
Abstract
Following the near-total destruction of mental health services during the Khmer Rouge regime (1975–1979), psychiatry in Cambodia underwent a gradual and resource-constrained revival from the early 1990s onward. This article traces the history of psychiatry in Cambodia from its early institutional foundations in the colonial period, through its collapse during the Khmer Rouge genocide, to its re-establishment and progressive institutionalization in the post-conflict era. Drawing on historical archives, policy documents, and published literature, the paper describes three main phases of development: initial reconstruction and training (1992–2000), expansion of services and education (2001–2015), and recent efforts toward institutionalization and specialization (2015–present). Particular attention is given to the interaction between western psychiatric models and Cambodian cultural frameworks of distress rooted in Buddhism, animism, and community-based healing practices. The article highlights the central role of international collaboration, nongovernmental organizations, and emerging local leadership in shaping psychiatric services, while also documenting persistent challenges including workforce shortages, uneven geographic distribution of care, limited inpatient capacity, and enduring stigma. By situating psychiatry within Cambodia's broader sociocultural and historical context, this review contributes to a transcultural understanding of mental health system reconstruction in post-conflict settings. It also underscores the importance of culturally responsive, community-oriented approaches for sustainable development.
Keywords
After decades of deterioration and neglect under the Khmer Rouge, psychiatry in Cambodia began a significant resurgence in the 1990s. This restoration is attributable to the collaborative efforts of national and international organizations aimed at reconstructing the nation's mental health facilities and infrastructure. Cambodian institutions, supported by international partners, contributed to workforce training, service development, and mental health research. These collaborations created training programs that improved treatment approaches in Cambodia. Nonetheless, despite significant advancements over the years, challenges such as restricted access to mental health services in remote regions and cultural stigma surrounding seeking mental health services persist.
This article initially provides a concise overview of the historical and cultural context within which Cambodian psychiatry exists (see Figure 1). The focus shifts to the destruction of psychiatry under a genocidal regime and its subsequent restoration, outlining the initiatives of local organizations and international collaborators that have enhanced access to care and lessen chimed the stigma associated with mental illness in Cambodian society. The authors also emphasize the significance of community-based efforts and mental health advocacy which have been integrated in local cultural perceptions of mental illness and recovery throughout time.
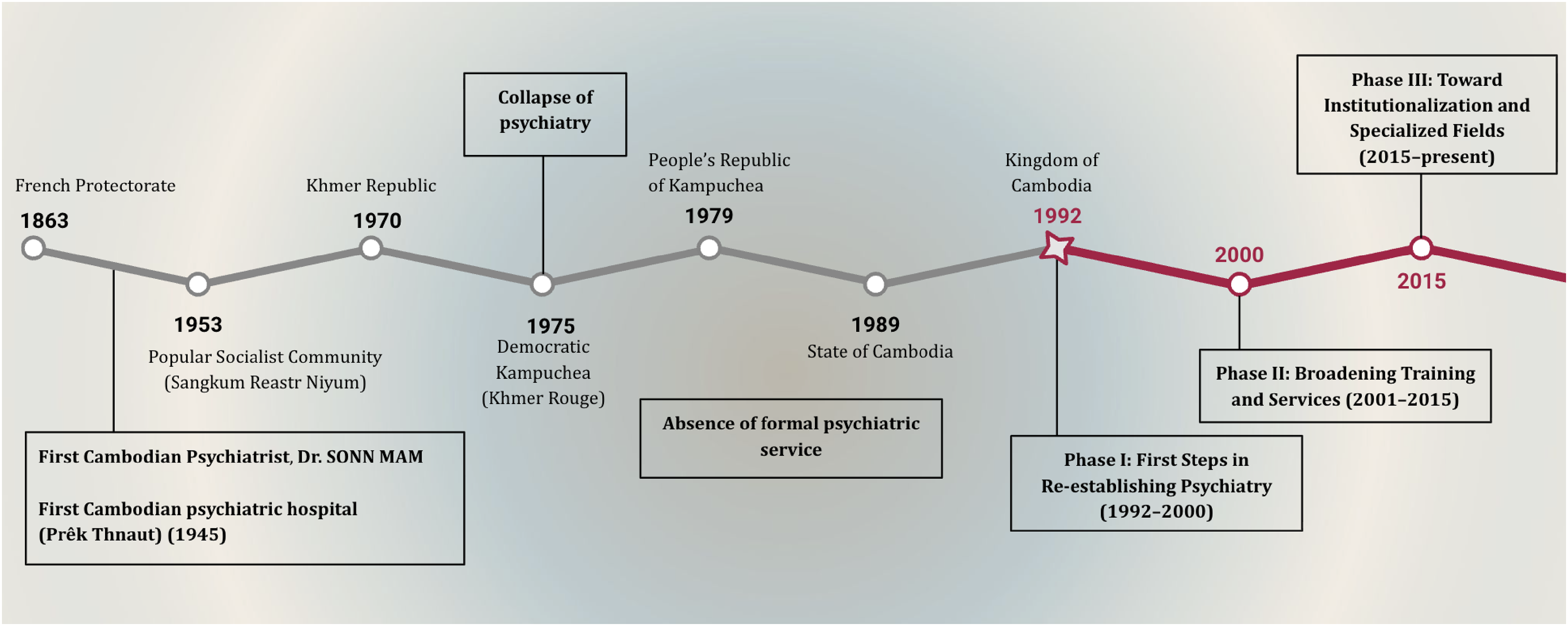
Summarized timeline of history of modern psychiatry in Cambodia. Source: Author.
