
Abstract
The personal recovery approach in mental health draws on people's own experiences to build care policies. Models of personal recovery constructed in recent decades have been based on studies in Anglo-European cultural settings. No study has been conducted in Martinique, where Creole culture is prevalent. Our work aimed to explore the recovery experiences of people with schizophrenia in Martinique. We carried out a qualitative study. Fifteen people participated in a face-to-face interview, with collection of sociodemographic data. Three themes emerged from the analysis: self-work; evolving illness role; and rebuilding identity. Our results described a recovery process in which strong importance is given to social norms, involving difficult adjustments among multiple therapeutic approaches and overcoming psychological trauma. Access to employment, housing, and financial autonomy was related to social recognition. These results suggested the value of different approaches to aid recovery, including: support from relatives, peers, and caregivers; valuing their experiential knowledge; support for psychological trauma; fighting against the stigmatization of schizophrenia in Martinique; social support for work and housing empowerment; and recognition of the complementarity of the biomedical, religious, and traditional health care sectors.
Keywords
Introduction
Schizophrenia affects approximately 24 million people, or about one in 300 globally (WHO, 2022). It is a highly debilitating disorder, ranked among the 10 diseases that contribute most to the global burden of disease (GBD, 2018; Murray et al., 1996) as tracked by the World Health Organization (WHO, 2022). Schizophrenia presents complex symptoms (positive, negative, and cognitive) and has multiple causes. It has been found to have high heritability (now estimated at 80% (Ripke et al., 2014; Sullivan et al., 2003), and has been linked to in utero adversity and obstetrical complications as well as disruption in early childhood (Bramon et al., 2005; Erlenmeyer-Kimling et al., 2000; Hulshoff Pol et al., 2000; McCutcheon et al., 2020; Murray et al., 1996; Xu et al., 2009), disrupted synchronization of neural oscillations including structural and functional reorganizations in the brain (Feinberg, 1982; Fusar-Poli et al., 2012; Kambeitz et al., 2016), and increased loss of grey matter in conjunction with increase in white matter (Kumra et al., 2001; Rapoport & Gogtay, 2011; Sporn et al., 2003). Studies of the effects on the brain of neuroleptics and drugs such as methamphetamine suggest that changes in neurotransmitters (such as dopamine) influence the pathological process (Di Forti et al., 2007). Several environmental factors have also been reported to increase the risk of developing schizophrenia, including: childhood trauma, cannabis use, living in urban areas, and being a first-generation migrant (McCutcheon et al., 2020; Radua et al., 2018).
Schizophrenic disorders adversely affect the daily lives of those who suffer from them and their loved ones. Yet it is estimated that globally more than 69% of people affected by schizophrenia do not receive appropriate care (Lora et al., 2012). Many are also exposed to recurring human rights violations within their communities and mental health services (WHO, 2022).
In late 19th-century Europe, schizophrenia was thought to progress inevitably towards dementia (Jablensky, 2010). Currently, this is no longer the case. Following the development of neuroleptic drugs and other therapeutic modalities, the majority of those treated for schizophrenia experience improvements in their condition (Hopper, 2007; Stuart et al. 2017; Warner, 2004). The development of psychotropic drugs was critical to these improvements (Jablensky, 2010).
Remission has commonly been evaluated based on symptomatic and functional criteria (Hopper, 2007). However, research has shown that subjective experience is an important dimension of recovery, and that it should not be conflated with symptomatic and functional criteria (Roe et al., 2011). Studies of such subjective experience (Davidson, 2003; Deegan, 1988; Koenig, 2016; Roe et al., 2001) have described personal recovery as a singular, non-linear, multidimensional, and progressive journey (Leamy et al., 2011). A research review identified five key personal recovery processes, given the acronym “CHIME”: Connectedness (the connection to and support of others); Hope and optimism about the future; Identity remodeling; Meaning of life (the subject's appropriation of activities and places to call their own); and Empowerment (power over oneself and the power to act) (Leamy et al., 2011). However, some authors have critiqued these early studies for their Anglo-European individualistic vision of identity (Leamy et al., 2011; van Weeghel et al., 2019). Subsequent studies with cultural minorities in anglophone countries have highlighted other dimensions of personal recovery, including spirituality, community, and the management of stigma and trauma (Ellison et al., 2018; Stuart et al., 2017). Few studies have been carried out outside anglophone or European countries.
In this paper, we report a study on personal recovery from schizophrenia in Martinique, one of the main islands in the Caribbean region known as the French West Indies or French Antilles, where Creole culture is prevalent. In Martinique, 11.50% of those who received publicly insured medical care in 2021 presented with psychotic disorders, as defined by the International Classification of Diseases (CNAM, 2021; ICD, n.d.). This is the second highest rate among French regions, coming after Guadeloupe (13.66%) (CNAM, 2021), another island in the French Antilles, and is significantly higher than the average for all French territories of 7.17%.
According to an epidemiologic study conducted under the aegis of the World Health Organization French Collaborating Center (WHO-CC) in 2004, the percentage of psychoses in the general population was 2.4 times higher in a French Antilles sample (comprised of Martinique and Guadeloupe) than in a French continental sample (Ballon et al., 2004). Hypotheses offered to explain this difference included significant abuse of cocaine and cannabis in the French Antilles; a supernatural interpretation of daily events based on magic practices maintained by a significant portion of French Antilleans; and the frequent expression of mood disorders with psychotic symptomatology (Ballon et al., 2004).
