experiences of Bosnian refugees
The last census conducted in Bosnia at the brink of the war (1991) indicated a population of 4.4 million, of whom 43.5% were Bosniaks (or Bosnian Muslims), 31.2% Bosnian Serbs, 17.4% Bosnian Croats, 5.5% Yugoslavs and 2.4% represented other ethnic groups (World Refugee Statistics, 1997). During the Bosnian war (1992–1995) about 2.2 million Bosnians were uprooted and driven away from their homes, about 200,000 were wounded and more than 250,000 were killed, with Bosniaks the main target ((World Refugee Statistics, 1997); World Bank Group, 1998). Brutal crimes and war strategies led not only to mass forced displacement, but also to the reappearance of concentration camps, systematic rape and executions and mass destruction of cultural and religious sites and monuments (Power, 2002). The escalating crisis led to a massive population movement and the biggest refugee crisis experienced post-World War II.
The huge influx of refugees to Europe in the 1990s had a major impact on admission processes and the provision of asylum. Instead of provision of humanitarian protection and permanent resettlement, Bosnian refugees that arrived in Austria were almost automatically provided with a temporary protection visa; were housed in temporary accommodations; and were denied the right to work, receive welfare benefits or reunite with family members outside of Austria – despite the persecution and atrocities they had experienced (Bauer, 2008; Franz, 2005). As a result, these de-facto refugees found employment on the black market, enabling them to move out of crowded, temporary housing, and eventually acquired working and residency permits (Krause & Liebig, 2011). Unfortunately, this process usually took years to achieve, exposing individuals and families to many years of stress associated with the migratory process. Currently there are about 150,000 Bosnians living in Austria (Statistics Austria, 2011).
Bosnian refugees resettled in Australia usually arrived under government-sponsored humanitarian programs. These refugees were identified by United Nations Higher Commission for Refugees (UNHCR) as the most vulnerable (UNHCR, 2011). In the 1990s, Bosnians were the largest group of refugees who received humanitarian sponsored visas and were permanently resettled in Australia (Jupp, 2002). As such, they immediately received permanent residency and unrestricted access to all services afforded to Australian citizens, including access to health services and welfare support, as well as additional services including language training, housing and vocational support. In addition, refugees resettled permanently in Australia had an option to reunite with their immediate family members and bring them to live in Australia (DIAC, 2009). Currently there are about 25,000 Bosnians living in Australia, with the majority resettled in Victoria and New South Wales (ABS, 2013). This description illustrates the differences in the resettlement experiences in the post-migratory environments that these two groups of refugees faced upon leaving their war-torn country.
Method
Participants and procedure
Participants were eligible for inclusion in this study if they were at least 18 years old, were exposed to war events in Bosnia during 1992–1995 and resided in Australia or Austria during data collection (2012–2014). Options used to recruit participants included snow-ball sampling, online recruitment, advertising in local media (Bosnian newspapers, radio and television) and recruitment through social clubs and associations. Participants responded in an anonymous self-report survey via an online hosted website or a hard copy of the survey which was returned anonymously in a prepaid envelope. More than half of the participants (n = 78, 57%) used a hard copy version. There were no statistical differences between those who filled a hard copy or an online version of the survey for any of the outcomes including levels of PTSD (χ2 = 31.54; p = .29) depressive (χ2 = 17.86; p = .53) or anxiety symptoms (χ2 = 12.26; p = .66).
All measures used in the study were translated from English into Bosnian by the first author, who is a native speaker of the language, and then back-translated by an independent bilingual academic, so as to allow for comparison between the two translations. Any discrepancies in translation were resolved by discussion and mutual agreement between the first author and the bilingual academic. This study was reviewed and approved by the Monash University Human Research Ethics Committee certificate number CF09/32382009001758.
Measures
The questionnaire included a set of demographic questions (age, gender, education and marital status). Traumatic exposure was a cumulative measure assessed with a set of trauma history questions using yes/no answers assessing exposure to war-related (e.g., torture, concentration camp, killing) and other traumatic events (e.g., exposure to disasters, accidents and assaults) experienced during the participant’s lifetime. The information on trauma exposure was derived from assessment measures commonly utilized among refugee populations to assess war-related (i.e., Harvard Trauma Questionnaire, part 1 (Mollica, McInnes, Sarajlić, Lavelle, Sarajlić, & Massagli, 1999)) and life-time history of potentially traumatic events (CIDI (Kessler & Üstün, 2004)).
Posttraumatic Stress Diagnostic Scale
The Bosnian translation (Powell & Rosner, 2005) of the Posttraumatic Stress Diagnostic Scale (PDS; Part 3 only) (Foa, Cashman, Jaycox, & Perry, 1997) was used for the assessment of current PTSD symptomatology. This measure is based on the DSM-IV PTSD symptom criteria (APA, 2013) which included 17 items scored on a 4-point Likert scale (from 0 = not at all or only one time, to 3 = five or more times per week/almost always). The alpha coefficient for the current Bosnian version of the PDS was excellent (α = .97).