Context of Psychiatry in Cambodia
In Cambodia, the understanding of illness reflects a complex and diverse system of healing that incorporates elements of beliefs such as animism, Buddhism, and Hindu philosophies. This complexity is thus shown in dialogues that mental illness is a result of natural (imbalances of body elements) and supernatural (spirits, curses, karma, etc.) factors. For instance, concepts like neurosis, psychosis or other psychological distress may be attributed to an individual's past actions leading to karma or unresolved duties to spirits. According to a research paper, interviews with Cambodian monks and healers indeed reveal the importance of karma in explaining suffering (Agger, 2015). Another example, in the case of help-seeking, when people consulted monks, religious or spiritual teachers about their mental suffering, they were often told that their symptoms—including persistent nightmares, anxiety, or “thinking too much”—reflected not only trauma, but also karmic debt that needed to be addressed through meditation and merit-making. When they experienced recurring dreams of deceased relatives who died violently during the war, it would be explained to them that those spirits were unable to find peace because proper funeral rites had not been performed. The recommended treatment would combine meditation practices to calm the mind with rituals where living relatives would transfer merit to the dead after making religious or spiritual offerings, helping the spirits progress toward rebirth. This is why scholars working on Cambodian healing practices for example, documented how healers and clients map illness not only to spirits or immediate trauma, but also to transgressions carried over lifetimes, requiring both psychological and ritual interventions, leading families to seek traditional healers who perform rituals to appease or expel these spirits before considering biomedical treatment (Sareth et al., 2014). Individuals showing signs of psychosis, for example, are typically taken to traditional healers (kru Khmer) or mediums, who perform rituals to expel or appease the spirits believed to be the cause (MacCabe et al., 2007). The words “kru” and “pet” refer to indigenous practitioners and biomedical practitioners, respectively, both of which are derived from Sanskrit terms (Ovesen & Trankell, 2010). These kinds of classifications sometimes overlap because individual healers may play multiple roles within the community.
This preference of traditional healers has been driven not only by the syncretic beliefs that guide expectations for healing, but also by the widespread shortage of health professionals in the country (Guillou, 2009). The paper illustrates in further detail below how the domain of psychiatry was built and expanded within the Cambodian historical timeline—from 1 psychiatrist in 1945 to just over 100 in 2025—and health professionals in general who can offer mental health care also increased in numbers. Psychiatry as a western science therefore did not arrive in Cambodia in isolation; it encountered robust local traditions rooted in long-standing community-based healing systems. As pointed out in the previous paragraph, before the introduction of formal psychiatric institutions during the French colonial period, most mental health care came from families, traditional healers, and monks using cultural and spiritual explanations (Somasundaram et al., 1999). These community-based approaches played a foundational role in shaping and extending formal mental health services as they emerged during the colonial and interwar periods up until the present day.
