
Abstract
In an increasingly diverse world, it is important for mental health professionals to be familiar with symptom presentations from a variety of cultures, including cultural concepts of distress. This study aimed to evaluate how U.S. clinicians diagnosed two cultural concepts of distress—hwa-byung and ataque de nervios—and whether the clinicians’ cultural values or competence influenced their diagnosis. A sample of 84 mental health professionals viewed three case vignettes in random order depicting hwa-byung, ataque de nervios, and Generalized Anxiety Disorder. The clinicians provided an unprompted free-response diagnosis and a forced-choice diagnosis from a predetermined list for each vignette. Clinicians provided a wide range of diagnoses for the hwa-byung and ataque de nervios vignettes, with only a minority of participants correctly labeling the cultural concepts of distress. Prompting diagnoses by providing a list of options improved the likelihood of selecting a cultural syndrome. The most common mental health diagnoses selected did not adequately capture the symptom profiles of the cultural concepts of distress. Clinicians appeared to be more familiar with Latinx cultural presentations than East Asian. U.S. clinicians could likely benefit from additional training and exposure to varying cultural presentations of psychopathology. Labeling a cultural syndrome with a psychiatric diagnosis may lead to decreased rapport and insufficient or ineffective treatment options.
An understanding of cultural variations in presentations of psychopathology is vital for clinicians treating individuals of diverse backgrounds. Some individuals may not present the same symptoms or in the same manner as patients with whom a clinician is more culturally familiar (Ventriglio et al., 2016). Currently, clinicians in the U.S. are more likely to encounter a patient who has ties outside of their cultural group than in the past. In fact, the U.S. Census estimates that 13.5% percent of the national population is foreign born (for the 2014–2018 period) and these numbers continue to rise (U.S. Census, 2019). However, available demographic data from the American Psychological Association (2022) estimate that 80.8% of U.S. psychologists identify as White. Cultural concepts of distress like hwa-byung and ataque de nervios do not fit the models of psychopathology represented in psychiatric diagnostic systems (Choi & Yeom, 2011). This study aimed to investigate how U.S. clinicians might diagnose cultural concepts of distress in their practice. We hoped to learn more about how clinicians in the U.S. conceptualize unfamiliar symptoms to better understand how cognitive representations of disorders may affect understanding of varied forms of psychopathology.
Psychopathology is expressed differently across cultures, as demonstrated by research on culture-bound syndromes (DSM-IV), cultural idioms of distress (DSM-5) and culture-specific disorders (ICD-10) (Choi & Yeom, 2011; Iwata et al., 2011). Cultural concepts of distress include cultural syndromes, that is, reoccurring patterns of symptoms, behaviors, and troubling experiences found in specific societies or cultural contexts that may or may not overlap with a formal diagnostic category (Guarnaccia & Rogler, 1999). The linkage of cultural concepts of distress to a particular geographic region or culture has led some to characterize them as less “real” due to their lack of universality (Cooper, 2010). Yet many authors have suggested that some cultural concepts of distress represent unique conditions worthy of their own classification, and that the localization of a disorder does not alter its “realness” (Balhara 2011; Cooper, 2010; Levine & Gaw, 1995). While referencing such concepts of distress as “cultural” can usefully distinguish them from psychopathologies defined in psychiatric nosology, this creates a false dichotomy that implies that psychiatric disorders are not embedded in a complex network of cultural meanings and epistemologies. Nevertheless, biomedical conceptualizations of psychopathology maintain a symbolic default position in psychiatric research, and the implicit hierarchies generated by this assumption need to be addressed as operating within a dynamic, and often problematic, system of colonial influences, both historic and contemporary. As others have acknowledged, “western psychiatry is in itself a cultural product that cannot be assumed a priori to have universal application” (Kong et al., 2023, p. 430).
There is empirical evidence of high levels of overlap between cultural syndromes and diagnostic criteria for psychiatric disorders (Guarnaccia & Rogler, 1999; Guarnaccia et al., 2005). This suggests that some cultural concepts of distress are similar to specific biomedical diagnostic counterparts, i.e., they are variations in presentation caused by culture. Even in cases of overlap, however, the correlation is not one-to-one, and a similarity in symptoms cannot, by itself, prove that two distinct syndromes are, in fact, a single syndrome presenting differently (Guaranaccia & Rogler, 1999). The idea that cultural concepts of distress are simply variants of psychiatric disorders has been criticized as implying that the disorders in psychiatric nosology are “pure” or “less culture-bound” than other disorders without strong evidence for this (Cooper, 2010).
The DSM-5 and ICD-11 acknowledge the underlying importance of culture in the classification of psychopathology and of interpreting and communicating deviations from mental health from diverse cultural perspectives (Ventriglio et al., 2016). However, both systems remain firmly attached to biomedical conceptualizations of psychopathology and offer only limited guidance on the incorporation of cultural perspectives. Mental health professionals in the U.S. are most exposed to and familiar with the DSM (First et al., 2018). Since a familiarity and reliance on biomedical interpretations of the classification of psychopathology may situate clinicians in a biomedical interpretive lens, clinicians encountering patients or clients with an unfamiliar presentation of symptoms may not recognize cultural concepts of distress and, instead, impose biomedical diagnostic idioms. For example, clinicians may misdiagnose patients who present in ways that do not align with a biomedical understanding, or, alternatively, may misdiagnose culturally normative behavior as psychopathological (Adeponle et al., 2012; Leseth, 2015). Such misdiagnoses can lead to incorrect or ineffective treatment (Adeponle et al., 2012).
