
Abstract
This qualitative study explores barriers to accessing treatment for Major Depressive Disorder (MDD) among Latino adults in the United States, with a novel focus on how these barriers were described based on participants’ preferred language. Fifty Latino individuals (n = 24 primarily Spanish-speaking; n = 26 primarily English-speaking) participated in Zoom interviews and completed a demographic survey and the Patient Health Questionnaire-9 (PHQ-9) MDD self-report measure in their preferred language. Thematic analysis of interview data identified barriers across three levels: individual (e.g., stigma, service literacy, treatment readiness, caretaking responsibilities), provider (e.g., language barriers, cultural humility, perceived care quality), and clinic (e.g., cost, time constraints, waitlists, geographical access). While many challenges were shared across groups, key differences emerged. Spanish-speaking participants emphasized the importance of bilingual providers and described feelings of mistrust, communication fears, and concerns about emotional safety when language concordance was absent. English-speaking participants described prioritizing working with bicultural providers who demonstrated cultural humility and a nuanced understanding of possible intergenerational and structural stressors. Structural barriers, such as cost and scheduling, were often compounded by emotional experiences such as shame and mistrust, underscoring the need for both system-level and culturally responsive solutions. These findings reinforce the need for equity-informed strategies that attend to the intersection of language, culture, and structural barriers to MDD treatment.
Introduction
Disparities in the diagnosis and treatment of Major Depressive Disorder (MDD) persist among Latino populations in the United States (Estrada-Martínez et al., 2019). Within this linguistically and culturally heterogeneous population, variation in English-language proficiency and language preference has been correlated with differences in healthcare access. The Institute of Medicine (Nelson, 2002) has underscored the link between language proficiency and treatment utilization trends, revealing disparities in MDD treatment between Spanish-speaking and English-speaking Latinos. Despite efforts to address structural barriers, such as cost, Spanish-speaking Latinos often report lower treatment satisfaction and receive lower quality of care compared to their English-speaking counterparts (Hsueh et al., 2021; Ramírez García, 2012).
Government institutions and professional associations have recognized these health disparities, advocating for research and action to address treatment access barriers. For instance, the U.S. Surgeon General released a report on mental health, culture, race, and ethnicity (2001), which highlighted the lower healthcare utilization rates among Latinos and emphasized the need for research on treatment access barriers. Mental health organizations, including the American Psychological Association, have echoed these calls to action, stressing psychology's role in addressing health inequities directly (Holden et al., 2023). The United States Preventative Services Task Force recommends MDD screening in the general adult population when adequate systems ensure accuracy and appropriate follow-up (Siu et al., 2016; USPTF, 2023), utilizing tools such as the Patient Health Questionnaire-9 (PHQ-9) (Kroenke et al., 2001), available in English and Spanish (Harry et al., 2021).
Research examining barriers to mental health care access for Latino individuals has identified barriers at multiple levels: client, provider, and clinic (Coombs et al., 2021). Client-level barriers include limited health literacy, perceptions of service necessity, and stigma surrounding mental health care within the Latino community (Andrade et al., 2014; Bauer et al., 2010). Provider-level challenges revolve around varying levels of cultural humility and the scarcity of bilingual practitioners (Grieb et al., 2023; Moreno & Morales, 2010; Soto et al., 2011). Clinic-related obstacles include geographical distance and restricted operating hours (Coombs et al., 2021). Qualitative research has deepened our understanding of barriers impacting mental health treatment access within the Latino community, yet a comprehensive exploration of barriers stratified by English-language preference remains crucial.
Given the national concern within the United States surrounding barriers to depression treatment, practical intervention efforts informed by community voices are urgently needed. Awareness of these barriers and client-proposed solutions can inform interventions aimed at improving equity in mental health service access. This study addresses this imperative by identifying barriers to accessing MDD treatment among Latinos in the United States, focusing on those primarily speaking Spanish or English. Through in-depth interviews conducted within the United States, this research aimed to capture diverse perspectives within the Latino community, contributing to broader health disparity initiatives and efforts to reduce mental health care access gaps.
Methods
Participants
Eligibility criteria for participation included being 18 years or older, self-identifying as Latino, speaking either English or Spanish, willingness to complete a Zoom interview in their preferred language, and residing in the continental United States at the time of the interview. Ethnic or racial identity was not predefined in recruitment materials; however, participants were asked to identify as Hispanic, Latino/a/e/x, or none of these during enrollment. Additionally, participants were asked to choose one or more races they identified with. All participants were willing to discuss their perceptions of accessing care for depression, irrespective of formal diagnosis or history of MDD. Table 1 displays participants’ racial identification.
Participant racial identification.
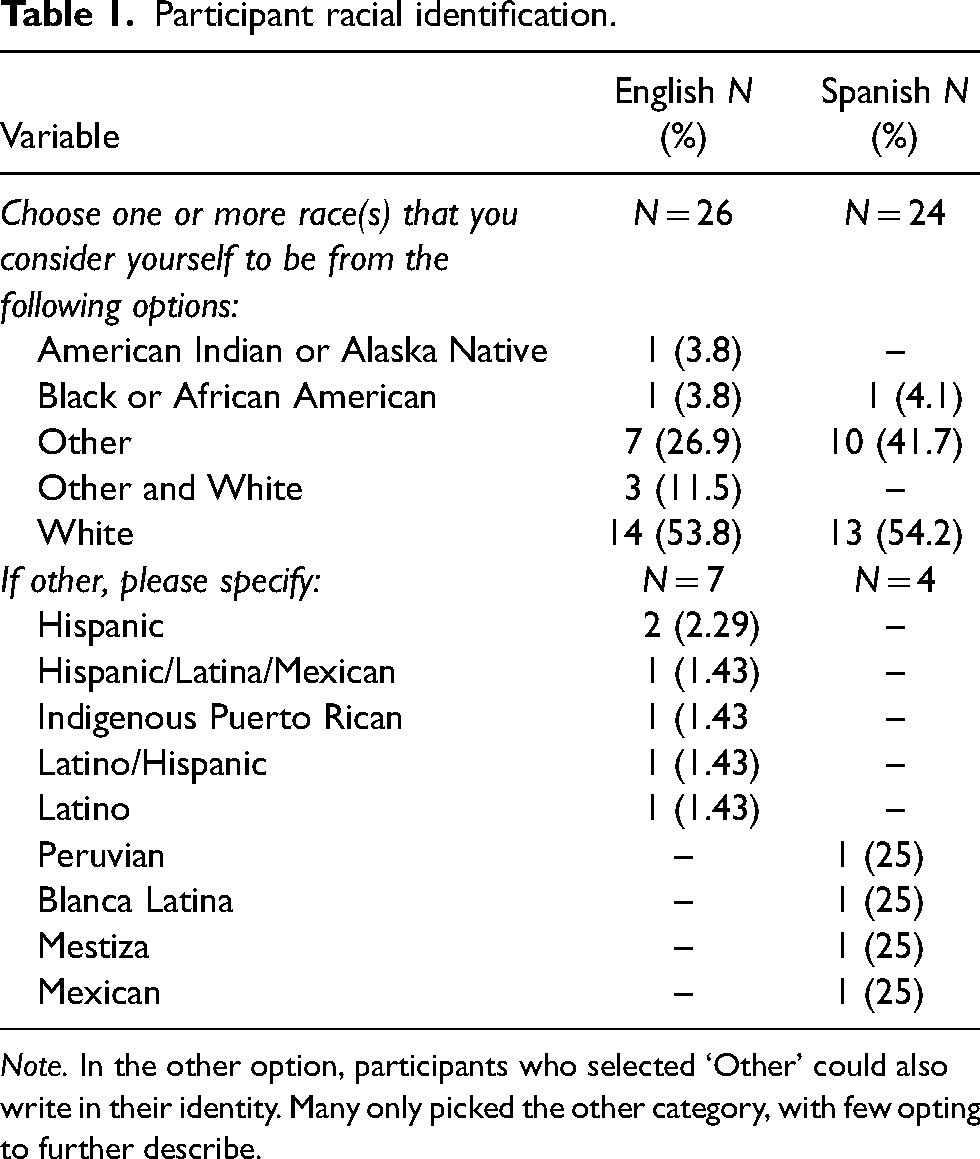
Note. In the other option, participants who selected ‘Other’ could also write in their identity. Many only picked the other category, with few opting to further describe.