The Early Foundation in the Field of Psychiatry
The beginning of formal psychiatry in Cambodia can be traced back to establishment of the first psychiatric hospital in 1945, known most commonly as “Prêk Thnaut Hospital” (see Figure 2). This hospital was located in the town of Takhmau, which is now a district in the capital city Phnom Penh. It also became known as “Pet Chhkout Hospital,” “Takhmau Hospital” or “Sonn Mam Hospital,” after Dr. Sonn Mam (1890–1966) a Khmer medical doctor and psychiatrist, who played a primary role in establishing this first formalized psychiatric institution in Cambodia. Before returning to Cambodia in 1940 to lead and design the country's first psychiatric hospital at Takhmau, Dr. Sonn Mam (see Figure 3) studied medicine in Hanoi and Paris and worked in psychiatric hospitals in France and Vietnam, including the Bien Hoa Hospital which opened in Vietnam in 1919. In fact, prior to 1945, Cambodian patients—as part of the Indochinese Union under French colonial rule—were sent to the Bien Hoa asylum as the closest psychiatric facility until Prêk Thnaut Hospital was opened (Edington, 2019). Until his death, Dr. Sonn Mam was the main physician at Prêk Thnaut Hospital, also serving as dean of the Royal Faculty of Medicine and holding government positions such as Minister of Public Health and Minister of Foreign Affairs. His influence reached across borders, with documented cases of families bringing patients from Vietnam and Thailand, from cities including Saigon and Bangkok, to benefit from his psychiatric care (Nécrologie, 1966).

Prêk Thnaut Psychiatric Hospital. Source: Documentation Center of Cambodia (n.d.).

DR. Sonn Mam. Source: Michel Caire (n.d.).
By late 1974, the Prêk Thnaut psychiatric hospital had expanded from a modest staff to a substantial institution, with dozens of doctors including 2 psychiatrists, 50–60 supervisors, and 180 nurses managing 600–800 beds. The team included administrators and occupational therapy assistants. Modern treatments like electroshock therapy were used for severe cases, and the hospital's routines were highly organized. Yet even then, the system faced serious obstacles that would persist for decades. With only one psychiatric hospital for the entire country located just outside the former border of the capital city of Phnom Penh, rural patients faced arduous journeys that could take days and cost more than many families could afford. The hospital's institutional model also created economic barriers—patients needed family members to accompany them and provide food during stays, making hospitalization unfeasible for poor rural families dependent on subsistence farming (Ka, 1998). Most families continued seeking help first from monks and traditional healers rather than the psychiatric hospital, viewing mental distress through the frameworks of karma and spirit possession rather than biomedical knowledge. These obstacles of geographic inequality, workforce shortages, tension between biomedical and traditional healing systems, plus the economic barriers to care that characterized the system in 1974, were catastrophically amplified by the Khmer Rouge and remain core challenges today.
The period from 1975 to 1979 saw the collapse of psychiatric and general healthcare services in Cambodia during the Khmer Rouge regime (1975–1979). There was the deliberate dismantling of medical infrastructure, mass killings (including patients and professionals), and thus a total absence of formal mental health services. The only psychiatric hospital was converted to a prison, and most surviving care shifted back to monks and traditional healers. Even after 1979, restoration of mental health services lagged far behind other health sectors, with refugee camp programs providing minimal support until reconstruction began in the 1990s (McLaughlin & Wickeri, 2017; Pheng, n.d.). Even so, the destruction of infrastructure, the complete rupture in psychiatric expertise and the resulting generational knowledge loss represented enormous barriers for the later rebuilding of mental health care.
Phase I: First Steps in Re-Establishing Psychiatry (1992–2000)
The re-establishment of psychiatry in Cambodia began in the early 1990s, when the Ministry of Health created the Subcommittee for Mental Health in 1992 to coordinate the development of mental health services. In the same year, psychiatry was introduced at the University of Health Sciences with support from Norway, and in 1994 the first specialized training program for doctors in psychiatry was launched. That year also saw the opening of the first outpatient psychiatric department in Phnom Penh (MacCabe et al., 2007). However, the Subcommittee for Mental Health faced immense challenges. At the time of its creation, it had no budget, no advisors, and no specialized staff (Ka, 1998). Despite these limitations, it began working in partnership with nongovernmental organizations (NGOs) and with assistance from the World Health Organization (WHO) office in Phnom Penh. Even though the framework was basic and fragile, the Subcommittee laid the foundation for a systematic approach to psychiatric services and policies in Cambodia.