Depression and Anxiety Scale
The Depression Anxiety Stress Scale (DASS-21) is a 21-item self-report inventory designed to provide measures of the three related negative affective states of depression, anxiety, and stress (Lovibond & Lovibond, 1995). In the current study, only the depression and anxiety subscales were used to assess the presence of symptoms over the past two weeks. Items are measured on a 4-point Likert scale (0 = did not apply to me at all, and 3 = applied to me very much/most of the time). Alpha coefficients for the depression (α = .95) and anxiety (α = .92) subscales in the current sample were excellent.
Language acquisition
Language acquisition was assessed using a host language acquisition subscale from the Language, Identity, Behavioral Acculturation (LIB) scale (Birman, Trickett, & Vinokurov, 2002). Ratings are made on a 4-point Likert scale ranging from not at all to very well, like a native-speaker. The language acquisition subscale consisted of nine items asking participants to rate their ability to speak and understand the host language. The alpha coefficient in the current study (α = .95) was excellent.
Statistical analyses
Descriptive and bivariate correlations were performed using SPSS version 22.0 (SPSS INC., 2013). Path analyses were performed in Mplus version 7.0.1 (Muthén & Muthén, 2010) testing direct and indirect effects. Gender and length of residence were identified as potential confounding covariates and were controlled in all analyses. Subgroup analyses were performed investigating the fit of the model based on the country of resettlement. We relied upon