Recruitment procedure
Participants were recruited using bilingual English-Spanish flyers containing a QR code. These flyers provided detailed information and compensation details. Fifty participants were recruited through word of mouth (n = 28; 56.0%), social media (n = 16; 32.0%), or flyers (n = 6; 12.0%). All study procedures were approved by the University of Arkansas Institutional Review Board (Protocol #: 2112375993
Interviews
Participants who expressed interest in the study filled out an electronic HIPAA-compliant consent form upon enrollment. Subsequently, they received further details about the study, including informed consent, confidentiality, the rationale for audio/video Zoom recording, and compensation (USD $10 Amazon gift card upon completion) via email and phone from the first author. Interviews were conducted from May to December 2022, each lasting approximately 60 min until data saturation was achieved. The interview questions focused on defining MDD, identifying barriers to MDD treatment, and discussing preferences for MDD treatment in that order. This manuscript presents findings specifically related to barriers to MDD treatment.
Interview
Identifying barriers to MDD treatment was guided by the following questions:
“Have you ever experienced depression?” If yes, “Have you sought care for depression in the United States or abroad?” If yes, “How many times have you experienced depression?” “If you experienced depression or were to experience depression, what barriers have hindered or would hinder you from seeking help?” “What provider characteristics are or would be important to you?”
Interviewer characteristics
Both interviewers are female. The first author, a US-born Latina-American, is fluent in written and oral Spanish and English. At the time, she held a master's degree in psychology and was completing her final year of a clinical psychology PhD program. Her research focuses on addressing treatment barriers for Latinos and other underserved populations. The second author is fluent in written and oral English. She is fluent in written Spanish. At the time, she was a senior majoring in journalism and was interested in public health. The first author had prior qualitative experience and received a refresher qualitative training from the final author, developed questions based on literature, and pilot-tested them with community members. The first and last author also trained the second author in qualitative coding. The authors followed the COREQ guidelines (Tong et al., 2007) for qualitative research reporting.
Reflexivity
The interviewers’ personal and professional identities may have influenced rapport with participants. The research team offered technical assistance downloading the Zoom app, potentially enhancing participant engagement. Interviewers conducted post-interview debriefing and reflection sessions with one another, ensuring rapport and interview quality. Audio and transcript reviews, conducted by the last author,suggested that participants were open and appreciated the opportunity to share experiences.
Measures
Demographics
Table 2 presents the demographic information provided by participants, further informing researchers of the similarities and differences between the sampled groups.
Demographics and scores by participants’ preferred language.
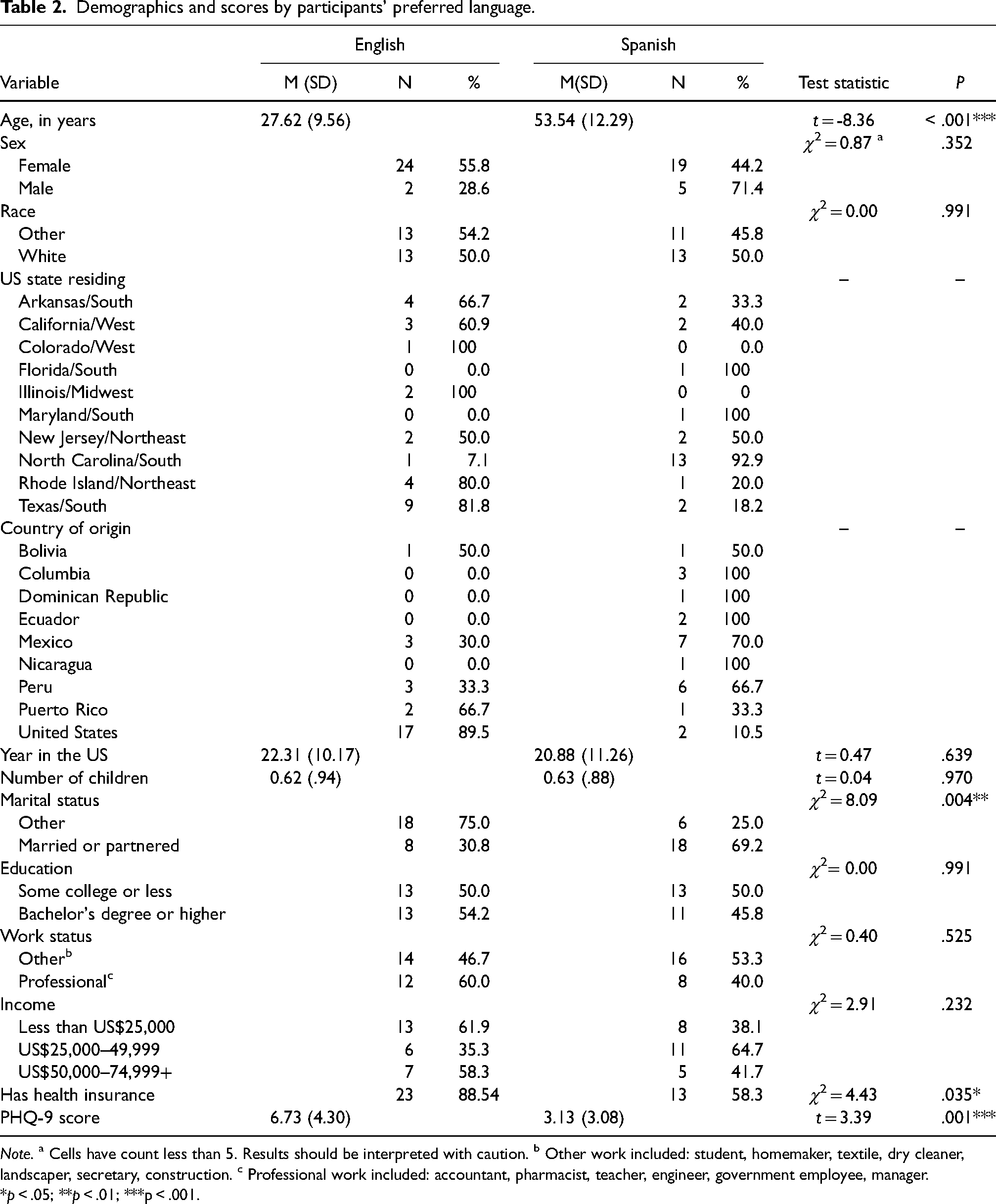
Note. a Cells have count less than 5. Results should be interpreted with caution. b Other work included: student, homemaker, textile, dry cleaner, landscaper, secretary, construction. c Professional work included: accountant, pharmacist, teacher, engineer, government employee, manager. *p < .05; **p < .01; ***p < .001.