The early reconstruction of Cambodian modern psychiatry was significantly shaped by the work of Professor Ka Sunbaunat, who chaired the Subcommittee for Mental Health established in 1992 and helped develop the first postgraduate psychiatric training in collaboration with the University of Oslo. Under his guidance, the first National Mental Health Plan (1995–1998) was introduced, outlining priorities for workforce training and the integration of mental health into general health services. He also emphasized community-based approaches, equitable access between rural and urban areas, and the inclusion of basic mental health care within primary health services. Drawing on Cambodian cultural and Buddhist concepts of compassion and mindfulness, Professor Ka promoted an approach that combined professional ethics, respect for human rights, and cultural sensitivity. Under his leadership, these early foundations helped establish the institutional framework upon which later programs and collaborations could develop (Ka Sunbaunat, personal communication, 2023).
Alongside local efforts, international support was critical. A Norwegian professor of psychiatry, Edvard Hauff, launched a five-year education program aimed at rebuilding Cambodia's psychiatric services. Funded by the Norwegian Council for Mental Health and the Norwegian Ministry of Foreign Affairs, with implementation by the International Organization for Migration and academic direction from the University of Oslo, the program had several objectives: to hold a national conference on psychiatric education, to establish an outpatient psychiatric service in Phnom Penh, to initiate a postgraduate training program in psychiatry leading to national certification, and to integrate psychiatric training into the medical curriculum at the Faculty of Medicine (Hauff, 1996).
The first training steps began in 1994, when 10 Cambodian physicians were selected by the Ministry of Health and the Cambodian Mental Health Training Program (CMHTP) to join postgraduate training. That same year, the first psychiatric outpatient service was set up at the Khmer-Soviet Friendship Hospital in Phnom Penh, supported by the Association of Medical Doctors in Asia and the CMHTP (Hauff, 1996; MacCabe et al., 2007). By 1995, the clinic had received 1,209 new cases and recorded more than 11,000 visits (Hauff, 1996). Patients presented with a wide range of problems: long-standing schizophrenia, acute psychosis, and mood and anxiety disorders often linked to poverty and trauma. The clinic thus became a critical site for residents to gain hands-on experience and for patients to access care that had been unavailable for nearly two decades. In 1998, the training program expanded to include 10 additional doctors and 20 psychiatric nurses. Many of these trainees came from outside Phnom Penh, with the aim of extending psychiatric care into the provinces. Although expatriate psychiatrists initially provided teaching, the first Cambodian graduates soon joined the faculty, beginning the gradual localization of training (Savin, 2000). By the end of the decade, the first cohort of 10 trainees had graduated (1998), and a second cohort was already in progress. In addition, about 40 psychiatric nurses had been trained in Cambodia, marking the beginning of a multidisciplinary workforce (MacCabe et al., 2007).
NGOs also played a key role during this formative period. The Marcel Roy Children's Foundation of Canada opened a child mental health clinic in Takhmau in 1994. The Harvard Training Program in Cambodia established an outpatient mental health clinic in Siem Reap Provincial Hospital in 1996 and provided training for 48 doctors and medical assistants the following year. At the same time, the Transcultural Psychosocial Organization (TPO) 1 began community-based mental health programs, drawing on anthropological research into traditional healing and local concepts of mental illness (Eisenbruch, 1990; Somasundaram et al., 1999; Van de Put, 1992). Dr. Chhim Sotheara, Executive Director of TPO Cambodia, later reflected that psychiatry's “rebirth” in 1993 involved the Subcommittee for Mental Health, international support, and the emergence of NGOs such as TPO. According to Dr. Chhim Sotheara (personal communication, 2024), this period laid the foundation for integrating trauma-informed care with community-based approaches, even as resources were scarce. The TPO initiative was particularly significant because it placed community-based care at the center of service development. A “core group” of 12 Cambodians was trained by an expatriate multidisciplinary team, and by 1997 this group had gone on to train 460 community workers, including monks, teachers, village elders, and local health staff (Somasundaram et al., 1999). Clinics opened in district hospitals in Battambang, Kampong Speu, and Kandal, run by local medical staff one day a week with TPO supervision and drug supply. By August 1997, these clinics had treated 839 new patients and recorded 4,342 follow-ups (Somasundaram et al., 1999).