a variety of model fit indices including the chi-squared goodness of fit, comparative fit index (CFI) (Bentler, 1990), the root mean square error of approximation (RMSEA) (Steiger, 1990) and the standardized root mean square residual (SRMR) (Vandenberg & Lance, 2000). Interpretation of the model fit was based on appraising multiple fit indices (Hu & Bentler, 1998, 1999). If the CFI values were <.90 the model was rejected. RMSEA values <.05 were considered a close approximate fit, values between .05 and .08 were considered reasonable and values ≥.10, indicative of poor model fit. A SRMR value near .08 was considered to support the model well.
Results
Participant characteristics
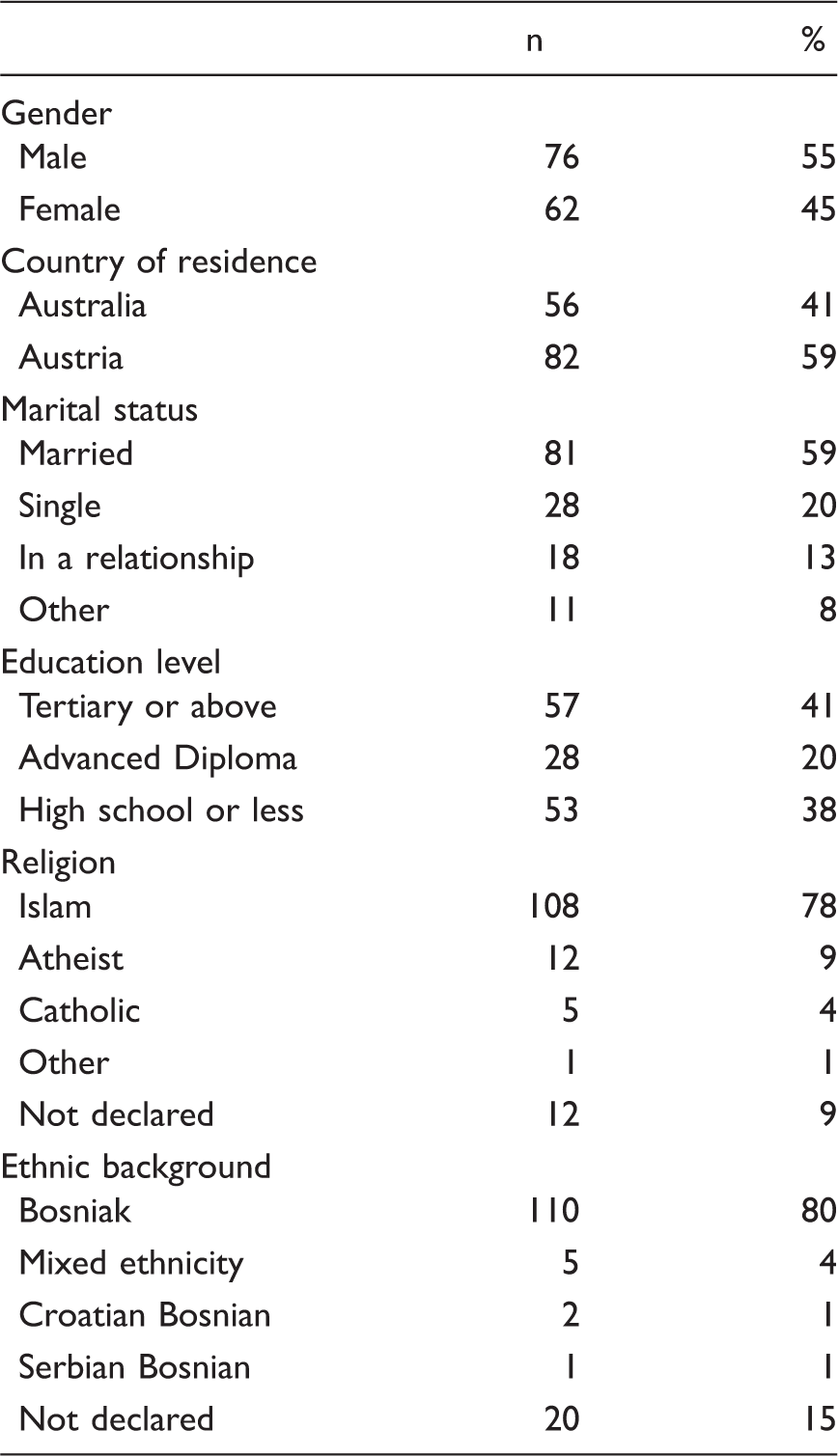
Socio-demographic Characteristics of Participants (N = 138).
Exposure to Traumatic Events Reported by Bosnian Refugees (N = 138).
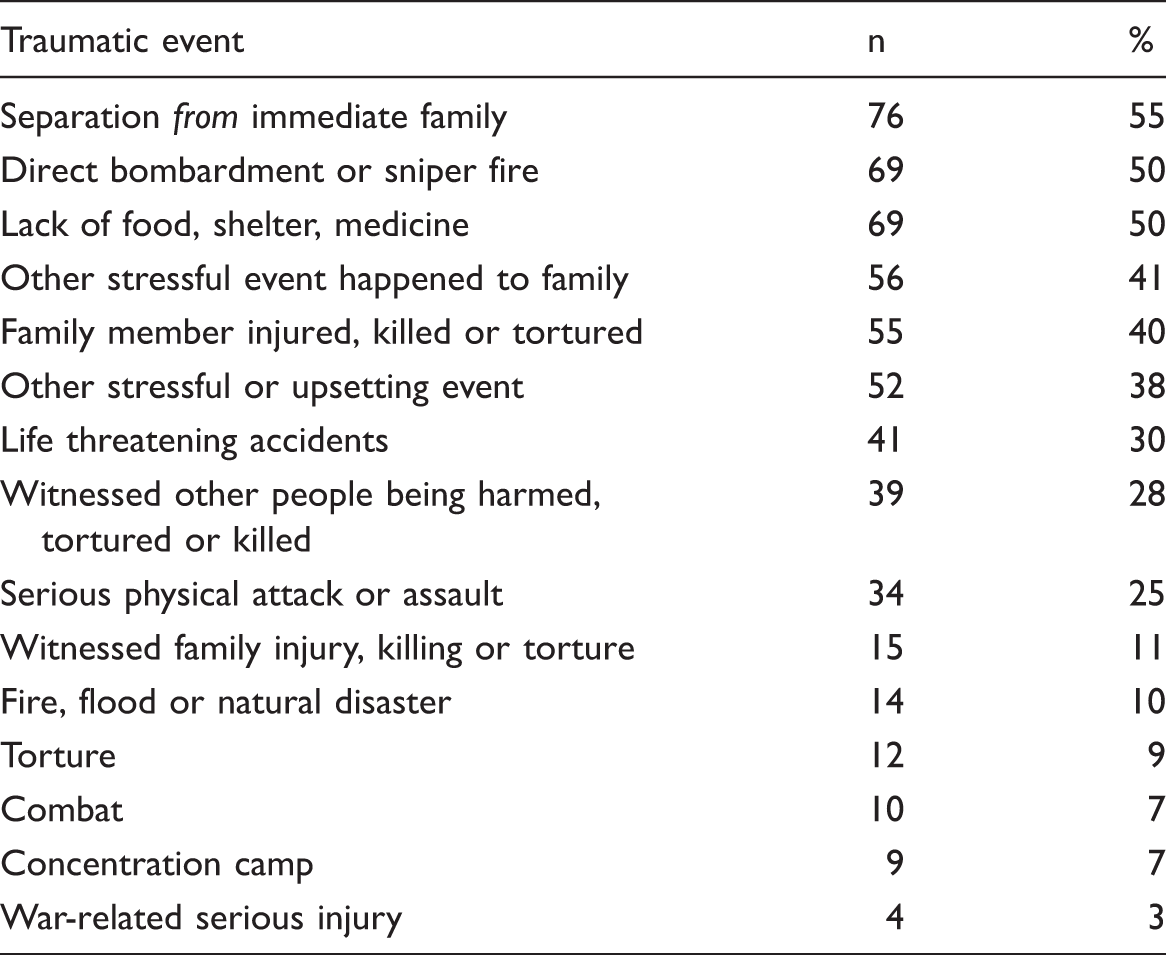
Eighty-two percent of the whole sample reported experiencing at least one traumatic event, while 70% reported experiencing three or more traumatic events in their life (M = 5.09, SD = 4.03, range 0–16). The most common experiences reported by participants include experiencing separation from immediate family members (n = 72, 42%), direct bombardment or sniper fire (n = 68, 46%) or lack of food, shelter or medicine (n = 68, 46%). There were no differences in traumatic exposure reported by men and women, but there were significant differences based on the country of resettlement with Australian Bosnians reporting more traumatic exposure M = 6.68 (4.00), than Austrian Bosnians M = 4.01 (3.70); t(136) = 4.02, p <.001.