This study utilized two cultural concepts of distress: hwa-byung and ataque de nervios to examine clinicians’ recognition of unfamiliar clinical presentations. Hwa-byung (“fire illness”), described among Korean immigrants in the United States, often manifests with feelings of heat throughout the body and commonly in the epigastrium, an accelerated heart rate, and feelings of anxiousness (Min, 2009). A mental health practitioner who encounters the symptoms of hwa-byung for the first time without prior training may mistake these for a manifestation of generalized anxiety disorder (GAD) with an unusual physiological presentation (American Psychiatric Association, 2013). This can lead to ineffective treatment given that hwa-byung is often tied to feelings of anger and injustice related to unfair social circumstances and interpersonal conflict (Lee et al., 2014). A treatment centered around a GAD diagnosis may therefore not address a core perceived cause of the patients’ distress.
Ataque de nervios is a cultural concept of distress primarily associated with the Spanish speaking populations of the Caribbean (Razzouk et al., 2011). Ataque de nervios manifests as acute emotional distress or agitation, sometimes with uncontrollable shouting or screaming, dissociative experiences (e.g., loss of consciousness), and, in some cases, physical or verbal aggression. Ataque de nervios is often caused by or associated with a stressful event. As with hwa-byung, clinicians unfamiliar with ataque de nervios might mistake it for a dissociative or brief psychotic disorder. This misdiagnosis may result in a treatment that does not address the acute stressor or family conflict.
This study examined how U.S. clinicians recognize and label cultural concepts of distress. The ability of clinicians to accurately diagnose patients from diverse cultural backgrounds is increasingly important. This study aimed to answer the following research questions: (a) Without any structure, how would clinicians diagnose vignettes of patients with hwa-byung and ataque de nervios? and (b) Would clinicians select a diagnosis of specific cultural concepts of distress if these are offered as an option?
Methods
Recruitment
We sent 11,666 invitation emails to psychologists listed in the American Psychological Association (APA) membership directory. Recruitment occurred between December 13, 2020 and December 31, 2020. The emails contained a link to the study in Qualtrics, which is an online survey platform. After indicating their informed consent, we screened participants for our inclusion criteria by asking whether they were seeing clients at the time of the study or were supervising someone who was, and if they were in a career where they diagnose mental health clients. If they fit the inclusion criteria, they were then directed to the survey. The survey took approximately 30 minutes to complete, but there was no time limit. Out of 11,666 emails sent, 826 were returned as undeliverable. A total of 161 participants completed some portion of the survey, and 84 completed enough for data analysis. Participants had the chance to be entered into a raffle for a prize of US $250 or two prizes of US $100. The study was approved by the Virginia Commonwealth University IRB (HM20019782).
Materials & Procedure
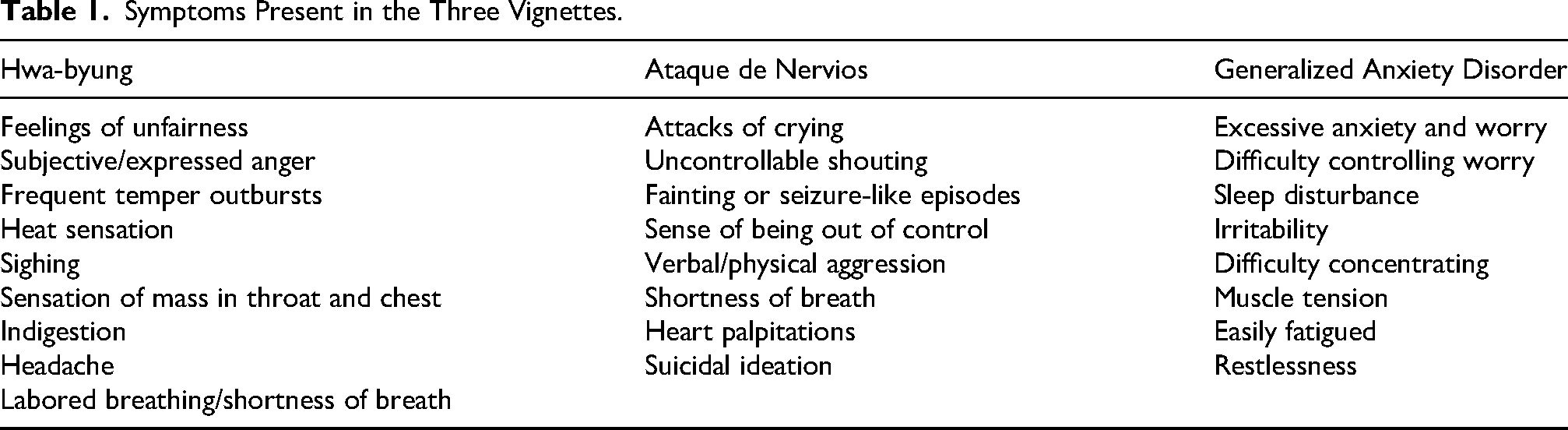
The survey used three vignettes depicting symptoms consistent with Hwa-byung, Ataque de Nervios, and Generalized Anxiety Disorder. Each vignette was constructed to match descriptions of the syndromes from the literature (Min, 2009; Min et al., 2009; Rhi, 2004; Razzouk et al., 2011). Table 1 provides an overview of the main symptoms included in each vignette. All characters in the vignettes were women and of similar socioeconomic status and age. Vignettes were prepared using recommended best practices for vignette studies of diagnostic decision-making (Evans et al., 2015). In order to verify the accuracy of these vignettes, they were pretested by diagnostic experts (n = 6) in psychiatry and clinical psychology with relevant cultural knowledge and experience. These experts confirmed the diagnosis and evaluated whether each symptom was truly representative of the disorder, offering recommendations and edits to the vignettes.