The diagnostic profile reflected both severe psychiatric illness and cultural understandings of distress. Schizophrenia and anxiety each accounted for 18% of cases, psychosis 15%, epilepsy 15%, and depression 14%. Post-traumatic stress disorder, despite the country's history of war and mass violence, was rarely diagnosed (3%). In light of Cambodia's history, mental health research and the work of NGOs have largely focused on trauma-related care. More recently, the need to focus on common mental disorders has been recognized and a number of prevalence studies have been conducted in Cambodia. Significant work has been done to describe syndromes and idioms of distress related to Cambodian culture, particularly with respect to trauma in adults and children. Examples described in Cambodia include baksbat (“broken courage”) (Chhim, 2013), kut chraen (“thinking too much”) (Somasundaram et al., 1999), mour mao (“easy anger”) in children, and khyâl (“wind-like substance”) attacks (Hinton et al., 2010). The importance of contextualized mental health research has been emphasized as crucial to developing accurate diagnostic criteria, effective interventions and appropriate long-term follow-up (Parry et al., 2020).
Many patients came from poor rural households, and women represented nearly two-thirds of attendees. Treatment combined pharmacological and psychosocial approaches. Basic drugs such as chlorpromazine, haloperidol, amitriptyline, phenobarbital, and phenytoin were supplied through local institutes and hospitals, proving effective in stabilizing severe cases. At the same time, counseling, psychoeducation, and culturally adapted relaxation techniques were introduced, drawing upon four traditional methods that harmonized with Cambodian Buddhist and healing practices. These included: (a) mindful breathing or Ana Pana Sati, in which clients practiced rhythmic breathing while repeating the sacred idiom Puthoo (“Puth” during inhalation and “thoo” during exhalation); (b) progressive muscular relaxation adapted from Jacobson's technique, the yogic Shanti or Sava-Asana, and Buddhist mindful body awareness; (c) repetition of meaningful words or verses such as Keatha, Angkam, Puthoo, or Buddhang Saranang Gachchami, similar to Benson's “relaxation response”; and (d) meditation practices including Samadhi and Vipassana, both integral to Cambodian Buddhist traditions. In addition, traditional massage (Thveu Saasay) was used to promote deep relaxation, making interventions both culturally resonant and therapeutically effective (Somasundaram et al., 1999).
Most public institutions and TPO Cambodia increasingly collaborated with traditional healers rather than replacing them, encouraging families to continue drawing on culturally meaningful healing practices while seeking biomedical treatment for conditions such as schizophrenia or epilepsy. Outcomes were mixed: around half of patients improved significantly, but dropout rates were high (nearly 40%), especially for anxiety and depression. Many stopped attending once they felt better or due to distance and cost. The performance of clinics varied: Battambang and Sangke became successful models, while Oudong struggled due to weak staff motivation and competition from strong traditional healing networks (Somasundaram et al., 1999).
By the end of the 1990s, psychiatry in Cambodia had made its first fragile steps toward revival. A small cadre of psychiatrists and psychiatric nurses had been trained, outpatient clinics were functioning in Phnom Penh and several provinces, and community-based programs had begun to integrate western psychiatry with local healing traditions. As MacCabe et al. (2007) note, the destruction of Cambodia's pre-1975 institutional system paradoxically allowed for the adoption of a community-based approach from the outset, without the difficulties of deinstitutionalization faced elsewhere. Resources were still extremely limited and services were unevenly distributed, but these early efforts created the foundations for future development.
Phase II: Broadening Training and Services (2001–2015)
The growth of psychiatric care occurred alongside enduring cultural frameworks that continued to shape how symptoms were expressed and how families approached caregiving. In Cambodia, distress is often expressed through culturally specific idioms rather than western diagnostic labels. For instance, baksbat—literally “broken courage”—describes fear, withdrawal, and loss of confidence following trauma, particularly among survivors of the Khmer Rouge period (Chhim, 2013). Another common expression is khyâl attack (kaeut khyâl), a panic-like episode believed to result from the upward flow of “wind” (khyâl) in the body, producing dizziness, shortness of breath, and fears of death (Hinton et al., 2010). These idioms illustrate how suffering is explained and treated within local ethnomedical frameworks that blend Buddhist, animist, and biomedical ideas (Somasundaram et al., 1999).
Dr. Chhim Sotheara emphasized in an interview that traditional healing practices remain central to how Cambodian communities interpret and respond to psychological distress. He explained that many of these practices coexist with biomedical approaches, shaping the way families first seek help. Consistent with earlier observations by Somasundaram et al. (1999), he distinguished between helpful and harmful practices. Helpful practices such as meditation, chanting, and ceremonies led by monks provide comfort, reinforce social support, and help restore moral and spiritual balance. By contrast, harmful practices involve coercive or stigmatizing responses, including forced exorcisms, prolonged confinement, or physical restraint, which may endanger patients and delay access to appropriate care. To address this, TPO Cambodia trained community workers, monks, and traditional healers to recognize mental health problems, manage them safely, and refer patients when needed. This approach, grounded in community participation and cultural sensitivity, aimed to reduce harm while preserving meaningful traditional resources that support healing and recovery (Somasundaram et al., 1999).