Prevalence of Mental Health Outcomes
Severity of PTSD, Depressive and Anxiety Symptoms Across Bosnians in Australia and Austria.
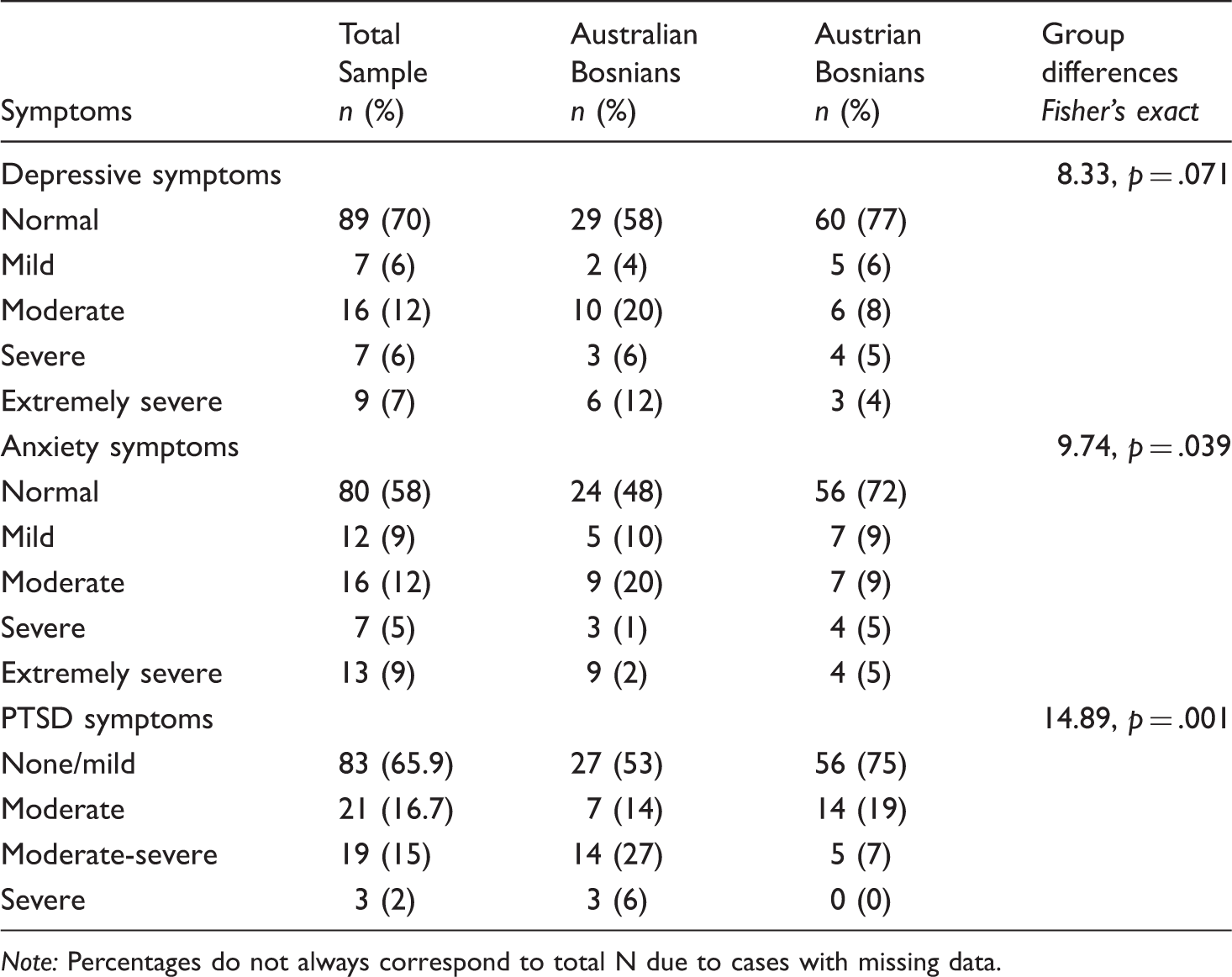
Note: Percentages do not always correspond to total N due to cases with missing data.