Depression symptoms
Depression symptoms were assessed using the Patient Health Questionnaire-9 (PHQ-9; Kroenke et al., 2001), a 9-item self-report measure. Participants rated each item on a 4-point scale from 0 to 3, reflecting the frequency of symptoms experienced. Total scores ranged from 0 to 27, with specific ranges indicating varying MDD symptoms. A score of ≥ 10 indicated potential MDD (Kroenke et al., 2001). The PHQ-9, available in both English and Spanish, was chosen for its cost-effectiveness, reliability, and validity in clinical practice. It is the measure that the United States Preventative Services Task Force recommends for screening (Siu et al., 2016; USPTF, 2023). The internal consistency of the PHQ-9 was acceptable, with Cronbach alpha coefficients of .80 for Spanish-speakers and .77 for English-speakers.
Study procedure
Participants completed the demographic questionnaire and PHQ-9 (Kroenke et al., 2001) screener before engaging in the qualitative interview. Following the interview, participants were debriefed on the study. At the debriefing, all participants were given a list of mental health resources tailored to their geographical area. None of the participants endorsed suicidality during the study. However, the study procedure included protocols to assess and address risk, such as halting the research study, discussing needs further, and connecting participants with appropriate services if necessary.
Community responsiveness
The first author engaged in community responsiveness efforts in line with the Kilbourne et al. (2006) health disparities research framework. After collecting data, the first author shared preliminary descriptive results and qualitative findings with two known Latino community organizations, El Futuro Inc. and Progreso Latino Inc., for their feedback. The responses from the community organizations were positive, with no points needing clarification. Community partners affirmed that the findings reflected barriers and facilitators they observe in practice and emphasized the importance of sustaining community–academic collaborations in future research.
Data analysis of qualitative interviews
Qualitative interviews were analyzed using Braun and Clarke's (2022) reflective post-positivist deductive thematic analysis guidelines to elucidate barriers and preferences in seeking help for MDD treatment among Latino adults. The research team executed six sequential steps in this analysis. The first step entailed immersing in the data to gain a profound understanding. Most interviews (n = 44; 88%) were conducted by the first author, supplemented by audio recordings of interviews conducted by the second author (n = 6; 12%), all transcribed verbatim in their original language. The first author noted exemplary quotes observed during transcription, while the second author listened to all audio recordings, which she did not conduct. Next, a list of initial codes was generated to identify crucial points raised by participants in response to qualitative questions relevant to their language group. The second author conducted accuracy checks of all transcripts after the first author reviewed and redacted identifying information from the transcriptions. The first author shared her coded transcripts with the second author, initiating discussions on response patterns based on language groups. In the third step, the coding was shared with the last author to ensure alignment with the data, leading to the development of potential themes specific to each language group. Synthesizing language group themes in the fourth step facilitated the exploration of commonalities and disparities, culminating in identifying overarching themes. These themes were further consolidated into three categories in the fifth step: individual, provider, and clinic. Finally, the themes were articulated and disseminated in the last step to communicate the findings effectively, and reviewed by the remaining authors and community organizations.
Results
Sample characteristics
A total of N = 50 participants aged 19–79 years (M = 40.06, SD = 16.99), with n = 43 (86%) identifying as female, n = 31(62%) foreign-born, and n = 24 (48%) primarily Spanish-speaking, completed the study. All Spanish-speaking participants identified as immigrants, with an average of M = 20.88 (SD = 11.26) years residing in the United States. No missing data were observed.
Depression symptoms and past help-seeking
PHQ-9 depression screening scores (Kroenke et al., 2001) were tabulated using SPSS Version 28.9.1.9 (Varghese et al., 2023) for participants self-identifying as either English- (n = 24; M = 6.73; SD = 4.30) or Spanish-speaking (M = 3.13; SD = 3.08) Latinos. Consistent with previous literature (Grieb et al., 2023), immigrant Spanish-speaking Latinos endorsed current depressive symptoms at lower rates than their English-speaking counterparts. Spanish-speaking participants reported experiencing more depressive episodes (M = 5.14) compared to their English-speaking counterparts (M = 2.67). However, English speakers (n = 13; 50%) were more likely than Spanish speakers (n = 4; 13%) to have ever consulted a mental health therapist for depression, despite being younger (M = 27.62; SD = 9.56 compared to M = 53.54; SD = 12.29). Additionally, English speakers (n = 23; 88.54%) reported higher insurance coverage rates than Spanish speakers (n = 13; 58.3%). Figure 1 depicts PHQ-9 depression severity based on language group membership.
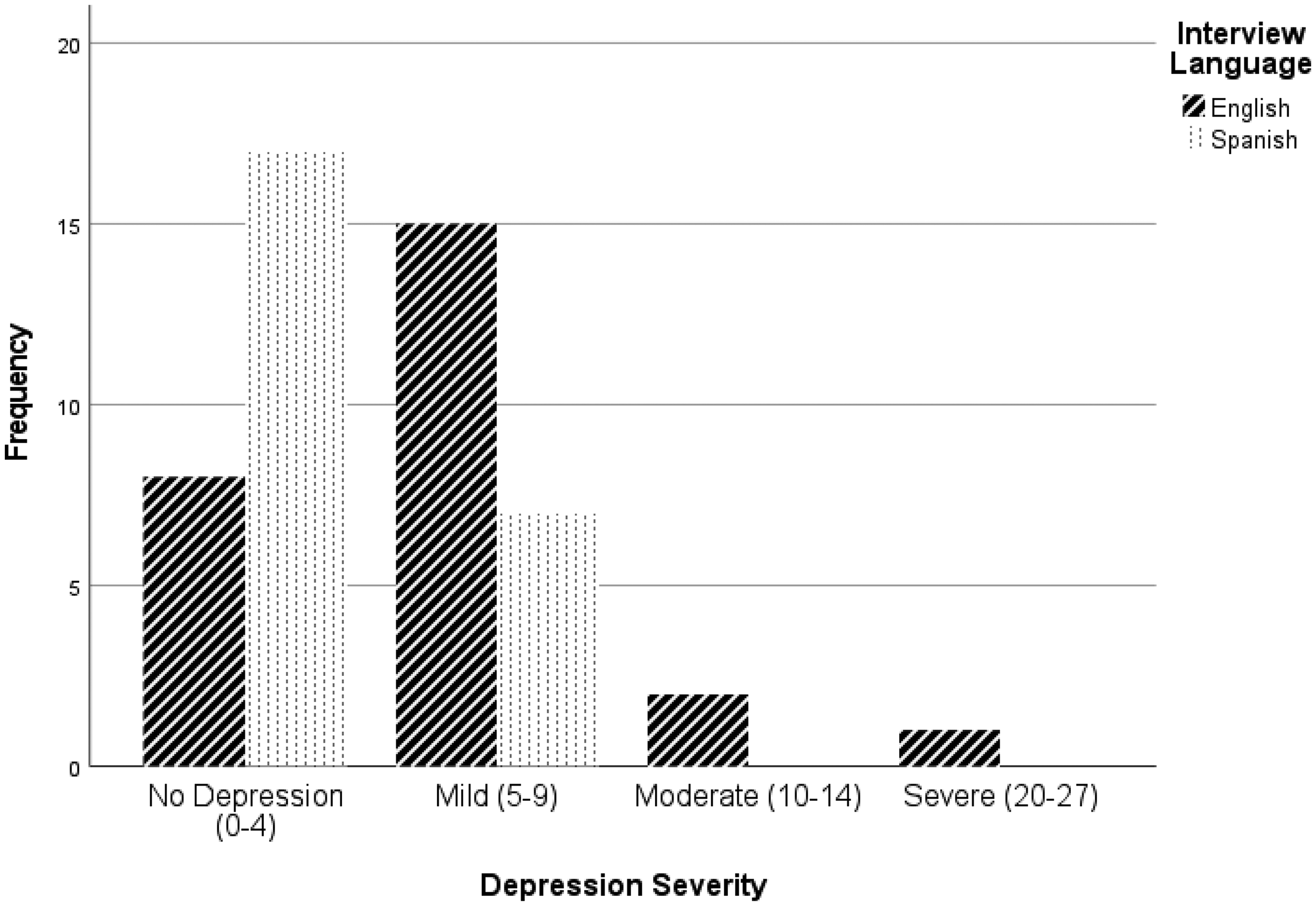
PHQ-9 depression severity based on language group membership.