From the early 2000s, training and services expanded, with local institutions gradually assuming responsibilities that external partners had initiated in the 1990s. After the joint Oslo–Phnom Penh program concluded in 2004, the University of Health Sciences (UHS) took over residency training in 2005; psychiatry was also embedded in the undergraduate curriculum to ensure basic exposure for medical students (Chhim, 2017; Olofsson et al., 2018). This transition reflected a broader recognition of the need for sustainability and national ownership, because reliance on donor-led initiatives was no longer viable. Momentum for this shift came from both the Ministry of Health's growing commitment to institutionalize mental health education and the efforts of Cambodian psychiatrists trained under earlier programs who advocated for integrating psychiatry within the country's medical education system.
Service delivery broadened beyond Phnom Penh, primarily through ambulatory and community-based care. By 2013, the Ministry's program reported 37 mental health clinics in referral hospitals and 172 in health centers, although only a few had short-stay beds for acute admissions (Chhim, 2017). Inpatient capacity remained limited, with approximately 15 psychiatric beds nationwide—equivalent to 0.10 per 100,000 population—mostly concentrated in Phnom Penh and a few provincial hospitals. Governance structures also evolved during this period.
The Subcommittee for Mental Health, established in 1992, initially coordinated national mental health activities under the Ministry of Health. Around 2002, this structure evolved into the National Program for Mental Health, expanding oversight of training and service delivery. In 2007, the Bureau of Mental Health was created under the Department of Hospital Services to strengthen implementation across referral hospitals and health centers. The most significant milestone came in 2014, when the Department of Mental Health and Substance Abuse (DMHSA) was officially established within the Ministry of Health, providing a permanent institutional framework to lead coordination, capacity building, and partnerships with NGOs (Department of Mental Health and Substance Abuse, 2023).
Despite significant efforts during the 2000s to expand psychiatric training and community services, Cambodia's mental health system remained fragile. Between 1994 and 2004, international collaborations with the IOM and the University of Oslo produced 26 psychiatrists and about 40–45 psychiatric nurses, while around 600 primary-care providers completed short mental health courses. When external support declined, psychiatric nurse training ended after 2006, and by 2012 nearly one-third of psychiatrists and most trained primary-care physicians had left the field (Chhim, 2017; Parry et al., 2020). This attrition reflected the limited absorption capacity of the public health system and the lack of a dedicated mental health budget—estimated at only 0.02% of the national health expenditure (McLaughlin & Wickeri, 2017). In this context, NGOs such as TPO Cambodia, Social Services of Cambodia, Center for Child and Adolescent Mental Health, and Supporter for Mental Health assumed a central role in service delivery, providing psychosocial support and community programs across multiple provinces (Chhim, 2017). By 2015, Cambodia had developed a modest but steadily growing mental health workforce, reflecting gradual progress since the 1990s. Yet this growth remained fragile, because it depended heavily on international support and NGO initiatives rather than consistent government investment. Overall, the period represented a phase of expansion constrained by dependency—conditions that would later prompt the move toward institutionalization and stronger national ownership (Parry et al., 2020).
Between 2001 and 2015, Cambodia made notable strides in rebuilding and expanding mental health services. Psychiatry was consolidated within national training at the UHS, and service delivery extended beyond Phnom Penh through outpatient and community-based care. The Ministry of Health gradually assumed stewardship, formalizing coordination under the DMHSA. However, progress was uneven. Inpatient capacity remained minimal, the number of specialists insufficient, and retention difficult, especially outside major cities. Training quality varied because of limited supervision, and nurse training programs came to a halt. Despite these challenges, this period marked a turning point: the country moved from dependence on external aid toward building the foundations of its own institutional and educational structures. Yet gains remained fragile, constrained by scarce resources and reliance on NGO partnerships, a reminder that the transition from external support to sustainable national leadership was still in progress. These constraints set the stage for the next period, which focused on consolidating national stewardship and formal institutional structures.
