
Abstract
The current study examined the ways in which 14 art therapists and adult clients from the Ultra-Orthodox sector in Israel perceive mental health and mental health treatment. Semi-structured interviews were subjected to an interpretative phenomenological analysis to capture the meaning ascribed to the treatment and its challenges. Four themes emerged: the perception of mental health as related to the centrality of functioning, purposefulness, and emotional balance; the specific challenges of therapy, in terms of suspicion regarding treatment and difficulties in establishing intimacy and self-disclosure; the interplay between the worlds of therapy and religion; and the intersection of art and religion. The discussion centers on an interpretation of the findings in light of the ontological typology of individualism versus collectivism.
Introduction
The role of culture in psychotherapy has been attracting increased attention in the past few decades. Specifically, the language of medicine, which makes clear distinctions between pathology and its etiology, symptoms, and cure, is localized and makes sense within a particular context (Littlewood, 2000). Acknowledgment of cultural background has thus contributed to shaping the meaning of mental health and pathology, as well as the goals and practices of therapy, given the growing diversity of individuals seeking help in times of distress (Asnaani & Hofmann, 2012; Sue & Sue, 2003).
Although specialists resort less and less to dichotomous constructs (Littlewood, 2000), one of the main typologies used to account for similarities and differences in mental treatment across societies is the distinction between individualism versus collectivism (Fischer et al., 2009). In Western individualistic societies, which emphasize autonomy, self-actualization, and a feeling of mastery and competence (Green, Deschamps, & Paez, 2005), mental health is perceived as intimately related to the pursuit of one’s personal goals, such that the person experiences a high degree of authenticity, positive affect, and happiness (Diener, Oishi, & Lucas, 2003; Kitayama, Markus, & Kurosawa, 2000). In these societies, emotional distress is explained in terms of biological and relational factors, and modern methods of treatment, such as psychotherapy and medical treatment, are considered curative. During treatment, clients strive to understand the nature of their symptoms (Rüsch, Angermeyer, & Corrigan, 2005) by engaging in the self-disclosure of feelings, fantasies, thoughts, and concerns (Kirmayer, 2007), while establishing close relationships with their therapists (Alperin, 2001; Burleson & Mortenson, 2003). Clients are expected to develop the abilities for free association and playfulness as part of therapy (Kirmayer, 2007; Whelton, 2004).
By contrast, collectivistic societies, such as the Arab (Dwairy, 2006), Turkish (Mocan-Aydin, 2000), Japanese (Kozuki & Kennedy, 2004), and Hispanic/Latino (Weisman, 2005) societies, evaluate mental health and wellbeing according to the degree of belonging and obedience to the group (Sato, 2001). Intimacy is established mainly in the context of the family and there are few close peer relationships (Triandis, 2005). Thus, the demand to develop a close relationship with the therapist over personal issues tends to elicit confusion and embarrassment (Dwairy, 2006; Weisman, 2005). Mental distress in these societies is explained by appealing to religious constructs and prompts individuals to seek help from religious leaders or traditional treatment methods (Triandis, 2005).
In collectivist societies, less emphasis is placed on the disclosure of personal feelings (Matsumoto et al., 2008). In some cases, revealing family secrets is perceived as destroying the community fabric, and hence, as an expression of selfishness (Dwairy, 2006; Sue & Sue, 2003). The therapeutic relationship tends to be a more hierarchical, direct, and concrete one, in which the client assumes a submissive role that aims to please (Mocan-Aydin, 2000; Sato, 2001). Therefore, individualistic healing practices, such as emotional expression, free association, and interpretation of transference, are experienced as strange (Weisman, 2005). Clients’ responses to the therapist’s questions are general and focus on symptoms rather than on emotions, and tend to stress the positive aspects of their lives (Matsumoto et al., 2008).
The Israeli Ultra-Orthodox Jewish community and mental health
The Ultra-Orthodox Jewish community in Israel can be considered a collectivist culture within the more Western, individualistic Israeli culture (Weiss, Shor, & Hadas-Lidor, 2013). Consisting of approximately 9% of the total population of Israel (Israel Central Bureau of Statistics, 2012), the Ultra-Orthodox community rejects modern Western values and isolates itself from society at large. It adheres strictly to Jewish law and is influenced by collectivistic values, such as the prioritization of the preferences of the community over those of the individual, obedience, and respect for adult figures (Huppert, Siev, & Kushner, 2007; Lightman & Shor, 2002). The members of this group are characterized by obedience to tradition, observance of the commandments of the Torah, and respect for religious leaders (Greenberg, Kalian, & Witztum, 2010). The community has enormous power over the life of individuals. Daily life revolves around community values and is maintained by traditions, such as distinctive clothing and geographically separated communities (Buchbinder & Shoob, 2013). Furthermore, this group is divided into several sectors, including the Lithuanian, Hasidic, Sephardic, Hutzniki (foreigners who immigrated to Israel), and Tshuva (individuals who were brought up secular and then adopted a religious way of life), according to ways that they worship God and their attitudes toward modernity and the Israeli society.
Studies have shown that the Ultra-Orthodox are less likely to turn to psychotherapy and generally avoid psychiatric treatment (Coleman-Brueckheimer & Dein, 2011). Many Ultra-Orthodox Jews believe that rabbinical wisdom deals with human psychology and that this knowledge is far superior to that of modern psychology (Huppert et al., 2007). They perceive psychotherapy less positively than the general population of Israel and are more likely to turn to their religious leaders for assistance or spiritual help in case of distress.
