
Abstract
This study aimed to understand the perceptions and experiences of suicide attempters in order to suggest potential initiatives to reduce the suicide burden in rural India. The study is based on 46 in-depth interviews with suicide attempters and 4 focus group discussions with their family members. Interview content analysis revealed information related to four anticipated themes: the characteristics of a suicide attempt are complex; suicide attempters are taken to public hospitals for first aid and treatment; the consequences of suicide attempts are diverse; and quality of life improved after the suicide attempt. There were also two unanticipated themes: suicide attempters sought help from potential rescuers; and the underreporting of suicide attempts. Emergent themes from the focus group discussions were the vulnerable group for suicide; poverty, indebtedness, family conflicts and unemployment are the main reasons for suicide; non-violent methods are used to commit suicide; there were no behavioral changes before suicide; the devastating effects on the families of decedents; positive community support to suicide survivor families; and expectations of preventive measures from both the community and government. The article argues that to reduce the suicide burden, the government should adopt a two-pronged strategy of creating a secure livelihood all-year round and providing psychological counseling at both the household and community levels.
Introduction
Suicide is a significant public health concern, and is responsible for more than 8 million deaths every year, equivalent to the death of 1 in 40 individuals (World Health Organization [WHO], n.d.a). Suicide accounts for 1.4% of deaths worldwide, making it the 18th leading cause of death in 2016 (WHO, n.d.a). Although suicide occurs throughout the lifespan, it is the second leading cause of death among the 15–29 years of age cohort globally (WHO, n.d.a). Suicide is responsible for more than 50 billion USD in medical and work loss costs (Florence et al., 2015). Compared with other regions of the world, suicide is second highest in Southeast Asia, with the highest suicide mortality rate reported in India (WHO, n.d.a). Over the past three decades, from 1990 to 2016, India's contribution to global suicide deaths has increased by 11.3% for women and by 5.3% for men (Dandona et al., 2018).
The most widely studied risk factors for suicide include sociodemographic variables and psychiatric disorders, genetic predisposition, and gene–environment interactions (Mandelli & Serretti, 2013). Although studies on suicide have tended to focus on individuals’ psychological, economic, and social conditions (Brancaccio et al., 2013), Emile Durkheim (2005) argued that suicide was not simply an individual action but had to be considered at the society level. Durkheim suggested that suicide is a pathological condition of society rather than an individual condition and may be the result of a lack of social integration or solidarity (Keyes & Daniel, 1983). In western countries, the ethical debate on suicide has centered around personal autonomy and freedom issues versus the responsibility of mental health professionals toward suicidal individuals. By contrast, in developing countries, the issues are more concerned with macro-level equity, justice, and social conditions related to mental distress and suicidal behavior (Khan & Mian, 2010).
In Telangana State, the age-standardized suicide death rate of 18.8 per 100,000 women and 25.2 per 100,000 men has been reported (Dandona et al., 2017). Further, over past decades, disability-adjusted life years due to suicide in Telangana have risen from ninth in the 1990s to fifth in 2016 (Institute for Health Metrics and Evaluation, n.d.). In Telangana State, suicide is the third leading cause of years of life lost and is a significant contributor to death in the 15–39 years age cohort (Institute for Health Metrics and Evaluation, n.d.).
To fully comprehend suicide in context, quantitative studies must be supplemented with qualitative ones. A qualitative approach allows us to examine relationships between factors in ways that quantitative studies using standardized questions do not. In particular, qualitative methods can examine the underlying reasons, motivations, and opinions involved in suicide (Hjelmeland & Knizek, 2010). Qualitative research investigates individuals’ attitudes, perceptions, and experiences in depth, focusing on “not only what people think, but how they think and why they think that way” (Kitzinger, 1995, p. 299). In India, qualitative research has been conducted at the community level to understand the effects of social structure and gendered roles on suicide behavior (Lasrado et al., 2016), and the reasons for farmer suicide (Dongre & Deshmukh 2012), as well as the feasibility of using centralized pesticide storage facilities as a suicide-prevention strategy (Mohanraj et al., 2014; Vijayakumar et al., 2013). Qualitative research in the hospital context has been used to explore nurses’ attitudes toward suicide attempters (Nebhinani et al., 2013) and to identify gaps in suicide-prevention training programs for physicians (Eynan et al., 2015).
In the southern part of India, only one community-level study has been conducted to better understand perceptions of suicide (Manoranjitham et al., 2007). To address the limited data, the current qualitative study sought to better understand the public's perception of suicide, investigate the experiences of suicide attempters, and gain insight into suicide and potential initiatives to reduce the suicide burden. This was accomplished by conducting interviews with previous suicide attempters and community members to provide a comprehensive view of suicidal behavior at both the community and individual levels.