Association between language acquisition and mental health indices
Exposure to traumatic events was found to be positively associated with PTSD (.695), depressive (.600) and anxiety symptoms (.642) and negatively associated with host language acquisition (−.281). Furthermore, host language acquisition was found to be negatively associated with PTSD (−.411), depressive (−.296) and anxiety (−.359) symptoms.
Path model analyses
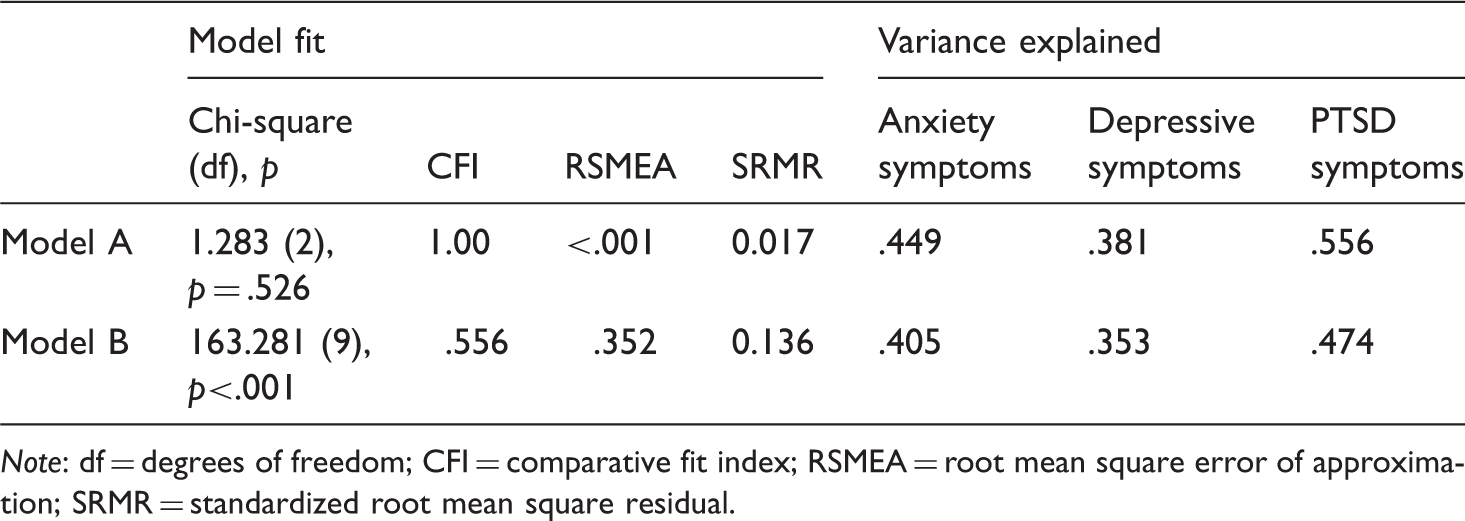
Separate mediation analyses tested two competing models about the roles of trauma, mental health and host language acquisition in refugees. Table 4 shows the goodness of fit indices for each of the competing models. Model A generated fit indices indicative of a well-fitting model. Importantly the finding of a non-significant Chi-square test is a rare indicator of how well Model A represents the data. In comparison the fit indices generated by Model B fail to support this model as being an adequate representation of the data. Importantly, with language acquisition as the outcome variable, all primary variables in the model other than PTSD (β = .659, p = .02) were non-significant predictors of language acquisition: depression (p = .18), anxiety (p = .14), traumatic exposure (p = .64). The CFI, RMSEA and SRMR scores were all representative of a poor-fitting model. Furthermore, Model A is a better predictor of mental health (PTSD, depressive and anxiety) scores than Model B as indicated by the higher levels of explanatory power (variance explained) detailed in Table 4. Therefore, we selected Model A (represented in Figure 2) as the best conceptualization of the relationships between trauma, host language acquisition and mental health in refugees. However, as shown in Figure 2, significant paths indicated that levels of host language acquisition mediated the relationship between exposure to traumatic events and PTSD and anxiety, but not depressive symptoms. Specifically, indirect effects of traumatic exposure via host language acquisition were statistically significant and indicated that language acquisition at least partially accounted for the relationship between traumatic exposure and the severity of PTSD (β = .067, p = .028) and anxiety symptoms (β = .063, p = .026), but not depressive symptoms (β = .048, p = .071).