Mental illness and referral for treatment are accompanied by tremendous shame and stigma, since it is usually associated with failure to fulfill culturally defined social roles, such as marriage, employment, Torah study, or raising children. This stigma may have a severe negative impact on the marriageability of the clients and even other family members (Greenberg & Witztum, 2001, 2013; Popovsky, 2010). Treatment is viewed with great suspicion, given fears of the potential penetration of secular ideas and the violation of religious principles (Freund & Band-Winterstein, 2013; Pirutinsky, Rosen, Safran, & Rosmarin, 2010). Rabbinic leaders often discourage seeking psychiatric treatment from secular professionals and many Ultra-Orthodox view mental health workers as representatives of the secular world who try to “de-convert” them or blame the clients’ religiosity for causing the illness (Greenberg & Witztum, 2001). Furthermore, in some cases, mostly among the Hasidic population, religious and kabbalistic explanations, such as messianic visions, are used to explain symptomatology (Coleman-Brueckheimer & Dein, 2011; Rosen, Greenberg, Schmeidler, & Shefler, 2008).
Nevertheless, since Ultra-Orthodox society cannot separate itself entirely from the general population, modern trends inevitably permeate it. This can be observed in the adoption of the goals and practices of psychotherapy in some Ultra-Orthodox communities (Rosen et al., 2008). Another tangible sign of this change can be seen in the hundreds of Ultra-Orthodox women who have completed their training as art therapists in the last 10 years.
Art therapy
Art therapy is defined as a mental health profession that enriches the lives of individuals, families, and communities through active art-making, the creative process, applied psychological theory, and human experience within a psychotherapeutic relationship (The American Art-Therapy Association, 2018). Art therapy theories posit that therapeutic changes occur within the context of an aesthetically attuned relationship, in which individuals can express themselves by engaging in art-making. This overlapping triangular relationship between the client, the therapist, and the artwork enables access to suppressed unconsciousness content and embodied knowledge. Further, it enhances levels of awareness by eliciting introjected object relationships, defense mechanisms, and inner conflicts and relational deprivation through symbolic communication and the reenactment of clients’ relational history within the therapeutic relationship. Moreover, through the manipulation of art materials, body movement, and sensory stimulation, art therapy provides joy, kinesthetic release, relief from stress, and facilitates the sublimation of aggression and affect regulation (Czamanski-Cohen & Weihs, 2016; Gerber, Bryl, Potvin, & Blank, 2018). This kind of therapy can be conducted with or without verbal communication, as a function of the therapist’s clinical approach and the clients’ needs. While, in some cases, the therapeutic process is focused on the creative process per se and its inherent healing value, in others, the creative process and its results serve as a vehicle to enable verbal therapeutic processes. In both cases, the therapy acts as an alternative mode of treatment to classical psychotherapy by offering an indirect mode of expression. This may help explain why it is gaining momentum in the Ultra-Orthodox sector, whose clients are regarded as less “psychological,” resist dynamic interpretations, and prefer to express their distress through other modes of expression (Littlewood, 2000). Similarly, the choice of treating art as an indirect treatment approach enables therapists to walk along the seamline between secular/Western treatment and the Ultra-Orthodox worlds. To better understand this new trend, the current study applied the individualism versus collectivism framework to examine the ways in which Ultra-Orthodox therapists and adult clients perceive art therapy.