Method
Study sites and participants
The qualitative data used in this article were part of a major government-funded project. The study protocol was reviewed and approved by the ethics committee, Department of Anthropology, University of Delhi. Participants of both focus group discussions (FGDs) and in-depth interviews gave verbal consent to participate in the study. The current study identified suicide decedents and suicide attempters from Mahatma Gandhi Memorial Hospital, Warangal, Telangana. Based on secondary data provided by the hospital for the period between 2010 and 2017, the villages of Devvanapet, Nagaram and Mutcherla in Hasanparthy Mandal, Warangal district were selected for conducting the qualitative research. Devvanapet village is in Hasanparthy tehsil (a local unit of administrative division in India) of Warangal district, 5 kilometers from Hasanparthy subdistrict headquarters and 10 kilometers from Warangal district headquarters. The village covers 80.19 hectares, with an 8-hectare non-agricultural area and a total irrigated area of 185 hectares. It has 1024 households and a total population of 4047 (49.8% male and 50.2% female). Devvanapet has a literacy rate of 56.3% and a working population of 55.7% (onefivenine.com, n.d.). Nagaram is located in the Hasanparthy tehsil of the Warangal district, 10 kilometers from the subdistrict headquarters at Hasanparthy and 20 kilometers from the district headquarters in Warangal. The village covers 13.66 hectares, the non-agricultural area is 10.4 hectares, and the total irrigated area is 412.4 hectares. It has 1115 households and a total population of 4077 (49% male and 51% female). The literacy rate is 57.1%, and the working population is 51.6% (onefivenine.com, n.d.). Mutcherla, the third village of the study, is in Hasanparthy tehsil of Warangal district, 5 kilometers from the subdistrict headquarters Hasanparthy and 7 kilometers from the district headquarters in Warangal. The village has 79.2 hectares of non-agricultural land and 402.7 hectares of irrigated land. It has 994 households and a total population of 3691 (50.4% male and 49.6% female). The village has a literacy rate of 61.9% and a working population of 51.6% (onefivenine.com, n.d.).
Before conducting the fieldwork, the head (sarpanch) of each village helped us to confirm the local incidence of suicide and gave additional details about suicide decedents and suicide attempters not reported to the hospital.
Qualitative data collection and analysis
Individual in-depth interviews with suicide attempters were conducted to investigate sensitive topics such as the characteristics of the suicide attempt (impulsive or planned), the rescue and treatment procedure, the outcome of the suicide attempt, coping mechanisms used post attempt, and quality of life. On average, each in-depth interview was conducted for 30–45 minutes with individual participants. These interviews were conducted at participants’ homes using a structured, in-depth interview guide, which was translated into Telegu and its accuracy reviewed by a bilingual speaker (coauthor). Research scholars moderated in-depth interviews, and a fieldwork translator (Telugu speaker) assured that the questions asked during the interview had the intended meaning in the local language. The translator gave additional explanations to the participants wherever required. For individuals with more than two suicide attempts, details of the most recent suicide attempt were asked for. The entire audio-recorded interview underwent professional translation for accurate interpretation. This transcript was then cross-checked by the Telugu and English bilingual speaker (coauthor KNS), and any discrepancies were resolved by reviewing the audiotapes.
FGDs with family members were held to identify and clarify shared knowledge about suicide in the village, methods used for self-harm, life stressors that lead to suicide, the impact on suicide survivors, behavioral or lifestyle habits observed before suicide, and suggestions to reduce suicide in their village. FGDs were held in the village center, which was convenient for the participants. The duration of each FGD was 45–60 minutes. During the FGDs, participants were served refreshments, but no monetary compensation was provided. To ensure an inclusive environment, FGDs were conducted by KSK and SR, research scholars fluent in Telugu and specializing in sociology who recently obtained their doctoral degrees from Kakatiya University, Warangal, Telangana State. Their combined expertise contributed significantly to the fieldwork conducted. The moderators used a semi-structured interview schedule comprising probe questions, introducing participants to the discussion; follow-up questions exploring the circumstances surrounding the suicide attempt, focusing on the reasons behind it, whether it was planned or impulsive, the location and witnesses, and any medical treatment received; and exit questions exploring the impact on relationships and personal health, coping mechanisms employed, current state of happiness, and any vulnerability to future suicidal thoughts. The moderators assured equal participation from each member. All the FGDs were audio-recorded. During the discussion, the observer made notes, including significant quotes, key points and themes, and follow-up questions. FGDs were transcribed, and a simple report comprising key findings was prepared after each individual FGD.
The qualitative data was managed and visualized in NVIVO Pro 11 (QSR International). The current study used the framework analysis method for qualitative data (Ritchie & Spencer, 2002). The stages of the analysis were: (a) preparation of transcription; (b) familiarization with interviews; (c) coding; (d) developing a working analytical framework; (e) applying the analytical framework; and (f) plotting data into the framework matrix (Gale et al., 2013).
Ethics approval
The study was approved by the institutional ethical committee, Department of Anthropology, University of Delhi, India. All the subjects gave informed written/verbal consent.