Qualitative findings
Client-level barriers
In our examination of treatment barriers for MDD, participant interviews revealed a range of barriers at the client-level. These encompass stigma, service literacy, readiness to seek treatment, and caretaking responsibilities. Similarities between both language groups are provided below. Table 3 presents qualitative findings organized by themes.
Themes informed by qualitative findings.
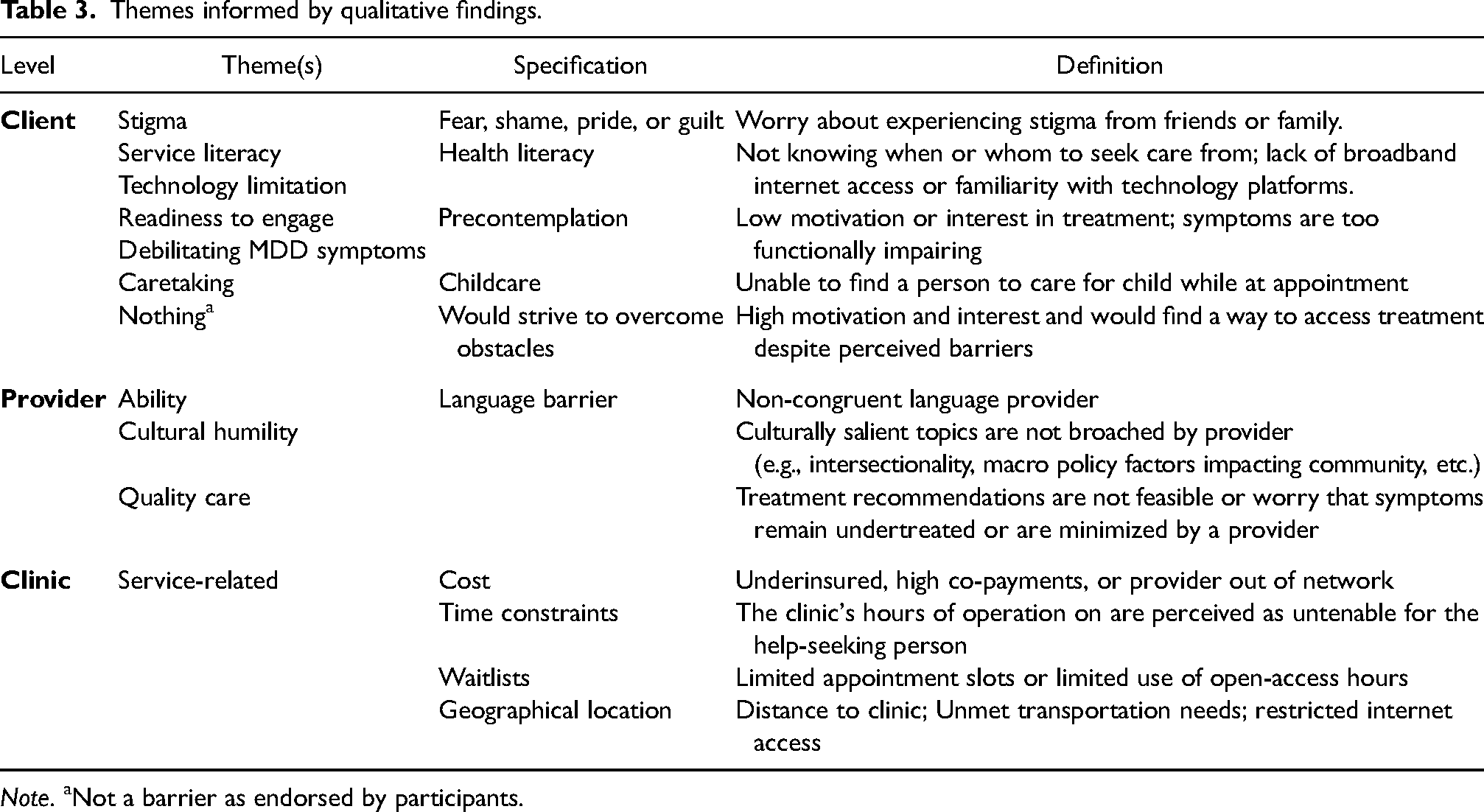
Note. aNot a barrier as endorsed by participants.
Stigma
Stigma surrounding mental health was a significantly discussed barrier among participants, often shaped by cultural attitudes and family dynamics. Many participants described shame, fear, or judgment as major obstacles to seeking care for depression. For instance, anEnglish-speaking participant shared her observations of how cultural stigma in some Latino families may deter someone from acknowledging or addressing a mental health issue: “I do have a lot of people in my life who I see don’t get the help that they need, just because certain Latino families don’t see it as a problem, or it is not seen as a problem.”
Another participant emphasized how shame and a lack of trust can make it difficult to disclose mental health struggles, particularly when support systems are not perceived as emotionally safe: “For depression, a few friends have called and asked me questions, just seeking help. It is hard to find someone you can trust. There is so much shame and embarrassment in admitting you need help. Those who face it [the shame] get help, while those who don’t don't."
For another participant, the barrier was rooted in the fear of being emotionally invalidated or harshly judged by family members. She recounted an experience of opening up about her depression only to feel dismissed: “I think fear of being told [by family] that … like … people telling you that you are not depressed or you don’t know what depression feels like or other I guess people telling you that … like I have heard people say … don’t be sad … as if that would make it go away. Things like that would be an obstacle to asking for help. Just the fear of being like … I don't know if I am using the word correctly, but I was rebuked by my family for telling them that I had depression. Maybe even opening up to them and telling them how you feel is an obstacle. It is just too scary.”