Method
Participants
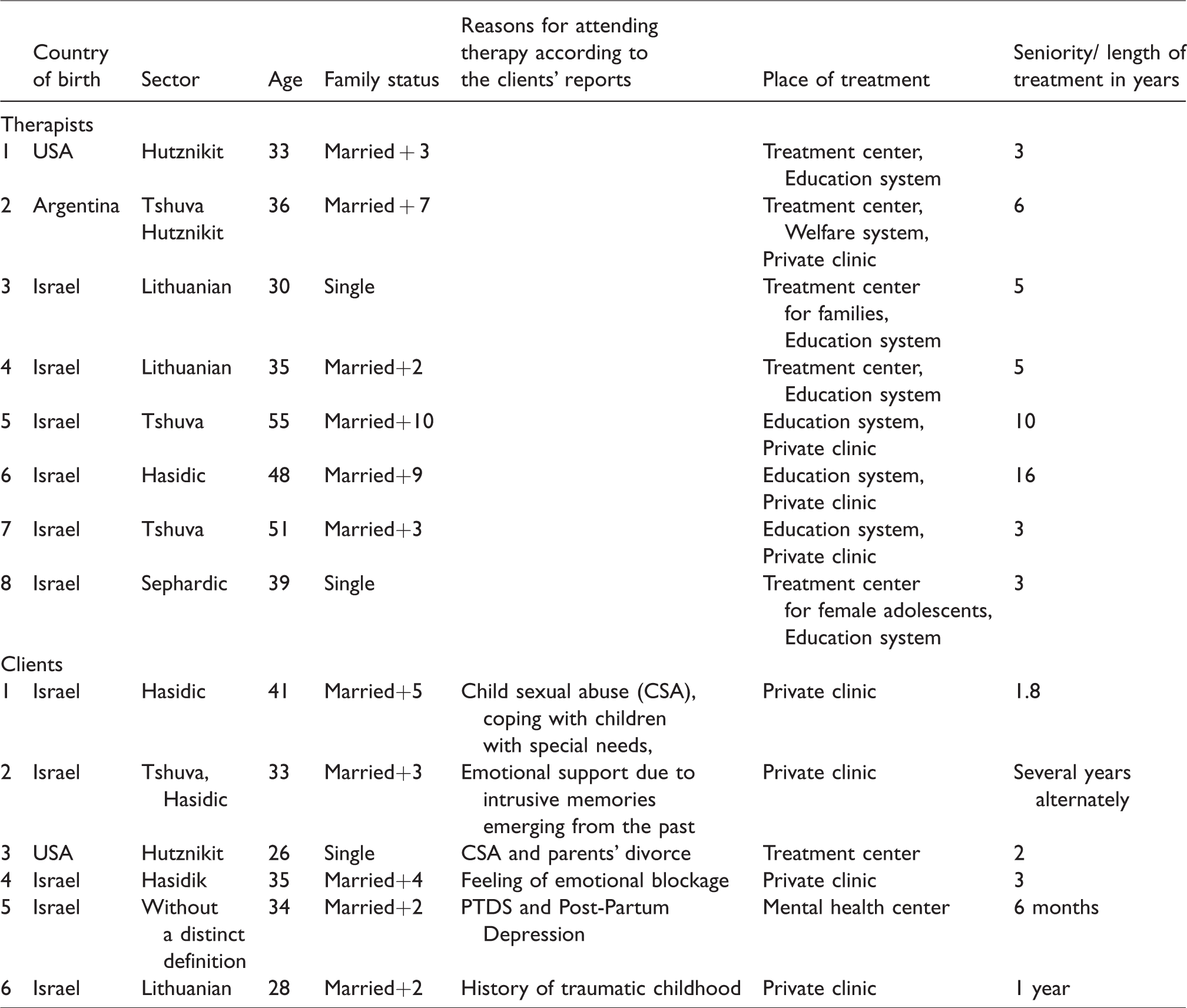
Eight female Ultra-Orthodox art therapists and six female Ultra-Orthodox clients who were recruited from different Ultra-Orthodox sectors participated in this study. Announcements were placed on bulletin boards at the Ultra-orthodox branch of the University of Haifa as well as in mental health clinics in the Ultra-Orthodox sector. The participants were recruited using snowball sampling. In addition, appeals were addressed to mental health treatment centers to publicize the study. All participants were required to meet two inclusion criteria: high verbal abilities, enabling the researchers to acquire a broad perspective on the participants’ and therapists’ experiences, and involvement for at least six months in art therapy on the part of the clients, and three years of clinical experience on the part of the therapists. The therapists ranged in age from 30–55 (M = 41) with an average of 6.5 years of seniority (3 to 16 years). Clients ranged in age from 26 to 41 (M = 33). The clients were in therapy for diverse reasons, such as coping with childhood sexual abuse, intrusive memories emerging from child neglect, anxiety, coping with children with special needs, parents’ divorce, and feelings of emotional blockage. One client was psychiatrically diagnosed with PTSD and post-partum depression. One client reported being prescribed psychiatric medical treatment. One client reported discussing SSRI treatment with her therapist.
All the therapists had an art therapy diploma from an Israeli institution of higher learning (M.A. degree and or equivalent diploma). Their training programs comprised secular classic psychotherapy and art psychotherapy classes, including theoretical and workshop courses. The therapists’ and clients’ demographic and psychiatric information appears in Table 1. Approval was obtained from the University of Haifa Ethics Committee for Research on Human Subjects (No.276/17).
Participants demographics.
The semi-structured in-depth interview
Upon receiving informed written consent, semi-structured in-depth interviews were conducted by the first author during home visits. In an attempt to understand the therapeutic experience, participants were asked to state how therapy influenced their lives and to describe its main challenges and benefits. Sample questions are: What is mental health for you? What, in your opinion, are the goals of the art therapy? Tell us about the process of your decision to go into treatment? What are the main dilemmas that you deal with as a therapist/client in Ultra-Orthodox society? What are the implications of being involved in art therapy as client/therapist in Ultra-Orthodox society? What is art for you? In your experience, what is the role of art during treatment?
Sampling in qualitative research is concerned with the richness of information and therefore the number of participants depends on the topic and the availability of the resources (O’Reilly & Parker, 2013). In the current study, due to the secrecy surrounding treatment, the recruitment of participants was relatively difficult. Thus, we used both the clients’ and therapists’ perspectives as multiple sources of information. We believe that this dual perspective can shed light on areas of similarity and differences between therapists’ and clients’ perspectives, providing rich data while facilitating saturation and triangulation (Golafshani, 2003; Fusch & Ness, 2015).