Creole culture in Martinique integrates multiple cultural elements from waves of immigration to the island since the 16th century. This has resulted in diverse representations of mental health and care combining elements from the Caribbean; enslaved Africans; migration from the Middle-East, India, and China; old and more recent European medical theories; and current esoteric practices (marabouts, fortune tellers) (Eynaud, 2015). According to Martinican authors, common explanations for illness are anchored in religious and magical practices. Illness is often attributed either to divine justice or to an act of sorcery, in which the illness is “sent” via a spirit from a person who is jealous and wants to harm the victim (Bougerol, 1997, 2008; Massé, 2002). In the first case, assistance will be sought from religious practices, while for the second, recourse will be to Quimbois, a local term referring to syncretic magical practice (Bougerol, 2008). The traditional healer—who is the steward of magical practice—is a seer-healer known as “gadé-dzafé”: “the one who looks into matters” (Bougerol, 2008; Eynaud, 2015). Their practice incorporates traditional magical practices from various origins (Africa, France, India, etc.) and elements of the Catholic religion (prayers, invocation of saints, combat against the Devil, etc.) (Bougerol, 1997) and operates by countering bewitchments, facilitating deliverance, and promoting existential discourse (Bougerol, 2008). During the consultation, the gadé-dzafé questions the client about their ailments and uncovers the origin of issues that cannot be rationally understood. In the case of bewitchment, their role is to defend their client against magical attacks (Bougerol, 1997). They confirm the act of sorcery and identify the assailant. Subsequently, they provide recommendations to counter the bewitchment, which may involve defensive practices such as avoiding the accused individual and using protective talismans (Bougerol, 1997), traditional herbal remedies, purification rituals, and prayer (Massé, 2002). Alternatively, they may employ more offensive practices aimed at sending the spirit causing harm to the victim back to the aggressor (Bougerol, 1997). Although there are theoretical or moral conflicts among different approaches to healthcare, individual healthcare journeys in Martinique tend to be pluralistic and often involve both biomedical care and various non-biomedical and syncretic approaches (Massé, 2002).
To the best of our knowledge, no study has explored personal recovery in Martinique. Studies have, however, focused on resilience in Martinique, suggesting two main factors: community spirit and religious spirit (Laguerre, 2014). Resilience, defined as “a dynamic process implying positive adaptation in the context of significant adversity” (Anaut, 2005), has been identified as a factor in personal recovery (as a component of empowerment, capacity for self-management) (Leamy et al., 2011), or as an adaptation process without being strongly associated with recovery (van Weeghel et al., 2019). Yet while resilience refers to “normal” adaptive development (Anaut, 2005), personal recovery (Koenig, 2016; Pachoud, 2012) has no predefined objective, encompassing multiple transformations to overcome illness (Davidson, 2003). Experiences of recovery thus need to be studied as a whole, beyond specific components such as resilience.
Our study aimed to address the question: “How do people with schizophrenia in Martinique experience their recovery?” We hope the findings can inform the creation of recovery-oriented tools, an essential objective of the recent Territorial Mental Health Program in Martinique, thereby contributing to the improvement of social and civic inclusion (ARS, 2020).
Material and Methods
This manuscript complies with the reporting criteria of the Consolidated Criteria for Reporting Qualitative Research (COREQ 32). We followed a qualitative approach using Interpretative Phenomenological Analysis (IPA) to explore the subjectivity of participants’ experience and how they make sense of that experience (Smith et al., 2009). IPA is based on three methodological frameworks (Smith et al., 2009). The first is phenomenology, which encourages researchers to put aside their own preconceptions and prejudices in order to observe how a phenomenon appears in others’ conscious experience. The aim is to explore informants’ views of the world. The second framework, hermeneutics, considers the research to be an “interpretative activity,” because access to a participant's personal world “depends on and is complicated by the researcher's own conceptions” (Smith et al., 2009: 53). IPA comprises two layers of interpretation: the researcher interprets the participant's interpretation of their own experience. The last framework is idiography, which refers to precise and in-depth study of the singularity of each case.
We opted to collect data through open-ended interviews with a guide, which allowed for in-depth exploration of each participant's experiences (Smith et al., 2009). We also collected sociodemographic data.
The study was conducted by a multidisciplinary team of psychiatrists, psychologists, general practitioners, and an anthropologist with ties to both Martinique and Metropolitan France. The principal researcher (CB) is a psychiatrist and worked in Martinique for two-and-a-half years. The anthropologist has family origins in Martinique but currently works in Metropolitan France. All investigators are trained in qualitative methods and familiar with reflexive approaches to research. Further details are presented in Appendix 1.
