
Abstract
The objective of this study was to describe the prevalence and demographic correlates of mental disorders and healthcare-seeking behavior of adolescents in Mozambique. Trained assessors administered sociodemographic questionnaires and the Portuguese Mini International Neuropsychiatric Interview for Children and Adolescents (MINI-KID) to adolescents in two schools in Maputo City, Mozambique to determine mental disorder diagnoses. Associations between sociodemographic factors and mental disorders were assessed with logistic regressions. Among 488 Mozambican students (ages 12 to 19; 66.4% female), the prevalence of mental disorders was 23.0%. Anxiety (17.8%) and depressive disorders (8.6%) were most common. Half of adolescents who were diagnosed with a mental disorder had two or more diagnoses. Females were more likely than males to have a mental disorder (odds ratio (OR) 1.60, 95% confidence intervals (CI) 1.00–2.57), and the likelihood of mental disorder diagnosis increased with age (OR 1.28, 95% CI 1.12–1.47) and grade (OR 1.24, 95% CI 1.07–1.45). Only 2.7% of adolescents with a mental disorder had sought mental health care in the previous year. To our knowledge, this is the among the first studies to use a structured diagnostic interview (MINI-KID) to report the prevalence of mental disorders among Mozambican adolescents. High rates of untreated mental disorders underscore urgent need for increased mental health services. High comorbidity of mental disorders suggests that transdiagnostic interventions may be an effective approach to care. Primary healthcare settings where adolescents routinely receive care may be appropriate for mental health treatment integration.
Introduction
Mental disorders are a leading cause of disability among adolescents globally (Gore et al., 2011). Despite the fact that 90% of the global adolescent population resides in low- and middle-income countries (LMICs), there is limited epidemiological data on the prevalence of adolescent mental disorders in these regions (Erskine et al., 2017). Key social determinants such as poverty, food insecurity, educational exclusion, and exposure to crime/violence, which are prevalent in low-resource settings, are positively associated with the development of mental disorders (Hart & Norris, 2024; Lund et al., 2018). Consequently, adolescents in LMICs may face higher risk of developing mental disorders compared to their peers in high-income countries (HICs). To date, much research from LMIC settings, and particularly Sub-Saharan Africa (SSA) has reported on the mental health of adolescents in high-risk contexts, such as individuals living with HIV and/or in conflict or post-conflict settings (Sequeira et al., 2022; Steel et al., 2022). There is a critical gap in the collective understanding of the burden of mental health disorders among adolescents outside these high-risk groups. Furthermore, global studies reveal considerable variation in the prevalence of mental disorders across countries (Kieling et al., 2011), highlighting the need to assess and address the mental health needs of adolescents across LMIC settings.
Half of mental disorders begin to appear before the age of 18, highlighting adolescence as a critical window of opportunity to address mental health needs as they emerge (Kessler et al., 2007; Solmi et al., 2022). Early intervention, particularly near onset, has been shown to prevent or reduce both the severity of mental health disorders and their long-term effects (Fusar-Poli, 2019; Fusar-Poli et al., 2021; Salazar de Pablo et al., 2020). However, LMICs often face significant barriers to addressing adolescent mental health needs due to shortage of trained providers, limited resources, and policies that do not center the needs of adolescents. These challenges are compounded by difficulties advocating for appropriate resource allocation without reliable data on the scope and scale of the issue. To effectively advocate for and guide the optimal allocation of limited resources toward addressing adolescent mental health in LMICs, it is essential to document the prevalence of mental disorders and identify the most efficient pathways for adolescents to access care.
Mozambique is a low-income, lusophone country in sub-Saharan Africa with an adolescent population of approximately 6.6 million, or 23% of the total population (Instituto Nacional de Estatística, 2011). Although there has been a marked increase in national mental health services in the past decade, Mozambique, like other LMICs, has limited trained and licensed mental health professionals. Per the latest available data, there are an estimated 500 psychologists, 550 psychiatric technicians, and 24 psychiatrists for a population of 31 million (Mozambique Ministry of Health, 2019). This is well below the average of 29 mental health nurses and 8 psychiatrists per 100,000 in HICs (World Health Organization, 2021). The Mozambican Ministry of Health is committed to expanding youth mental health services (Departamento de Saúde Mental, 2015), and understanding the mental health needs and healthcare-seeking behaviors of adolescents is critical to effectively targeting limited resources and implementing interventions for the most vulnerable populations. Early intervention in this setting is vital given recent findings that more than half of Mozambican adults attending primary care facilities met the diagnostic criteria for at least one mental disorder (Gouveia et al., 2023).
To the best of our knowledge, few studies have been published on the mental health of adolescents in Mozambique, and even fewer have used clinical diagnostic interviews such as the Mini International Neuropsychiatric Interview for Children and Adolescents (MINI-KID) to assess prevalence of mental disorders among adolescents in schools. To address this gap in the literature, this study aimed to (a) describe the prevalence and demographic correlates of mental disorders among adolescents in Mozambique; and (b) explore adolescents’ mental health and primary healthcare-seeking behaviors and key predictors.
Methods
Sample
For this cross-sectional study, adolescents were recruited from two secondary schools in Maputo City, the Mozambican capital. One school was urban (total school enrollment 3243; 58.2% female) and the other was peri-urban (total school enrollment 2987; 55.1% female), with student bodies that were representative of higher and lower socioeconomic classes, respectively (Instituto Nacional de Estatística, 2017). The two schools were selected in collaboration with the Ministry of Education to ensure that (a) adolescents of diverse socioeconomic backgrounds would be included and (b) the schools would be located directly next to a primary care clinic with a psychologist on staff.