All interviews were recorded and fully transcribed and analyzed based on the principles of Interpretative Phenomenological Analysis as defined in the guidelines by Smith, Flowers, and Larkin (2009). Each interview was treated separately by the two authors to achieve investigators’ validity (Golafshani, 2003), and the analysis began with an intensive, detailed reading and re-reading of the interview transcripts and notes, in an attempt to identify descriptive comments in relation to the data (such as processes, relationships, and events) and to gain an understanding of their meaning for the participants and their conceptualizations. This inductive analytic process led to a preliminary list of initial themes, which included wellbeing as strength and adjustment, suspicion toward treatment, and parallels between religious and treatment values. Next, a second list was produced by identifying patterns, connections, and interrelations between the conceptual comments. These themes included art as a bridge for the treatment of Ultra-Orthodox society and unique challenges. Finally, after examining the situations, contexts, actions, strategies, and outcomes in depth, a list of subordinate themes was generated to complete the analysis. The clients’ and the therapists’ interviews were analyzed separately. The themes were only integrated in the last phase of the analysis.
Results and discussion
Four main themes emerged from the analysis of both the therapists and the clients. The first theme related to the perception of mental health. The second theme dealt with the specific challenges arising in therapy. The third theme described the nature of the encounter between therapy and religion, and the fourth captured the encounter between art and religion.
“Make it more practical”: Ultra-Orthodox society’s perception of mental health
During the interviews, the participants were asked to describe how they perceived the concept of mental health and their views on the goals of treatment in general and art therapy in particular. As defined in the literature (The American Art-Therapy Association, 2018), the art therapist’s role is to guide clients to a state in which they are able to play, create, and explore the art materials as a way of growing and developing. Surprisingly, in the current study, although art therapy deals with creativity and expressiveness, in both the clients’ and therapists’ responses, the ideal of purposefulness, functioning, and the ability to deal efficiently with life events dominated. The clients considered that their engagement in treatment derived from their desire to improve their functioning, coping abilities, and strategies after experiencing stressful life events as mothers and wives. The clients repeatedly used phrases such as “getting the tools to cope” (Client 1), “to function better” (Client 2), “be a better mother, a better wife” (Client 5) to describe their therapeutic goals. Many of the clients described therapy as a “checklist.” The therapeutic session was sometimes compared to a “lesson,” in which they accomplished one step after another to achieve as many goals as possible: “What made me stay is that we check off a great deal of things. In almost every lesson, not lesson, therapy, we check off something” (Client 1); “What does a therapist do? Helps you make decisions in life” (Client 6); “Adults are supposed to have tools. They are supposed to manage by themselves” (Client 4). These statements suggest that optimal functioning and successfully fulfilling what their society expects of them were perceived as achieving self-realization.
A similar description emerged from the therapists’ reports. They perceived therapy as a vehicle to correct failures or malfunctions, as an objective, and as a means of coping. As the therapists stated: “Mental health means to be equipped with strengths, to deal with crises and challenges” (Therapist 1); “It is a person who is connected to his or her reality, a person who functions on a daily basis. Who succeeds in fulfilling his/her duties and roles (Therapist 2); “I think it is a balance, to able to contain the abundance of emotions we experience in our day-to-day struggles. Not to collapse, not to break down, to act with discretion” (Therapist 8).
This purposefulness can best be understood in light of Ultra-Orthodox society’s views of the role of the Ultra-Orthodox woman. As an “auxiliary” (Genesis 2:18), women are supposed to support their husbands emotionally and financially, since men are exclusively expected to excel in the study of the Torah and adherence to its laws (Globman & Lifshitz, 2004). For strictly Orthodox men, particularly in Hasidic circles, the most valued career track is religious study, which is characterized by high intellectual demands focusing on Jewish law and commentary. Although women may have a broader education than men, they are expected to contribute to the family’s livelihood, and sometimes be the principal breadwinners, in order to free their husbands for religious study (Loewenthal, 2006a). The stress of purposefulness and efficient coping of Ultra-Orthodox women is also evident in the Jewish gender division between spirituality and pragmatism. Specifically, spirituality is reserved for men, whereas pragmatics and purposefulness are reserved for women. Supported by the verses “You shall observe it day and night” (Joshua 1:8) and “There is no wisdom for women but in the spindle” (Talmud, Yoma 6:2), this division is nurtured early on in the education system, in which boys are expected to devote eight hours a day to Jewish studies (Globman & Lifshitz, 2004), while girls are expected to take active caregiving roles in the home in preparation for future family life (Loewenthal, 2006b). This may suggest why the participants adopted a pragmatic point of view regarding the goal of therapy and perceived it as a vehicle to promote their societal role.
The specific challenges during treatment
Numerous challenges were mentioned in relation to treatment. These included suspicion about treatment and difficulties in establishing intimacy, engaging in self-exposure, and emotional expression.
Suspicion about treatment
All the therapists and clients described the negative perceptions of treatment at length, which are prevalent in Ultra-Orthodox society and are rooted, as was found previously, in the stigma associated with seeking treatment outside the family (Coleman-Brueckheimer & Dein, 2011; Greenberg & Witztum, 2001). In this respect, the participants attributed this negative reaction to a lack of understanding of the role of therapy and its transformative mechanisms and to negative attitudes toward Western psychology. According to the participants, there is a widespread belief in the Ultra-Orthodox sector that mental health difficulties are part of an overall divine plan to improve the individual. Thus, treatment itself contradicts the divine plan and can cause mental imbalance, fragmentation of the self, and can undermine family cohesion (Loewenthal, 1995). The therapists suggested that this “comes from a lack of knowledge, a lack of experience, and misunderstanding” (Therapist 1); “They come with a lot of stigma and devaluation, prejudice and resistance” (Therapist 2). The clients pointed out that a referral to therapy equates seeking help with insanity, as manifested by terms as “crazy,” “defective,” “broken,” and “needs to be fixed” (Client 3). Requesting treatment is accompanied by deep feelings of shame, self-condemnation, and self-blame. These feelings create a sense of self-stigmatization and negatively affect the course of treatment by questioning its effectiveness (Henderson, Evans-Lacko, & Thornicroft, 2013).
