
Abstract
This article examines the scope and prevalence of vicarious posttraumatic growth (VPTG) among service providers working with Syrian refugees in Istanbul, Turkey. VPTG is the phenomenon that, under certain conditions, exposure to traumatic material because of work with traumatized individuals can result in positive psychological growth. This growth can include greater appreciation for life, changed priorities, and an enriched spiritual life, among others. We surveyed 104 service providers throughout Istanbul in 2018. A multivariable logistic regression was used to examine how professional trauma exposure (proportion of clients who disclose trauma, secondary traumatic stress [STS]), support systems (perceived social support, perceived organizational support), and professional experience are associated with VPTG. We hypothesized that greater exposure to traumatic material, stronger support systems, and greater professional experience were associated with higher levels of VPTG. We found nearly half (44.66%) of service providers surveyed had moderate-to-high levels of VPTG. Our hypothesis was partially supported. Moderate/high/severe STS [aOR:3.98, (95% CI:1.26, 12.59)], higher social support [aOR:1.05, (95% CI:1.00, 1.10)], and higher organizational support [OR:1.11, (95% CI:1.02, 1.20)] were associated with moderate-to-high VPTG. However, the proportion of clients who disclose trauma and years in profession did not show significant associations. While secondary stress may be a natural biproduct of work with traumatized individuals, providers may also experience growth from those same experiences. Findings from this analysis elucidate pathways whereby organizations may foster VPTG, such as providing a peer support program to facilitate social support and establishing a feedback loop to enhance organizational support.
The past decade has witnessed an overwhelming number of refugees displaced globally (UNHCR, 2025). The Syrian Civil War, which began in 2011, continues to be the source of one of the largest refugee populations with over 5.5 million Syrian refugees displaced worldwide (Cratsley et al., 2021; UNHCR, 2025). Although the situation in Syria has improved and hundreds of thousands of Syrian refugees have returned to their country, Turkey remains host to the largest number of Syrian refugees, with over 2.3 million registered under temporary protection (Ministry Interior of Turkey, 2026). Service providers working with Syrian refugees in Turkey have supported a population traumatized by war and who experience ongoing displacement-related stressors related to adjustment to the host country (Alpak et al., 2015; Hassan et al., 2016).
The adverse psychological consequences associated with supporting traumatized individuals and listening to painful stories of suffering and despair is well documented among a variety of service providers, including professionals and volunteers working with displaced populations (Roberts et al., 2021), asylum attorneys (Harris & Mellinger, 2021), interpreters (Geiling et al., 2021), and those working with Syrian refugees (Brooks et al., 2022). This cumulative exposure to traumatic material in addition to having an empathic relationship with traumatized clients can negatively affect service providers’ personal and professional lives. This can contribute to the development of Secondary Traumatic Stress (STS), which has similar symptoms to posttraumatic stress disorder (PTSD) (Branson, 2019; Collins & Long, 2003). However, few studies have examined how working with traumatized individuals can result in positive psychological growth.
Growth Following Trauma: Posttraumatic and Vicarious Posttraumatic Growth
A growing body of literature has explored how the aftermath of a direct traumatic event, such as those experienced during combat, displacement, natural disasters, sexual assault, as well as acute and chronic illness, among others, can provide an opportunity for personal growth (Hirad et al., 2023; Ramos & Leal, 2013). Calhoun and Tedeschi described this phenomenon as posttraumatic growth (PTG), which refers to the “positive psychological change experienced as a result of the struggle with highly challenging life circumstances” (Tedeschi & Calhoun, 2004, p. 1). Not all trauma survivors experience PTG, but for those who do, positive changes in certain aspects of their life include an increased appreciation for life, changed priorities, closer and more meaningful intimate relationships with others, increased personal strength, and an enriched spiritual life (Tedeschi & Calhoun, 2004).