Results
Findings from the in-depth interviews with the suicide attempters
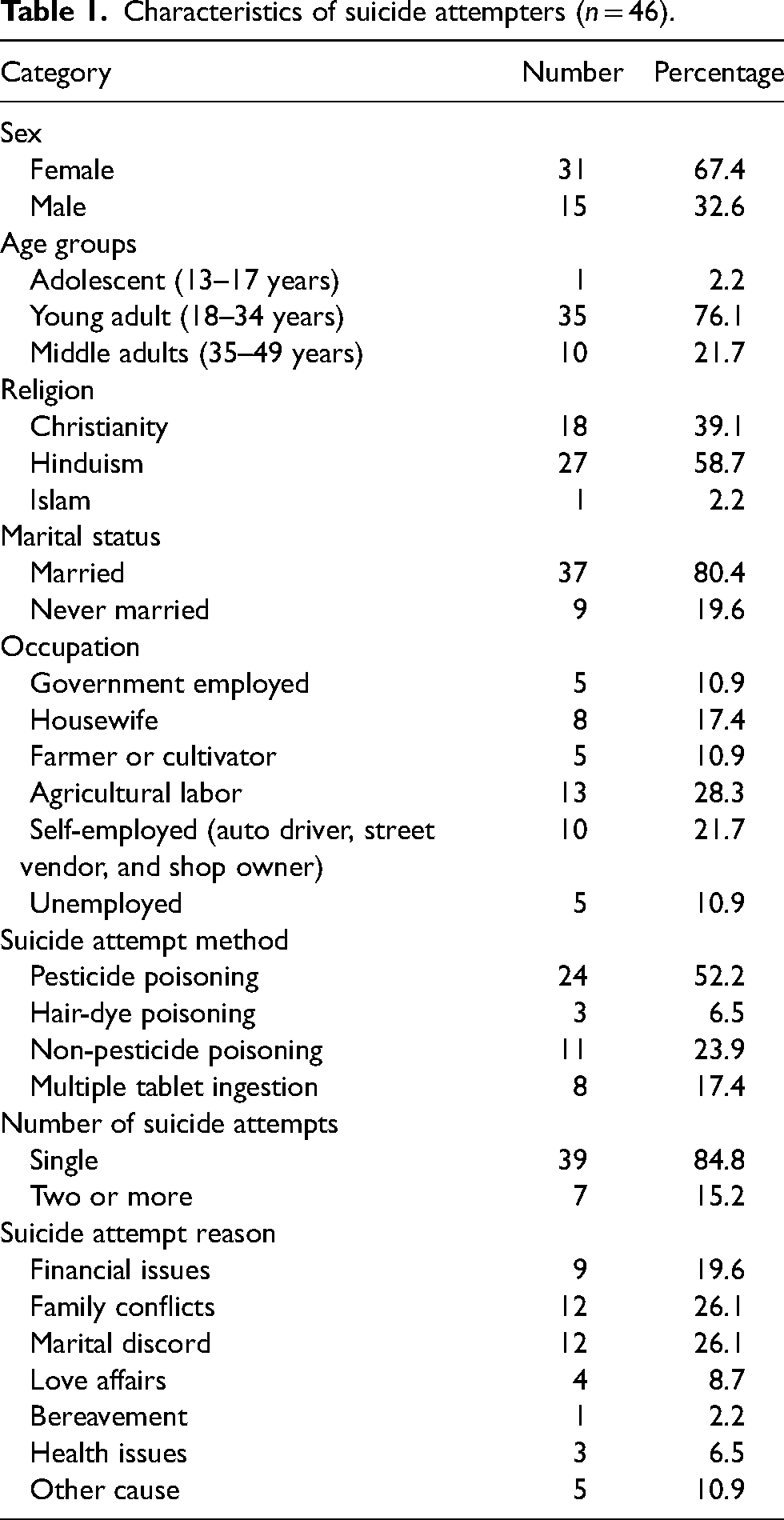
The interviewed suicide attempters were 32.6% males and 67.4% females. Most were young adults (76.1%), identified as Hindu (58.6%), married (80%), and working as agricultural laborers (28.3%). The most common method of attempted suicide was pesticide poisoning (52.2%), followed by non-pesticide poisoning (23.9%), multiple tablet ingestion (17.4%), and hair-dye poisoning (6.5%). Of the 46 participants, 15.2% reported two suicide reattempts. Family conflict (26.1%) and marital discord (26.1%) were the most common triggers for suicide attempts (see Table 1 for demographic information and details of suicidal behavior).
Characteristics of suicide attempters (n = 46).