The primary objective of data collection was to validate brief instruments (e.g., adapted Generalized Anxiety Disorder-7 (GAD-7) and Patient Health Questionnaire-9 (PHQ-9)) to reduce the burden of assessing mental disorders among adolescents, which previously was done using long structured diagnostic interviews. Accordingly, the final sample size was determined to ensure appropriate margins of error for sensitivity and specificity estimates. The results of the validation study and additional methodological details have been published (Lovero et al., 2022a). We aimed to enroll 50 adolescents (ages 12–19) per grade (8–12) to achieve an even distribution of participants across ages and grades and enable comparison of mental disorder diagnoses by age and grade. A random selection of two or three classes per grade from each school were invited to participate. Research staff described the study to teachers of the selected classrooms two weeks prior to data collection, after which students were given paper consent forms to review with their caregiver(s) and return signed. Of 1320 adolescents who received consent forms, 87.1% (n = 1150) returned signed consent forms. Among those who provided signed caregiver consent, 493 (42.9%) were randomly selected for eligibility evaluation. Five adolescents were excluded for the following reasons: (a) consent form that was not signed by caregiver(s) (n = 1); (b) over 19 years of age (n = 3); or (c) incomplete assessments (n = 1).
Measures
All questionnaires were administered in Portuguese by trained interviewers and included items on demographic characteristics (e.g. age, gender, religion), socioeconomic indicators (e.g. household amenities), and healthcare-seeking behavior, a battery of mental health screeners, and the Portuguese version of MINI-KID (Sheehan et al., 2010).
Demographic characteristics and socioeconomic indicators were assessed with questions designed for an appropriate reading level. Examples included: “What is your race? (options: Black, Mixed, White, Indigenous, Other, I don’t know)”; “Who do you live with? (options: Family, Friends, Others (not family or friends))”; “Do you have internet at home? (options: Yes, No)”; “Do you have your own cell phone? (options: Yes, No).”
Participants reported healthcare-seeking behaviors for specified time frames (past month, past year, and lifetime) and settings (primary care clinic, hospital, traditional healer, mental health services) by answering questions such as: “Have you sought care at a primary care clinic in the past month?” Similar questions were posed for each healthcare service and time frame. Participants were asked about past month and year care seeking at a particular setting only if they had endorsed lifetime use.
Diagnoses reported in this paper were based on responses to the MINI-KID, which is a brief, structured, diagnostic interview that assesses 24 unique mental health disorders according to criteria set by the International Classification of Diseases, 10th Revision and the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition. The MINI-KID applies specific time frames to define “current” status for each of the disorders it assesses (Sheehan et al., 2010). The current study assessed 13 mental health conditions selected by local stakeholders as most relevant in the setting (Lovero et al., 2022b), which are listed here with the time frames that define what it means to have a “current” diagnosis: major depressive episode (MDD, past 2 weeks), anxiety (panic disorder, past month; agoraphobia, current; separation anxiety disorder, past month; social anxiety disorder/social phobia, past month; and generalized anxiety disorder, past 6 months), posttraumatic stress disorder (PTSD, past month), substance use disorder (SUD, alcohol use disorder, past 12 months; and substance use disorder, past 12 months), disruptive behavior disorder (DBD, including conduct disorder, past 12 months; and oppositional defiant disorder, past 6 months), and attention-deficit hyperactivity disorder (ADHD, past 6 months). The MINI-KID was previously translated into Portuguese by a multidisciplinary and multilingual team in Brazil (Rijo et al., 2016), who used the gold standard method of translation and back-translation and worked with the author of the MINI-KID to ensure consistency with the original English-language MINI-KID.
Data Collection
Thirteen local psychologists administered the study questionnaires between 9 September and 2 October 2019. Each day, eligible students from two classes were selected for participation using randomly ordered consent forms. All participants first answered sociodemographic questions and were subsequently randomly assigned to receive either the screening battery or the MINI-KID first. A different interviewer administered the final remaining measure. Data was collected in real-time on tablets through the REDCap electronic data collection platform (Harris et al., 2009, 2019).
Adolescents who screened positive for a mental health disorder on the MINI-KID were invited to participate in a brief mental health intervention conducted by on-site research team members (SA, CB, MEF, TR) and referred to the local primary healthcare clinic. In the event that an adolescent reported acute suicide risk, caregivers were immediately contacted and the adolescent was accompanied to the psychologist at the primary care clinic. The psychologist then assumed responsibility of engaging the caregivers further under treatment as usual, including providing support and guidance to those who chose to engage. Additional detail on data collection can be found in a previous publication (Lovero et al., 2022a).
Data Analysis
Analyses were conducted in Stata IC 14. Due to overlap in the kinds of care provided at primary care clinics and hospitals in Mozambique, we collapsed these services into a single “general healthcare” category. In addition, given that the vast majority of adolescents in the schools we recruited from are Black, Portuguese-speaking, and practice a form of Christianity, and that being in an ethnic minority group has previously been shown to be associated with mental health problems (Al-Sharifi et al., 2015; Mangalore & Knapp, 2012), we created a “minority” variable under which participants identifying as non-Black, not primarily Portuguese-speaking, and/or non-practicing of Christianity were included. We calculated summary statistics for participant demographics, MINI diagnoses, comorbidity of diagnoses, and care-seeking behavior. Bivariate logistic regression models evaluated associations between demographic characteristics (independent variable) and any mental disorder (dependent variable) or individual mental disorders (dependent variables).