Among Spanish-speaking participants, stigma was similarly present but often expressed through feelings of vergüenza (embarrassment). One participant candidly shared his internal conflict about seeking help: “Es embarazoso buscar ayuda. Uno se pregunta qué pasará si su familia se entera de que está luchando.” [It's embarrassing to seek help. You wonder what will happen if your family knows you are struggling.]
Together, these narratives illustrate how stigma may operate not only as a personal feeling but also as a social process shaped by intergenerational expectations, family loyalty, and community norms. They underscore the need for culturally responsive outreach and education efforts aimed at destigmatizing depression within communities.
Service literacy
Another barrier identified by participants was limited service literacy, which encompassed a lack of knowledge about available mental health services, how to access them, and what the treatment process entails. This barrier often intersected with participants’ language preference, level of education, and familiarity with the healthcare system. One English-speaking participant described uncertainty about where to start if she were to seek help for depression. Her lack of exposure to available services left her unsure of what treatment even entailed: “I think I have depression, but I don’t know any of the treatments or where I would go for care. Maybe I would see my primary care doctor first. Perhaps they could give me a referral or guidance on where to start.”
A Spanish-speaking participant shared how limited technological literacy and poor video quality on his mobile phone made telehealth particularly challenging, further reducing his comfort level with accessing services remotely: “Es más fácil hablar con una persona frente a usted que por teléfono porque puede leer sus respuestas, como sus expresiones faciales y su lenguaje corporal, y a veces la imagen del video no es buena [en mi teléfono] y no siempre puedo arreglarla.” [It is easier to talk to a person in front of you than over the phone because you can read their responses, like their facial expressions and their body language. Sometimes the video image is not great [on my phone] and I can’t always fix it.]
Together, these quotes demonstrate how service literacy extends beyond knowing that treatment exists; it also involves understanding how to navigate the system, interpret health-related information, and use available platforms (like telehealth) with confidence. For some, the complexity of the system itself is a deterrent to seeking care.
Readiness to seek treatment
Readiness to seek treatment was shaped not only by attitudes toward care but also by the emotional and functional effects of MDD. Some participants expressed ambivalence or hesitation around engaging with treatment, particularly when symptoms felt overwhelming or when motivation was low. One participant noted how the very nature of depression, its ability to sap energy, interest, and hope, can itself become a barrier to help-seeking: “Depression itself [is a barrier]. If I am really depressed, I don’t think I am going to listen to the radio or music, read, spend time with family or friends, or much less have the energy to seek help.”
Caretaking responsibilities
Caretaking responsibilities, especially for children, were a commonly cited barrier to accessing mental health treatment. Participants described difficulty balancing their roles as caregivers with their own emotional needs, often prioritizing family obligations over personal health. One participant explained how parenting duties could interfere with attending or even initiating therapy. Without adequate childcare support, she felt that engaging in treatment would be nearly impossible: “My kids interrupt. If my kids are acting up at the same time I’m seeking help, I wouldn’t have anyone to look after them and I might not be able to engage in therapy.”
Summary of client-level barriers
These findings underscore the complex interplay of cultural, social, and personal factors influencing help-seeking behaviors and access to MDD treatment within a Latino community. Addressing these barriers necessitates culturally informed and tailored interventions aimed at promoting mental health literacy, reducing stigma, and facilitating access to care.
Provider-level barriers
Effective mental health treatment requires providers who strive to navigate cultural nuances, language preferences, and treatment modalities tailored to individual needs within the heterogeneous Latino community. This section explores the provider-level barriers identified in the study, encompassing language barriers, cultural humility, and perceptions of quality care.
Language barrier
Language concordance between provider and patient was identified as a core component of treatment accessibility, especially for Spanish-speaking participants. Many emphasized that the ability to communicate in one's native language was essential to establishing trust, expressing emotions, and understanding treatment recommendations. One participant, a Spanish speaker with some English language proficiency, explained that even minimal misunderstandings in health contexts can be serious. She expressed a strong preference for fully Spanish-language interactions with her provider to avoid any potential communication errors: “Aunque hablo un poco y entiendo inglés, prefiero que ella [la proveedora] hable español para que no haya ‘malentendidos’. Para la salud, prefiero el español al cien por ciento para que no haya un malentendido. Y que toda la información [escrita] se proporcione en ambos idiomas.” [Although I speak a little and understand English, I prefer she [the provider] speak Spanish so that there are no misunderstandings. For health, I prefer 100% Spanish so that there is not a misunderstanding. And that all [written] information be provided in both [Spanish and English] languages.]
Another participant shared that her preference for Spanish language services was rooted in the ability to articulate her emotions and ideas fully. Even when she could “get by” in English, she felt most empowered when communicating in her native language: “Preferiblemente, sería completamente en español para poder expresarme. Porque es mi idioma y el que mejor puedo comunicarme. Para una buena comunicación, prefiero el español … Quiero un proveedor que hable español porque es más empoderador poder compartir tus ideas o emociones directamente que depender de un intérprete.” [Preferably, it would be entirely in Spanish so I can express myself. Because it is my language and the one I can communicate in best. For good communication, I do prefer Spanish … I want a provider who speaks Spanish because it's more empowering if you get to share your ideas or emotions directly than relying on an interpreter.]
Meanwhile, English-speaking participants did not emphasize bilingualism as much as bicultural competence. One participant, while fluent in English, described how providers who acknowledged cultural differences and tailored their communication built more trust and relevance into treatment: “Offering information in bilingual methods helps a lot [with building trust]. That is one way more information can get across. I think [the provider] is adapting to the fact that it might look different. That people who are suffering from depression might be because of different things … first generation living in an immigrant household. Their parents growing up [abroad]. A unique dynamic in the household. Depression is very taboo in some Latino communities. Trying to navigate that with empathy and carefully. I know there can be a lot of distrust for healthcare professionals. There is a lot of reasonable distrust.”
Taken together, these quotes illustrate that linguistic proficiency is not just a practical asset; it is a relational and ethical imperative in the treatment of Latino clients. Spanish-speaking participants often viewed language concordance as a prerequisite for trust, while English-speaking Latinos emphasized cultural understanding and empathy. These differences underscore the need for a bilingual and bicultural workforce that is sensitive to how language preference intersects with identity, power, and safety in clinical care.
Cultural humility
Participants across both language groups emphasized the importance of cultural humility in their providers. This went beyond cultural awareness or shared identity; participants described a need for providers who demonstrated a willingness to understand complex cultural, immigration-related, and family dynamics without making assumptions or minimizing lived experiences. One English-speaking participant reflected on how family obligations and cultural norms can influence treatment decisions, noting that providers often overlook these layered dynamics: “You’d rather NOT sacrifice that peace between them [family] to keep your family ties stable … There are very few providers who are Hispanic/Latino, I’d say, and paying attention to family dynamics is important. When one's depressed, and family is very important to them, it can add another layer of burden.”