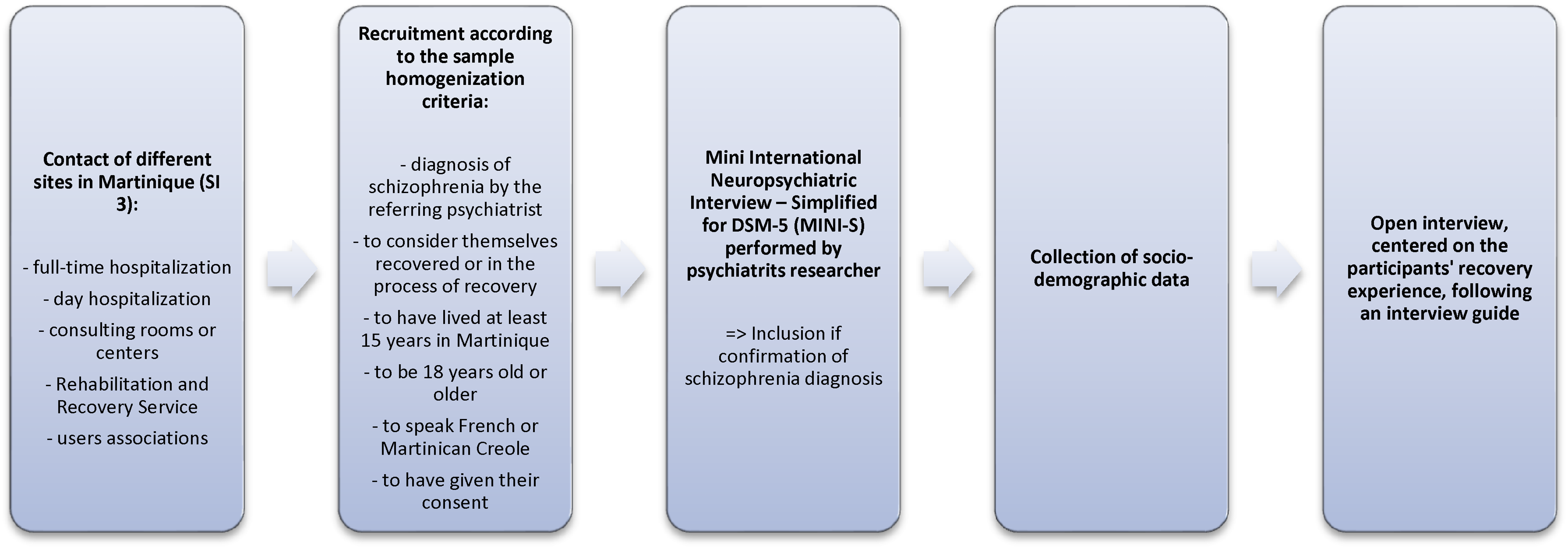
Directed recruitment was carried out on several sites (SI 3) from February 2019 to September 2020 according to the inclusion criteria shown in Figure 1. In IPA, homogenization of the sample is based on a phenomenological approach that is embodied and contextualized (Eatough & Smith, 2017). The intention is to obtain full, rich personal accounts from participants and to explore concepts and commonalities across these accounts in order to reach an in-depth understanding of the phenomenon under study.
Recruitment procedure and data collection.
The PI contacted health professionals and associations of psychiatric care users, and then both of these groups provided names and coordinates of potential participants to the PI. Interested individuals were then contacted by phone or in person to describe the study and the implications of participation. All participants received and signed an information and consent form. The study obtained ethics approval from a Parisian Institutional Review Board, the Comité de Protection des Personnes Ile de France X (Number ID RCB: 2018-A02858-47).
Interviews were conducted at Lamentin Adults Day Hospital, Maurice Despinoy Hospital, and North-Atlantic-South Center. Socio-demographic questions and questions to identify the main systems/powers they believe in were followed by a semi-structured interview lasting an average of 54.3 (32–81) minutes. The interview guide (Appendix 2) was based on the literature and the researchers’ concerns, and was refined following exploratory interviews. During interviews, participants were encouraged, through open-ended questions, to express themselves freely, expand on their thoughts, and give examples. Interviews were recorded, transcribed verbatim, and anonymized for analyses (Smith et al., 2009), then translated into English by a professional translator for publication.
IPA does not provide formal guidelines on the minimum number of interviews necessary to draw conclusive findings, given its emphasis on the singularity of experience (Mason, 2010). Sample sizes typically range from three to 15 interviews (Smith et al., 2009). Researchers in our study stopped collecting further data when they assessed that they had attained the information sufficiency threshold, that is, when interview data provided a sufficiently deep understanding of the study questions given the limits of research (delimitation of aims, targeted demographic, quality of dialogue, and depth of analysis for each interview), which are considered as essential criteria for high information power (Malterud et al., 2016). This threshold had not been anticipated before.
In this study, given the small target population (people with schizophrenia in Martinique), researchers felt in-depth analysis of 15 interviews was sufficient to identify common themes and draw conclusions (Malterud et al., 2016).
Interview transcripts were qualitatively analyzed in several steps. After repeated readings, researchers formed pairs to write descriptive notes about the form and content of participant statements, including participants’ linguistic specificities (fluency, expressions, metaphors). Researchers then fleshed out their conceptual and psychological implications (implicit content, questions about the meaning of the words, reflexivity, contextualization). The next step was to identify emerging and recurring themes by processing, associating, and synthesizing the initial data. We analyzed the data from each interview separately and then together, organizing the material into relevant categories. This inductive approach comprised descriptive, thematic, and interpretative levels of analysis, followed by the use of a matrix (Smith et al., 2009). Researchers discussed the analysis regularly and triangulated their results; that is, they regularly compared their points of view in order to ensure greater objectivity in the exploration of the experience. Any disagreement or discrepancies were resolved by group discussion before reaching consensus. The transcripts and results were not returned to the participants for validation.
Results
Details on recruitment are reported in Appendix 2. We conducted 15 in-depth interviews with four women and 11 men with an average age of 36.8 (range 24–46) years. French was the first language for all participants and Creole the second language for 13. Five participants were currently employed. In terms of religion, 10 were Catholic, two indicated they had no religious affiliation, and three gave no response. Other participant sociodemographic characteristics are detailed in Appendix 4. The average time since symptom onset was 14.6 years (range 2–27). In terms of illness, spiritual beliefs, or practices, participants mentioned: God (n = 12); Quimbois, magic, or bewitchment (12); astrology or clairvoyance (4); karma (1); higher good power distinct from God; African-origin marabout practice (1); and no belief (1). Three themes emerged from the analyses: self-work, evolving illness role, and rebuilding identity. The themes and sub-themes are summarized in Appendix 5, with further examples of citations.
Theme 1: Self-Work
Participants described living through painful experiences before they were able to accept their illness. They experienced their illness as a sudden intrusion locking them into a present without prospects, stimulating a sense of constant failure and a loss of certain parts of the self, of projects and dreams, and of parenthood. As one participant stated: “We’re not actually going anywhere; we’re building nothing; we’re exhausting ourselves in fact” (PN).
