
Abstract
Research with Indigenous communities has demonstrated the detrimental impacts of intergenerational trauma and disproportionate adverse childhood experiences (ACEs) on health and behavioral outcomes in adulthood. A more balanced narrative that includes positive childhood experiences is needed. The construct of benevolent childhood experiences (BCEs) facilitates assessment of positive early life experiences and their impact on well-being for Indigenous peoples. We consider associations between BCEs and well-being when taking into account ACEs and adult positive experiences. Participants are from Healing Pathways, a longitudinal, community-based panel study with Indigenous families in the Midwestern United States and Canada. Data for the current analyses are derived from 453 participants interviewed at wave 9 of the study. Participants reported high levels of positive childhood experiences in the form of BCEs, with 86.5% of the wave 9 participants reporting experiencing at least six of seven positive indicators. BCEs were positively associated with young adult well-being. This relationship persisted even when accounting for ACEs and adult positive experiences. While ACEs were negatively correlated with young adult well-being, they were not significantly associated with well-being when considering family satisfaction and receiving emotional support. Evidence of high levels of BCEs reflects realities of strong Indigenous families and an abundance of positive childhood experiences.
The Stress Process Model (Pearlin et al., 1981) is a foundational sociological explanation of the interplay of stressors with coping resources and responses in relation to health outcomes. A critical feature of the model is awareness of the antecedents and fundamental causes of stress (Aneshensel et al., 1991; Link & Phelan, 2005): stressor exposure is non-randomly distributed throughout society, with members of marginalized groups (e.g., those of lower socio-economic status, racial/ethnic minorities, etc.) differentially exposed to greater stress (Turner, 2010). Heightened stress exposure, in turn, increases adverse health outcomes (Pearlin et al., 1981). For American Indian and First Nations communities, fundamental antecedents of contemporary stress exposure include pervasive intergenerational oppression and associated processes of historical and ongoing colonization and marginalization (Fryberg et al., 2018; King et al., 2009; McKinley et al., 2020). This point is a centerpiece of the Indigenist Stress Coping Model (ISCM; Walters & Simoni, 2002), which beckons researchers to consider socio-historical experiences of Indigenous communities as foundational to understanding modern health inequities and disproportionate risk for stress and trauma exposure (Walters & Simoni, 2002; Walters et al., 2002). Given this backdrop, it is unsurprising that heightened stress burden (American Psychological Association, 2017; Baldwin et al., 2011) and lower life expectancy rates are observed for Indigenous peoples than are found for any other racial/ethnic group in the United States (Arias et al., 2022).
At the same time, Indigenous communities host countless strengths conducive to health and wellness (Kading et al., 2015; Kirmayer et al., 2011; Rasmus et al., 2019). The seminal works of Michael Chandler for whom this Special Issue is dedicated illuminate, for example, how Indigenous community efforts to preserve and revitalize traditional cultural ways correspond to community level well-being, including lower suicide rates (Chandler & Lalonde, 1998). Chandler and colleagues also showed how Indigenous language use confers special protective effects against suicide: in communities where more than half of Band members spoke their Native language conversationally, suicide rates were substantially lower than in those where language use was less consistent (Hallett & Chandler, 2007). These and other protective factors, including an emphasis on family and community, can serve as coping resources or buffers to offset the harmful effects of stress (Pearlin & Schooler, 1978; Walters & Simoni, 2002). While Indigenous communities consistently call for strengths-based approaches to health equity research (National Congress of American Indians et al., 2015), science to date continues a perseverance on deficits and pathology that perpetuate negative narratives about Indigenous peoples. To balance these narratives, and as a direct response to community interest in understanding drivers of positive development, we focus this study on stress process factors influencing well-being among Indigenous young adults. As detailed below, we consider two early life factors: Adverse Childhood Experiences (ACEs; a stressor), and Benevolent Childhood Experiences (BCEs; a protective factor); and two adult constructs: social support and family connections (protective factors) in our analyses.
Early life factors: Adverse and benevolent childhood experiences
In terms of stress exposure, traumatic events have been posited to have greater impacts on health than other stressors (Wheaton, 2010). The timing of traumatic events may also matter. For example, adverse childhood experiences (ACEs) have been shown to be stronger predictors of poor health than traumatic events experienced during adulthood (Wolff & Ratner, 1999). Indeed, childhood is a defining time in the life course that sets the foundation for later health and development (Elder & George, 2016). Research with Indigenous communities reveals disproportionate exposure to ACEs that are associated with negative health and behavioral outcomes in adulthood (Brockie et al., 2018; Elm, 2020; Evans-Campbell, 2008; Warne et al., 2017).