Symptoms Present in the Three Vignettes.
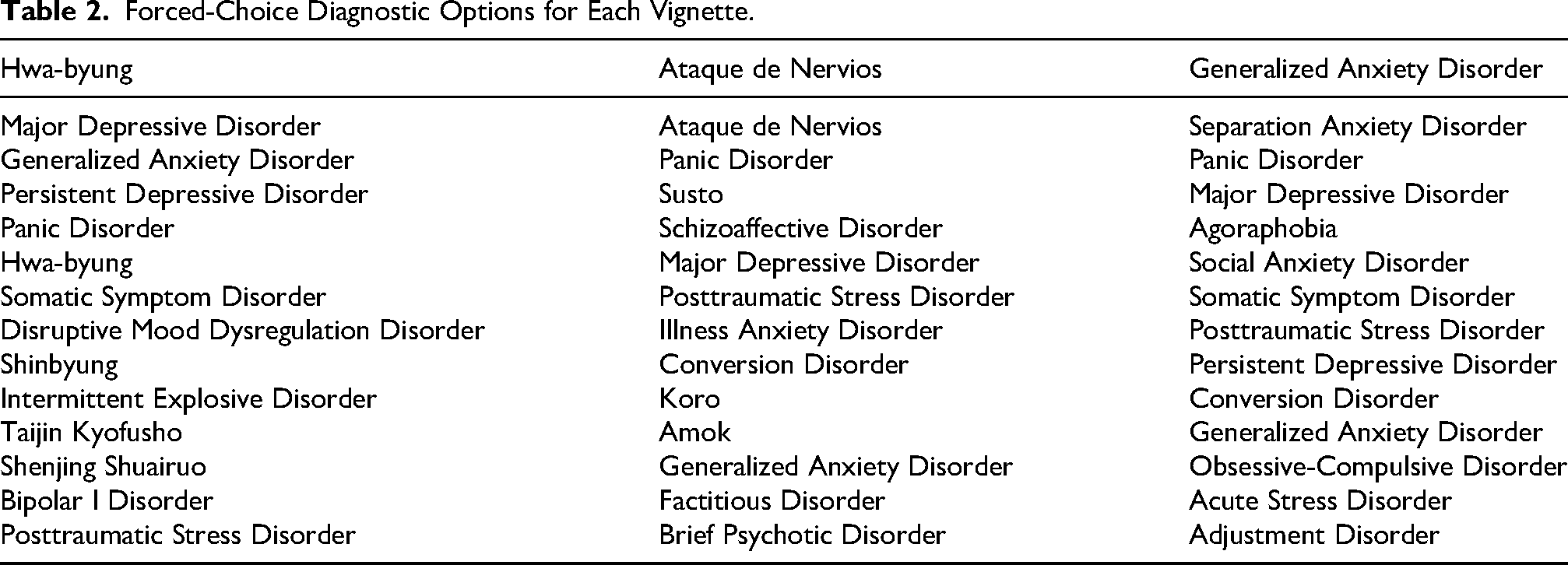
Each participant was presented with all three vignettes in text form, but the order of presentation was randomized. After reading each vignette, participants first offered a free response to the question “What is your diagnosis of the patient presented in the vignette?”. Next, participants were asked an open-ended, free response question about the strategies they used to arrive at their diagnosis (“What strategies did you use to come to your diagnosis, for example, the DSM-5 or ICD-10, your own note taking, etc.?”). After their initial diagnosis, clinicians were asked to select a diagnosis from a pre-set list (“What diagnosis would you give the vignette from the list presented below?”). The diagnostic options included a list of DSM-5 diagnoses and cultural concepts of distress that shared similar symptomatology (see Table 2).
Forced-Choice Diagnostic Options for Each Vignette.
After completing the survey, participants were asked to complete a questionnaire collecting basic sociodemographic data and additional information about their clinical experience, such as years of experience, area of expertise, average caseload, frequency of use of DSM-5 and ICD-10, familiarity with various diagnoses (including cultural concepts of distress), and degree of experience with members of various cultural communities.