Some spoke of the injustice of being sick without social recognition. Participants often viewed hospitalization as an unjust punishment, where restrictions on everyday freedoms reinforced their dependency on friends and family without a compensatory affirmation of their subjectivity through their treatment. This led to a sense of illness as causing setbacks: “Each time I had to start over again” (PB).
Very gradually over the span of their illness experience, the possibility of living with the illness appeared in participants’ narratives. Participants also recounted how they made efforts to cope. Aware of their psychological fragility, participants developed different strategies of control (with respect to emotions, words, actions, medication adherence, ritualization, resistance to change, selection of relationships) and avoidance (for example, of attachment relationships experienced as insecure, withdrawal from social relationships). As one participant, who was living like a monk, described this process: “Do you know (…) It is a bit this analysis that I made in my solitude. I behaved a little like a meticulous person, (…) who is very careful” (PM).
Participants engaged in highly disciplined routines to structure their daily lives. They prioritized early-morning rising, rigorous personal and dietary hygiene, regular exercise, and rest as conditions of an active and healthy life, with the aim of “keeping busy” and avoiding intrusive thoughts. In the words of one participant: “Especially getting up in the morning. When you manage to do this on your own, you have gained a lot from the illness” (PA).
In this arduous and lengthy process, patients expressed a need to “hold on,” “serrer les dents,” make efforts, and struggle to constantly adapt, “move forward,” and leave the past behind them.
Participants’ narratives of recovery comprised multiple shifts towards reaching a new equilibrium. For some, a sense of courage, restored dignity, and agency eventually emerged from their efforts to cope. Improving emotional regulation capacities and executive functions helped them regain confidence in their ability to overcome obstacles, to know what was good for them, to reflect about their desires, and even to allow themselves some leisure and risk taking. Awareness of their strengths and weaknesses made it possible for participants to set reasonable goals. Here is an example of a personal decision to choose the day hospital because of the benefits that the participant received: “I also feel free because I am free to go to the day hospital, I don’t have to, and it's me who goes there (…) because it brings me a lot of things” (PF).
While still suffering, participants’ perception that they were improving brought them substantial relief. Most participants associated their perception of progress with a lived experience of reconciliation, of transcending their shame and guilt, and of bridging the gap between their delusions and their dreams or imaginations in a way that all these feelings and thoughts were recognized as belonging to themselves. In the words of one participant: “Recovered is … a better view of everyday life, which was not possible before” (PI).
This long and arduous work on “the self” led to transformations that participants later identified as beneficial maturations and cornerstones of their identity. Their efforts to improve their prognosis evolved through successive experiences: “For me, having recovered is learning to live with what we went through, (…) with what happened, and trying to do something good with it” (PF).
Theme 2: An Evolving Illness Role
Participants referred to their illness and its causation as something outside themselves. They reported experiencing the sudden onset of illness as a rupture, accident, fall, even a catastrophe, that deviated their life from its previous trajectory. Patients understood their schizophrenia as foreign and as deeply disruptive to their sense of self. As one participant put it, their illness was “a moral, psychic, physical disaster, et cetera” (PD).
At the onset of their illness, participants explained their disorder with religion or magic: they perceived it to be intentionally thrust upon them as a Quimbois (spell), an intrusion of the devil or diabolical spirits, an ordeal or divine punishment. This usually was clearly stated: “I don’t really feel schizophrenic, because for me it was not schizophrenia, it was more the Devil who did this to me …” (PE).
Alongside supernatural causes, participants mentioned other external factors such as shocks or trauma, hereditary affective deficiencies, physical and/or emotional abuse, drug abuse, other illnesses, and bad company. They did not see different causal explanations as contradictory.
Participants initially sought out external therapeutic spaces and assistance. To address their illness, they described first looking for outside help, sometimes with the hope of returning to their previous state. All participants turned to traditional magical practices and interventions on occasion. Most, however, also relied on regular prayer and medication. This was described in terms of therapeutic experiences and causal explanations: “A marabout. (…). He got my voices out” (PI); “Despite everything that happened to me, I did well. (…) I think it is thanks to God” (PF).
Participants described the rituals as mysterious and beyond their understanding, which seems to have encouraged them to take a passive role. This is echoed in their approach to medical treatment, which privileged professional discourse, thereby devaluing their experiential knowledge. Participants’ use of different therapeutic modalities provoked tensions. They saw drugs as helpful but as “shooting you” and making you “ababa” (dopey). Participants also expressed doubts about their faith in God during hard times. More generally, participants viewed their magical and religious beliefs as contradicting the medical model, while they also opposed traditional magical rites to religion. This hampered the concurrent use of complementary sources of support: But most of the doctors would tell me “no, that has nothing to do with religion.” So I was against it from the start, (…) I did not trust. (…) Because I didn’t feel listened to. And I wanted to make religion take precedence over everything, and most of the doctors who saw me talk about religion, they did not agree with that (…) that set me against them even more. (PE)
Participants described taking charge of their illness and care, achieving self-determination. In their trajectories, various magical or traditional practices, such as gadé-dzafé, astrology, clairvoyance, and herbal medicine, were intertwined with biomedical care. They did not distinguish sharply between Quimbois, voodoo, and marabout practices. By trial and error, participants learned to explore these systems and to orient themselves towards wellness in a flexible manner, capable of tolerating doubts and double meanings. As one participant put it: “Through this way, I took my personality, my identity, as well as my strength” (PM).
Participants’ attempts to grapple with their illness and diverse techniques of care became more complex as they integrated these into their lives. Gradually, participants came to see it as existing within them, while still attributing its emergence to external causes. This sometimes conflated biomedical and spiritual explanations: “I take it more spiritually; I take it more like a hallucination” (PE).