Phase III: Toward Institutionalization and Specialized Fields (2015–Present)
The Ministry of Health established the DMHSA, marking a shift toward institutionalizing psychiatry within the health system (Jegannathan et al., 2015). The department was tasked with coordinating services, developing training, and working with NGOs, although its resources remained limited. By 2022, Cambodia had 97 psychiatrists and 33 psychiatric nurses registered nationally. In addition, the Ministry of Health reported that by 2020 it had trained 296 physicians and 627 nurses in mental health through on-service modules, aiming to integrate basic care into general health facilities. The strategic plan also highlights the urgent need to expand subspecialty training in fields such as child and adolescent psychiatry, geriatric psychiatry, and addiction psychiatry. These figures underline both the modest progress made in scaling up human resources and the continued imbalance between national needs and available capacity (Department of Mental Health and Substance Abuse, 2023).
Since 2005, the UHS has operated the Diplôme d’Études Spécialisées (DES) in psychiatry, a three-year specialized residency training program delivered in Khmer and English. France has historically contributed to shaping Cambodia's medical education through long-standing academic and linguistic ties since the early post-colonial period. The UHS followed the French medical model, including the DES structure, which facilitated later collaborations and resident exchanges in psychiatry (Lim, Cheab, et al., 2024). However, psychiatry—together with ophthalmology—long stood as an exception: unlike other DES specialties, no residents traveled to France for in-residency training. From 2017 onward, a collaborating psychiatrist involved in training initiatives worked with UHS colleagues to strengthen psychiatric training by mobilizing existing France–Cambodia links. Building on the Programme international/International Program (IP) 2 (Lim, Vilhem, et al., 2024), he collaborated with Cambodian colleagues to enable residents to train in France during their DES. Since 2018, approximately 10 Cambodian psychiatrists and residents have undertaken Diplôme de Formation Médicale Spécialisée/Approfondie (DFMS/A) placements in France 3 , covering broad specializations and marking a move toward subspecialties in areas such as child, adolescent, and geriatric psychiatry.
France can be considered as a pragmatic partner for Cambodian psychiatry because of shared language, aligned training architectures (e.g., DES), and established mobility channels such as DFMS/A. Recently alongside these, more collaborations with institutions in other countries like Taiwan, Singapore, the Netherlands (Van Hoof et al., 2020), and the United States have offered targeted clinical exchanges opportunities, giving Cambodian early-career psychiatrists broader exposure to international practices. To our knowledge, France has been a partner permitting supervised, hands-on clinical practice through DFMS/A, which has supported selective mobility in medicine and psychiatry.
Alongside these training links, a modest but growing research ecosystem has taken shape. Within UHS, the elective IP introduced structured research methods teaching as part of its dual aim of training local trainers and preparing students for mobility, illustrating a pilot-and-scale approach to context-appropriate innovation (Lim, Vilhem, et al., 2024). Building on this capacity, early-career psychiatrists have initiated collaborative studies, including the first ethnopsychiatric investigation of anorexia nervosa in Cambodia, a qualitative project to describe clinical features and associated Khmer idioms of distress, and to map therapeutic itineraries across biomedical, religious, and traditional sectors (Bora et al., 2025; Vilhem, 2026; Vilhem & Bora, 2023). This initiative illustrates a shift from one-way training to reciprocal co-production of knowledge tightly coupled to clinical work.
Nonetheless, workforce development has remained insufficient. As of 2024, Cambodia's population is estimated at 17 million (Worldometer, 2024), served by about 108 psychiatrists (internal professional records). 4 This represents roughly 0.63 psychiatrists per 100,000 people, a ratio far below regional and global averages. The distribution is also highly uneven, with most specialists based in Phnom Penh (see Figure 4), leaving provincial populations dependent on general practitioners, nurses with short training, or NGO-led services. The WHO's Mental Health Gap Action Programme (mhGAP) has been promoted as a strategy to support non-specialists in recognizing and managing common disorders (World Health Organization et al., 2008).

Psychiatry Department at the Khmer-Soviet Friendship Hospital, Phnom Penh (2021). Source: Author photograph.