Coding Procedure
The content of the free-response questions was independently coded into response groups by two coders (YLC & IL). For the initial diagnosis, participants were free to use any diagnostic terms (not only those included in the DSM or ICD). The coding team created categories based on an initial review of responses. They then independently placed responses into these categories. Note that some participants offered more than one diagnosis, so the number of diagnoses exceeds the number of participants. Coders also independently assessed the consistency between participants’ free-response and forced-choice diagnoses. Responses were counted as concordant if the selected diagnoses overlapped in symptomatology when the diagnostic term was not represented in the forced-choice list. For example, one participant gave the free-response answer of “other specified depressive disorder” and migraines but selected persistent depressive disorder in the forced-choice. Given that their first response included depressive symptoms, the answers were categorized as consistent. Intercoder reliability was assessed at the end of the coding procedure, and the following agreement rate was found for each of the vignettes: Hwa-byung: 95.31%; Ataque de nervios 100.00%, GAD: 94.12%. All discrepancies were discussed until consensus was reached.
Results
Participant Characteristics
The average age of survey participants was 51.1 years (SD = 16.83) and clinicians saw an average of 17.24 clients (SD = 11.18) in a week. Over half (57.63%) identified as a woman and 35.59% identified as a man; one clinician identified as transgender and two clinicians identified as non-binary. One clinician preferred not to disclose their gender identity. The majority of clinicians identified as White (79.69%). One clinician was Latinx, three clinicians were Native American/Alaskan Native, two were Black/African American, and four were South Asian/Asian American. The majority of clinicians were third generation Americans or higher (i.e., both of their parents were born in the United States). Approximately 10% of clinicians were born in another country or had at least one parent who was born in another country. The most common degree type was PhD (69.49%) or another doctoral degree (PsyD, 18.64%; EdD, 3.39%) while 8.47% of clinicians had a Master's degree.
Clinicians reported working in a variety of settings. Approximately one quarter (24.51%) of clinicians worked in outpatient settings while approximately 10% worked in a hospital setting, psychiatric or otherwise, and 30.39% worked in private practice. Another 8.82% of clinicians worked in university settings, while two clinicians worked in rehabilitation facilities. Telehealth best described the setting for 17.65% of clinicians. Approximately half the clinicians (47.72%) worked with adults between the ages of 18 and 64 years old, while approximately a quarter of clinicians worked with children/adolescents under the age of 18 or older adults (25.69% and 26.61%, respectively). Clinicians had a wide range of years of experience, with approximately one-third of clinicians (32.20%) having between 1 and 10 years of experience, 22.03% having between 11 and 20 years, 18.64% having between 21 and 30 years, 18.64% having between 31 and 40 years, 6.87% having between 41 and 50 years, and one clinician having more than 50 years of experience.
Approximately one-third of clinicians had between 1 and 10 clients, while a second one-third of clinicians saw between 11 and 20 clients. Another 28.81% of clinicians saw between 21 and 30 clients. One clinician had between 31 and 40 clients and one clinician had between 61 and 70 clients. Clinicians were asked to report on sources of diversity training they have experienced. While 12.66% of clinicians reported that they had little to no diversity training experiences, the majority of clinicians reported having had at least one diversity training experience. The most frequently endorsed source of training was through work experience (18.99%); other sources were reading/writing (6.33%), personal experience (8.86%), teaching courses (5.06%), community outreach (3.80%), clubs/groups (5.06%), diversity committees (2.53%), research (5.06%), additional training (13.92%), workshops/lectures (11.39%), peer consultation (5.06%), and continuing education credits (1.27%).
Clinicians were asked to report on the cultural populations, if any, with which they had experience working. Notably, 69 clinicians (82.4%) had experience working with clients from an Asian cultural background and 38 clinicians (45.24%) had experience working with clients from a Latinx/Spanish Origin background. A full overview of these experiences is available from the authors upon request.