Obviously, perceiving oneself as weak, dependent, unable to cope, and emotionally imbalanced are signs of poor mental health. Hence, going for treatment or disclosing one’s treatment in public is viewed as an actual risk to these clients’ mental health. This is also because treatment jeopardizes their families’ reputation. The fear of not finding a decent match for themselves, their siblings, or children was palpable in the clients’ statements. This situation forces clients to either withdraw from treatment, conceal their treatment from their immediate environment, or learn to cope with derision from their social circles. As a result, referral for treatment is seen as a last resort and only in extreme circumstances. For example, some clients indicated that: “I would not dare tell anyone that I am in therapy. If I said so, I would be perceived as crazy, problematic” (Client 3); “There are severe consequences for going for treatment, the damage to the children’s reputation, what will happen to them when they grow up? This is dangerous. This is existential” (Client 2); “Everyone is constantly hiding their problems so that they can get a decent match in the future” (Therapist 7).
Individualized psychological influences which are incompatible with the worldview of the Ultra-Orthodox community increase these suspicions (Greenberg & Witztum, 2001; Loewenthal, 2006b). While the Western psychoanalytical stream of psychology emphasizes the centrality of the individual and free will, the Ultra-Orthodox viewpoint underscores the importance of the community and adherence to the commandments of the Torah (Struch et al., 2007). The fear of secular worldviews was heightened by the fact that the therapists had studied in secular institutions of higher learning, which is forbidden in some Ultra-Orthodox sectors (Loewenthal, 2006a, 2006b). This suspicion leads to scrutiny of the therapist’s religiosity, way of life, and loyalty to Judaism. As Therapist 2 pointed out: “In the eyes of my community, the fact that I have an MA degree makes me less Ultra-Orthodox. I constantly feel the clients’ fear that I will ‘taint’ them and encourage them to negate Judaism.”
In order to cope with these potentially negative consequences, the community adopts monitoring mechanisms, involving infiltration and interference with the course of treatment. Client 5 reported: “My mother was terrified. She was concerned that I would go mad […] that I would tell my children strange things. People warned me that my husband would suffer and divorce me.” Client 2 said: I was sure that people [in my community] would understand that if a person is in a complex condition, he/she may need mental help […] I was surprised. Even my husband was afraid that our family would be ostracized. They [the community] wanted people to come to my home to see that the treatment was not making me crazy.
“I felt naked”—Difficulties in creating intimacy and self-exposure
During the interviews, the participants were asked how they experienced intimacy, as well as the revealing, disclosure, and expression of feelings over the course of treatment. This question elicited more attention than any other question in the interview. While most therapists were positive about the value of intimacy in treatment and saw it as an essential and integral part of the therapeutic relationship, at the same time, most also described it as a potential obstacle that derives from cultural attitudes. According to the therapists, the very use of the word “intimacy,” which seems to be connected with a lack of modesty during treatment, can create anxiety that alienates the clients from their therapists. They stated: “I used the word ‘intimacy’ in our first session, and she ran away. Closeness with a strange woman is frightening” (Therapist 1); “It was challenging for them to be intimate with me. They did everything they could to destroy me” (Therapist 7).
To reduce this anxiety, therapists engage in a self-disclosure technique and use the therapeutic setting itself, which promotes confidence and trust: “It takes time, but it happens when you listen to them and reflect and compliment and appreciate and disclose yourself” (Therapist 4); “A meeting between two people in a room, on a regular basis, one hour on a set day, so in the end, intimate relationships are formed” (Therapist 8).
Similarly, the clients also described their discomfort with the therapeutic relationship and their attempts to avoid intimacy. These attempts, which are consistent with the tendency toward purposefulness in Ultra-Orthodox society (Globman & Lifshitz, 2004), were expressed in contra-phobic reactions such as using idle and trivial speech, garrulity, or production of repetitive and stereotypical art, which were designed to blur closeness and calm anxiety. In their testimonies, closeness was perceived as childish and was accompanied by a sense of self-condemnation over the need for relatedness. As the clients stated: “At first it was awkward for me to sit with a strange person, I spoke to her constantly, to distract her from concentrating on me, just not to create intimacy” (Client 4); “The intimacy is sometimes disturbing […] I felt like a baby, and it drove me crazy” (Client 2); “I was petrified to feel intimate, I felt vulnerable, it took me a great deal of time to feel safe” (Client 3).
This difficulty in establishing intimate relationships also emerged in the clients’ statements about their inability to share their past experiences, their flaws, their parents’ flaws, and their negative emotions toward the therapists. It was described as an intimidating experience and was compared to “physical nudity” and “washing one’s dirty laundry in public.” It evoked feelings of shame and terror and demanded enormous resources on the part of the clients to persevere in treatment: “I was used to keeping everything to myself. I wanted to control my disclosures. I felt so exposed” (Client 5); “It was too much, I felt naked” (Client 2); “To be exposed is like walking down the street with no clothes on” (Client 4). They raised questions about their therapists’ guarantees of confidentiality and expressed deep concerns regarding self-fragmentation and self-labeling as mentally ill. The clients described being flooded with feelings and experiencing a fear of going mad while revealing their painful memories: “I was emotionally overwhelmed. I was afraid I would go mad, lose control” (Client 1); “Treatment is stormy, shocking. There is a whole world inside.” (Client 6).