Participants symbolized their recovery experience as a rite of passage and/or as a growing pain that strengthened their being. Psychotherapy, theories of magic, and idiosyncratic interpretations bolstered participants’ efforts to understand themselves.
As they progressed, they reported experiencing a sense of restored freedom and of having agency in their recovery, while they continued seeking outside help when needed. Knowledge of the illness—aided by psychological education—allowed participants to build personalized strategies (sport, relaxation, creativity, etc.). They integrated medication as an active tool due to its experienced effectiveness in managing symptoms. The ability to deal with lingering symptoms became a source of control, and their faith a source of inner strength, in which they saw submission to God's will as a deliberate choice: “I tend to have an inner conversation with my voices, so I manage them” (PC); “I first took refugee with God to feel protected because I was so scared. Now I feel free. I’m not so constrained (…). I feel free to keep going with Jesus!” (PF). Finally, they learned to value patience as a source of strength, helping them accept an illness they did not choose for themselves.
Theme 3: Rebuilding Identity
Many participants reported experiencing a loss of their sense of legitimacy within the group. Having felt shame about their condition and moral judgment on their actions, some initially dissimulated their illness. In response to what they perceived as negative judgments, many felt the need to adopt a stoic countenance. Some appropriated the stigma, labeling the illness as dangerous, a form of insanity, incurable, or a “whim” and a product of “laziness.” For many, past delinquent behavior was central to this type of representation: “And it made me do so much nonsense that I don’t even want to talk about it because for me this illness, given what happened, it's shameful” (PE).
In addition to periods of social exclusion, all participants described a divergence between their trajectory and that of others, as well as the loss of communal roles, which in turn generated feelings of incapacity or uselessness. They found it difficult to feel comfortable with and express themselves, which prevented bonding. It nurtured a dependence on loved ones mingled with a feeling of oppression, a desire for autonomy, and a fear of abandonment: “I want freedom, I don’t want to be oppressed, I don’t want those around me to call me … (…) the others I can’t let them in because I wouldn’t know how to react to that” (PM).
Some felt guilty about past mistakes, disappointing their loved ones, or causing them pain. Many felt they owed a debt to family and caregivers; this feeling of indebtedness was, for some, overwhelming, while for others it drove recovery. For many, morality and religion structured their recovery, giving meaning to their disorders and helping them to achieve forgiveness and a sense of solidarity. Adopting a position of humility, austerity, patience, acceptance, and tolerance, as valued by the Christian religion, provided participants with some necessary distance between themselves and their grandiose ideas and feelings of failure, while nonetheless limiting their self-esteem. For some, adopting a moral stance becomes a personal identity: “To be myself, for me it is what morality is about … I identified it to my identity” (PM).
Participants reported getting support from a larger collective in the process of reconstructing their identity. The family group guaranteed reliable relationships and material survival. The mother figure, in particular, was strong and reassuring in their narratives, although sometimes intrusive. The figure of the father was more withdrawn, or often absent. For example, some reported that their fathers were rarely present during hospitalizations, while others said that the person they turned to in times of crisis was usually their mother, as they knew she would be more available.
Being in the hospital remained a difficult time for many, although it led to the formation of some satisfying relationships. Outpatient care centers were seen as protective and associated with therapeutic and re-socializing activities rather than with an image of crowded consultation centers. Participants characterized healthcare professionals as supportive, personally invested, and efficient experts: “It was not so much the doctor, the doctors who passed by who healed me you know, it was the Rehabilitation Center with the sociability that there was, there I felt that I was reviving” (PL).
Psychiatrists were a benevolent authority, almost a parental figure, in participants’ accounts, but some participants criticized them for overly brief consultations that focused narrowly on symptoms and medications. For some, psychotherapeutic work with the psychologist was important: The doctor really cared about me. Sometimes I disagreed with him. Sometimes he irritated me (…) but even if I did not see him a lot, I knew I could always rely on him. And this made me feel safer. (PA) I met several psychologists. But I met one who could really understand what I felt. She was patient. I saw her every week. She really helped me to restore my confidence. (PE)
Benevolent ways of viewing themselves helped participants to see recovery as a social and moral posture, valuing their reintegration into the community as well as their rehabilitation. They stressed the importance of proving oneself, to not disappoint others and to be worthy of the help they had received: “I try to pay attention to … the clothes uh, what I think about, what I say, to … to still be uh, poised. To be in … to be also uh, a little uh, to be also uh … interesting” (PJ).
Participants actively sought approval through socially valued investments (caring for others, intellectual or artistic activities, sport, work) or by adhering to predefined patterns (home, family, work).
Participants described creating a space of interplay between the self and the collective, helping them regain legitimacy as social actors. For some, work brought a sense of utility and progression along with autonomy, allowing them to contest their disability status. I feel more stable, more … Better in society. Despite the illness. (PI) When I managed to go back to work, I had at last the feeling I was no longer a burden. If I was able to do my job, was I really disabled? I felt I had turned a corner. (PL) But uh to be what I am, to be free, to be myself, to be … to be, to … to be able to express myself as I want. Always with respect but as I want. Being able to say … Before I didn’t say things, I kept to myself. So I’m proud of all that. (PK)
Discussion
Exploration of the recovery experience of people with schizophrenia in Martinique suggests that they experience a period of intense self-examination, followed by an evolution of their illness role and a need to anchor their new identity to relationships with others. The following discussion points appeared salient to the experience of our participants: social norms and support. We compare them to previous models of recovery reported mainly in studies set in anglophone culture.