Results
Across the two schools, 488 Mozambican adolescents (66.4% female, mean (M) age = 15.9 years, SD age = 1.7 years) participated in this study. A majority of students self-identified as Black (95.5%), preferred to speak Portuguese (90.8%), and practiced Catholicism or Christianity (87.6%) (Table 1).
Demographic Characteristics of Study Sample (n = 488) From Two Mozambican Secondary Schools.
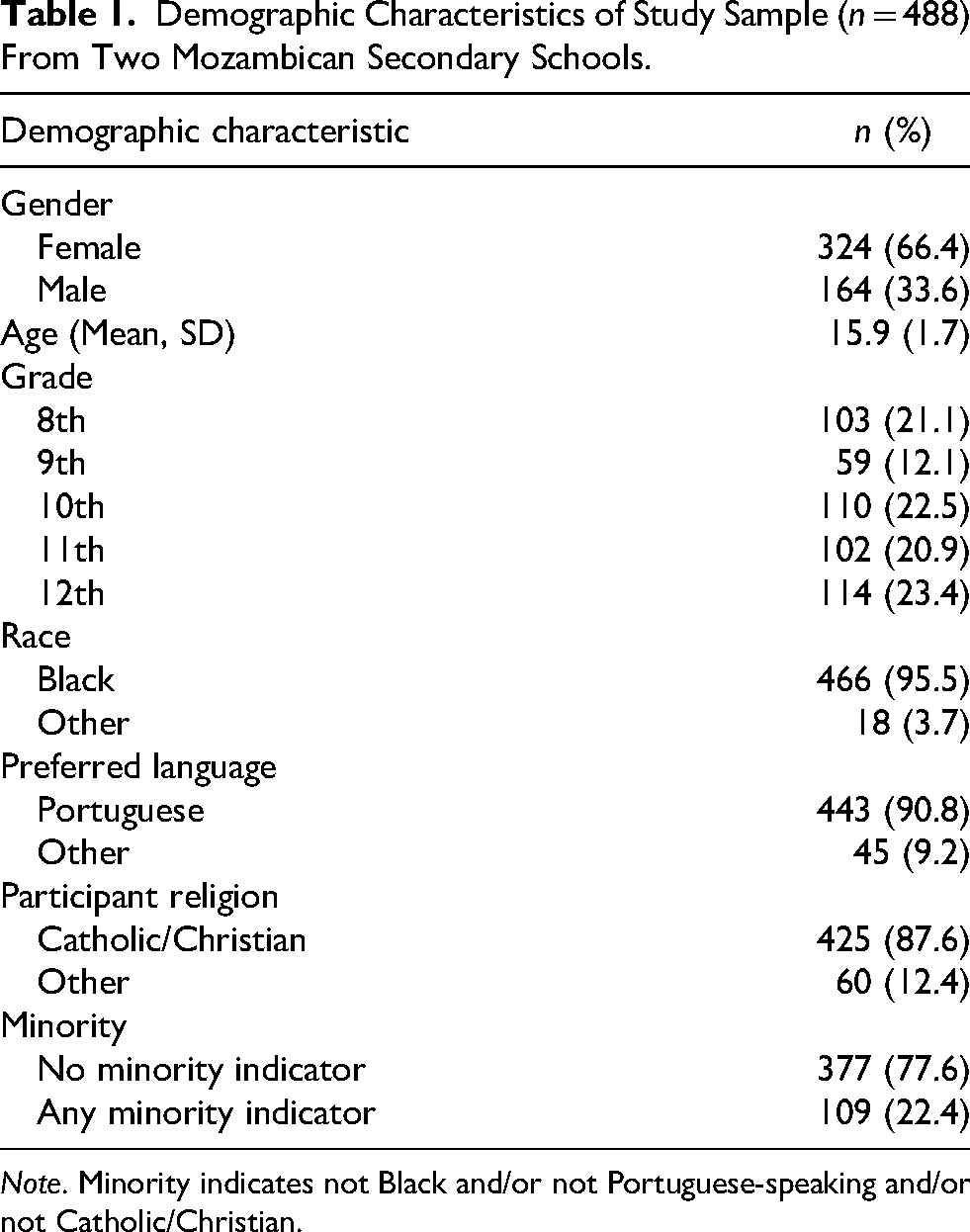
Note. Minority indicates not Black and/or not Portuguese-speaking and/or not Catholic/Christian.
Prevalence
Nearly one-quarter (23.0%) of participating adolescents met the criteria for at least one mental disorder. The most common disorders were anxiety disorders (17.8%), major depressive episode (MDD) (8.6%), and disruptive behavior disorder (DBD) (6.6%). Less prevalent disorders were SUD (4.5%), ADHD (3.3%), and PTSD (1.2%). The prevalence of mental disorders across the entire sample population, broken into diagnoses, is shown in Table 2. Half of adolescents (50.0%) who screened positive for any disorder screened positive for multiple disorders. A majority (n = 31; 55.4%) of individuals with comorbid diagnoses had two diagnoses, 13 (23.2%) had three diagnoses, 8 (14.0%) had four, and 3 (5.4%) had five. Anxiety was the most commonly comorbid diagnosis; Three-quarters (76.0%) of adolescents diagnosed with MDD, 100% of those diagnosed with PTSD, 75.0% of those diagnosed with ADHD, 81.3% of those diagnosed with DBD, and 59.1% of those diagnosed with SUD also met criteria for an anxiety disorder (Supplementary Table 1).