Research on PTG has extended to individuals indirectly affected by trauma, which includes service providers who work with trauma survivors. Vicarious posttraumatic growth (VPTG) is the development of positive psychological growth as a result of indirect trauma from working with traumatized individuals (Arnold et al., 2005). VPTG was first examined among psychotherapists who worked with traumatized clients who, in addition to reporting negative psychological consequences of their work, also reported positive growth in certain areas of their life (Arnold et al., 2005). VPTG has been reported in a wide range of service providers, including counselors working with survivors of domestic and sexual violence, therapists working with traumatized children, interpreters, doctors, nurses, social workers, as well as clinical and managerial staff working with refugees (Cohen & Collens, 2013; Manning-Jones et al., 2016).
A constructivist self-development theory (CSDT) can be used to understand how indirect exposure to trauma can result in VPTG (Cohen & Collens, 2013). The CSDT suggests that individuals construct their own realities using cognitive structures or schemas to view the world (McCann & Pearlman, 1990). These schemas include service providers’ beliefs, assumptions, and expectations about themselves and a safe world (McCann & Pearlman, 1990). Vicarious trauma occurs when these schemas become modified, invalidated, or even shattered when working with traumatized clients and incorporating traumatic materials—which often results in distress among the service provider (Cohen & Collens, 2013; McCann & Pearlman, 1990). VPTG is the growth associated with the adjustment and adaptation to a new schema that incorporates traumatic material disclosed by traumatized individuals. Service providers who report VPTG express increased levels of sensitivity, compassion, insight, tolerance, empathy, and spirituality (Arnold et al., 2005). Our paper incorporates Cohen and Collens' (2013) CSDT framework as a guide to understanding VPTG.
Indirect Exposure to Trauma: Conceptual Underpinning and Extant Literature
Utilizing the CSDT framework, indirect exposure to trauma is a necessary steppingstone in the development of VPTG. Several studies have examined the relationship between the cumulative effect of indirect trauma exposure and STS among services providers in relationship to VTPG. In a study of 255 social work professionals in Israel, service providers with greater exposure to cases with abused children were associated with higher levels of VPTG (Weiss-Dagan et al., 2022). In another study of 143 domestic violence therapists and 71 therapists at social service departments in Israel, the study found STS to be significantly associated with VTPG (Ben-Porat, 2015). Study findings suggested, however, that greater exposure to traumatic material may not always necessarily translate into greater levels of VPTG, as findings suggest a plateauing or decline in VTPG at a higher level of STS (Ben-Porat, 2015). Similar findings were found among a study of 317 aid workers working with Syrian refugees in Jordan, where increased vicarious trauma was associated with increased VPTG (Rizkalla & Segal, 2020). However, the extent of exposure to trauma stories was not directly associated with VPTG, in that it was only associated through the mediating effects of meaning finding. This complex relationship between indirect trauma exposure and VPTG is also highlighted in a systematic review of quantitative studies of VPTG (Manning et al., 2015), as well as a recent review of service providers that emphasized additional research is further needed to examine the relationship between indirect trauma exposure and VPTG among displaced populations (Ebren et al., 2022). These findings suggest the relationship between trauma exposure and VPTG is not a simple direct association, rather a nuanced one, whereby service providers may even respond negatively to vicarious trauma exposure and experience low levels of VPTG.
Extant literature has shown that the level of support that service providers receive in their personal lives and the support they receive at work is associated with VPTG. A systematic review of VPTG suggests that social support may facilitate VPTG by improving social resources, decreasing isolation, and enhancing coping and adaptation following indirect trauma exposure (Manning et al., 2015). There exists a gap in the literature examining the role of social support and VPTG among refugee service providers; however, a study of 227 ambulance personnel in China found a direct relationship between social support and VPTG and suggests fostering support to promote VPTG (Kang et al., 2018). The limited literature that examines the role of organizational support and VPTG is conflicting. A study of 118 therapists working with traumatized individuals highlighted that organizational support did not predict VPTG (Brockhouse et al., 2011). However, a recent study of aid workers working with Syrian refugees in Jordan highlighted how organizational support is crucial in mitigating the negative impact of trauma work, and enabling space for growth [VPTG] (Rizkalla & Segal, 2020). These studies highlight the need to further explore the role of organizational support and VPTG.