A Particular Emphasis on Social Norms and Support in Martinique
Our results were consistent with studies highlighting the importance of social support (Leamy et al., 2011). However, the weight given to the group appeared to be particularly important in Martinique. As in previous studies, our results showed the important role of identity remodeling, regaining control, and allowing self-determination and empowerment in supporting recovery (Leamy et al., 2011; van Weeghel et al., 2019). For the participants in this study, however, these individual-level factors of recovery are part of broader efforts that aim, first and foremost, to achieve social reintegration, with personal transformation coming second. In other words, conforming with a group appeared to be a condition of personal recovery in Martinique. By contrast, previous models of recovery support a disengagement from social norms to establish distance between patients and the stigma associated with their condition. In the “Identity” dimension of the CHIME model, for example, this is seen as a condition for attaining a sense of personal freedom (Leamy et al., 2011; van Weeghel et al., 2019). In our study, participants instead seem to have viewed—albeit with some ambivalence—community standards as a protective framework that could promote both autonomy and a meaningful social role despite the constraints these standards implied. Thus, our research supports collectivist social theories (Hofstede, 2001; Tse and Ng, 2014) and the interdependent self-construal theory (Markus and Kitayama, 1991; Tse and Ng, 2014), which are often considered to be applicable to recovery approaches across cultures (Tse and Ng, 2014).
Some participants justified the rejection they experienced as resulting from their previous lack of respect for social norms and morals, which they identified as characteristic of schizophrenia. Such transgressions included delinquent behavior, drug use, physical attacks, adultery, or upsetting their parents. Some of spoke of these as “sins” with reference to Christian morality, and many expressed a strong identification to social or Christian moral values. Our results thus suggest that recovery in Martinique requires accountability for faults and re-appropriation of community values—moral and/or religious—with a redemptive aim. Shame, guilt, and debt, although elicited by and sustaining the internalization of stigma, also seemed to be experienced as structuring and driving forces in a dynamic of repair, suggesting that these feelings are a mode of expression of moral values. However, this stance also led some participants to feel a lack of legitimacy in managing their recovery. For instance, despite having a deep understanding of their illness, they still felt less capable than their caregivers of taking control of their own well-being. As a result, they took longer to embrace empowerment and experiential knowledge in their recovery journey. This appeared to promote reliance on external strategies, postponing the utilization of their internal resources.
Freeing oneself from stigma seems to be an essential stage of recovery in the French (Koenig, 2016) and anglophone (Goffman, 1963) contexts. However, its internalization seemed deeply entrenched among the Martinican participants in our study, even at an advanced stage of their recovery. The internalization of stigma has been reported as a barrier to recovery by lowering self-esteem and hope (Link et al., 2001; Yanos et al., 2008), self-efficacy (Kleim et al., 2008), and confidence in one's ability to take part in social interactions (Perlick et al., 2001). Authors have identified various strategies to reduce the impact of discrimination and social stigma on recovery: community-level initiatives influencing the behavior and attitudes of the general public; supporting people throughout their recovery journey to support their ability to resist reactive self-deprecation; and identification of certain harmful professional practices to promote destigmatizing approaches (Corrigan and Phelan, 2004; Kondrat and Teater, 2009). These strategies could be adapted to respect the cultural, moral, and religious values of Martinique.
Most participants reported “distanced” strategies for connecting with other people at an advanced stage of their recovery. This ties in with techniques of “positive withdrawal” (Corin and Lauzon, 1992) or the avoidance of overly exposing relationships (Leamy et al., 2011), which have been described in accounts of people with schizophrenia from the U.S. (Davidson, 2003). These allow individuals to frequent public spaces—a way of “being with”—while limiting overly complex social interactions (Corin and Lauzon, 1992; Davidson, 2003). Work on resilience in Martinique (Laguerre, 2014) suggested the potential use of “avoidant coping” as a valuable strategy. Such “emotionally centered coping” aims to “regulate emotional distress,” and differs from “vigilant coping” which aims to “manage the problem” (Laguerre, 2014). The internalization of stigma could also favor this strategy (Yanos et al., 2008). Furthermore, considering that stigma internalization may be present until late in the recovery process in Martinique, it might be relevant to ask what people really experience as stigma. In other words, people may transform their stigma experience in a singular way that departs from the original definition of stigma, and which helps them develop useful recovery strategies.
More recent work emphasizes “feeling secure” as a factor of recovery (van Weeghel et al., 2019), with reference to the “secure base” in Bowlby's attachment theory (Bowlby, 1981). This denotes the possibility of being reassured when a person feels threatened, thus allowing children—and even adults—to freely explore the world, especially relationships with others, without reactivating fears (Fraley, 2019; Simpson and Rholes, 1998). This secure base-centered approach tempers an emphasis on factors such as courage and controlled risk in the recovery process (Deegan, 1988). Participants in this study reported that the encouragement of loved ones, caregivers, and peers has supported them in their recovery, highlighting the importance of “therapeutic input” (Stuart et al., 2017) in the recovery process. While “distance strategies” can be protective in individuals’ broader interactions, receiving support from close relatives, peers, and caregivers can help personal recovery. Likewise, respecting community standards, as part of a social contract, seemed to provide security to participants.
Reconciling Plural Therapeutic Approaches
Laguerre identified “religious spirit” as a key factor of resilience in Martinique (Laguerre, 2014). Religion also helped many participants in our study give meaning to their experience. This does not, however, seem to be a way of overcoming stigma, as participants did not report seeking God as a means of being forgiven, or absolved from responsibility, for their illness. Participants do not seem to find the three common causal explanations of illness—Quimbois spells, divine or diabolical ordeals, and individual vulnerability factors—to be contradictory. The diversity of responses these entail seem to promote a flexible approach, and play a role in the remodeling of identity and self-determination. This process of being able to combine therapeutic approaches was seen as a “rite of passage” that strengthened individual maturation and spirituality, independently of religious community practices. Descriptions of this process echo those of “personal growth” by overcoming negative trials (Koenig, 2016).