Mediation Model A with the path relationship between trauma and mental health outcomes and mediated by host language acquisition. Significant parameters are indicated by black lines with standardized beta weights. The model controls for gender and length of residency. PTSD = Posttraumatic Stress Disorder. Fit Indices for the Path Models of Relations Between Traumatic Exposure, PTSD, Depressive and Anxiety Symptom Severity and Host Language Acquisition. Note: df = degrees of freedom; CFI = comparative fit index; RSMEA = root mean square error of approximation; SRMR = standardized root mean square residual.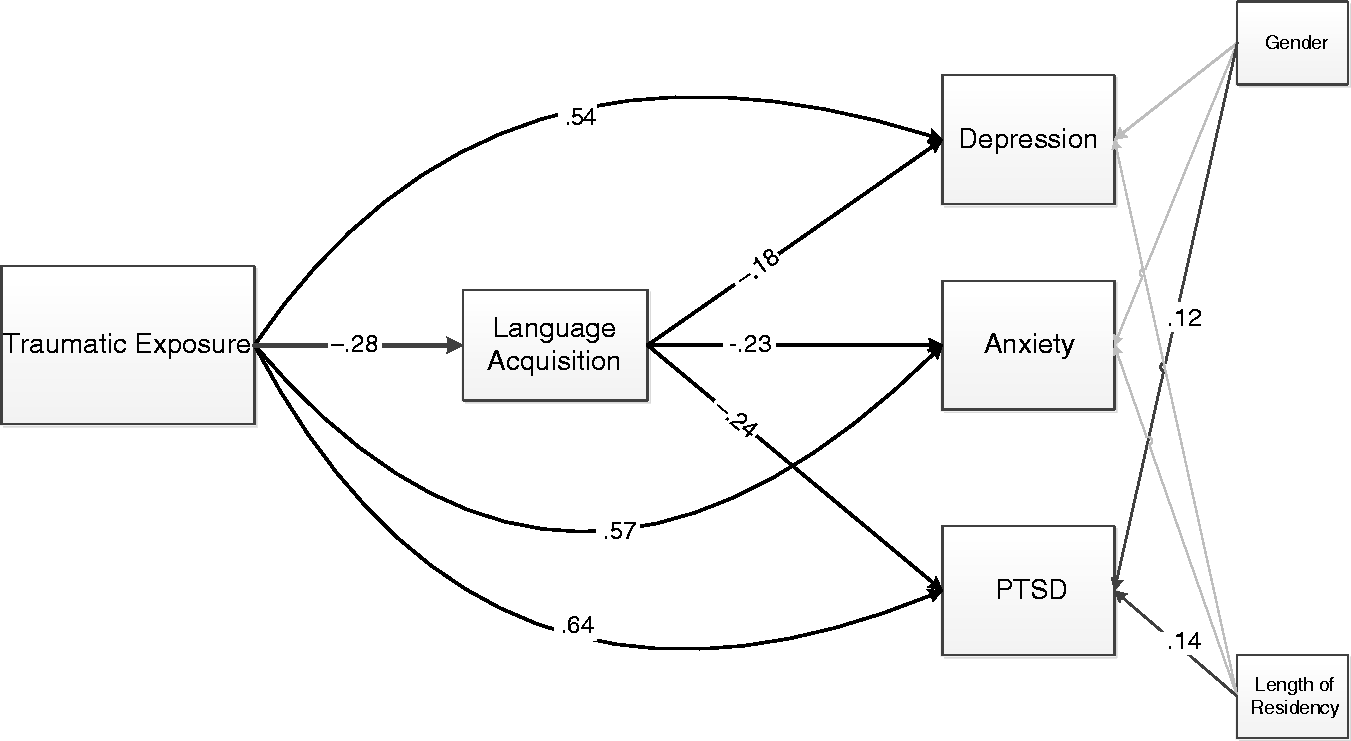
We also considered the potential confound of age in the analyses and tested a moderated mediational model following the approach recommended by Hayes (2013). We observed that age did not moderate the mediation model we have tested and therefore we can conclude this is not an important confound to our analyses.
Subgroup analyses
Subsequently we explored whether the path coefficients found in Model A differed between participants resettled in Australia and Austria. While it is not within the scope of this paper to report the full post-hoc analyses, the results indicated a robust model fit for both subgroups [Australia model fit: (X2(2) = 2.097, p = 0.350, CFI = 0.999, RSMEA = 0.029, SRMR = 0.036, SS-BIC = 1230.990); Austria model fit: (X2(2) = 0.438, p = 0.804, CFI = 1.00, RSMEA = 0.00, SRMR =0.012, SS-BIC = 1741.871)] with one significant difference in the pathways identified. Specifically, Wald tests (p = .013) indicated that the path coefficient between traumatic exposure and PTSD was stronger in Austria (β = .659, p <.001) than in Australia (β = .606, p <.001), therefore indicating that trauma history is a stronger predictor of PTSD in Austria than in Australia. However, with a β > 0.5, both models still observe a large effect for traumatic exposure and PTSD.