Similarly, emotional expression was also perceived as challenging. The therapists described a split between their clients’ inner and outer worlds, where positive emotions are expressed in the outer world, and negative emotions are vigorously suppressed. This split elicits feelings of self-alienation, self-condemnation, and self-hatred. Certain clients stated: “My inner self is completely different from my outer self. In my outside world, I am extremely happy while my inner self is flooded with sadness” (Client 1); “Some feelings are profoundly suppressed and are more difficult to access. I feel that I cannot reach anything. It upsets me enormously” (Client 2); “We are full of secrecy. We do not just talk or go out.” (Client 4).
The need to maintain secrecy forced clients to invest enormous efforts in maintaining an ideal image of perfectionism, joy, and strength, which involved repressing their internal negative feelings from those seen positively from the outside. Throughout the interviews, they described their ongoing attempts to appear healthy and in control, while disguising or rationalizing their imperfections and flaws. The comments included “It is shameful if you expose your bad sides” (Client 4); “I was afraid; I did not want to be perceived as trash. I constantly needed to explain the origins of my problems, the things that screw me up” (Client 6).
Thus, similar to the situation experienced in other traditional collectivist societies, the therapeutic techniques of exposure, emotional expression, and the establishment of intimacy appeared to have elicited unbearable feelings of embarrassment, vulnerability, and shame (Dwairy, 2006; Triandis, 2005). The intricacy involved in expressing emotions can also be attributed to the values instilled through Ultra-Orthodox education. Based on sayings from Jewish sources such as “Who is a hero who conquers his inclination” (Proverbs 16:32) and “All who are angry as though they are idolatrous” (Shabbat 45:30), individuals are encouraged to refrain from expressions of negative feelings, such as jealousy and anger. This may increase the difficulties encountered by Ultra-Orthodox clients in recognizing and revealing their feelings (Greenberg & Witztum, 2001).
The encounter between religion and treatment
There is extensive literature on the associations between religion and mental treatment in traditional societies in general (Andersen, Oades, & Caputi, 2003; Weaver, Pargament, Flannelly, & Oppenheimer, 2006) and in Ultra-Orthodox society in particular (Hess & Pitariu, 2011; Pirutinsky, Rosmarin, Pargament, & Midlarsky, 2011). Although studies have suggested that spirituality can be a source of support in times of crisis by enhancing physical and psychological functioning (Andersen et al., 2003; Pargament & Saunders, 2007), other work has suggested that negative religious coping, manifested by activating anger towards God, decreased engagement in religious activities, as well as increased guilt and doubts can be an obstacle to mental health and lead to a decline in mental health (Exline & Rose, 2005; Pargament, Koenig, Tarakeshwar, & Hahn, 2004) (Ano & Vasconcelles, 2005). For instance, a recent longitudinal study among the Ultra-Orthodox population reported an association between negative religious and spiritual coping and increased symptoms of depression (Pirutinsky et al., 2011). Here, the participants discussed the reciprocal relations between the worlds of religion and therapy and raised concerns about the extent to which the treatment and its values were consistent with their religious values.
Similarities between religion and treatment
Most of the therapists searched for parallels between the worlds of religion and therapy. They emphasized that Jewish literature inherently contains the world of therapy and that religious concepts are interwoven in the therapeutic process. Some of the therapists actively integrated religious content into the treatment by referring to the written sources of Judaism. They considered the combination of the two worlds as a significant part of their professional identity: Everything is connected. The Torah enriches therapy, and the therapy wonderfully enriches the Torah. (Therapist 5) It’s important for me to be alert, I ask myself what kind of therapeutic content I should use, thus, I am constantly looking for a connection to my religious outlook. It’s important for me not to get lost in unrelated works but rather to rely on content from my own culture. Therefore, when I look for a theory I try to look for it in my culture. (Therapist 4)
Similarly, the clients also felt that the therapeutic process was taking place under the canopy of religious values. On the one hand, treatment was perceived as promoting spiritual development and religion was described as a means towards fulfillment of treatment. In terms of religious development, the clients stated that, as part of their treatment, they engaged in reviewing their relationship with God and its spiritual and pragmatic significance in their lives. Others emphasized that their relationship with God was directly influenced by the therapeutic work. Specifically, they expressed that the therapy enhanced their wellbeing and enabled a stronger connection to God, which was manifested in praying and fulfilling the commandments with greater enthusiasm, zeal, and dedication. Others stressed that the enhancement of their self-image reflected the love of God towards them, and that they felt more connected to the worship of God: “Because I am happier, I fulfill the commandments with more joy” (Client 6); “Why did we come into the world? We are on the path to the next world. We have to complete our mission. The treatment helped me to maximize my mission. I pray with more devotion and connection.” (Client 3). Other clients stated that religion protects them from obstacles in the therapeutic relationship. As Client 2 said: “Religion protects me. It provides stability and protects me from emotional turmoil.”