Characteristics of suicide attempt
Of the total number of suicide attempters (SA), 73.3% reported having made their attempt at home, whereas for the others the suicide attempt was made either in an agricultural field (22%) or the backyard of their house (4.4%). About half (53.5%) of participants reported that their attempt was carried out in solitude. Further, most of the suicide attempters (72.7%) said that their decision to end their life was impulsive and devoid of any thoughtful introspection in the aftermath of the act. However, a number of participants (27.3%) reported intense suicide ideation and planned preparation (purchasing pesticide, poison, or tablets for the attempt) before the suicide attempt. Among the male participants, 46.2% reported having consumed alcohol before their suicide attempt. I did not plan the attempt; it was a sudden decision to die. I was very sad at that time; I attempted suicide near the well in the middle of the agriculture field. There were some pesticide bottles for agriculture; I drank around one liter of pesticide. (SA 4) For those two days before the day of the attempt, I was behaving properly and doing my normal routine, but deep inside, I was empty and sad. I had consumed alcohol, and at around 5.30 pm, I told my mom I was not feeling good. I went to the field and attempted suicide. (SA 21) I bought the pesticides solely to attempt suicide. Since my parents were not alive, I was alone; I started crying and feeling depressed. I was not able to eat for two days. I attempted suicide inside my house at around 11 am when no one was in the house. That day I started drinking white water [homemade alcohol] early in the morning around 7 am. (SA 17)
First aid and treatment procedure
Most (91.1%) of the participants reported being admitted to the nearest government hospital, whereas 8.9% were admitted to a private hospital because of potentially fatal health complications. The suicide attempters reported that they were not admitted to the primary health center in the village because of a lack of medical facilities such as a gastric lavage machine and ventilator, and because they required antidotes for the poisons consumed. However, four participants mentioned that they were given first aid in the village before being taken to hospital. She [sister-in-law] started screaming and called everyone [family members], telling them that I drank poison. …They tried to make me vomit [using salt water], and after I vomited, they took me to hospital. (SA 2) My elder son and one of my neighbors were present at that time in my home. My neighbor put his hands in my mouth and removed some tablets. I was taken to the hospital after that. (SA 31) My aunt came inside, and she got the smell of kerosene and asked me what I did. I told her that I had taken kerosene. She called everyone, and nearly ten people came. They gave me salt water to vomit and then took me to hospital by auto. (SA 38)
Police also came and enquired about the incident. But I told them I took the poison because of some pain. I did not tell them the truth. So, they did not register a case. (SA 6; suicide attempt due to marital conflict)
At the hospital, I did not tell them [police] that I attempted to commit suicide; instead, I told them I had a severe stomachache, so I took several tablets. (SA 18; suicide attempt due to infertility).
About one-quarter (22.7%) of the participants immediately informed family members about their suicide attempt because of the manifested health complications. This plea for timely rescue possibly hints toward their weak suicide intent. After drinking the poison, I called my brother-in-law and told him I took the poison, immediately my sister and brother-in-law came to the spot, and they took me to the hospital. (SA 3) After I took poison, I went to my uncle's house, which was nearby, and I told my relatives that I had taken poison. (SA 5) I was thinking of attempting suicide for three days before finally attempting. I went to do agricultural work in the field in the afternoon. I found some pesticides in the field, and I brought them home. In the evening, I consumed the pesticide. After taking the poison, my stomach started hurting, and it was getting hard to tolerate. I later told my husband that I had taken pesticides. (SA 46
The consequences of suicide attempt