MINI-KID Mental Disorder Diagnoses Among Mozambican Adolescents (n = 488) Aged 12–19.
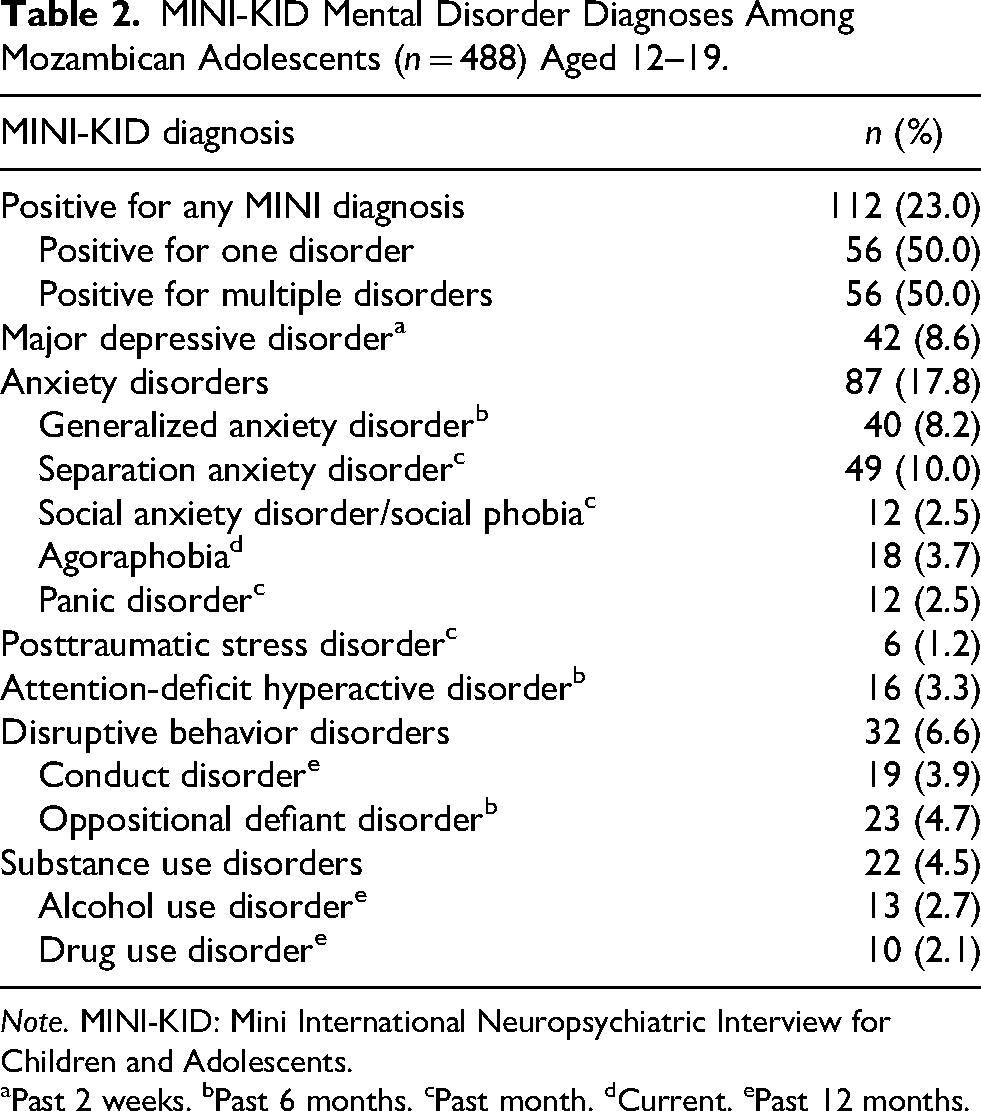
Note. MINI-KID: Mini International Neuropsychiatric Interview for Children and Adolescents.
Past 2 weeks. bPast 6 months. cPast month. dCurrent. ePast 12 months.
Sociodemographic Correlates of Mental Disorders
There was no significant difference in the prevalence of mental disorders between schools (27.63% vs. 22.1%; odds ratio (OR) 0.74; 95% confidence intervals (CI) 0.43–1.29). Table 3 compares the prevalence of mental disorder diagnoses by key demographic characteristics. The average age of students experiencing any mental disorder was 16.4 years (SD 1.5). One-quarter of female (25.6%) and nearly one-fifth of male adolescents (17.8%) had any mental disorder. The most common mental disorder among both female and male students was anxiety (22.5% and 8.5%, respectively). Among female adolescents, the second most common diagnosis was MDD (10.8%), followed by DBD (7.1%) and SUD (4.0%). Among male adolescents, the next most common diagnoses were DBD (5.5%) and SUD (5.5%).
MINI-KID Diagnoses by Demographic Characteristics Among Mozambican Adolescents (n = 488) Aged 12–19.