Although scientific inquiry into the prevalence and impact of ACEs has permeated the literature and informed public health practice for decades (Felitti et al., 1998; Roh et al., 2015), ACEs are only part of the story (Anda et al., 2020). ACEs-related research, policy, and practice have been critiqued for numerous reasons, including potential stigmatization and internalization of deficits narratives and labels by those who experienced ACEs (Finkelhor, 2018; Kelly-Irving & Delpierre, 2019). In part as a response to these very issues, and as a testament to Indigenous survivance (LaPier & Beck, 2015; Vizenor, 1999) and resilience, Indigenous communities have championed strengths-based research (Henson et al., 2017; Morse et al., 2016; Ullrich, 2019). A strengths-based focus has spurred many researchers to highlight pathways to well-being for Indigenous youth and adults (Friesen et al., 2015; Kading et al., 2019; Rountree & Smith, 2016; Simard & Blight, 2011). To our knowledge, this study is the first to focus on how childhood experiences may be connected to well-being of Indigenous peoples into adulthood generally or while also accounting for the realities of differential stressor exposure.
The impacts of positive childhood experiences are not left behind in childhood but carry forward into adulthood. Positive childhood experiences have been shown to support adult well-being (Sroufe et al., 2006), are associated with a reduction in adult psychosocial problems (e.g., uncontrollable anger; Hillis et al., 2010), and are promotive of physical, mental, cognitive, and social wellness even in the presence of ACEs (Crandall et al., 2019).
Traumatic and positive experiences and memories are not mutually exclusive. Even when stress and trauma are prominent in childhood, supportive parenting, positive peer relationships, and access to, and use of, community resources can produce resilience in childhood (Easterbrooks et al., 2013). Adult memories of feeling loved and cared for during childhood may co-exist with the impacts of childhood maltreatment (Narayan, Ippen, et al., 2017). One way that positive childhood experiences have been assessed is through the construct of benevolent childhood experiences (BCEs). The construct of BCEs incorporates safety, security, and positive and predictable qualities of life from birth to 18 years old (Narayan et al., 2018). In a study with low-income pregnant women, BCEs predicted lower levels of post-traumatic stress symptoms and fewer stressful life events among participants, even when accounting for ACEs (Narayan et al., 2018). In addition, and consistent with stress process models, positive childhood memories with caregivers moderated associations between childhood maltreatment and mental health outcomes in a diverse group of mothers (Narayan et al., 2019). The examination of BCEs thus provides an opportunity to assess positive early life experiences and their impact on well-being for Indigenous peoples.
Adult factors: Social support and family connections
Benevolent and adverse childhood experiences have been shown to impact people into adulthood, but it is unclear how such experiences impact well-being when considering adult experiences. Strong social support networks in adulthood may confer better health. Results from a meta-analytic review showed that pro-social relationships significantly reduced risk of mortality (Holt-Lunstad et al., 2010). When multidimensional assessments of social relationships were used, including family connections and emotional support, this association increased (Holt-Lunstad et al., 2010).
Social support and family connections in adulthood represent two major constructs robustly linked to health and well-being. Extensive evidence indicates that perceived availability of social support, rather than receipt of support or perceived responsiveness, is an important predictor of health (Berkman et al., 2000; Reis, 2007). Perceptions of available emotional support may act as a secure attachment base where an individual knows they have support they can rely on if they were to need it (Bowlby, 1988; Feeney & Collins, 2015). Family networks further support well-being for many Indigenous peoples (Martin & Yurkovich, 2014). Strong family relationships facilitate deeper connection to cultural protective factors (Ore et al., 2016) and such relationships have been shown to be salient to wellness in many studies with Indigenous people (Coser et al., 2018; Kading et al., 2019). Notably, family connections and social supports have also been shown to operate as stress-buffering factors or coping resources across cultures (Cohen & McKay, 1984; Gayman et al., 2018; Schultz et al., 2021).
Well-being
Much research with Indigenous communities has focused on the important work of understanding the relationships between historical trauma, ongoing experiences of oppression and racism, and symptoms of depression, loneliness, and anxiety (Evans-Campbell, 2008; O’Keefe et al., 2015; Yellow Horse Brave Heart et al., 2011). However, mental health is not merely the absence of mental illness; rather mental health and mental illness are separate unipolar dimensions and need to be addressed as such (Keyes, 2005). For example, Walls et al. (2016) found that levels of positive mental health among Indigenous Peoples were equal to or greater than comparison studies with non-Indigenous populations even in the presence of comparatively higher rates of anxiety and depressive symptoms. In parallel to the concepts of flourishing or positive mental health, as measured by Keyes (2005) and Walls et al. (2016), is the construct of well-being (Diener et al., 2018; Ryff, 1989). Well-being entails self-perceived success in areas such as capability, purpose, and optimism (Diener et al., 2010). In this article, we take a holistic view of the impact of childhood experiences on adult mental well-being among Indigenous young adult participants.
To solely focus on ACEs without giving similar attention to BCEs and positive adulthood factors sends a message that the impacts of ACEs are destiny and amplifies the power of deficits-driven narratives about Indigenous communities. Congruously, focusing solely on either BCEs or ACEs does not consider impacts across life-course development or offer ways to improve outcomes. In this study, we examine associations between ACEs, BCEs, and adult protective factors with respect to Indigenous well-being in young adulthood (Figure 1A and C). Drawing upon the Stress Process Model and the ISCM, we further examine the potential for BCEs (an early life protective factor) and early adult family satisfaction and social support to moderate the impact of ACEs on adult well-being (Figure 1B).