Another participant described a past experience with a provider who failed to understand her intersecting identities as a Latina immigrant. This disconnect left her feeling unseen and misunderstood, reinforcing her skepticism toward care: “I would want to be assessed and treated by a provider who had experience working with immigrants, particularly Latino immigrants, because of the fact that I am an immigrant myself, and have parents who are immigrants, and work with the Latino immigrant community. [The provider] does not have to be bilingual, but it would be wonderful if they were. And I would definitely look for– I would want to ensure that [the provider] is culturally competent, to provide that care. It's having knowledge, both in terms of that community but also in areas that impact that community in particular. Having knowledge of concepts of marianismo, machismo, immigration, the impact of that experience on an individual on a community. And then, competency also about the intersections of race, ethnicity, education, and income. As immigrants, we have our culture from that home, and we have two cultures that we’re dealing with. I would want someone to have that experience. When you asked me earlier, about having been diagnosed, I struggled the first time decades ago. I was sent for an evaluation when I went to go see a counselor at the school, but I was very turned off because I was sent to a white clinician who gave the diagnosis of depression. But when I spoke to the counselor who was a white counselor, you know, I spoke to her afterward. She had no concept of what I was dealing with as a young immigrant student from a very strict Latino family. She just told me, “Well, if you don’t want to go home during the break, then don’t go home.” But I had nowhere else to go. She didn’t understand what I was struggling with with my family. She had no concept of the culture, of the needs of a young adult immigrant in this country. You’re dealing with those two cultures. There's the American culture and your immigrant culture. So, having that competency to understand the experiences of immigrants is important!”
A third participant echoed this theme, describing how even well-meaning providers can miss cultural cues or unintentionally dismiss important aspects of a client's experience: “I feel that something I have encountered with my current therapist is some cultural barriers or some cultural differences that are not as understood. They obviously tried to understand, but that aspect of it would just be easier for like certain issues to make sense or be understood if it were somebody who had that cultural background or open to be familiar with it.”
Collectively, these accounts suggest that cultural humility is not a static skill, but a continuous, relational process. Participants said that they valued providers who are not only informed but who listen deeply, acknowledge systemic barriers, and recognize how cultural identity may shape mental health experiences. Workforce training efforts should consider incorporating these insights by preparing clinicians to engage in ongoing self-reflection and cultural inquiry.
Quality care
Participants in both language groups underscored the importance of receiving quality mental health care, not just in terms of how care is delivered. For many, quality care was defined by the provider's willingness to listen, tailor recommendations, and avoid dismissing the client's concerns or preferences. Spanish-speaking participants, in particular, expressed hesitancy to question providers directly, leading to internal doubts about whether they were receiving appropriate care. One Spanish-speaking participant voiced frustration with providers who appeared disinterested or emotionally disengaged. She described the therapeutic relationship as a kind of “mission” that required full presence and commitment from the clinician: “Creo que muchos proveedores no están interesados en su profesión—en escuchar al cliente, al paciente. Si el proveedor no está cien por ciento comprometido con su profesión, debería retirarse o tomarse unas vacaciones y volver cuando sienta energía y deseo. No llame a lo que hace trabajo porque es una misión. Es más un don … Cuando uno está sufriendo, es como si otros intentaran ver tu dolor con los ojos vendados, y muchas cosas no se ven. Y eso es lo que buscamos: alguien que se tome su tiempo para tratar de entender tu dolor y que con habilidad trate de ayudarte a quitarte esa venda.” [I think many providers are not interested in their profession—in listening to the client, the patient. If the provider is not one hundred percent invested in their profession, they should retire or go on vacation and come back when they feel full of energy and want to. Don’t call what you do work because it is a mission. It's more of a gift … When one is suffering, it's like others try to see your pain while wearing a blindfold, and many things go unseen. And that's what we’re looking for, someone who takes their time to try to understand your pain and will skillfully try to help you take that blindfold off.]
Summary of provider-level barriers
In addition to attunement, participants expressed a desire for practical and respectful treatment recommendations. Some questioned the tendency of providers to default to medication without adequate explanation or exploration of treatment alternatives. Others shared that recommendations often felt “out of touch” with their realities or values. While this was not limited to one language group, Spanish-speaking participants shared that they were less likely to voice these concerns in session, possibly due to power dynamics or a fear of appearing disrespectful. Moreover, participants valued clinicians who could acknowledge hesitation about treatment decisions and work collaboratively. For instance, an English-speaking participant shared that while she trusted her provider, she felt some treatment options weren’t feasible, especially given her financial or caregiving responsibilities. Others noted that a lack of follow-up or feeling rushed undermined their confidence in the provider's care. Taken together, these narratives emphasize that “quality care” is not simply about credentials or treatment protocols, it's about how recommendations are delivered, whether they are feasible, and whether the provider earns the client's trust. Quality care may involve navigating subtle dynamics of respect, shared decision making, and empowerment.
Clinic-level barriers
Accessing mental health care can be hindered by various structural barriers, including cost, time constraints, waitlists, and geographical location. This section examines the clinic-level barriers identified in the study.
Cost
Cost was one of the most frequently cited clinic-level barriers across both English- and Spanish-speaking participants. Even when individuals recognized the value of mental health treatment, concerns about insurance coverage, high co-pays, or out-of-network providers created substantial obstacles to accessing care. One English-speaking participant described the challenges she faced when transitioning off Medicaid and having to navigate private insurance. Her experience reflects a common scenario in which previously accessible services become financially prohibitive: “I would say cost is a big thing. It all depends on health insurance. So before, year [X], I was on Medicaid. So moving forward, again, I’d have to go through the whole spiel of figuring out therapists that take my insurance, so accessibility in terms of cost.”
For participants without insurance or with limited coverage, the perception of mental health services as a financial luxury further reduced their likelihood of seeking treatment. Even a small co-payment was enough to delay or avoid scheduling appointments. Several participants also expressed concern that high costs might be incurred without noticeable benefit, particularly if they were unsure of how many sessions would be needed or whether treatment would “work.” Importantly, cost concerns were not always voiced as the primary barrier but were often mentioned in combination with others, such as time constraints or limited provider availability, which compounded the difficulty of accessing care. Overall, this theme underscored the need for structural interventions that address affordability through expanded insurance coverage, transparent billing practices, and access to low-cost or sliding-scale services. While provider-level improvements (e.g., bilingual, culturally humble care) are essential, they cannot fully address disparities if services remain financially out of reach for many individuals.
Time constraints
Time constraints were another common barrier to accessing mental health care, especially for participants balancing work, school, or caregiving. While both English- and Spanish-speaking participants acknowledged time limitations, the way these constraints were experienced and described differed slightly between groups. An English-speaking participant highlighted how rigid work schedules made it difficult to attend therapy during traditional clinic hours. Her lack of paid leave created a conflict between financial security and self-care: “… it was difficult to find a time that went well with my job … I had no leave time.”
A Spanish-speaking participant similarly expressed difficulty attending sessions due to schedule conflicts, though she framed the issue as one of limited clinic availability rather than her own inflexibility: “Solo mi disponibilidad de tiempo. Sería útil si las clínicas tuvieran horarios más flexibles. Definitivamente iría.” [Only my time availability. It would help if clinics had more flexible hours. I would definitely go]
Taken together, these quotes reflect how time, like cost, is not merely a logistical issue but a structural one. For many individuals, particularly those managing multiple jobs or family obligations, attending care during standard business hours is unrealistic. Clinic policies that prioritize efficiency over accessibility may unintentionally exclude those most in need. Improving access will require not just provider training but also systems-level change, such as open-access scheduling, telehealth flexibility, or drop-in sessions, that meet people where they are.