This pluralism is consistent with representations of identity in the West Indies, which is composed of distinct elements that are interlinked but not completely homogenized (Delisle, 2008; Eynaud, 2015). Some authors associate this identity with a process of “creolization,” 1 following Edouard Glissant's conceptualization of a “rhizome identity” 2 or “identity-relation” 3 (Glissant, 1997, 2020), drawing on the work of Gilles Deleuze and Félix Guattari (Deleuze and Guattari, 1987). “Normality” reconciles multiple cultural representations that can be found, for example, in the pluralism of worship and care (Eynaud, 2015).
However, while the use of traditional healers is widely practiced in Martinique (Bougerol, 2008; Eynaud, 2015; Massé, 2002), it is denounced by the Catholic Church (Delisle, 2008) and invalidated by the Anglo-European biomedical model (Eynaud, 2015). Participants described feeling torn between contradictory messages, and devaluing their own capacity to navigate different approaches. Opposition to therapeutic pluralism can postpone recovery. The complementarity of popular, traditional, and biopsychosocial therapeutic approaches (Kleinman, 1980) seems to be consistent with the personal recovery paradigm's prioritization of lived experience perspectives rather than practitioners’ predefined categories (Anthony, 1993).
Martinique's recent Territorial Mental Health Program does not recognize the value of religious and traditional healers’ impact on patient recovery. Our research highlights a need to consider how plural elements of recovery provide overlapping and complementary contributions to patients’ care. This might lead, for example, to health professionals discussing the potential advantages of alternative approaches with individuals for whom they might be meaningful (Mouchenik, 2019). It might also include inquiring about patients’ beliefs and affirming their responses empathetically (Mouchenik, 2019). Professionals might also explore potential interactions between—without imposing a hierarchy on—the medications prescribed by different practitioners. They might even facilitate connections with healers that patients perceive as vital for their recovery, thereby adjusting treatment plans (particularly in cases where conflicting approaches arise) (Mouchenik, 2019). Certain clinics have established transcultural consultations designed specifically to address the cultural aspects of health (Kirmayer et al., 2023; Mouchenik, 2019).
Taking Trauma into Account
Participants in our study described the onset of illness as a sudden rupture—often using hyperbolic terms such as “inhuman,” “disaster,” and “hell”—that overwhelmed their capacities for control. This has traumatic effects that persist, manifesting in hypervigilance among some participants, beyond the residual persecutory symptoms of schizophrenic experiences of paranoia and delusion. This traumatic dimension has been recognized in the recovery literature (Ellison et al., 2018), while the comorbidity of Post-Traumatic Stress Disorder with schizophrenia has also been documented (Seow et al., 2016). Moreover, people with psychosis have an increased prevalence of traumatic experiences in their early childhood compared to the general population (Varese et al., 2012).
Authors have suggested a link between the pluralistic construction of Martinican identity and cultural ways to provide meaning in life as being linked to resilience in the face of adversity—(to survive in slave plantations, for example) (Glissant, 1997). This suggests that both traumatic elements and modalities of resilience have influenced Martinican identity. The violent psychotrauma of slavery, with its physical aggressions (transport, whips, irons, etc.) (Pétré-Grenouilleau, 2006) and psychological torture (separations, identity ruptures, etc.) (Charles-Nicolas, 2018; Wiltord, 2018), has been linked to cerebral effects on memory encoding and stress regulation (Charles-Nicolas, 2015, 2018). Various studies have shown that serious psychological trauma, without therapeutic support, is transmitted to subsequent generations (Miljkovitch et al., 2004; Tarabulsy et al., 2005; van IJzendoorn, 1995). There has been little collective reckoning of this history in Martinique (for example, through official apologies, reconciliation processes, restorative justice, etc.) (Laguerre, 2014), making it difficult to overcome dehumanizing physical and psychological humiliations and abuse (Charles-Nicolas, 2018; Wiltord, 2018).
Thus, various processes—transgenerational, developmental, and experiential—might contribute to psychological trauma in individuals dealing with schizophrenia in Martinique,
intertwining in distressing resonances with one another. Taking these processes into account—with the resulting specificities of identity building—seems essential to support these individuals in their recovery.
The Role of Employment, Housing, and Financial Autonomy in Social Recognition
Participants in our study stressed the importance of having a job, housing, and financial autonomy in order to build a new equilibrium. They presented these as essential conditions of social recognition and reintegration, and thus as factors of recovery. This is consistent with studies showing that access to a job reduces symptoms (Burns et al., 2009). For some authors, the degree of clinical and social recovery is more highly correlated with socioeconomic factors, such as work, than with progress in treatment (Warner, 2004). Access to paid and voluntary employment extends social networks (Rüesch et al., 2004). Consistent with our participants’ testimonies, having a job has also been found to affirm an active and committed identity, rather than that of a passive patient, stimulating in turn a feeling of belonging (Borg and Kristiansen, 2008). In line with the weight of social judgment in participants’ recovery, as described above, these external criteria appeared to be more important to them than symptomatic remission such as the disappearance of voices.
These findings challenge the paradigm according to which symptomatic remission must be secured before addressing socio-economic factors. Recently, interventions have supported an inverse approach, such as “housing first” (Kirst et al., 2020; Laval and Estecahandy, 2019). These recognize the structural barriers faced by individuals with mental disorders in accessing employment and housing (Corrigan et al., 2004). Such interventions were included in the Territorial Mental Health Program in Martinique (ARS, 2020).