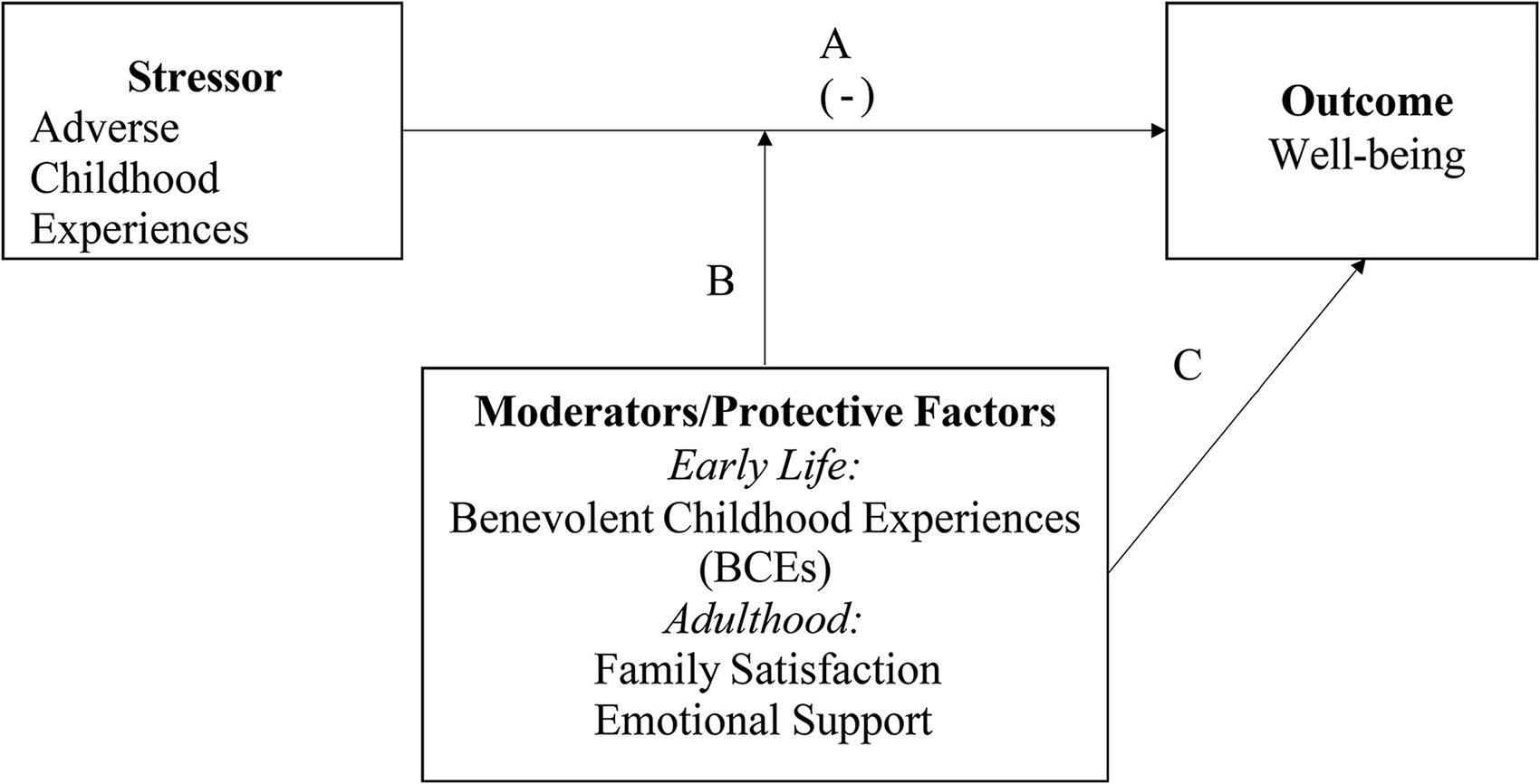
Conceptual model. Note: (-) denotes expected inverse relationships. Line B represents expected stress-buffering (moderating) associations.
Our analyses account for three control variables: gender (females have been shown to experience greater psychological distress than males; Kessler, 2002); income (those with higher income have been shown to have greater well-being; Mirowsky & Ross, 2003); and relationship status (current relationship status has been linked to well-being, such that those in committed or stable relationships tend to have better mental health than those who are not; Braithwaite et al., 2010; Girme et al., 2016).
Methods
Participants
Participants are from the Healing Pathways study, a longitudinal, community-based participatory research panel study with Indigenous families from four reservations in the upper Midwestern United States and four reserves in Ontario, Canada. The baseline sampling procedure (2002) involved contacting all families with a tribally enrolled adolescent aged 10–12 living on, or within, 50 miles of participating reservations/reserves. Interviewers received training in human subjects’ protection and conducting paper and pencil surveys. Trained interviewers contacted participants and completed in-person survey interviews annually from 2002–2010 (average adolescents, 11–18 years old), then re-contacted participants in 2017 when the average age was 26 years. Data for the current analyses are derived from the 453 young adult participants interviewed at wave 9 of the study (2017–2018). Participants received a $50 visa gift card or check at the completion of the interview. Community Research Council (CRC) members are involved in all aspects of study design, implementation, and data dissemination. All participating reservations/reserves granted Tribal Resolutions to support this work and all study procedures and materials were approved by the University of Minnesota institutional review board.