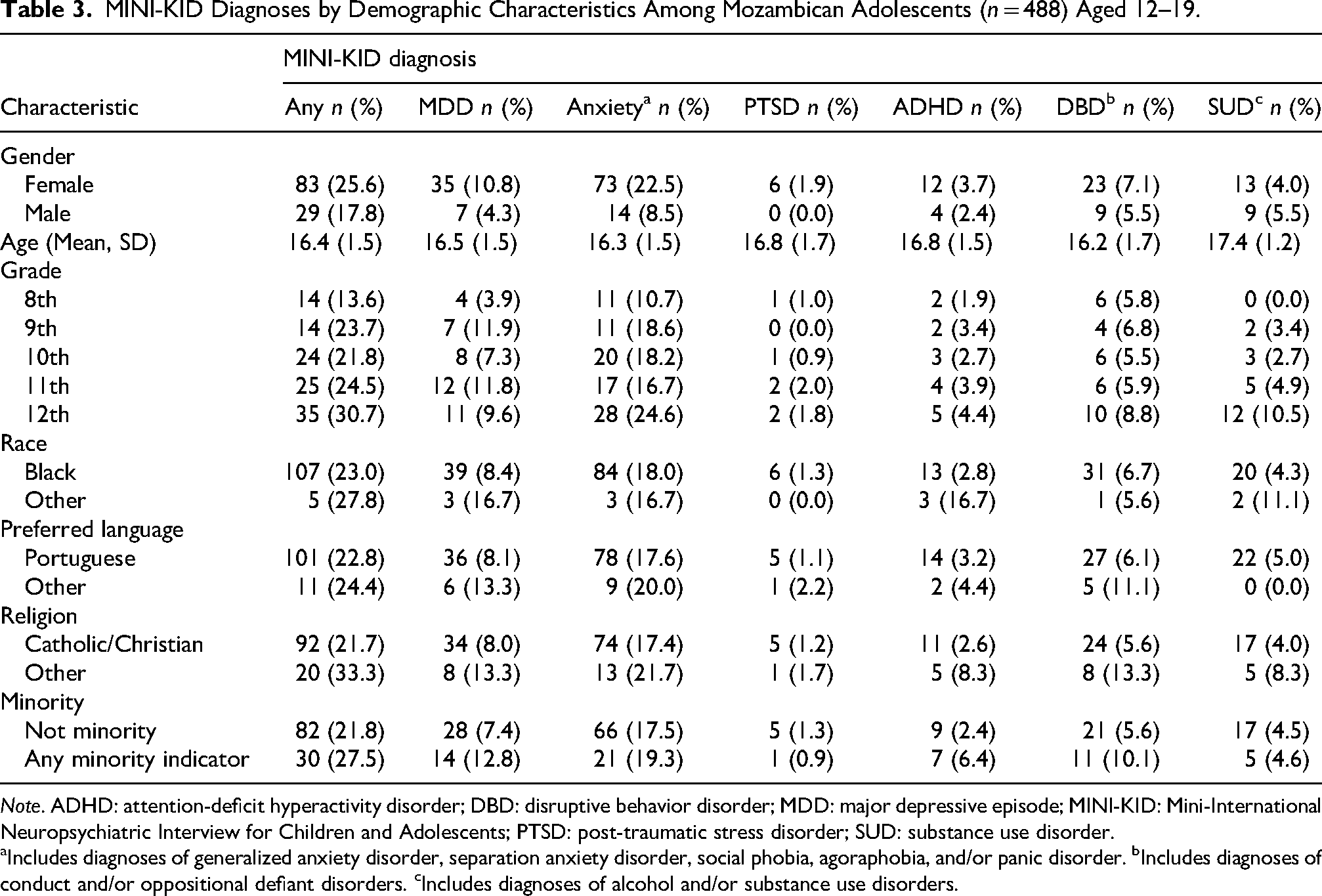
Note. ADHD: attention-deficit hyperactivity disorder; DBD: disruptive behavior disorder; MDD: major depressive episode; MINI-KID: Mini-International Neuropsychiatric Interview for Children and Adolescents; PTSD: post-traumatic stress disorder; SUD: substance use disorder.
Includes diagnoses of generalized anxiety disorder, separation anxiety disorder, social phobia, agoraphobia, and/or panic disorder. bIncludes diagnoses of conduct and/or oppositional defiant disorders. cIncludes diagnoses of alcohol and/or substance use disorders.
Adolescents with a diagnosis of any mental disorder were significantly more likely to be female (OR 1.60, 95% CI 1.00–2.57), older (OR 1.28, 95% CI 1.12–1.47), and in a higher grade (OR 1.24, 95% CI 1.07–1.45; Table 4). Among specific diagnoses, MDD (OR 2.72, 95% CI 1.19–6.26) and anxiety (OR 3.12, 95% CI 1.70–5.72) were more common in female adolescents, whereas ADHD, DBD, and SUD were equally common among male and female adolescents (p > .05). Older age was associated with increased likelihood of all mental disorders except DBD, but higher grade was only significantly associated with increased likelihood of meeting criteria for an anxiety diagnosis (OR 1.22, 95% CI 1.03–1.43). Preferred language was not associated with diagnosis of any mental disorders. Adolescents with any minority characteristic were not more likely to have any diagnosis but were almost three times as likely (OR 2.81, 95% CI 1.12–1.47) as those without any minority characteristics to have ADHD.
Association of Demographic Characteristics and MINI-KID Diagnoses Among Mozambican Adolescents (n = 488) Aged 12–19.