Discussion
Bosnian refugees in this study reported high levels of traumatic exposure to war and other traumatic stressors. More than two decades after the war, these stressors were still associated with high severity of PTSD, depressive and anxiety symptoms. These findings are consistent with studies conducted with other refugee samples (Fazel et al., 2005; Silove et al., 1998) and with Bosnian refugee samples in other countries (Knipscheer & Kleber, 2006; Mollica, Sarajlić, Chernoff, Lavelle, Vuković, & Massagli, 2001; Momartin, Silove, Manicavasagar, & Steel, 2003). Significantly higher levels of trauma experienced and reported by Australian Bosnians could be explained by their older age, which has been associated with more mental health symptoms in refugees (Bogic et al., 2012; Porter & Haslam, 2015). Varying degrees of exposure found in Australian and Austrian Bosnians are consistent with prior research conducted with ex-Yugoslav refugees, including Bosnians, resettled in European countries that identified varying degrees of exposure and posttraumatic symptoms across samples resettled in different countries (Bogic et al., 2012). Different resettlement trajectories could explain this difference between the samples and the higher severity of posttraumatic symptoms identified in Australian Bosnians. In particular, Australian Bosnians went through resettlement under the UNHCR scheme, which granted resettlement and residence to the most vulnerable and those who experienced particularly traumatic ordeals during the war (UNHCR, 2011).
Analyzing the two different pathways proposed to underlie the relationship between traumatic exposure, mental health and host language acquisition, the results clearly supported Model A, indicating that the relationship between traumatic exposure and mental health was mediated by host language acquisition. Whereas in Model A all paths met criteria for significance, all primary variables in Model B, with the exception of PTSD, were non-significant predictors of language acquisition. Thus, there was no support for the hypothesis that mental health status affected the relationship between trauma and language acquisition. It is important to remember that in Model A the direct relationships between trauma and mental health are still very strong, thus suggesting that difficulties with language acquisition are not the sole reason for mental health problems, but are a mechanism that worsens these outcomes. On the other hand, in Model B, trauma did worsen language acquisition, but the associated mental health problems were not observed to be a mechanism that further inhibited this skill acquisition beyond the influence already observed for trauma.
This finding complements the established evidence base on the cumulative impact of post-migratory stressors (Beiser & Hou, 2001, 2006; Bogic et al., 2012; Schweitzer et al., 2011; Schweitzer et al., 2006; Steel et al., 1999) and language acquisition in particular (Kartal & Kiropoulos, 2016; Robertson et al., 2006; Söndergaard & Theorell, 2004) on mental health outcomes in refugees. However, while this finding was significant for posttraumatic stress and anxiety symptoms, it only approached significance for depressive symptoms, suggesting that the mediation effect of host language acquisition varies based on the type of psychopathology. One explanation for these findings might be the duration of residence in the host country. Longitudinal studies conducted with refugees have reported that depressive symptoms start to decrease after prolonged residence (i.e., more than 10–12 years), which suggests that the early stages of resettlement are highly stressful but a stage of adaption is reached when stress starts to decrease with increased length of stay in the host country (Fenta et al., 2004; Tran, Manalo, & Nguyen, 2007). These results are consistent with findings in the current sample (mean length of residence in host country: 17.66 years), where the migratory stressor of language acquisition did not significantly impact depressive symptoms.
Importantly, subgroup analyses for country of resettlement found support for the mediating role of host language acquisition in both Australian and Austrian Bosnian samples. While there were differences in the direct relationship between trauma and PTSD, the overall findings suggest Model A is robust across different cultural approaches to migration. Indeed, language acquisition difficulties form significant psychological and social barriers to the adaptation and integration of refugees, difficulties that are often intensified by the wider host society. The process of segregation based on competence in the host language can lead to social exclusion and discrimination (Correa-Velez, Gifford, & Barnett, 2010; Sorgen, 2015), which have been associated with poor mental health outcomes (Aichberger et al., 2015; Ellis et al., 2008).
The importance of language acquisition and its effect on mental health and integration of refugees cannot be underestimated. Barriers to communication not only exacerbate the symptoms associated with pre-migratory traumas, but also limit adaptation and social integration (UNHCR, 2001), daily functioning (Beiser & Hou, 2001), participation in the employment market and job satisfaction (Birman, Simon, Chan, & Tran, 2014; Chiswick, Lee, & Miller, 2004). Therefore, difficulty with host language acquisition not only aggravates pre-existing psychopathology of refugees, but also inhibits adaptation to the new cultural landscape.