Measures
Survey development processes for the study included intensive CRC brainstorming meetings and pilot sessions during which Indigenous community members provided feedback on comprehension and validity of various survey items. In addition, CRC members met regularly over the course of several months to review drafts of survey documents. They provided the university team feedback on cultural and community “fit” or relevance of measures, offered suggestions for improving local understanding/wording, and nominated survey items for addition or deletion.
Dependent variable
Well-being was measured using an adapted version of the Flourishing Scale (Diener et al., 2010). Respondents were asked how strongly they agreed with 8 items related to self-perceived success in areas of well-being such as relationships, self-esteem, purpose, and optimism. Examples include, “I lead a purposeful and meaningful life,” and “I am optimistic about my future.” Item scores ranged from 0 (strongly disagree) to 4 (strongly agree). Items were summed to create a final variable (range 0−32) with higher values indicating greater well-being (α = .89). The Flourishing Scale has been shown to be both reliable and valid in studies involving thousands of people across many cultures and among diverse age groups (De la Fuente et al., 2017; Diener et al., 2010; Martín-Carbonell et al., 2021; Romano et al., 2020; Tong & Wang, 2017). This scale has demonstrated high convergence with other psychological well-being measures including Deci and Ryan's Basic Need Satisfaction in General Scale and Ryff's Scale of Psychological Well-Being (De la Fuente et al., 2017; Diener et al., 2010; Martín-Carbonell et al., 2021; Romano et al., 2020; Tong & Wang, 2017).
Independent variables.
Benevolent childhood experiences (BCEs) were measured using an adapted version of the Benevolent Childhood Experiences scale (Narayan et al., 2018). Members of CRCs provided intensive feedback to suggest removing two of the original items from the measure. The resulting items assess favorable experiences that occur between birth and 18 years old and are characterized by perceived safety, security, and support, and positive and predictable qualities of life. Examples include, “Did you have beliefs that gave you comfort?” and “Did you have at least one caregiver who you felt safe with?” Response options were no (0) or yes (1). We conducted a confirmatory factor analysis of a single latent variable in MPLUS and factor loadings were >.40 once “Did you have a predictable home routine, like regular meals and a regular bedtime?” was removed. Items were summed to create a final BCE score.
Adverse childhood experiences (ACEs) were measured using an adapted version of the Adverse Childhood Experiences – International Questionnaire (World Health Organization, 2018). To maximize validity of the measure for the contexts in which this research takes place, slight modifications driven by CRC input were made to the ACEs questionnaire. For example, question stems that started with “did you see …” were changed to “how often did you see …” when the response options asked for frequency of experiences. Items used in this study assessed for exposure to eight adversities that occurred during the first 18 years of life. These included child abuse (i.e., sexual, physical, and emotional abuse) and exposures typically referred to collectively as household dysfunction (i.e., divorce/separation, household violence, growing up with someone who had mental illness or a substance abuse problem, having a household member go to jail or prison). Participants were considered exposed to each adversity type if they reported ever having the experience during the first 18 years of life (1 = yes, 0 = no). ACE variables were then summed to create a continuous ACEs score index (α = .78). Participants were included in this continuous index assessment if they completed responses for at least four of the eight ACE variables.
Family satisfaction was measured using an adapted version of the Marital Satisfaction Scale (Schumm et al., 1986). Respondents were asked how satisfied they were with their relationship with their family. The item score ranged from 0 (very dissatisfied) to 4 (very satisfied).
Receiving emotional support was measured using a subscale of the 2-Way Social Support Scale (Shakespeare-Finch & Obst, 2011). Examples include, “there is at least one person that you can share most things with,” and “you feel like you have a circle of people who value you.” Items scores ranged from 0 (not at all true) to 3 (always true). Items were summed to create a final variable with higher values indicating greater experience of receiving emotional support (α = .87).
Controls.
Three demographic variables were included as controls. We relied on reports of gender at wave 1 for complete gender information. Gender was coded as female = 1; male = 0. Income was a continuous measure in thousands of dollars. Current romantic relationship status was coded as yes (in a relationship) = 1; no (not in a relationship) = 0.
Analytic strategy
A total of 12 participants were missing data on at least one variable included in the analyses and were removed from the final analyses. The final analytic sample is 441 participants. We conducted an attrition analysis of those who did not participate in the current study wave compared to those included in the analyses. Males and participants who resided off reservation/reserve land at baseline had higher odds of attrition compared to females and those who resided on reservation/reserve land at baseline. We present bivariate zero-order bivariate correlations of all variables included in the analyses. Next, we present multiple linear regression models predicting well-being. In the first model, we examine the association between ACEs and well-being controlling for demographics controls. We separately enter each of the positive coping variables individually. In the final model, we examine the joint contribution of all variables. To examine possible buffering effects between ACEs and BCEs, family satisfaction, and receiving emotional support, three interaction terms were created and tested individually.
Results
An average of 6.5 (SD = .91) BCEs were reported with 66.7% of the participants reporting experiencing all 7 possible BCEs. An average of 3.4 (SD = 2.4) ACEs were reported with 86% reporting at least 1 ACE (Table 1).