Note. Odds ratios from analyses with n < 5 were not calculated. ADHD: attention-deficit hyperactivity disorder; CI: confidence intervals; DBD: disruptive behavior disorder; MDD: major depressive episode; MINI-KID: Mini-International Neuropsychiatric Interview for Children and Adolescents; OR: odds ratio; PTSD: post-traumatic stress disorder; Ref: reference; SUD: substance use disorder. Statistically significant associations are shown in bold.
Includes diagnoses of generalized anxiety disorder, separation anxiety disorder, social phobia, agoraphobia, and/or panic disorder. bIncludes diagnoses of conduct and/or oppositional defiant disorders. cIncludes diagnoses of alcohol and/or substance use disorders.
Healthcare-Seeking Behavior
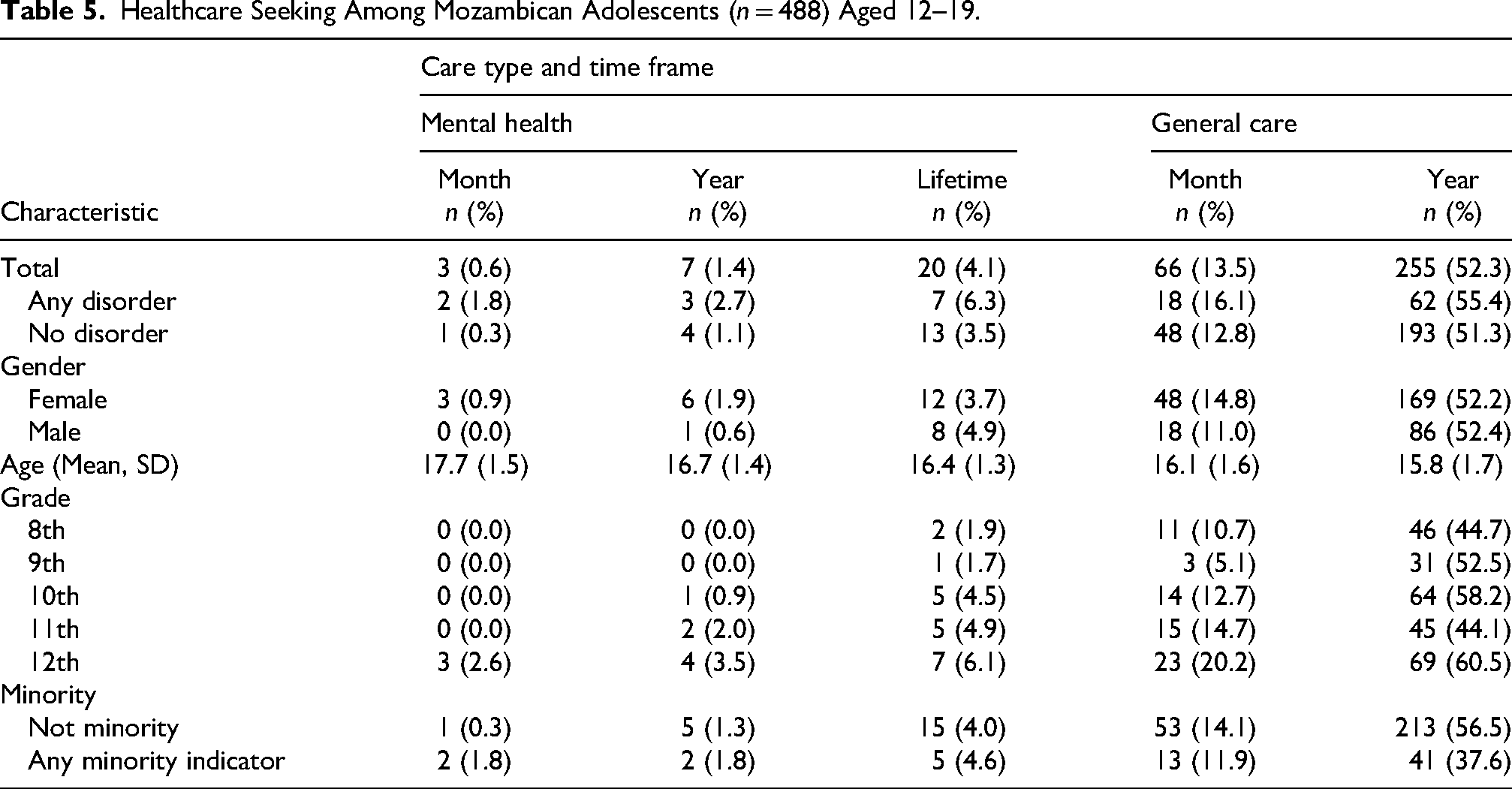
Slightly more than half (52.8%) of all adolescents had sought general healthcare in the past year, and 13.5% had utilized general healthcare in the past month. Mental health care seeking was rare, with only 4.1% of adolescents having sought mental health care in their lifetime. Of the 112 adolescents with a current diagnosis of a mental disorder, 7 (6.3%) had ever sought mental health care, 3 (2.7%) had sought mental health care in the previous year, and 2 (1.8%) had sought mental health care in the previous month.
Table 5 shows data on care seeking by sociodemographic characteristics. Having a current mental disorder was not significantly associated with seeking general healthcare in the past year (OR 1.17, 95% CI 0.8–1.8) or past month (OR 1.3, 95% CI 0.73–2.4). Notably, adolescents who identified with any or multiple minority characteristic (OR 0.46, 95% CI 0.3–0.72) were less likely to have sought general healthcare in the past year. Having a current mental disorder was also not associated with having ever sought mental health care (OR 1.86, 95% CI 0.7–4.8). Recent and lifetime mental health care seeking was so rare in this sample that we were unable to conduct additional statistical comparisons of sociodemographic factors.