NGOs continue to play a central role in both service delivery and advocacy. TPO Cambodia has sustained community programs, incorporating Cambodian cultural idioms of distress and trauma-informed care. A prominent example is Operation Unchain, an initiative to release and treat people physically restrained by families due to lack of access to care. In many rural communities, families often resort to chaining or confinement as a last resort to manage relatives with severe mental illness, especially when public psychiatric services are unavailable. This practice reflects both the burden families face and their central role in caregiving. Operation Unchain, led by TPO Cambodia in partnership with the Ministry of Health, seeks to end such confinement through outreach, medical treatment, and family education, promoting humane care and community reintegration (GlobalGiving, n.d.; TPO Cambodia, n.d.-b). Dr. Chhim described a case in Prey Veng where a man, previously chained at four limbs, regained health and freedom after intervention. Although the initiative has grown rapidly, he acknowledged its fragility, operating largely on volunteer work and donations rather than national funding.
Despite these developments, several obstacles persist. Training capacity remains limited due to a shortage of senior psychiatrists able to provide supervision. Integration of psychiatry into primary health care is weak, with many rural clinics lacking staff who can reliably diagnose or manage psychiatric conditions. Inpatient and emergency services are scarce, and reliance on older generations of psychotropic medications remains the norm. Stigma and cultural barriers also continue to limit help-seeking, even where services exist. Looking to the future, Dr. Chhim emphasized the need for unified action among all stakeholders to mobilize resources, reduce discrimination, and build cross-sectoral collaboration. He stressed that mental health is “a cross-cutting issue in all fields” and highlighted the importance of international partnerships and technology in sustaining progress.
Alongside governmental initiatives, new community-based actors have emerged to promote mental health literacy and accessibility. AROM Station is a community-based initiative established in 2022. This period saw the rise of youth-driven mental health promotion in Cambodia. AROM Station works to enhance mental well-being through online psychoeducation, training, workshops, and individual consultations, emphasizing accessibility and cultural relevance for young people. AROM Station thus extends the earlier tradition of community-based mental health care pioneered by NGOs like TPO Cambodia, continuing this model through youth-led and digitally driven psychoeducation initiatives. This initiative reflects the growing momentum of community-led approaches that complement governmental and NGO efforts, illustrating how new generations of Cambodian professionals are shaping a more inclusive and locally rooted mental health landscape. 5
As this article shows, Cambodia has taken steps toward institutionalization since 2015, with a dedicated department in the Ministry of Health, continuity of national training, and early moves toward subspecialization through international exchanges. Services have expanded but capacity remains thin and unevenly distributed. NGOs continue to fill critical gaps, often pioneering approaches that address both clinical needs and cultural realities. The current stage reflects gradual institutionalization, but with persistent limitations in resources, training, and integration that must be addressed to sustain progress.
Conclusion
The development of psychiatry in Cambodia reflects the interaction of historical disruption, cultural frameworks, and institutional rebuilding. The country has slowly rebuilt its mental health services, even though there have been times of trouble and loss, especially during the Khmer Rouge regime. Since the 1990s, international collaborations and local expertise have contributed to these efforts. Traditional beliefs, Buddhism, and strong family bonds have played important roles in sustaining mental health care in the absence of formal infrastructure.
Early historical records about Cambodian psychiatry are sparse and often incomplete, making it challenging to trace sociocultural influences on mental health care over time. There is also a lack of qualitative research exploring the experiences of those who interacted with psychiatric services, limiting our understanding of cultural beliefs and societal attitudes. Future research using interviews or ethnography would help fill these gaps and deepen insight into Cambodia's psychiatric history.
Today, challenges remain in ensuring access, training, and quality care across the country, especially in rural areas. Progress will depend on expanding multidisciplinary training and integrating culturally responsive practices into clinical and community settings. A sustainable future for Cambodian psychiatry lies in ongoing collaboration, adaptation, and a clear recognition of Cambodia's unique social context which are the qualities that will be essential in improving mental health for all.
Footnotes
Acknowledgments
The authors would like to express their sincere gratitude to Professor Sunbaunat Ka and Dr. Chhim Sotheara for generously sharing their time and perspectives through interviews that informed the historical and professional understanding presented in this manuscript. We also thank Professor Kieth Rethy Chhem for his guidance, and Dr. Tampa Keo for his valuable support and encouragement throughout this work. We further acknowledge colleagues in the mental health field in Cambodia whose continued clinical, academic, and community efforts contribute to the ongoing development of mental health care in the country. Their work plays an important role in strengthening present services and shaping the future of mental health in Cambodia.
Ethics Statement
This article is a historical and documentary review and did not require ethics committee approval.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.