Descriptive statistics (N = 441).
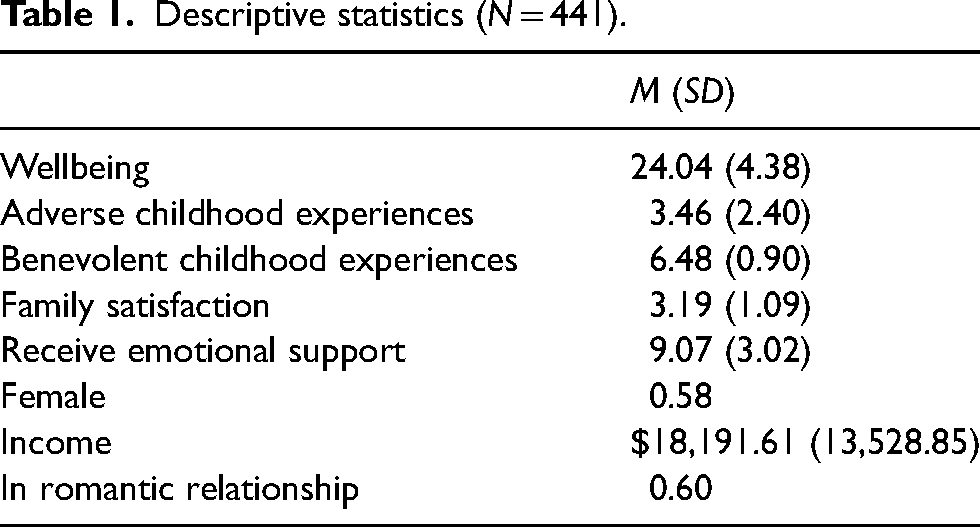
Table 2 present the bivariate correlations of all variables included in the analyses. The major predictor variables (i.e., early life and adulthood stress/coping factors) were all significantly associated with well-being at the bivariate level in expected directions (i.e., ACEs negatively associated and protective factors positively associated with well-being). ACEs were negatively associated with BCEs, family satisfaction, and receiving emotional support. BCEs, family satisfaction, and receiving emotional support were all positively associated with one another.
Correlations matrix (N = 441).
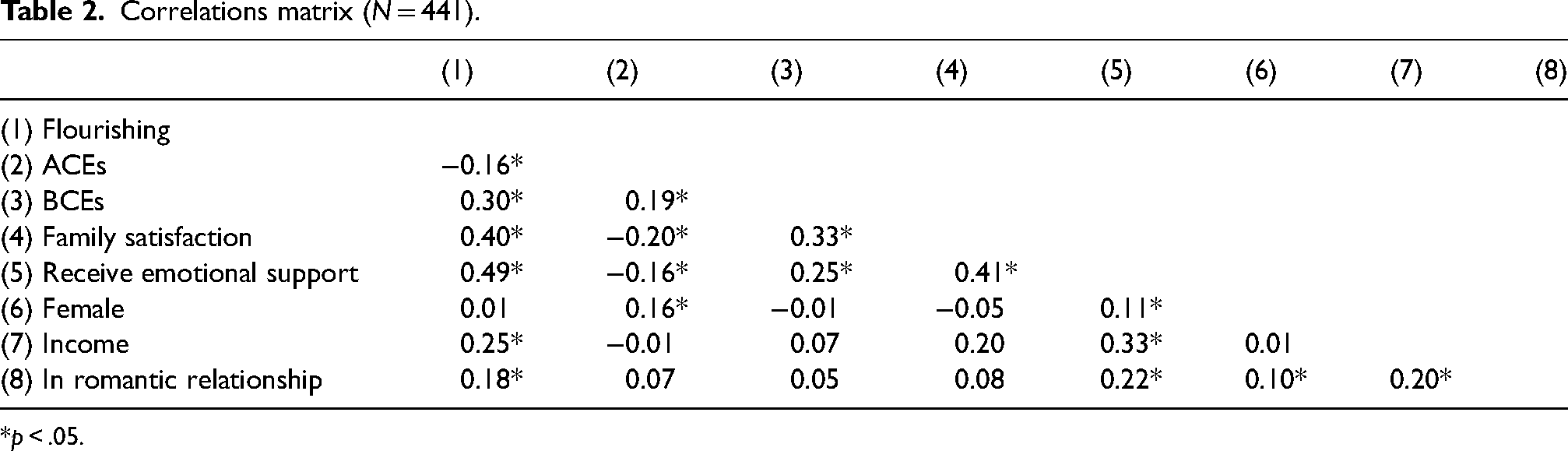
*p < .05.
Table 3 presents the regression models predicting well-being. In Model 1, ACEs were negatively associated with well-being (β = −.17; p < .01) controlling for demographics. In Models 2–4, BCEs, family satisfaction, and receiving emotional support were added to the models individually. In each of these models, ACEs remained negatively associated with well-being, but the association attenuated. The models with family satisfaction and receiving emotional support showed the largest decreases in the association between ACEs and well-being, compared to the model with BCEs. In Model 5, all variables were included. ACEs were no longer associated with well-being. BCEs (β = .14; p < .01), family satisfaction (β = .19; p < .001), and receiving emotional support (β = .33; p < .001) were positively associated with well-being. We tested for possible buffering interactions between ACEs and BCEs, family satisfaction, and receiving emotional support. None of these interactions were significant (results not shown).