Healthcare Seeking Among Mozambican Adolescents (n = 488) Aged 12–19.
Discussion
This research aimed to contribute to the global understanding of adolescent mental health by using a structured diagnostic tool (MINI-KID) to measure the prevalence of adolescent mental disorders in a school setting in Mozambique. The cross-sectional study of 488 school-aged adolescents in Maputo City found that almost a quarter of participating adolescents met the criteria for a current mental disorder (23%). Anxiety disorders were the most common (17.8%), followed by MDD (8.6%), DBD (6.6%), and SUD (4.5%). PTSD (1.2%) and ADHD (3.3%) were the least common. Notably, half of adolescents who met the criteria for any mental disorder also met the criteria for more than one disorder, indicating high levels of comorbidity. Female adolescents, older adolescents, and those in higher grades were more likely to endorse mental health symptoms, which is consistent with global trends (Martel, 2013; Merikangas et al., 2010). Despite the high prevalence of mental disorders in this sample, only 6.3% of adolescents with a current mental disorder had ever sought mental health care - an indication of a notable treatment gap.
The prevalence of mental disorders identified in this study exceeds the global estimate of the burden of mental disorders (13.4% prevalence) among children and adolescents reported in a 2015 meta-analysis (Polanczyk et al., 2015). This disparity may partly reflect a difference in study methodologies, as the meta-analysis included studies using parent-reported measures and studies among younger children, both of which are associated with lower reported prevalence rates (McDonald et al., 2021; Merikangas et al., 2010; Vasileva et al., 2021; Whitney & Peterson, 2019). Moreover, only two studies from Africa were included in the meta-analysis, highlighting the critical gap in high-quality, context-specific data on adolescent mental health in African contexts (Ashenafi et al., 2001; Polanczyk et al., 2015; Robertson et al., 1999).
There is a significant lack of data on the occurrence and burden of adolescent mental disorders in African countries, which is compounded by substantial heterogeneity in the assessment tools used and populations included across studies (Greene et al., 2021; Kieling et al., 2011). Existing research on adolescent mental health in African contexts has often focused on specific populations (e.g. individuals living with HIV or those in conflict-affected settings) and has often relied on screening tools rather than diagnostic interviews (Di Gennaro et al., 2022; Jörns-Presentati et al., 2021; Nguyen et al., 2023; Pengpid et al., 2024). Studies conducted in Africa with the MINI-KID have found high prevalence of mental disorders among adolescents, including a study in Botswana that found that 34% of public school students met the criteria for having a mental disorder and another in rural Uganda, which found that 27% of children and adolescents met criteria for an anxiety disorder (Abbo et al., 2013; Olashore et al., 2022). The current study's findings add to the growing evidence that adolescent mental health is a pressing issue in many African countries, including Mozambique.
The unique sociocultural and structural context of Mozambique may contribute to the current study's findings of high prevalence of mental disorders and the wide treatment gap. The high levels of anxiety observed in this study, in contrast with global estimates (where depression tends to be most common), may be partially explained by contextual stressors within Mozambique, such as widespread poverty, family separation due to economic migration, and exposure to violence (Gore et al., 2011). This hypothesis is consistent with findings from previous studies in Mozambique (which used screening tools such as the PHQ-9 and GAD-7) that reported similarly high prevalences of psychosocial distress, depression, and anxiety (Amu et al., 2020; Pengpid et al., 2024). In Mozambique, traditional healing practices and low mental health literacy may also influence adolescents’ conceptualization of mental disorders and health-seeking behaviors (Lovero et al., 2022b; Mlambo, 2012). Although the adolescents in the current study did not report commonly seeking care among traditional healers, recently-published studies in Mozambique have found that traditional healers are often sought for health concerns, including mental health symptoms (Pengpid et al., 2024; Takeyama et al., 2022). This divergence in findings may result from the phrasing of the questions (e.g., asking about seeking healthcare vs. seeking help), or from the regional location of the studies (capital city vs. outer provinces with different cultural and religious representations).
Although recent research indicates that depression and anxiety are increasingly recognized and normalized among Mozambican adolescents, barriers including stigma, lack of services, and misconceptions about mental health persist. For example, mental disorders in Mozambique are sometimes seen as either a moral failure or a normal (and temporary) part of adolescence, which may discourage adolescents from seeking care (Lovero et al., 2022b). These beliefs may have contributed to the low lifetime and recent mental health care seeking behavior observed in this study, even among adolescents with a current mental disorder diagnosis.
The treatment gap found in this study is higher than in most other global reports. While this study found a treatment gap of almost 95%, previous studies in South America and other LMICs have found treatment gaps of 81%–88%, with an estimated 12%–19% of children and adolescents with mental disorders currently accessing or having previously sought mental health services (Duarte et al., 2022). In addition, studies in the USA have found that approximately one-third to one-half of adolescents with mental disorders receive services for their illness (Merikangas et al., 2010; Whitney & Peterson, 2019). Future research should investigate adolescents’ motivations for and barriers to accessing mental health services to identify effective pathways to improve access to treatment. The current research provides a hint; more than half of all adolescents in this sample had sought services at a general healthcare facility in the past year, suggesting that primary care settings may be an effective setting for integration and continued destigmatization of mental health services (Chandra-Mouli et al., 2015).