Waitlists
Long waitlists for mental health services were described as a frustrating and discouraging barrier by participants across language groups. Although interest in seeking care was high, participants reported often feeling disillusioned by the delays between requesting help and receiving it. These lags often led to disengagement, especially for individuals in acute distress or those with limited time and flexibility. One English-speaking participant explained how extended wait times not only delayed care but also created emotional discouragement, making it more difficult to maintain motivation to pursue treatment: “I know that there are many individuals in my position that are on waitlists or that get discouraged.”
For Spanish-speaking participants, waitlists were similarly disheartening but were often compounded by language-based shortages. Some described difficulty finding any Spanish-speaking providers available in their area, let alone ones accepting new clients. Though not every participant explicitly named “waitlist” as the issue, narratives reflected long delays in appointments or gaps in continuity after initial visits. These findings underscore how structural limitations, such as provider shortages, understaffed clinics, or high demand, can stall treatment engagement. While individual motivation or provider quality may be high, access bottlenecks like waitlists remain a point of system failure. Addressing this barrier requires increasing the mental health workforce, particularly linguistically and culturally informed providers, as well as expanding short-term, interim services to bridge patients to care.
Geographical location
Geographical location and limited proximity to mental health clinics were discussed as additional barriers, particularly for participants without reliable transportation or those living in areas with few culturally informed services. Distance was not only a matter of miles; it represented a broader issue of access shaped by neighborhood infrastructure, transportation availability, and regional provider shortages. One English-speaking participant articulated the tension between wanting high-quality care and having limited options nearby. For him, the inconvenience of travel and inconsistency in provider quality were intertwined obstacles: “I would say location and the quality of the provider. There are some really good providers but they are really far away or some of them … they apparently have 4 or 5 stars but they are really not that good.”
Summary of clinic-level barriers
For Spanish-speaking participants, location concerns often intersected with immigration-related fears or limited driving access, though these were sometimes implied rather than explicitly stated. Some shared concerns about traveling unfamiliar routes or needing to rely on others for transportation, factors that could make attending weekly sessions burdensome or inconsistent. These challenges point to a broader issue of service deserts, where high demand for care is not met by local availability, especially in linguistically diverse or immigrant-heavy communities. Addressing geographical barriers may involve expanding telehealth offerings, developing mobile mental health units, or investing in local community-based services with flexible, culturally adapted care. Ultimately, geographical accessibility must be seen not just as a question of physical distance but as one of equity, whether individuals can consistently and comfortably reach services that are relevant, responsive, and rooted in their lived realities.
Discussion
Our study joins others, noting that members of the Latino community may face numerous barriers to accessing needed mental health care for MDD (Anastasia & Bridges, 2015; Coombs et al., 2021). Beyond structural barriers, trust and fear were cited as critical but often overlooked factors influencing treatment engagement. Participants’ fear of disclosure, misinterpretation, or stigma was described as potentially informing their willingness to seek help. Additionally, a lack of trust in providers, particularly when cultural and linguistic concordance was absent, compounded these barriers. Understanding how trust and fear interact in treatment seeking is essential for designing culturally responsive interventions.
Fear of disclosing struggles with MDD is not solely an individual concern but is shaped by historical and systemic inequities in healthcare access for Latino communities (Nelson, 2002). Some participants expressed concern that discussing their MDD symptoms might lead to unwanted consequences, such as being labeled as ‘mentally ill’ or having personal struggles exposed. This fear was particularly pronounced among Spanish-speaking participants who worried about confidentiality breaches or misinterpretations when using interpreters. Given that medical mistrust among Latino communities has been documented in prior research (Hsueh et al., 2021; Moreno & Morales, 2010), addressing these concerns requires not only clearer communication about privacy protections but also systemic efforts to build rapport through trauma-informed and culturally responsive care. Providers should be aware that patients may be reluctant to discuss MDD symptoms. Should any symptom of depression be revealed by a Latino patient, it is critical that the provider not move quickly to dismiss this since it is possible that it took a great deal for that patient to overcome stigma and describe feeling low or sad (Andrade et al., 2014). Instead, small indications of depression should prompt providers to pause and assess more fully what may be happening to the patient, taking care to validate and explore the phenomenological experience the patient is describing. Additionally, when available, healthcare providers might consider working with care navigators and social workers to help patients access resources as needed to help mitigate structural barriers such as internet broadband access and transportation (Kilbourne et al., 2006).
Expanding the linguistic capacity of providers is essential for Spanish-speaking patients. However, even English-speaking Latinos expressed a strong preference for bicultural providers. This preference highlights the importance of understanding ethnic identity, sociocultural stressors, and systemic barriers shaping mental health experiences (Stein & Guzman, 2015; Wallace et al., 2024). Beyond language concordance, fostering trust is a critical yet under-discussed component of improving depression care access (Bridges et al., 2019). Many patients were hesitant to disclose depressive symptoms fully if they did not perceive their providers as trustworthy or culturally aligned. Trust is particularly fragile in initial interactions (Hale et al., 2020) and must be intentionally cultivated by addressing confidentiality concerns early in the clinical relationship, particularly when working with Spanish-speaking individuals. Using motivational interviewing techniques to explore patient concerns rather than assuming resistance can be beneficial. Explicitly acknowledging cultural stressors, such as intergenerational conflict, immigration-related stress, and discrimination, can help shape patients’ perceptions of mental health treatment (Falicov et al., 2021). Finally, ensuring continuity of care is essential, as trust develops through repeated interactions rather than a single visit.
Additionally, bilingual providers and trained interpreters can help mitigate concerns about misinterpretation or lack of understanding of cultural nuances. When bilingual providers are not within reach, trained interpreters can help increase patients’ understanding of provider recommendations (Moreno & Morales, 2010), if done well. Psychotherapy encompasses discussing sociopolitical stressors impacting mood and stress. Among persons with precarious immigration backgrounds, the use of an interpreter might shift the focus away from treatment to worrying about the potential consequences of disclosing information that might impact their immigration status if confidentiality is broken. Thus, if using an interpreter, discussing confidentiality as it relates to the client, clinician, and interpreter is crucial when working with limited English proficiency populations (Fennig & Denov, 2021), especially if services are provided to persons from immigrant communities (Buchanan & Wiklund, 2020). Assessing the quality of interpretive services is essential. Bauer et al. (2010) have documented that disclosing sensitive information in the therapeutic context is slower when interpretation is provided by untrained bilingual staff instead of a trained interpreter. Relatively, in our sample, participants shared that talking about mental health is a sensitive subject, and slower disclosure of presenting concerns is probable with interpreters. This might be for multiple reasons that need further empirical study. Much linguistic complexity exists within Spanish-speaking sub-groups (e.g., accent, dialect, vernacular, cultural idioms). Fears that interpreters would not accurately capture phrases’ emotional intonations and cultural underpinnings are possible among language-brokered recipients.