About half (56.1%) of the participants stated that their suicide attempt did not solve their problems. Further, for 32.6% of individuals, their attempt led to a greater economic burden because of the additional cost of treatment and regular check-ups after the suicide attempt. More than half of the participants (60%) complained of deteriorating health after the suicide attempt. However, 40% of participants reported that their suicide attempt solved their problems. I have more debt after my suicide attempt than before my attempt. We borrowed more money from my sister-in-law and others to pay hospital bills. We are already in debt, and again, we had to borrow money because I attempted suicide. (SA 15) The total cost of the treatment was around one lakh rupee [US $1400]; at that time, my relatives paid my expenses and later took a portion of my land in exchange. (SA 16) After my suicide attempt [pesticide poisoning], I could not stay in the sun for long; I feel dizzy, I am taking less food, I eat little. I also have chest and back pain; I also started having digestion problems, so I eat less. All this started after my attempt. I could not work more, and if I work for one or two days, I feel very lethargic and weak, so I could not work more; I am not very active. (SA 3) There were differences between my husband and me for quite some time, but after my attempt, there are minor changes in his behavior. … But, after this episode [suicide attempt], he started listening to me and once told me there was no point in fighting like this; we should happily stay together. (SA 6) My parents repaid my auto loan [post suicide attempt]; they paid the amount through monthly installments. (SA 41)
All my family members were very sad and worried. They were also disappointed in me and my decision to attempt suicide. Some even abused me for taking poison. (SA 4)
Everyone kept on saying I should not have done that; everybody cried a lot, my parents cried a lot. (SA 7)
My mother went into depression for 2–3 months, maybe because I was her first child, she felt awful that I attempted suicide. Her health was affected. (SA 18)
Coping strategies among suicide attempters
The coping strategies used by participants after their suicide attempt included: minimizing the importance of the problem (minimization coping style); dealing with the problem by finding alternative solutions (replacement coping style); avoiding the problem or specific situations (suppression coping style); engaging in relaxation activities to reduce stress (substitution coping style); and developing strong religious belief or practices (religiosity). Now I do not see the problem as big as I used to see it before attempting suicide, it is okay, now I do not overthink, and I keep myself happy for the betterment of my children. (SA 14; minimization coping style) Before my attempt, I used to be very casual with my life, and I used to roam around the village a lot. I felt that I was spoiling myself and my family all those days. After I realized that, I stopped drinking alcohol altogether, concentrating on my work and my earnings. (SA 10; replacement coping style) Though my mother-in-law has to stop cursing me, whenever I give my opinion about some things, all of my in-laws disagree with me and argue with me. So, to avoid arguments, I do not give my opinion anymore. I buried my feelings inside. (SA 13; suppression coping style) I am also a poet, and I kept on writing things ‘Birth is a gift of God, death also is a boon given by God; we should not play with life, we should not kill ourselves’. (SA 12; substitution coping style) We had fought for ten years, and now he has been fine with me for the last five years. I do not think situations have improved after my suicide attempt, but it is only due to my belief in God that things have improved. (SA 30; religiosity)
The kind of unpleasant experience I had during that time I am scared now to attempt suicide. Now I do not have any thoughts of suicide. (SA 22)
I am feeling quite happy and satisfied now. I do not have any major issues. Looking after my husband and my kids and hoping a better future for them is what I am looking forward to. (SA 43)
I will not repeat suicide attempts. Thinking about what would have happened if I had died due to my suicide attempt bothers me a lot. The fact that I am alive, and I can take care of my family is a blessing. (SA 7)
Sometimes I feel like committing suicide [due to husband's domestic abuse under the influence of alcohol and sudden death of elder son] … I do not feel there is any life left for me now. (SA 44)
Findings of focus group discussions
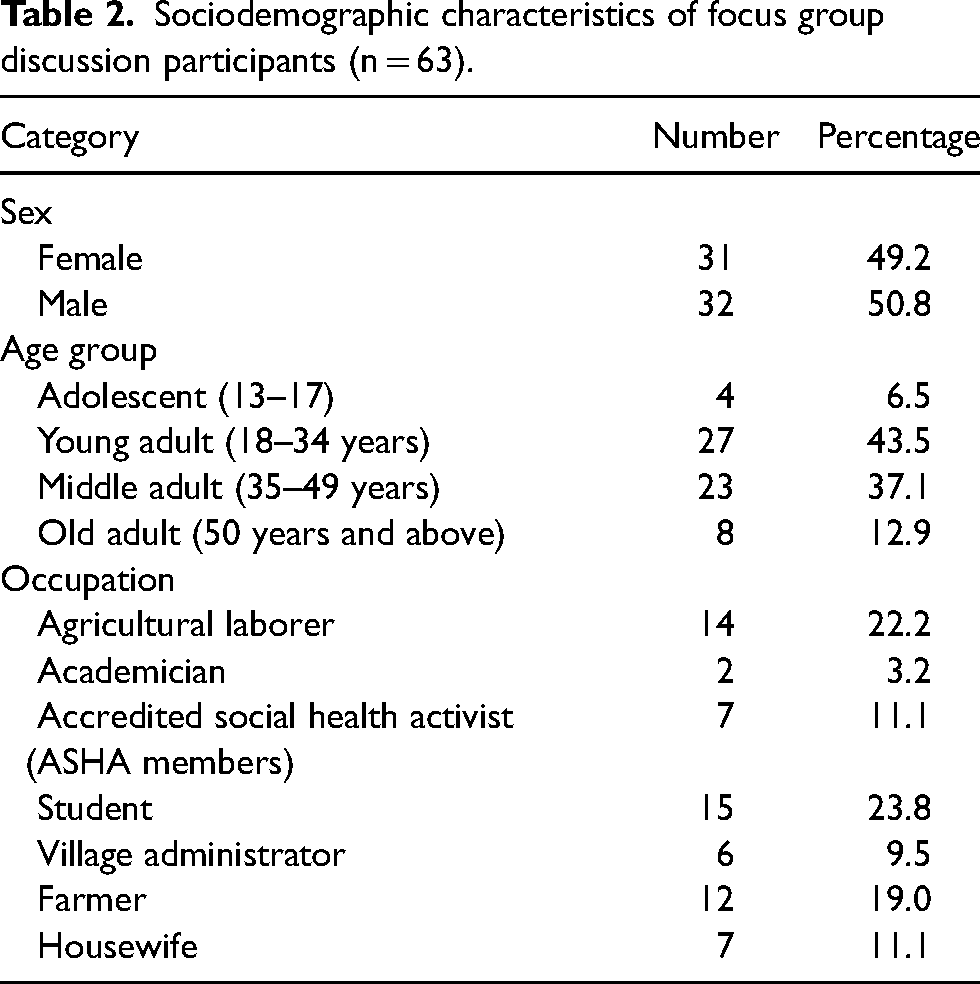
The four FGDs conducted in the three villages comprised groups of 15 individuals on average, with 49.2% female and 50.8% male participants. The participants were young adults (43.5%), middle-aged adults (37.1%), old adults (12.9%) and adolescents (6.5%), and were representative of a wide range of occupational groups including students (23.8%), academics (3.2%), village administrators (9.5%), accredited social health activists (ASHA members) (11.1%), farmers (19.0%), agricultural laborers (22.2%) and housewives (11.1%) (see Table 2 for details). The average duration of the focus group discussions was 45–60 minutes.
Sociodemographic characteristics of focus group discussion participants (n = 63).