Diagnostic Selection
Free-response questions
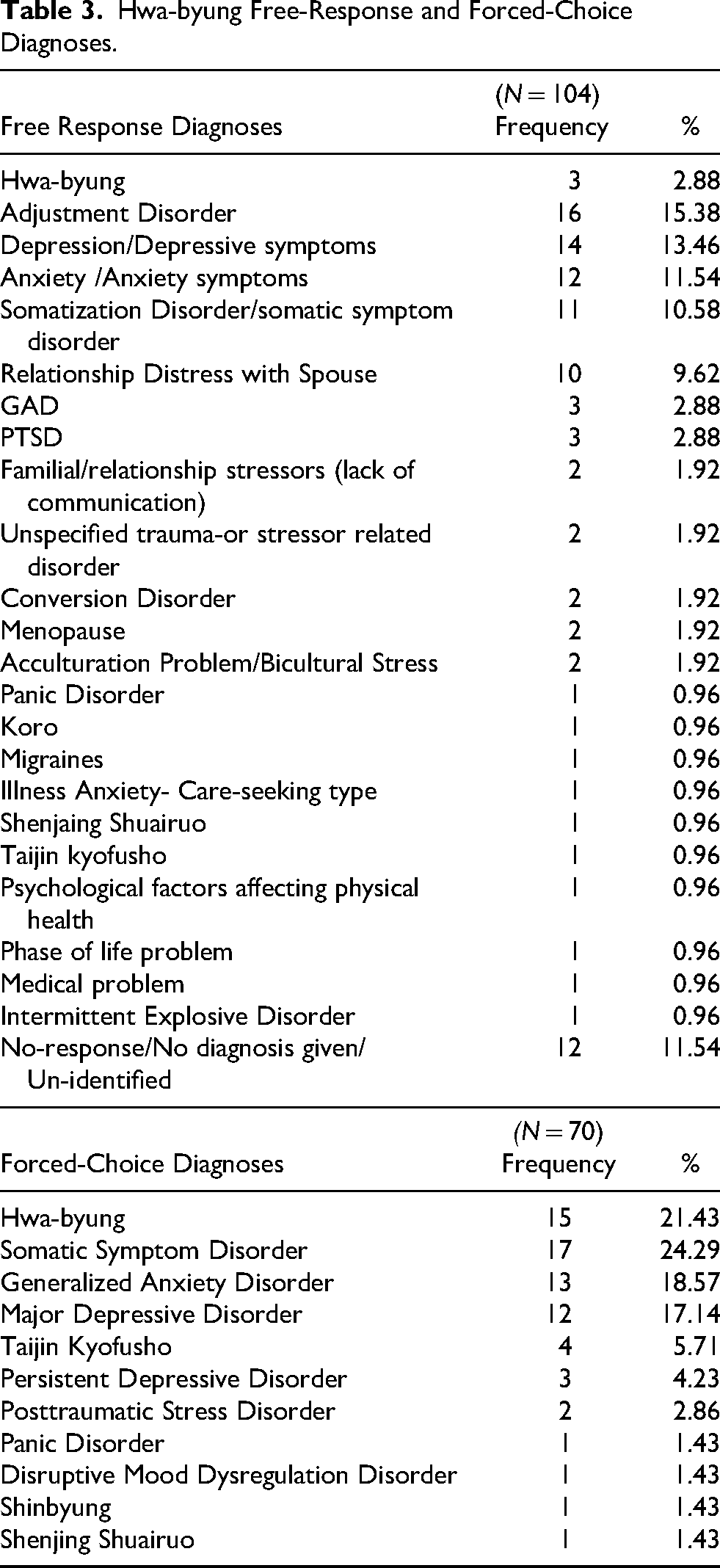
It is important to note that the sample size is referring to the number of diagnoses involved in the analysis. Only 2.88% of free-response diagnoses were hwa-byung for the hwa-byung vignette (Table 3). Participants offered a wide range of diagnoses for this vignette. Out of the 104 reported diagnoses, 6 were East Asian cultural concepts of distress, only 3 of which were hwa-byung. Some of the other cultural concepts of distress named, such as Koro, are highly dissimilar to hwa-byung. A portion of the diagnoses, 27 (25.96%), reflected biomedical disorders (anxiety/depression) that have a similar symptomology to hwa-byung. The three most common diagnoses were adjustment disorder (15.38%), depressive disorder (13.46%), and anxiety (11.54%).
Hwa-byung Free-Response and Forced-Choice Diagnoses.