As with many other studies (Coombs et al., 2021; Costantini et al., 2021), our participants reported numerous structural barriers that interfered with seeking care. These all largely fell into the domain of “limited accessibility.” For instance, lacking insurance or the perceived high cost of services were significant barriers to care. Similarly, geographical distance from clinics limited accessibility. These are difficult to change rapidly but speak to ongoing needs to promote equitable health policies and reimbursement practices that make services more affordable. In addition, telehealth and mobile clinics can help bridge geographical divides (Hilty et al., 2020). More within the control of a clinic is addressing barriers to care, such as long waitlists and limited availability. Some clinics have begun using walk-in times rather than scheduling follow-up appointments to utilize providers better (Kalb et al., 2022). Others have considered opening later to allow for later closing times without extending the day or requiring additional staff (Tulimiero et al., 2021).
Ultimately, a multipronged approach will be needed to continue ensuring Latinos residing in the U.S. receive timely access to quality depression care. Our participants were enthusiastic about treatment but faced diverse barriers (client/internal, provider/interpersonal, and clinic/structural). Enhancing health equity involves attending to factors that reduce the burden of a disease (Kilbourne et al., 2006). To reduce the burden of depression in Latinos and thus improve health equity, clinics should attend to these myriad factors.
Workforce training recommendations
Less than 11% of psychologists can provide services in non-English languages (Hamp et al., 2016), suggesting that the mental health workforce cannot meet the demand for providers who can give services in languages other than English, and interpreters fill this gap. Regarding increasing the number of culturally and linguistically diverse psychologists that are part of the global majority reflecting the diversifying population in the U.S., this could be done by studying and addressing trainee and practitioner barriers. Regarding trainees, concerns about retaining recruited minorized groups that experience systemic and structural racism in doctoral programs are increasing (Windsor et al., 2021). The American Psychological Association provides recommendations for the field to address disparities in recruitment and retention and transform curricula in training programs to address systemic barriers (Holden et al., 2023). Regarding current practitioners, discomfort regarding addressing issues of racism in clinical practice abounds (Buchanan & Wiklund, 2020), suggesting that learning about and practicing cultural humility is a lifelong process requiring continual attention. Additionally, several experiential training programs exist for working with Spanish-speaking populations. One such program is PASEO (www.paseoprogram.com), a cultural and Spanish-language immersion program open to trainees and professionals in psychology and related fields.
Study strengths
Recent efforts have focused on identifying and better understanding specific barriers to accessing culturally responsive, evidence-based treatments for immigrant populations (Holden et al., 2023). This study adds to the literature by focusing on the differential endorsement of barriers examined by an English- or Spanish-preferred language community sample, expanding our knowledge gathered from work in geographically limited or college samples (Guzman et al., 2024). Our multipronged recruitment methods (e.g., distribution of flyers, social media, and word of mouth) allowed the recruitment of N = 50 participants who completed quantitative self-report measures and a qualitative interview. In addition to structural barriers commonly described in the literature, such as cost and location of services (Coombs et al., 2021), we offered insight into nuances of individual, provider, and clinic barriers affecting access to MDD treatment from understudied consumer voices and ways that participants think best to address barriers. We ensured the sharing of the findings of these results with participants and community organizations known to serve the Latino community. These findings contribute to the literature on health disparities in accessing MDD treatment and highlight future directions for improving access to culturally responsive depression screening and treatment.
Study limitations
Regarding our sample, we had an uneven proportion of Caribbean (n = 4; 8%), Central (n = 1; 2%), North (n = 29; 58%), and South (n = 16; 32%) American Latino representation, thus not allowing for geographical comparisons (e.g., urban versus rural; enclaved versus not, etc.) of barriers. Males were highly underrepresented in this study; therefore, our understanding of how barriers are endorsed across the sexes is limited. Spanish speakers were, on average, older than English speakers, despite spending the same amount of time within the United States. Thus, differences in barriers might intersect with language preference and age cohort effects. Participants were interviewed once; longitudinal data could help researchers examine how barriers fluctuate over time and across age groups. Lastly, persons comfortable with this data collection involving audio/video recording self-selected to participate. These limitations may impact the generalizability of the findings.
Conclusion
This study provides a more nuanced understanding of the barriers that individuals identifying as Latino may face when seeking treatment for MDD. These findings reinforce previous work on linguistic barriers (Escobedo et al., 2023) but extend the literature by showing how language preference interacts with trust, treatment readiness, and cultural norms around authority and respect. This study revealed intra-group variation that is often obscured in prior research. While structural barriers, such as cost, time, and provider availability, were common across the sample, Spanish-speaking and English-speaking participants described distinct emotional, relational, and systemic factors that influenced how they experienced and navigated those barriers.
Spanish-speaking participants expressed a desire for language-concordant care, often viewing the ability to communicate with a provider in Spanish as a prerequisite for trust and safety. Language mismatch contributed to fears of being misunderstood, particularly when discussing sensitive topics such as immigration, trauma, or family dynamics. Many also voiced reluctance to question provider recommendations due to perceived power differentials, which may impact adherence and disclosure in clinical settings.
In contrast, English-speaking participants, many of whom were U.S. born, were more often concerned with the provider's cultural humility and bicultural understanding than language proficiency alone. They described mental health experiences shaped by intergenerational conflict, systemic discrimination, and acculturative stress, and emphasized the value of working with providers who understood these dynamics without requiring extensive explanation. These narratives suggest that English-speaking Latinos may encounter a different kind of cultural dissonance in care: one rooted not in language barriers but in the level of provider awareness about how cultural identity, immigration background, and racialization affect mental health.
Our findings contribute to the literature by underscoring that Latino identity is not homogenous, and that language preference may serve as a proxy for understanding service delivery needs within the broader Latino community. This has direct implications for research, intervention development, and health policy. Mental health services targeting U.S. Latino populations must be tailored to the linguistic and cultural nuances within this group, not only expanding access to bilingual providers but also investing in training that cultivates cultural humility. Moreover, we found that emotional barriers such as shame, fear of judgment, and mistrust of providers were embedded in participants’ narratives and often as potent as logistical constraints in preventing help-seeking. This points to the need for community-facing psychoeducation and stigma reduction campaigns that are linguistically accessible and culturally relevant. In sum, this study adds a much-needed layer of specificity to the understanding of possible MDD treatment barriers among Latinos by centering the voices of both Spanish- and English-speaking individuals. It calls for a shift from one-size-fits-all models of culturally responsive care to stratified, equity-oriented approaches that recognize the within-group diversity of Latino communities and actively dismantle the multi-level barriers they may face in accessing mental health care.
Footnotes
Acknowledgments
We appreciate the participants who completed qualitative interviews, which provided valuable insight into their perceived barriers to depression treatment. We also thank community organizations, particularly El Futuro Inc. and Progreso Latino, Inc., for their valuable feedback on our findings.
Ethical approval and consent to participate
The University of Arkansas Institutional Review Board (Protocol #: 2112375993
Author contributions
Conceptualization: L. E. Guzman; Data curation & formal analysis: L. E. Guzman, K. M. Fite; Investigation & project administration: L. E. Guzman, K. M. Fite; Resources: L. E. Guzman, A. J. Bridges; Writing original draft: L. E. Guzman, A. J. Bridges, H. E. Frank, R. G. Martinez, K. M. Fite. All authors approved the submitted version, agreed to be accountable for their contributions, and attested to the work's accuracy and integrity.
Funding
Dr. Guzman was supported by the National Latino Psychological Association's 2021 Cynthia de las Fuentes Dissertation Award and is currently supported by NHLBI T32HL176428-01.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.