Reasons for suicide in the village
The participants reported that the reasons for suicide in their village were poverty and unemployment. Indebtedness due to loans for agricultural or farm equipment was a common suicide trigger for farmers. Common triggers for males were alcohol addiction and marital conflict, whereas for females, family problems, dowry-related issues, and infertility were common triggers. Among adolescents, failure in love and conflicts with parents were common triggers. The reasons for suicide are love failures, financial difficulties, and family problems. Most of the males became alcohol addicts as they could not deal with family problems and financial difficulties. The problem of suicide is serious in this village. It is going viral. (Ex-village head, Devvanapet) There are more people who have taken the land on lease from the landlords and are unable to clear the debts due to lack of crop yield. These people [tenant farmers] are committing suicide. (FGD participant, Devvanapet) Reasons for suicides among women are unable to give dowry where the in-laws harass the women. Some women have gynecology problems [infertility], and they are unable to bear the medical expenses and commit suicide. (FGD participant, Devvanapet)
Groups vulnerable to suicide
Participants mentioned a higher prevalence of suicide from the Scheduled Castes (SC) and Scheduled Tribes (ST) families, tenant or landless farmers, the cohort aged 40 years and above, and individuals experiencing a financial crisis or personal reasons. Majority of the persons who committed suicide in this village are youth. More people from SC community than backward caste and forward castes. (BC member, Mutcherla) The vulnerable groups prone to suicide are individuals above 40 years of age; those with financial problems; those with negative feelings; and those with extramarital affairs. Both men and women are equally prone to suicide. (Registred Medical Practitioner, Devvanapet) The vulnerable group who are more prone to suicidal behavior are farmers above 40 years of age. Since farmers have these pesticides, it is more convenient for them to consume pesticides. (Pesticide shop owner, Mutcherla)
Suicide methods
Participants reported that non-violent (poisoning) and violent (jumping in front of a moving train, drowning, self-immolation, self-inflicted sharp object injury, and hanging) suicide methods were usually used in their village. The methods used for suicide are drinking poison, dying on the railway track, hanging, jumping in the well [drowning], and pouring kerosene oil [self-immolation]. Recently one person committed suicide on the railway track. (FGD participant, Devvanapet) The common methods adopted to commit suicide are primarily the consumption of pesticides, by mixing the poison in food or eating or drinking the poison directly after being drunk, secondly, hanging themselves, and others are pouring kerosene on the body [self-immolation], drinking wall paints. (FGD participant, Nagaram)
Behavioral and lifestyle changes observed among suicide decedents
Most participants denied noticing any behavioral or lifestyle changes among suicide decedents prior to their death. However, two participants noticed hopelessness and isolation among suicide decedents. Before the suicide behavior, very few [suicide decedents] showed symptoms like low mood. Majority of the time, it is difficult to predict if the person is going to commit suicide. (FGD participant, Devvanapet) They remain in solitude, feel psychologically low or depressed, are in their world [isolation], and show this suicidal behavior when nobody is there. (FGD participant, Nagaram) Indicating behaviors before suicide is not observable as we hardly get in touch with them…. One of the villagers, a few years back before committing suicide, was very jovial with everyone. After some time, he heated the knife under the flame and cut his throat in his house. (FGD participant, Mutcherla)
Impact on family members of suicide decedents
Participants described suicide as a devastating event that resulted in unfavorable emotional and economic aftermaths. The impoverished families found it challenging to conduct a funeral for the suicide decedents and borrowed money from neighbors or relatives. Bereaved family members faced financial constraints and suicide ideation after the sudden demise of the sole breadwinner. Participants also mentioned that young children had to discontinue their education. After their father's suicide, children were forced to take up work to make ends meet. Even old people who have lost their children due to road accidents, suicide, and sudden deaths are also committing suicide as they do not have any support system. Women who lost their husbands are also committing suicide as no one supports them. (FGD participant, Devvanapet) If the farmer dies without paying the bank loan, then his children and other family members work as daily laborers and slowly repay the loan. (FGD participant, Devvanapet) The children would discontinue studies and go to earn as a daily wage laborer to meet the expenses of the household. The children are forced to work instead of attending school as they cannot afford to bear education expenses. (FGD participant, Devvanapet) The family members of the suicidal committers feel bad, and they feel a void in the absence of the victim. They keep remembering the victim in every walk of life. (FGD participant, Nagaram)
Community support
Community members offered emotional support to bereaved family members and assisted in the funeral rites for the deceased. In some instances, the villagers voluntarily donated money to the bereaved families. Farmers’ union groups (Rthyu Sangam) aided the bereaved family members. At the community level, nobody helps the victim's [suicide decedent] family financially. Only assistance [manpower] to conduct funeral rites is given but not financial support. (FGD participant, Devvanapet) There are farmer union groups (Rthyu Sangam) who pay Rs.10,000 to Rs.20,000 (US $140–290) to the families of suicide decedents. However, this is only to the members of farmer union group. (FGD participant, Devvanapet) At the community level, there is a group where we collect Rs.300 to Rs500 [US $3–6] from the whole village irrespective of caste and economic level. We give this money to the deceased family members. (FGD participant, Mutcherla)
Government support
Participants highlighted the need for schemes that generate a constant flow of income throughout the year beyond agricultural income. They advocated providing loans to weaker sections of the society, financial aid to suicide decedents’ family members, and curtailing unauthorized pesticide purchases by issuing identification cards to farmers. In a year, through farming, we work only for three months; other months, we do not have any work. We can earn a living if the government can provide us with small jobs. In this way, the financial crisis can be sorted out. We cannot even pay that minimum premium of Aam Admi Bhima Yojana [social security scheme]. (FGD participant, agricultural labor, Devvanapet) Banks were not giving loans to our small farmers. They hardly come to our village as we cannot invest much in big amounts. Government should investigate this matter and support us in giving small loans with small interest. Here in this village, those farmers who are friendly with the local politicians benefit. Backward class people, farmers who do not have political contacts are not getting any support. (FGD participant, Devvanapet)