For the Ataque de Nervios vignette (Table 4), 8.14% of free-response diagnoses were Ataque de Nervios. The top four most common diagnoses among responses were panic disorder (24.42%), PTSD (20.93%), adjustment disorder (11.63%), and depressive disorder (11.63%). These biomedical diagnoses overlap in symptomology with Ataque de Nervios. None of the responses to this vignette included a cultural concept of distress diagnosis, by contrast with the hwa-byung case.
Ataque de Nervios Vignette Free Response and Forced-Choice Diagnoses.
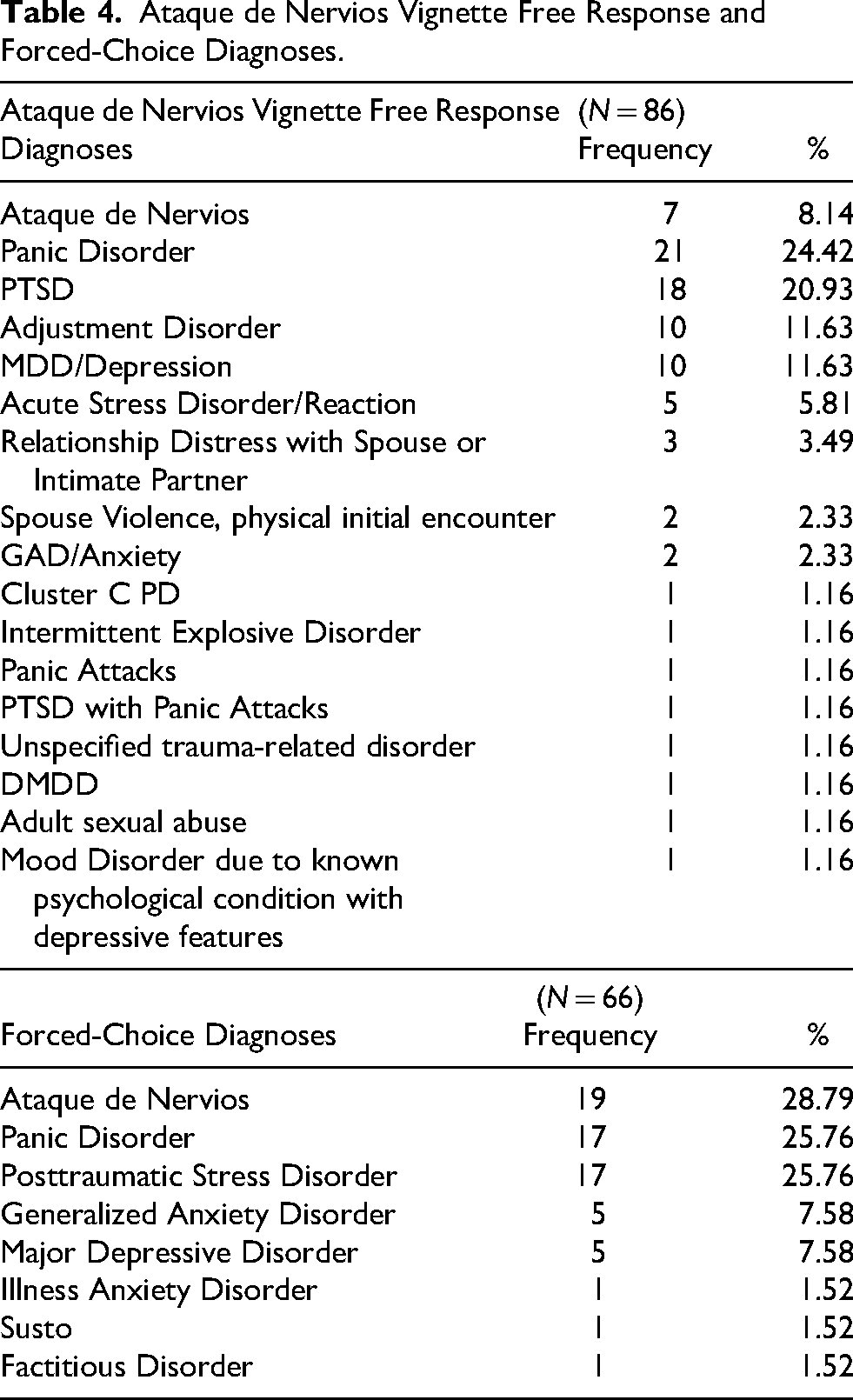
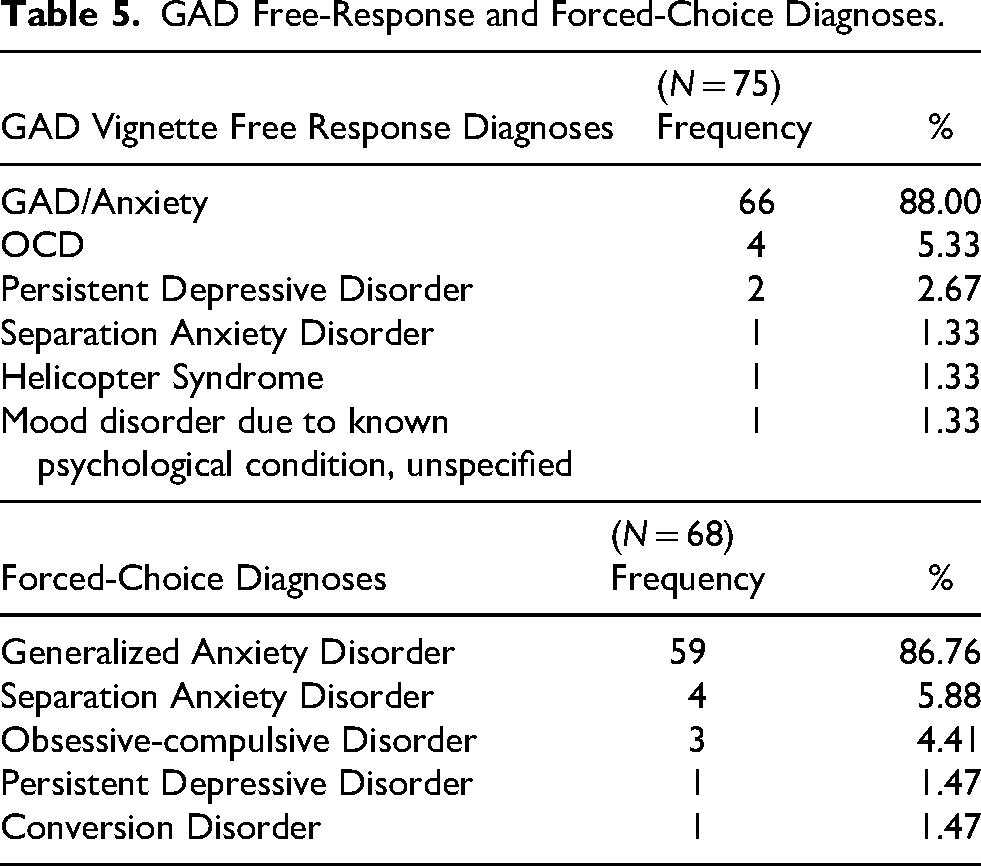
Table 5 lists the diagnoses clinicians gave when presented with the GAD vignette, which was included as a control. A great majority of diagnoses (88.0%) were GAD for this vignette.
GAD Free-Response and Forced-Choice Diagnoses.