Regression models predicting well-being (N = 441).
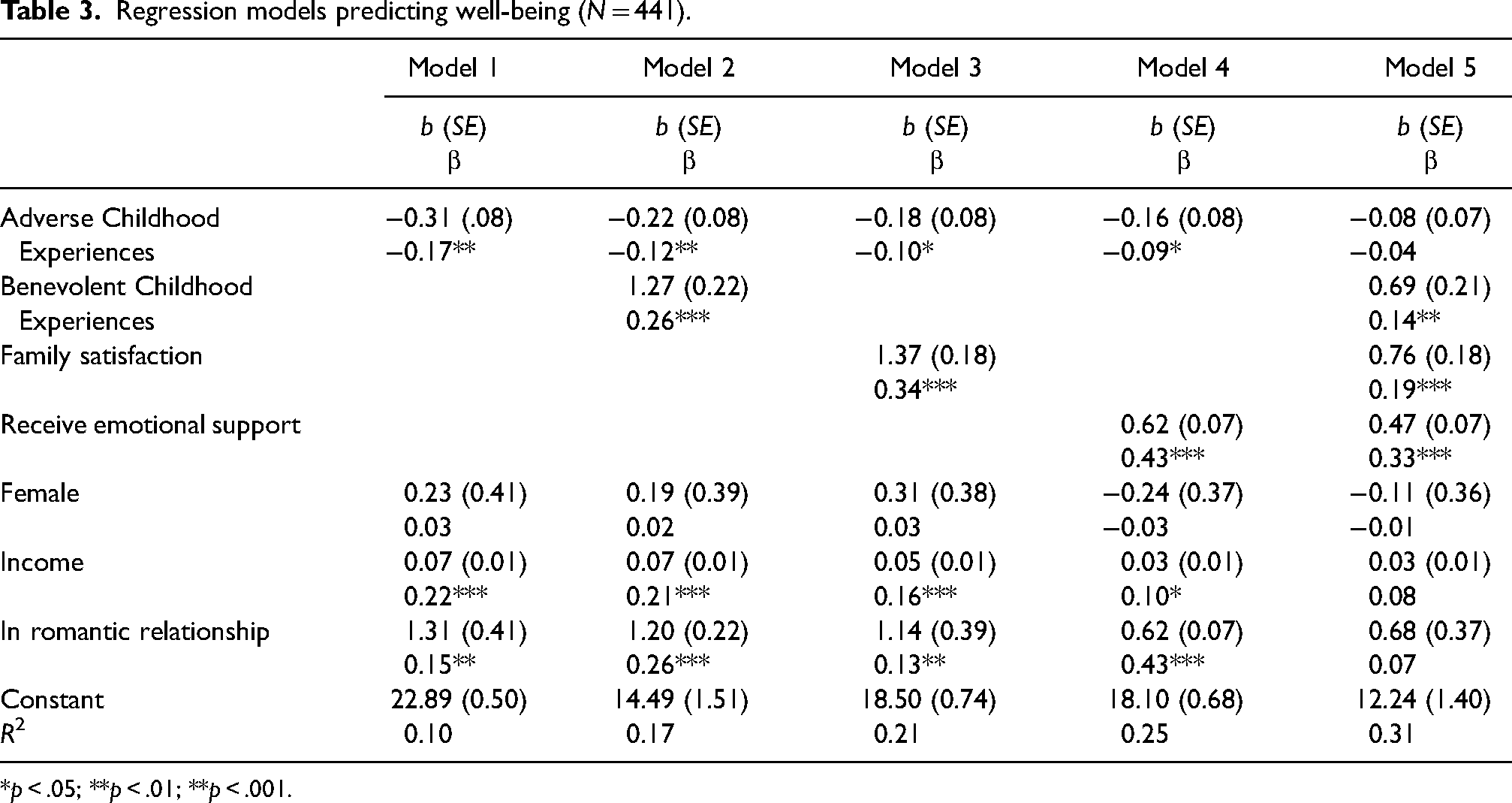
*p < .05; **p < .01; **p < .001.
Discussion
The expansive body of ACEs research has revolutionized our understanding of early life stress and trauma and how the effects of such can last a lifetime (Merrick et al., 2017; Roh et al., 2015). However, this body of work is not without challenges (Anda et al., 2020; Lacey & Minnis, 2020), and such narratives when applied to groups like Indigenous peoples can perpetuate erroneous and stigmatizing narratives of victimization, ignoring positive lived experiences and important work in advocacy and social change (LaPier & Beck, 2015; Vizenor, 1999). Key factors of individual and community well-being include protective and stress buffering effects, which can be considered in tandem using stress process theoretical frameworks.