Participants also highlighted the need for bank loans for low-income families and farmers, a reduction in the price of pesticides, fixing crop prices, employment for qualified youth, financial scholarships for the children of suicide decedents, and a ban on the sale of alcohol in the villages. Loans are given only to people who have land but not to the lower socio-economic classes. Many people agree that jobless postgraduates have gone mad. Some young people with BEd (trained teachers degree) do not have any jobs. Government should give loans to poor people. (FGD participant, Mutcherla) From central government level, they should give loans to farmers, increase scholarships for children who want to study further, introduce some schemes. The benefits are not reaching the poor person. (FGD participant, Nagaram) The state government should ban wine shops. Due to this, health and family finances are getting spoiled. Alcohol must be banned … because of this, and there are fights at home. They [men] are spending all the money they earn on alcohol. If it is banned, money would be saved, and children can be sent to school. (FGD participant, Mutcherla)
Discussion
Suicide has been recognized as a global public health concern by the WHO whose Comprehensive Mental Health Action Plan 2013–2020 aims for a 10% decrease in the suicide rate by 2020 and to reduce premature mortality by one-third, according to sustainable development goals (WHO, n.d.b). It is estimated that 84% of suicides occur in middle and low-income countries, with India and China contributing to ∼49% of global suicides (Phillips and Cheng 2012). The National Crime Record Bureau (NCRB) of India maintains annual systematic and nationally representative data on suicides in India (National Crime Record Bureau, n.d.). Studies exploring the analysis of NCRB secondary data between 2001 and 2010 (Dandona et al., 2017), 2004 and 2013 (Aggarwal, 2015), and 2001 and 2013 (Arya et al., 2018) showed an increase in the overall suicide rate, a slight increase in male to female suicide ratio (from 1.8 to 2) and a peak of suicide among males in their mid-50s and 60s and females in their mid-20s and 30s. The National Mental Health Survey of India, 2015–2016, reported higher suicidality among women than men, a higher suicide rate among less-educated individuals, widowed or divorced women, individuals residing in urban metropolitan cities, and unemployed individuals (Amudhan et al., 2020). These findings are also reflected in the current qualitative study.
In the current study, alcohol addiction was considered to be the most important factor in facilitating suicide attempts among young males. Alcohol misuse causes a two- to threefold increased risk for workplace, marital and social problems, and a three- to fourfold increased risk of anxiety, depression, and suicidality (Nadkarni et al., 2016). At primary health centers in Goa, the introduction of CAP (counseling for alcohol problems), a brief psychological treatment for alcohol users focusing on the development of problem-solving skills, drink refusal skills, and handling peer pressure or a difficult situation, has shown significant remission and an abstinence from alcohol (Nadkarni et al., 2017). Hence, alcohol cessation interventions could also be incorporated and tested in other parts of India with high levels of alcohol dependency among males.
The Indian population is stratified into tribal and non-tribal populations; tribal populations are involved in traditional hunting, gathering, foraging, and seasonal agriculture for their livelihoods, whereas non-tribal populations are socially stratified based on occupation. The SCs and STs are officially designated as the historically disadvantaged people of India, constituting 16.6% and 8.6% of the Indian population, respectively (Ministry of Tribal Affairs Government of India, n.d.). In the current study, participants reported a predominance of suicide in SC and ST residents of their village. This observation was also made by Singh et al. (2013), who reported higher suicide attempts among the Idu Mishmi tribal population than the urban population of Arunachal Pradesh, and a retrospective analysis of NCRB 2014–2015 data by Arya et al. (2019) reported a higher suicide rate among ST/ Other Backward Classes (OBC) populations than the general population for the southern states.
FGD participants also identified bereaved family members as vulnerable to suicidality because of sudden financial crises, unsettled loans, and emotional turmoil. A recent meta-analysis illustrated that exposure to suicidal behavior leads to a threefold increase in the risk of suicide among bereaved family members, friends, and acquaintances (Hill et al., 2020). Interventions such as the family bereavement program that promote and strengthen adaptive skills and coping mechanisms among bereaved parents and children promote fewer mental health problems (Sandler et al., 2018) and could also be initiated in the Indian context.
Most of the suicides in the current study were reported among housewives, self-employed farmers, and agricultural laborers. However, the study's findings should be interpreted with caution because of the limited sampling conducted. Dandona et al. (2017) analyzed National Crime Records Bureau data spanning 2001–2010 to study suicide trends in India. They found stable national suicide rates, with higher rates in more developed states. Housewives showed the highest suicide rates due to personal and social issues, often by poisoning. Aggarwal (2015) reviewed a decade of data (2004–2013), highlighting youth as being at a high risk of suicide, often using hanging or pesticides, linked to social and economic factors like alcohol, unemployment, and poverty. Arya et al. (2019) focused on 2014–2015 data across religious and caste groups, noting higher rates among Christians and other religious groups than among Hindus, and among general populations compared with SC, ST, and OBC groups in India. Marriage is believed to be protective against suicide because it provides emotional and financial stability in one's life (Kyung-Sook et al., 2018). However, among young Asian women, being married is not necessarily a protective factor because of psychosocial stressors, including arranged marriages, early age at marriage, young motherhood, domestic violence, and economic dependence on the husband (Vijayakumar, 2018). Past literature has reported an approximately twofold increased risk of suicide among farmers and agricultural laborers within the various occupation groups. This could be due to work-related access to a means of suicide (pesticide), harmful exposure to toxins, and psychosocial working conditions, e.g., long working hours, physically demanding work, and occupational stress due to capricious weather conditions (Milner et al., 2013; Klingelschmidt et al., 2018).In the Indian context, suicides by farmers are prompted predominantly by indebtedness, decreased agricultural investment and irrigation improvement, the production of cash crops, increased use of noninstructional credit sources, and reduced trade barriers (Merriott, 2016).