There was a significant difference in diagnostic accuracy across the three vignettes, χ2(2, n = 265) = 51.57, p < .001. Responses to the cultural concept of distress vignettes were less accurate than the control GAD vignette: the comparison of GAD and hwa-byung was χ2(1, n = 179) = 133.27, p < .001 and of GAD with Ataque de Nervios χ2(1, n = 161) = 103.10, p < .001. Diagnostic accuracy was not significantly different between the hwa-byung and ataque de nervios vignettes.
Forced choice
For the hwa-byung vignette, the top three most common forced-choice diagnoses selected were somatic symptom disorder (24.29%), hwa-byung (21.4%), and GAD (18.57%), as shown in Table 3. Out of 70 responses to this vignette, 6 (8.57%) selected an East Asian disorder other than hwa-byung.
Table 4 shows the results of the ataque de nervios forced-choice question. The top three diagnoses were ataque de nervios (28.79%), panic disorder (25.76%), and PTSD (25.76%). Only one diagnosis (1.52%) was a cultural diagnosis (susto) other than ataque de nervios.
Table 5 shows the results of the GAD forced-choice question. The leading diagnosis was GAD (86.76%) with few other diagnoses selected.
There was again a statistically significant difference in diagnostic accuracy in responses to the forced-choice question across the three vignettes, χ2(2, n = 214) = 25.66, p < .001.
As with the free-response question, participants were more accurate in their diagnosis of the GAD vignette than of either cultural vignette: the comparison of GAD with hwa-byung resulted in, χ2(1, n = 148) = 68.01, p < .001, and GAD with Ataque de Nervios gave χ2(1, n = 134) = 46.28, p < .001. Accuracy in the diagnoses provided for the two cultural vignettes was statistically equal.
Free-Response and Forced Choice Comparison
The comparison of free- and forced-choice responses highlights several differences. For the hwa-byung vignette, 26 of 59 participants (44.07%) did not change their diagnosis between the questions, while 33 participants (55.93%) did. Among the latter, 15 (45.45%) participants changed their diagnosis from a biomedical disorder to a cultural concept of distress, including 10 (30.30%) who correctly selected the forced-choice hwa-byung diagnosis.
About a fifth of participants (21.4%) selected the correct hwa-byung diagnosis when presented with it as an option. The number of diagnoses of somatic symptom disorder was higher (24.29%) for the forced-choice question than for the free-response question (10.58%). Diagnoses of anxiety disorder increased from 11.54% to 18.57% between the free-response and forced-choice questions. Diagnoses of an East Asian cultural concept of distress other than hwa-byung similarly rose from 2.88% to 8.57%.
For the ataque de nervios vignette, 42 individuals out of 60 (70.00%) did not change their diagnosis, while 18 (30.00%) changed it in response to the forced-choice question. Of these 18, 13 (72.22%) changed from a biomedical to a cultural diagnosis, including 12 (66.67%) who correctly chose ataque de nervios in the forced-choice question. In the free-response questions, panic disorder was the most commonly reported diagnosis (24.42%), but in the forced choice-question, the highest proportion of responses was Ataque de Nervios (28.79%). In the forced choice question, 1.52% of participants selected a cultural diagnosis of Susto while no other cultural diagnosis other than ataque de nervios was given in the free-response question.
The percentage of correct responses to the GAD vignette decreased slightly from 88.00% to 86.76% between the free-response and forced-choice questions. Of 62 responses, 5 (8.01%) changed, of which one (20.00%) was changed for a GAD diagnosis. In the free-response question, the second and third most reported diagnoses were OCD (5.33%) and persistent depressive disorder (2.67%), respectively, while in the forced-choice question, they were separation anxiety (5.88%) and OCD (4.41%).
Discussion
This study aimed to investigate how U.S. clinicians would label or diagnose patients presenting with symptoms of cultural syndromes of hwa-byung and ataque de nervios in comparison with the presumably more familiar presentation of generalized anxiety disorder. We answered this question by eliciting participant diagnoses in response to vignettes, first with an open-ended question and then by asking them to choose from a predetermined list. For hwa-byung, clinicians most frequently diagnosed adjustment disorder (15.38%), depression (13.46%), anxiety (11.54%), and somatization disorder (10.58%) and very rarely provided a diagnosis of hwa-byung (2.88%). The high rate of diagnosis of adjustment disorder could be explained by its categorization in ICD and DSM as a disproportionate reaction to stress (Patra & Sarkar, 2013). Although that could correspond to the patient's social situation, the diagnosis might still be considered inappropriate given that the symptom profile of hwa-byung does not match that of adjustment disorder. The three other diagnoses—depression, anxiety, and somatic symptom disorder—have some overlapping symptoms with hwa-byung, such as somatic symptoms of headache, feeling a mass in the chest, or lump in the throat (Rhi, 2004; Min et al., 2009). Generally speaking, there was little agreement among participants on the diagnosis of this vignette.