The impact of language acquisition difficulties on refugee mental health is also an important clinical issue. Inability to understand or communicate appropriately with mental health providers not only impairs the communication itself, but is also a barrier to access and utilization of services (Crosby, 2013). In Australia alone, linguistic barriers are associated with inaccurate diagnosis of mental illness, low hospitalization rates, longer hospitalization duration, and greater rates of involuntary admissions (Cross & Singh, 2012; Pirkis, Burgess, Meadows, & Dunt, 2001). Language also influences the effectiveness of treatment (Miller, Martell, Pazdirek, Caruth, & Lopez, 2005) as it shapes understandings and expressions of distress and mental health symptomatology (Hollifield et al., 2002) and influences the establishment of rapport and trust (Miller et al., 2005). Assisting refugees in acquiring the host language would assist with adaptation to migration and with recovery from mental health problems associated with pre-migratory traumatic exposure.
While language class provision may already be part of the resettlement policies for refugees, previous research indicates that only providing language training opportunities is not enough. Refugees experience access barriers due to social, gendered and cultural issues and potentially even lack of pre-migration education and literacy (Watkins, Razee, & Richters, 2012). Limitations in the accessibility, availability and quality of education in service provision also compound these problems (Watkins et al., 2012). This is particularly an issue if refugees are resettled in rural areas, where student retention challenges and restricted or lack of professional development for educators can be experienced by educators with regard to refugee education (Major, Wilkinson, Langat, & Santoro, 2013).
More can be done to address these barriers and enable refugees to access language services and successfully acquire host language skills. This may include creating culturally responsive education by offering different types of learning opportunities such as activity- or visually-based learning for illiterate students (Maher, 2006), training bilingual refugees as educators (McKay, 2008) and providing home-based learning (Watkins et al., 2012). Finally, informing educators about the possible mental health issues that may be present in refugees is also important, given that exposure to pre-migratory traumatic events is strongly related to disturbed cognitive functioning and learning ability in individuals experiencing posttraumatic symptoms. Enabling and supporting refugees’ adaptation to the host-country environment may best be achieved by implementing resettlement policies that provide multidisciplinary provision of services such as access to social services, health, education, language and vocational training.
Limitations
There are several methodological limitations with this study. First, the study included a relatively small sample of refugees who were recruited via community associations, events and online forums. While this strategy enables data collection from a broader section of participants, the sample of refugees in this study may be more open to reporting their distress than the refugees who did not take part in the study. In addition, the small sample size limits the power of the analyses and comparisons between the two countries in particular. Hence, all conclusions from this study should be interpreted with caution. Secondly, we recruited participants from two countries, and while the refugees targeted may share similar cultural backgrounds, they may also differ in their pre- and post-migration experiences, as indicated by group differences identified in this study. Such differences may reflect recruitment bias, hence limiting the generalizability of these findings to the broader Bosnian refugee population and to other refugee groups in other countries. Thirdly, the current study relied on self-report measures and retrospective reporting, which may present a risk of recall bias and inaccurate measurement of symptoms. Fourthly, prior psychiatric history and presence of mental health symptoms associated with other mental health disorders (i.e., not just PTSD, anxiety and depression) were not assessed in this study. Finally, the psychometric properties of some of the measures used in this study have not been validated in Bosnian refugee populations.
Future directions
Future research should employ a larger sample to replicate these results. Furthermore, longitudinal multi-ethnic and multi-national research is needed to test whether the proposed model fits with other refugee groups and other cultures. Such research should start when refugees arrive in the host country and investigate if the provision of language classes assists in the wellbeing of refugees. Moreover, such studies should be conducted across different refugee groups and resettlement countries, as prior research has indicated that resettlement context impacts on how refugees acculturate into the host society (Berry, 1997). Attention should be given to subgroup differences, such as exposure to trauma, age, gender and length of resettlement, but also differences inherent in the origin culture. Despite the limitations, this study is the first to report on the effects of host language acquisition on the relationship between traumatic exposure and symptoms of PTSD, depression and anxiety among refugees.
Conclusion
Building on our understanding of the risk factors and challenges facing refugees, these findings indicate that more could be done to address the long-term effects of traumatic exposure in refugees and the associated mental health problems. Assisting refugees in the acquisition of the host language could benefit their adaptation to the new environment and lead to improvements in mental health. The findings of the current study draw attention to the proximal environmental settings crucial to recovery (Miller & Rasmussen, 2010). While trauma-related migratory factors are increasingly the target of recovery programs offered to asylum seekers and refugees, health programs implemented in resettlement societies also need to incorporate educational and language acquisition programs aimed at lessening the impact of post-migration stressors.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.