Nationally, the leading method of suicide is poisoning with agrochemicals or a medication overdose, followed by hanging, self-immolation, drowning and jumping from a moving train or vehicle (Dandona et al., 2017), which is similar to the observations of the current study. A recent study exploring method-specific suicide rates between 2001 and 2014 found a decline in rates of suicide by pesticide poisoning with an increase in hanging (Arya et al., 2019; Dandona et al., 2017). However, pesticide self-poisoning is still of significant concern because it accounts for 30% of suicides globally and 20% of suicides in Southeast Asia (Gunnell et al., 2017). Because of this, the WHO launched the Global Pesticide and Health Initiative, which recommends formulating a new pesticide policy, conducting epidemiological surveillance, developing programs to minimize pesticide self-poisoning, and medical management of pesticide self-poisoning (WHO, n.d.b). Further, promising approaches to curtailing pesticide suicide mortality include the withdrawal of more toxic pesticides (Zalsman et al., 2016)., the introduction of communal storage centers (Zalsman et al., 2016), and the identification of high-risk customers by providing training to pesticide vendors (Weerasinghe et al., 2018).
Psychological autopsy studies have reported lifestyle and behavioral changes before the suicidal act (González-Castro et al., 2016). Close family members and peers can play a vital role in suicide prevention by identifying red flags, deviant lifestyle habits, and behavioral changes before a suicide attempt and providing psychosocial support (Ivbijaro et al., 2019). In addition, promoting resilience through engagement in leisure activities, and following up suicide attempters after hospital discharge could potentially reduce suicide (Ivbijaro et al., 2019). Coping strategies are protective risk factors for suicidal behavior. Studies have shown that negative coping strategies such as confronting, distancing, and escape avoidance are higher among suicide attempters (Mathew & Nanoo, 2013). Religious coping is associated with traditional notions of relying on God, divinity, or a higher power to deal with stressful life events. A study in India found lower suicidal ideation and fewer attempts among psychiatric patients having higher religiosity (Gupta et al., 2011).
Some of the best-supported suicide-prevention strategies in lower and middle-income countries include restricting access to the method, introducing mental health and alcohol policies, early identification and treatment, training health workers, and follow-up care and community support (Fleischmann et al., 2016). In the Indian context, various implementation programs have been introduced to control and reduce the burden of suicide. The SPIRIT trial (in progress) introduced in the state of Gujarat is aimed at evaluating the implementation, effectiveness, and cost of the three integrated interventions: school-based intervention (a Youth Aware of Mental Health program, communal storage facilities, and community health worker training) (Pathare et al., 2020). In Vidarbha, Maharashtra, a grassroots community-based mental health program, VISHRAM (Vidarbha Stress and Health Program), focused on suicide risk factors, such as depression and alcohol, showed higher mental health literacy and a decline in suicide rate from 5.2% at baseline to 2.5% 18 months after intervention (Shidhaye et al., 2017).
Conclusion
This study provides a snapshot of suicidal behavior in rural Warangal, Telangana, India. One of the main objectives of the study was to suggest potential targets for initiatives to reduce the suicide burden in the study area. These initiatives could be introduced at the levels of households and communities. At the household level, livelihood strategies and stable economic opportunities for females (beedi making, tailoring, or a cottage industry) and males (skill-based jobs) can ensure a steady flow of income throughout the year. At the community level, measures can include restricting the sale of alcohol, the regulation of pesticide sales (by issuing permit cards to farmers), and providing communal pesticide storage facilities to limit accessibility. Mental health training and counseling can also be provided at the household and community levels. At the household level, training can be provided to identify suicide risk, lifestyle, or behavioral changes, and there could be repeated follow-up with the families of suicide attempters (either by telephone or in-person) by health workers. At the community level, regular meetings can be organized to address villagers’ problems. The government should also help various occupation groups to form authorized unions and support them financially so that the family members of suicide decedents could receive some financial aid. These initiatives could help reduce the suicide burden in the study area.
Footnotes
Acknowledgements
The authors are extremely thankful to Professor V. Ramachandran of the Department of Psychology, Kakatiya University, Telangana, for his local assistance during the study tenure. We especially thank all the respondents for their most valuable feedback during the group discussions and in-depth interviews.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors are thankful Indian Council for Social science research (ICSSR) (F.No. 02/270/2016-17/RP) for providing financial assistance in fieldwork and data collection.