This same trend was found for free-response diagnoses of the ataque de nervios vignette, in which clinicians most often diagnosed panic disorder (24.42%), PTSD (20.93%), adjustment disorder (11.63%), and depression (11.63%). These responses could be due to the panic disorder symptoms of feeling out of control, the PTSD symptom of angry outbursts, or the depressive symptom of suicidal ideation, which overlap with those of ataque de nervios; however, these diagnoses would not fully capture the latter. The choice of adjustment disorder for this vignette could also reflect a view of it as a disproportionate reaction to stress, but again, this diagnosis does not fully encompass ataque de nervios, which includes additional symptoms, such as fainting episodes, that could not be explained by any of these disorders.
These results bring attention to a potential cognitive bias that clinicians develop through their training and clinical experience. Clinicians develop their own schemas for common forms of psychopathology that guide the perceptual and interpretive process of diagnosis (Foster et al., 2017). This schematization of psychopathology integrates a network of individual and cultural meanings. As others have noted, because these schemas reflect dominant models in psychiatric nosology based on Western or Euro-American populations, in intercultural situations, they may function as an implicit form of colonial power inscribed in psychiatric nosology (Bemme, 2023).
Clinicians who have not acquired schemas for interpreting cultural concepts of distress may find it harder to retain the unique symptoms involved in the vignettes in this study (Alba & Hasher, 1983). This may lead them to attend to familiar symptoms and ignore or dismiss unique cultural features, resulting in a less accurate diagnosis.
Clinicians’ self-reported average level of familiarity on a sliding scale from 0–100 with Ataque de Nervios was 25.17 (SD = 31.67), whereas the average level of familiarity with hwa-byung was 6.06 (SD = 9.91). This difference may be attributed to the prevalence of Latinx patients compared to those of East Asian backgrounds in U.S. health settings (U.S. Census Bureau, 2019). A more varied range of diagnoses was given for the hwa-byung than the ataque de nervios vignette. Contrary to that possible explanation, a higher percentage of participants reported having worked with East Asian individuals than with those of Latinx descent.
Responses to the forced-choice question yielded higher rates of correct diagnosis for the hwa-byung and ataque de nervios vignettes. This may be attributable to a greater capacity to
recognize rather than free-recall information (Postman et al., 1948). While responses of hwa-byung diagnosis increased from 2.88% to 21.4% between the free-response and forced-choice questions, the most common selection in the latter was somatic symptom disorder, which also increased from 10.58% to 24.29% of responses to each question. Somatic symptom disorder is not as common a diagnosis as depression or anxiety in U.S. mental health practice, and thus may have been less likely to come to mind (Dimsdale et al., 2013; Twenge & Joiner, 2020). In other words, clinicians’ selection of somatic symptom disorder when prompted (but not during free recall) may be an example of the availability heuristic (Tversky & Kahneman, 1973).
Finally, most participants correctly diagnosed GAD in response to both questions. Familiarity and regular experience with GAD could explain this. Furthermore, these results rule out that the possibility that the variability seen in responses to the other vignettes reflects general poor diagnostic practice, or high rates of disagreement in the diagnosis of any given case.
Implications
Based on the findings of this study, we found significant deficits in the ability of clinicians to correctly diagnose cultural concepts of distress, which could lead to diagnostic and therapeutic errors. Developing an awareness of how diagnostic labels function in the dialogic space of a clinical interaction is essential, especially since this interaction operates within complex sets of epistemic politics (Bemme, 2023). Moreover, the typical treatment for a biomedical diagnosis may miss key features of a cultural concept of distress. For example, quite a few individuals diagnosed the hwa-byung and ataque de nervios vignettes as adjustment and depressive disorders. Common treatments for these disorders are unlikely to address the rage and anger created by unfair conditions that are associated with the cultural concepts of distress.
Studies have shown lower rates of diagnostic accuracy for minoritized populations, which might imply a lack of cultural training and conceptualization (Borowsky et al., 2000; Kim et al., 2008; Rivera Mindt et al., 2010). Potential solutions include educating students about cultural concepts of distress through practicums, classes in cultural aspects of psychopathology, or diversity training. Changing the epistemic landscape of clinical conceptualizations of psychopathology, especially transculturally, will take time and consistent attention to the geopolitical ethics of biomedical practice.
Limitations
There were several limitations to this study. The first is the small sample size, which limits the generalizability of findings. The study was also conducted during the COVID-19 pandemic, which affected response rates. Another potential limitation is that the within-participant nature of the study, where participants were presented with all three vignettes, may have led to priming and increases in diagnostic accuracy during later parts of the study since it may have become obvious that the study was centered around cultural differences. This effect was controlled by randomizing the order of presentation of the vignettes; nonetheless, rates of cultural diagnosis may have been even lower if clinicians saw only a single vignette.
Conclusion
The results of this study revealed that U.S. psychologists rarely recognize cultural concepts of distress in case vignettes; instead, clinicians focused on familiar psychiatric symptoms/disorders that are commonly seen in the U.S. This points to the need for more research on the process of attending to cultural symptoms and syndromes in clinical diagnosis and further education of psychologists on cultural concepts of distress to increase diagnostic accuracy for individuals of diverse cultures.
Footnotes
Acknowledgements
The authors would like to thank the participating mental health professionals who volunteered their valuable time to complete this study. They would also like to thank Isabel Li for her valuable contributions to data cleaning and handling.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The data that support the findings of this study are available from the corresponding author, JWK, upon reasonable request.