Strengths and Limitations
To our knowledge, this is the first study reporting on the recovery experience in Martinique, according to the criteria of the COREQ32 (SI 1). Our methodology allowed in-depth exploration, appropriate to the phenomenon under investigation. However, the study's qualitative approach limits the generalizability of our findings. Moreover, due to the framework of our methods, we cannot assert having achieved data saturation. Additionally, the multicenter recruitment was confined to individuals who volunteered and were motivated to take part in extensive interviews delving into personal and intimate emotions and thoughts.
Furthermore, the medical background of the principal researcher, along with the influence of French metropolitan culture, may have affected the data collection process by unintentionally discouraging critiques of care, such as the denunciation of an overly paternalistic approach in psychiatry, which might have been expressed with a non-medical interviewer. This might have rekindled power dynamics in the doctor–patient relationship while amplifying the dominance of metropolitan culture. Finally, ethical considerations constrained our ability to directly obtain feedback from participants. Notably, individuals with schizophrenia were not part of our research team. Consequently, despite our endeavors to diversify our research team's composition, all data analysts were professionals who lacked firsthand experience with schizophrenia and interpreted its recovery through the perspectives of those who study it, rather than those who live it. The insights of caregivers and healthcare professionals closely involved with our participants were also absent, a measure taken to limit externally imposed views and attitudes in favor of empathizing with the unique experience of individuals with schizophrenia.
Conclusion
This exploration of the recovery experience among individuals with schizophrenia in Martinique indicated that those grappling with the condition undergo a phase of profound self-reflection, a transformation of their illness-related role, and a requirement to ground their emerging identity in connections with others. These initial results suggest the value of different approaches to aid recovery: benevolent and regular support from relatives, peers, and care providers to strengthen individuals’ secure base; valuing their experiential knowledge; support for psychological trauma; fighting against the stigmatization of schizophrenia in Martinique while respecting traditional cultural, moral, and religious values; social support for work and housing empowerment; and recognition of and respect for the complementarity of the biomedical, religious, and traditional health care sectors.
Future research can explore the validity of our findings and extend them to better support recovery-oriented practices in several key ways: incorporating individuals with mental disorders into the research team; conducting participant recruitment that simultaneously includes individuals with schizophrenia, their primary caregivers, and healthcare professionals (triangulation); and testing the results across a broader sample of individuals with schizophrenia in Martinique. This could involve translating our findings into “patient-reported outcome measures” (Churruca et al., 2021) across the three dimensions indicated by our findings that can be used both for research and clinical outcome evaluation. Finally, recovery outcomes among individuals with schizophrenia could be compared to those with other types of mental disorders (such as eating disorders) in Martinique. This comparative approach can clarify cultural differences that may be present across mental disorders.
Supplemental Material
sj-docx-1-tps-10.1177_13634615261446908 - Supplemental material for Personal Recovery of People with Schizophrenia in Martinique: A Qualitative Study
Supplemental material, sj-docx-1-tps-10.1177_13634615261446908 for Personal Recovery of People with Schizophrenia in Martinique: A Qualitative Study by Coralie Bourzeix, Manon Salvetax, Christelle Samot, Julie Gilles De La Londe, Jean-Sébastien Cadwallader, Marie Koenig, and Marie-Aude Piot in Transcultural Psychiatry
Footnotes
Acknowledgements
The authors would like to thank all the participants for their trust and their rich testimonies. The authors also thank the User Associations (Tombolo Association, Equinoxe Association), the Service User Centers (Klarté Association, Limiè Association, Difé Association), the Martinican Hearing Voices Movement—and all the health and research teams who supported the recruitment and data collection—the Adult Day Hospitals of Lamentin, Perrinon, and Trinité, the consulting centers of Rivière-Salée, Saint-Pierre, Perrinon, Sainte-Marie, and Le François; the Doctor Labyt office and the Anse Colas Clinic. The authors additionally thank the Institute Mutualiste Montsouris, 42 bd Jourdan, 75014 Paris, involved in the funding of the manuscript translation, especially Prof. Maurice Corcos for supporting the research; and Dr. Rémy Slama and Mrs. Ariane Fonsat for authorizing the research to be carried out at the Maurice Despinoy Hospital Center. Finally, the authors thank Mr. Olivier Weiss and Mrs. Claire Bourzeix for reviewing the English translation for errors.
ORCID iDs
Ethics Approval
We received ethical approval from a Parisian Institutional Review Board (Comité de Protection des Personnes Ile de France X; Number ID RCB: 2018-A02858-47) before beginning the study. The information sheets and consent forms contained a number of elements; in particular was the risk of triggering emotions—anger and sadness, for example—further questions, and reactive behaviors (e.g., self-harm). Prior to recruitment, participants were assured that they would have access to rapid care and support in the event of such experiences.
Author Contribution Statement
Coralie Bourzeix: Conceptualization, Methodology, Software, Formal Analysis, Investigation, Data Curation, Writing—Original Draft, Visualization.
Manon Salvetax: Formal Analysis, Data Curation.
Christelle Samot: Validation, Formal Analysis, Resources.
Julie Gilles De La Londe: Validation, Writing—Reviewing & Editing.
Jean-Sébastien Cadwallader: Validation, Writing—Reviewing & Editing.
Marie Koenig: Validation, Writing—Reviewing & Editing.
Marie-Aude Piot: Conceptualization, Methodology, Formal Analysis, Writing—Reviewing & Editing, Supervision, Project Administration, Funding Acquisition.
Funding
Funding source: Institut Mutualiste Montsouris, 42 bd Jourdan, 75014 Paris.
Involved in: Financing translation of the final manuscript.
The funding source has no involvement in: study design; collection, analysis, and interpretation of data; writing of the report; decision to submit the article for publication.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Although recordings and transcripts of qualitative semi-structured interviews were anonymized, their content remains highly sensitive and intimate. Data collected can be shared with reviewers upon request to the corresponding author. It cannot be shared in open access for ethical reasons.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.