This work empirically identifies select stress process factors from across the life course and is rooted in stress process models of health that have implications for improving well-being within Indigenous communities. We support the call for strengths-based research from tribal communities and acknowledge that narratives of strength and well-being are much needed (Kading et al., 2019; National Congress of American Indians et al., 2015). This study responds to this call and findings are a step toward balancing deficits-based research about Indigenous families. We are not alone in this regard: the work of Dr. Michael Chandler highlighted throughout this Special Issue was among the earliest to empirically examine Indigenous strengths. His innovative approach included recognizing Indigenous community assets and active efforts to preserve cultural strengths as “cultural continuity,” and to tie such continuity to positive population-level health outcomes (Chandler & Lalonde, 1998).
Among participants, 86% reported at least one ACE. This is consistent with other studies’ reports of one or more ACE among American Indian participants (82% in Brockie et al., 2018; 83% in Koss et al., 2003; 86% in Warne et al., 2017). Adverse childhood experiences are an important consideration for future well-being, yet they are only part of the story. Indeed, the strength of association between ACEs and young adult well-being was weaker than that between BCEs and well-being. In addition, the sizes of the correlation coefficients for BCEs with adulthood protective factors were larger than correlations between ACEs and these same protective factors. Thus, while ACEs are associated with fewer adult assets like family satisfaction and emotional support, BCEs were correlated even more strongly with these protective mechanisms. These findings amplify the need to delineate stressors and protective factors and outcomes in the stress process and clarify how each of these may have different impacts. It could be that ACEs (or other stressors) are more strongly associated with negative outcomes, while BCEs (or other protective factors and/or stress-buffering resources) may be more strongly associated with positive outcomes, a topic worthy of additional inquiry in stress process studies.
Results of this study reveal very high occurrences of positive early life experiences in the form of BCEs among study participants. Although some measurement differences caution comparisons to other studies, BCEs reported here are much higher than found in prior literature (Narayan et al., 2018). Our study uses an adapted questionnaire with 7 out of the original 10 BCEs; 66.7% of the Healing Pathways wave 9 participants reported experiencing all of the BCEs measured. Studies that have used the 10 item scale have found that 39% and 27.7% of the participants reported experiencing all of the BCEs, respectively (see Crandall et al., 2019; Narayan et al., 2018). Paralleling these findings, prior studies have revealed other important strengths in the form of mental health outcomes in Indigenous communities and communities of color. For example, Walls et al. (2016) found disproportionately high rates of psychological well-being (even amidst elevated rates of depressive symptoms) across two distinct Indigenous samples compared to findings from previously published studies with non-Native groups. Further, Keyes (2009) found paradoxically high levels of “flourishing” mental health status among Black Americans, despite differential exposure to structurally rooted stressors like discrimination. An important message is revealed by this line of research: when we take the time to measure positive outcomes and protective factors in diverse communities, we in turn observe them. Indeed, the centrality of community strengths and connectedness are hallmarks of Indigenous frameworks of well-being (Ullrich, 2019) and such cultural values likely propel the elevated levels of BCEs we observed.
Strengths-based research and perspectives have shown the important distinction between mental health and mental illness, and that health is not merely the absence of disease (Kading et al., 2015, 2019; Keyes, 2005). Health paradoxes have been observed among Black Americans who experienced better mental health compared to White Americans despite experiencing greater stressors (Keyes, 2009) and Indigenous communities who experienced flourishing mental health coupled with heightened psychological distress (Walls et al., 2016). Just as the absence of mental illness does not equal mental health (Keyes, 2005), the presence of mental illness, or psychological distress, does not prevent mental health (Walls et al., 2016). Our findings extend this framing to include other positive experiences that are conducive to well-being. That is, BCEs and ACEs are not mutually exclusive (Narayan, Ippen, et al., 2017), and BCEs exemplify survivance, an active sense of resistance, presence, and endurance (Vizenor, 1999). In the midst of historical oppression, lived experiences include the reality and opportunity for positive factors. Reducing risk and promoting strengths are both important to well-being.
Our findings also suggest that BCEs are associated with well-being beyond childhood, even when considering ACEs and positive adult experiences. The association between ACEs and young adult well-being dropped from statistical significance after accounting for positive childhood and adult experiences. There are a few ways this could be interpreted: (1) adult positive experiences may attenuate the impacts of ACEs on well-being; (2) BCEs may interact with adult positive experiences in additive effects to impact well-being.
Family satisfaction and receiving emotional support were robust predictors of adult well-being in our multivariate models and this is a promising point for promoting well-being. While the onslaught of colonization resulted in far reaching disruption of family systems among Indigenous communities, traditional and contemporary values and practices in many Indigenous communities reinforce the interconnectedness of individuals, family, community, and spirituality. Connectedness is posited as “one of the keys to Indigenous survival and well-being” in direct opposition to colonization (Ullrich, 2019, p. 121). The impact of family satisfaction on adult well-being may be especially pronounced because of the value placed on family connections as well as the broad nature of what family entails among many Indigenous communities (Kading et al., 2019; Martin & Yurkovich, 2014). Further, our results expand the importance of emotional support for well-being among Indigenous communities (Richmond et al., 2007). These analyses used select childhood and adult stress process factors to determine associations with well-being. While childhood experiences are important associations with adult well-being, a balanced picture of both positive and negative childhood and adult stress process factors is necessary to have the greatest understanding of the associations with well-being. These results may have important implications for understanding how these factors operate to impact well-being.