In addition to identifying appropriate settings for mental health treatment integration, novel treatment approaches may be beneficial in this context. Anxiety is known to be associated with suicidal ideation among school-aged Mozambican adolescents, pointing to the urgent need for targeted, evidence-based, and culturally-informed interventions in this high-prevalence context (Amu et al., 2020; Come et al., 2022). Modular, transdiagnostic approaches designed to address multiple and/or comorbid mental health problems using common therapeutic elements may be particularly well-suited for a Mozambican context for two main reasons (Giusto et al., 2023). First, there was high prevalence of comorbid mental disorders in this study, consistent with prior research in LMICs that has found fewer distinctions between diagnostic categories when compared to HICs (Bolton et al., 2012; Murray et al., 2006; Rasmussen et al., 2011). Second, transdiagnostic approaches often employ task-shared, non-specialist healthcare workers, which is particularly relevant for low-resource settings where mental health resources are often scarce (Le et al., 2022; Murray et al., 2014).
To the best of our knowledge, this study is among the first to provide estimates of the prevalence of mental disorders among Mozambican adolescents using a structured diagnostic tool. We hope that these results can offer actionable data for policymakers. Improving adolescent mental health in Mozambique will require integrating culturally sensitive mental health education into existing healthcare frameworks, reducing stigma on a wider scale, and expanding access to services across the country (Lovero et al., 2022b; Wainberg et al., 2021). By focusing on scalable and sustainable interventions, Mozambique can take critical steps toward closing the treatment gap and improving mental health outcomes for its young people.
There are many questions that remain to be answered. For example, the gender differences in externalizing disorders that is typically found in high-income settings (boys are more likely to be diagnosed with externalizing disorders) was not found in this study, which could indicate that boys in Mozambique with ADHD or DBD are more likely to drop out of school, a phenomenon seen in other low-resource settings (Howard et al., 2016; Kent et al., 2011; Kuriyan et al., 2013). Future research should explore the dynamics of externalizing mental disorders in non-school based samples. This study had some limitations. First, it was conducted in Maputo and is therefore not generalizable to the national population. However, one urban and one peri-urban school were purposely included in order to capture the experiences of students from diverse sociodemographic backgrounds. Second, the MINI-KID, as a standard diagnostic tool, could not be culturally adapted to the local context. Third, the sample size prevented us from making comparisons between some mental health diagnoses (PTSD and ADHD) and sociodemographic characteristics. Similarly, the low number of adolescents who had ever sought mental health care limited our ability to examine all factors related to care-seeking behaviors. Despite these limitations, we believe this paper makes a significant contribution to the literature as one of the first publications reporting the prevalence of mental disorders among Mozambican adolescents using a clinical diagnostic tool in a school setting.
Conclusion
The high prevalence of mental disorders and disproportionately large treatment gap among the Mozambican adolescents in our sample underscores the need for increased access to mental health care in this setting. Current care-seeking behaviors and high levels of comorbid mental disorders point future researchers to explore the potential benefits of transdiagnostic interventions and integrating mental health services into general healthcare settings. Lastly, our research highlights that the resource allocation in LMICs should be based on setting-specific data rather than global estimates, and should rely on high-quality diagnostic tools to identify accurate distribution of disorders across sociodemographic factors.
Supplemental Material
sj-docx-1-tps-10.1177_13634615251409683 - Supplemental material for Prevalence of Mental Disorders and Healthcare Seeking Among Mozambican Adolescents in School
Supplemental material, sj-docx-1-tps-10.1177_13634615251409683 for Prevalence of Mental Disorders and Healthcare Seeking Among Mozambican Adolescents in School by Aisha King, Salma Adam, Carolina Bila, Maria Eduarda Fernandes, Teresa Rodrigues, Palmira Fortunato dos Santos, Milton L. Wainberg, Cristiane S. Duarte, and Kathryn L. Lovero in Transcultural Psychiatry
Footnotes
Acknowledgements
The authors would like to thank the study participants as well as Leonor Sebastião, BS; Lourena Chemane, BS; Lino Conjo, BS; Ana Cristina Gamito, BS; Olência Gulube, BS; Carolina Matsolo, BS; Marcia Mathe, BS; Meriba Mazove, BS; Nilza Simbine, BS; Aldo Saute, BS; Lourenço Zilria, BS for support in data collection.
ORCID iDs
Ethics Statement
The New York State Psychiatric Institute Institutional Review Board (#7479) and the Eduardo Mondlane University Institutional Health Bioethics Council (CIBS FM & HCM/54/2017) approved all study procedures and materials. Written consent was obtained from all participants and their parent or guardian (adolescents ages 12–17).
Author Contributions
AK and KL conducted analyses and drafted the manuscript. All other authors reviewed and edited the manuscript critically for intellectual content. SA, CB, MEF, TR, CR, KL, AK, and PFS contributed significantly to data acquisition and curation. KL and MW were responsible for obtaining funding for the research. KL conceptualized the project and is the corresponding author. All authors approved final version of the manuscript for publication.
Funding
This study was funded by the National Institute of Mental Health (K01MH120258, U19MH113203, and T32MH096724) and Fogarty International Center (D43TW009675). The funders had no role in study design; data collection, analysis, and interpretation; or manuscript writing and submission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
Anonymized data sets used in the current study are available under reasonable request addressed to the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.