Several participants also felt that religion acts as a therapeutic tool and that the use of religious language should be an essential part of the therapy in that it facilitates the therapeutic goals. They discussed the significant role of faith in therapy. For instance, Therapist 6 said: “As an Ultra-Orthodox therapist, I do not understand how I can treat others without faith.” Similarly, Client 1 recalled: “My therapist connected me to my values, how could I survive without my faith? She strengthens me with faith.” This is consistent with the review by Coleman-Brueckheimer and Dein (2011) on health care behaviors and beliefs in Hasidic Jewish populations, which pointed to the incorporation of religion in individuals’ explanations of illness.
By contrast, other therapists resisted the use of religious terminology as a therapeutic device and perceived it as dangerous. Therapist 3 said: “The use of religion can burden the clients, make them feel guilty and confused, so I do not use it.”
“Freud is banned”: Treatment as a source of doubt about religion and the danger of secular influence
Most of the therapists and the clients felt their involvement in therapy presented a danger to their religious world. About half of the clients felt that the treatment negatively affected their religious development. They expressed anger toward God, a slackening of their observance of the commandments, and a questioning of their faith. They attributed this to the anger elicited as a result of dealing with difficult past experiences. Clients said: “I have had a lot of religious questions, […] especially in a time of anger, to whom you direct the anger? If you are a religious person, you will say it is from God, and why did it happen to me? I did not always get answers” (Client 3); “I was not sure of my religious views. It shook me. I had to look after myself. I had conversations about faith with my husband and consulted books not to get carried away. However, it was very confusing” (Client 4); “I began to be less observant […] I feel that the treatment released me from a certain burden, but I do not feel comfortable with it.” (Client 5).
One of the prime difficulties in therapeutic work comes from the underlying assumption in therapeutic theory that primary caregivers influence the development of one’s mental health and pathology. However, this underlying postulate contradicts the prohibition against defamatory, harmful speech about the dead and the commandment to honor one’s mother and father, which implies refraining from condemning one’s parents (Popovsky, 2010). The participants highlighted their dilemma regarding the morality of sharing and exposing their views. In particular, exposure in therapy is perceived as a violation of these religious commandments and as a step toward detachment from faith and religion. Some of the comments included: “I learned to give anger a place, that it is okay to be angry at my mother. It is allowed by religion to talk about it, it is permissible to speak of things God decreed” (Client 6); “Clients are constantly dealing with defamation, is it permissible to be angry, not to be angry.” (Therapist 4).
In their discussions on the difference between religion and therapy, the therapists also talked about the threats to their religious faith stemming from their profession and indicated that a pivotal moment in their professional training was when they first encountered dangers to their own beliefs. In particular, they described the encounter with classic theories of psychotherapy, which emphasize the importance of impulse and instincts (such as Freudian theory) and talked about how controversial and even shocking they found them, presumably because they clashed with the religious values of suppressing impulses and sexuality and encouraging modesty, as well as Freud’s view of religion as a universal obsessional neurosis and as a mechanism to enable individuals’ releases from neurosis (Zohar, Goldman, Calamary, & Mashiah, 2005). The comments included: I had questions about what to read. I started to read When Nietzsche Wept [a novel by psychoanalyst Irvin Yalom about a woman with hysteria treated by Breuer]. I stopped reading in the middle, the descriptions were horrifying, full of sexual thoughts […] I was disgusted. (Therapist 4)
The encounter between art and religion
The encounter between art and religion was also loaded and complex. Historically, art has been an integral part of Jewish religious work (Raphael, 2009). Traditionally, art is found in synagogues, which are filled with paintings, engravings, mosaics, and decorative elements (Levine, 2002). Today, art and art making are often perceived as modern alternative practices that are antithetical to religion (Franke, 2007). Thus, the Ultra-Orthodox population generally detaches itself from art making unless it is for religious purposes, while maintaining special restrictions (such as prohibiting sculpturing a human figure or drawing immodest images). Halakhic texts on art instruct their readers as to what is forbidden and permitted in art making, such as painting rabbis in a way that reflects wisdom and kindness, and refraining from painting images that would turn the figure into a statue.
This ambivalence toward art making was also manifested in the participants’ narratives. On the one hand, many participants described God as an artist and the wonders of the universe as works of art. As Therapist 3 said: “God Himself is a painter. There is no painter like God.” In addition, participants referred to art as a bridge to the clients’ inner world, since it enables the expression of hidden content in a gentle, moderated way. Clients reported that they specifically chose art therapy, stating: “Direct verbal conversations were very difficult for me. Expressing myself in art was more comfortable and easier” (Client 4); “We talk about the artwork, it acts as a third party that blurs the exposure” (Therapist 6); “Art is a multi-sensory tool that speeds up and encourages the process of therapy. It can help create the soul from scratch, expressing something from yourself” (Therapist 1).
Throughout therapy, the clients decided in a flexible manner whether to use art or verbal communication. They felt that their therapists were attuned to their needs and abilities and felt free to switch from one mode of expression to the other. For instance, Client 6 stated: What led me to go to art therapy is the desire to really restructure myself, there are a lot of things that I drag out of my home and I want to recover from them and I felt that verbal treatment is not really suitable for me. Art opens things up that I have not dared to share until now. I just want to get myself to a place where I am feeling better about myself, more complete, more aware of the things that operate inside me.