The impacts of childhood experiences on adult well-being are not destiny. For those who have experienced ACEs and lack emotional support and family satisfaction in adulthood, there are still opportunities to foster wellness. Involvement in traditional spiritual and cultural activities and connectedness to family, nature, and community have been found to be protective for mental and physical health among Indigenous populations (Bear et al., 2018; Brockie et al., 2018; Chandler & Dunlop, 2015; Chandler & Lalonde, 2008; Kading et al., 2015). Additionally, select therapeutic approaches have shown promise for improving emotional, social, and cognitive indicators among adults who have experienced ACEs (Korotana et al., 2016). Thus, for those adults who have experienced ACEs and lack emotional support or family satisfaction, increased engagement in cultural and spiritual activities, as well as seeking out appropriate therapeutic opportunities, may strengthen well-being.
Limitations and future research
This study showed that BCEs were positively associated with well-being. However, there are additional factors, such as language use, traditions, and environmental and spiritual connection, which are not included in the BCE scale that have been shown to be protective for health among Indigenous populations (Gonzalez et al., 2017; Ullrich, 2019). Relatedly, an important part of our community-based participatory research (CBPR) approach is collaborative measurement development and adaptation. Based on community feedback, our team adapted and included 8 of 10 possible BCE indicators (one of which was removed from analyses based on factor analysis findings—see Results section) from the original source measure. Moreover, there was a ceiling effect with the BCE measure in that most respondents reported all 7 BCEs. This lack of variability precludes examination of whether there are tipping points with BCEs where protective effects are most pronounced. Additionally, we recognize that, while the Flourishing Scale (Diener et al., 2010) includes a constellation of factors widely considered vital for well-being, this measure is limited in its capacity to fully encompass holistic well-being and may not incorporate culturally relevant components specific to Indigenous communities. There is considerable need for measurement development and evaluation work to develop Indigenous-centric measures of BCEs and well-being, assess psychometric properties of these novel measures, and improve the relevance of such indicators to diverse Indigenous contexts.
In this study, we were unable to determine the temporal ordering of ACEs and BCEs. Future research could better establish timing of ACEs and BCEs, as well as examine mediation and moderation of outcomes. This study involved retrospective reporting of ACEs and BCEs among a cohort of young adult participants. This may have led to underestimates, or overestimates, of the occurrence of each of these kinds of childhood experiences.
The impact of BCEs extending across the life course has yet to be determined. Just as ACEs can be intergenerational (Narayan, Kaltabakken, et al., 2017), it is possible that BCEs may persist across generations. These intergenerational pathways may operate through using benevolent childhood memories as examples for positive methods of interaction with subsequent generations, as well as adult support networks that encourage and support positive decisions (Lieberman et al., 2005; Schofield et al., 2013). Future research is needed to explore the intergenerational pathways of BCEs.
Conclusion
This article responds to the call for strengths-based research with Indigenous communities and takes a holistic approach to examining influences on adult well-being by looking at select childhood and adult stress process factors. By illuminating the abundant presence of BCEs experienced by the majority of study participants, this study contributes to a body of work that uplifts the strengths of Indigenous communities and combats dominant, deficit-based narratives about Indigenous families (Gray et al., 2019; Kading et al., 2019; Martin & Yurkovich, 2014). In demonstrating the influence of BCEs and adult positive experiences on adult well-being, even in the presence of ACEs, this study provides possible directions for interventions to promote adult health and well-being.
Footnotes
Acknowledgements
The authors would like to thank the Community Research Council members and interviewers of the Healing Pathways team: David Bruyere, Laura Bruyere, Annabelle Jourdain, Priscilla Simard, Trisha Bruyere, Jake Becker, Laureen Hill, Frances Whitfield, GayeAnn Allen, Tina Handeland, Victoria Soulier, Bagwajikwe Madosh, Betty Jo Graveen, Clinton Isham, Carol Jenkins, Bill Butcher Jr., Delores Fairbanks, Devin Fineday, Bernadette Gotchie, Gloria Mellado, Marilyn Bowstring, Gary Charwood, Gina Stender, Darold Madigan, Kathy Dudley, Geraldine Brun, June Holstein, Frances Miller, Brenna Pemberton, Ed Strong, Barbara Thomas, Charity Prentice-Pemberton, FaLeisha Jourdain, Penny King, Valerie King, Linda Perkins, Christie Prentice, Gabe Henry, Howard Kabestra, Dallas Medicine, Glenn Cameron, Jackie Cameron, Gerilyn Fisher, Virginia Pateman, Irene Scott, Cindy McDougall, Chantel King, Whitney Accobee, Celeste Cloud, Pat Moran, Stephanie Williams, Natalie Bergstrom, Bonnie Badboy, Elizabeth Kent, Sue Trnka, and Laurie Vilas. The authors would also like to thank Lucas Kosobuski for his work on the references.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: research reported in this manuscript is supported by the National Institute on Drug Abuse of the National Institutes of Health under Award Number DA039912 (M. Walls, PI). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.