Nevertheless, although the participants underscored the advantages of art as an indirect alternative channel for self-disclosure, they also expressed ambivalence toward art. Attitudes toward playfulness are influenced by cultural, environmental, and social differences. Hence, cultural values shape ludic activities, such as time devoted to gameplay and game content (Holmes, 2012). In this respect, many clients and therapists noted the negative perception of Ultra-Orthodox society toward playfulness, probably because of the enforced need for purposefulness mentioned above, and a condemnation of the waste of time and materials embodied in playfulness in the treatment room. Many clients described the anxiety and guilt that they experienced during the various stages of treatment, when they found themselves playing with materials without a clear or known purpose, rather than fulfilling their religious or familial duties. Playing and creating were considered a waste of time and as sabotaging the opportunity to engage in acts of charity and kindness as is expected of them in their spare time (Loewenthal, 2006b). Thus, it is clear why extensive parts of the therapeutic process were devoted to regulating the anxiety related to loss of control and cultural condemnation of playfulness.
For instance, as part of the ideal of purposefulness, some of the clients disparaged art using terms such as “childish” (Client 1), “nonsense” (Client 4), “not serious” (Client 3). This was accompanied by feelings of guilt and discomfort: I came very closed and restrained to the treatment. When the therapist asked me to draw the relationship with my mother, I drew very quickly and carelessly. It was really hard for me. I was not used to paint freely, it seemed very strange to me […] Gradually I learned to focus on the process rather than on the result. I learned to play, to break loose, to go wild on the page, to do nonsense. (Client 4) I left with guilt feelings about what I was doing in the morning, playing, instead of taking care of things I needed to do. (Client 5) The day is short and the work is long. You hear about young people who die, and you say how can I sit and draw? Let’s do an act of kindness. (Client 6)
In attempt to cope with the clients’ ambivalence, the therapists turned to decorative art as a way to strengthen the clients’ worship of God, which better aligns with the traditional role of art as being designed to glorify God and Judaism. Therapist 6 stated: “When people are reluctant to engage in art, I immediately suggest that they make an ornament for the holidays.” However, at the same time, the therapists noted that the engagement with the aesthetic and spiritual aspects of art making left no room for formless, essentially instinctive, spontaneous creation. Thus, the use of art therapy was both perceived as a relatively alternative safe therapy that does not necessarily demand free-ranging discussion and masks unbearable feelings of nakedness, but also as subject to the restrictions on art in Ultra-Orthodox people’s life, the deliberate avoidance of uncensored output, and the perceived danger of exposure to secular images that evokes apprehension with art making in general and art therapy in particular.
Conclusion: Practical implications and limitations
Similar to Greenberg and Witztum (2001), who took a sympathetic position toward their clients and appreciated the fundamental experience of Ultra-Orthodox clients, the current study concentrated on the influence of the social taboos and conventions stemming from the system of values and cultural beliefs of the therapists and the clients. In particular, it showed that conducting art therapy within Ultra-Orthodox culture demands an in-depth understanding of the subtleties of Ultra-Orthodox society, which shapes the perception of mental health and the function of art, as well as a grasp of the challenges and dynamics within therapy for this sector. These include the significance of perfection and purposefulness as an indicator of mental health, the need to handle issues of self and social stigma, the fear of undermining the client’s faith through sense of inadequacy, jeopardizing the family reputation and embarrassment when establishing an intimate therapeutic relationship and creating art, and the reluctance to accept classic impulse-oriented psychological theories.
Thus, when providing treatment to the Ultra-Orthodox sector, the goals and practices of art therapy should adhere to the expectations of this culture, while preserving the nature of the therapeutic processes and its main principles, such as providing dynamic interpretations of inner and object relation conflicts, transference, and countertransference in order not to mask the therapeutic work. In this respect, treatment should create a balance between encouraging emotional expression and practical responses that aim to increase clients’ reflection and enhance clients’ wellbeing. In addition, the theoretical foundation of treatment may combine the implementation of classical psychological theories with developmental approaches, such as attachment theory, and more behavioral conceptualizations that will not be perceived as endangering the clients’ and the therapists’ faith. References to the Bible and the clients’ faith can be harnessed to facilitate clients’ self-disclosure and mentalization. Finally, art should be used intelligently and sensitively and therapists should consider the traditional use of art in worship and the delicate interplay between verbal expression and interpretation and the use of the process of art making as a form of healing itself.
Nevertheless, the current study has certain limitations, which relate mainly to the sample. Since being in therapy in Ultra-Orthodox society is shrouded in secrecy, there was tremendous difficulty recruiting individuals to participate in this study. The rare clients who agreed came from a more liberal sector of Ultra-Orthodox society and were being treated in private clinics. Thus, the voices of more conservative communities and mentally ill clients could not be accessed. In addition, the current study did not include therapist–client dyads. Getting the point of view of the dyad could shed light on the ways each sees the treatment. Finally, the findings are based on the viewpoints of 14 women. Future studies should include the voices of men, rabbis, and public figures. In order to obtain a more comprehensive and valid picture, future work should also attempt to investigate more diverse samples in Ultra-Orthodox society.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. We declare that this work was carried out in the absence of any personal, professional, commercial, or financial relationships that could be construed as a potential conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.