Existing literature has suggested how time [years of professional experience] might facilitate the development of VPTG among service providers. A systematic review of VPTG highlighted a wide range of service providers that include interpreters, social workers, and those who work with refugees. These service providers initially react with distress as a result of traumatic exposure with traumatized individuals; however, over time they are able to react and cope with the meaning of the traumatic exposure or event (Manning et al., 2015).
Study Purpose
This article examines the scope and prevalence of VPTG among 104 service providers working with Syrian refugees in Istanbul, Turkey. First, we examine the frequency of moderate/high vicarious posttraumatic growth (including its five subscales) among our sample of service providers. Second, we examine the association between indirect trauma exposure (proportion of clients who disclose trauma, and level of secondary traumatic stress [STS]), level of support (perceived social support, perceived organizational support), and years in profession on vicarious posttraumatic growth. Our study hypothesizes that greater exposure to traumatic material, in addition to having greater support systems, and greater experience as a professional are associated with higher levels of VPTG. Gaining insight into the growth and resilience service providers experience while serving traumatized individuals is vital, as VPTG may occur most often in the presence of support and professional experience.
Methods
Study Design and Sample
Data was collected from Providers ASPIRE, a mixed method study conducted in late 2018 in Istanbul, Turkey that examined the mental health of service providers working with Syrian refugees. This analysis used the quantitative data of the Providers ASPIRE survey, which included 104 service providers recruited from 17 civil society organizations (CSOs) and public agencies. Public agencies are government-run service centers whereas CSOs are independent organizations that provide programs for refugees funded by national or international institutions. All CSOs and public agencies providing services to Syrian refugees in Istanbul (44 in total) were identified from a publicly available published list and invited to participate in the study. A total of 17 CSOs and public agencies approved our request. Agency focal points were contacted and facilitated connection to staff working with Syrian refugees in each agency.
A convenience sample was used, where participants were recruited on a rolling basis to consider availability of staff and existing workloads and to ensure equal gender representation. Eligibility criteria for the study included participants that were 18 years of age or older, worked with Syrian refugees more than 50% of the time, spoke English, Arabic or Turkish fluently, and did not show any signs of cognitive impairment (Folstein et al., 1975). Surveys were interviewer-administered in English, Turkish, or Arabic. Trained research assistants completed recruitment and surveys in private rooms at participant agencies. Written consent was obtained from all participants. In accordance with local custom, compensation was not provided to participants. Study protocols were approved by Columbia University Institutional Review Board and Ethics Committee of Istanbul Aydin University prior to the start of the study.
Measurement
Dependent Variable
The Post-Traumatic Growth Inventory (PTGI): is a 21-item scale that has been used to measure vicarious posttraumatic growth (VPTG) among service providers (Calhoun & Tedeschi, 1998). The PTGI consists of five subscales that measure areas of growth 1) new possibilities; 2) relating to others; 3) personal strength; 4) spiritual change; and 5) appreciation for life. Previous studies have adapted and validated the PTGI scale in Turkish (Aydin & Kabukçuoğlu, 2020) and in Arabic (Kira et al., 2012), where the internal reliability of the overall scale and its five subdimensions of growth were found to be satisfactory. The PTGI asks participants about changes that have occurred in their life as a result of working with refugees using a 6-point Likert scale: (0) “I did not experience this change as a result of working with refugees” – (5) “I experienced this change to a very great degree as a result of working with refugees.” Total scores were added, ranging from 0 to 105. In accordance with previous studies, a cutoff score of 63 and higher was used to represent moderate/high levels of growth, while scores lower than 63 represent low levels of growth (Wu et al., 2019). Cronbach's alpha estimating internal consistency among our sample was excellent (α = 0.93).
Independent Variables.
Exposure to Indirect Trauma
Proportion of clients who disclose trauma: a 5-point Likert scale that asks service providers the portion of their clients who disclose trauma: (0) no clients, (1) less than half but some clients, (2) around half of clients, (3) more than half but not all clients, and (4) all clients.
Secondary Traumatic Stress Scale (STSS): a 17-item scale to measure symptoms associated with indirect exposure to traumatic events via one's professional relationship with traumatized clients (Bride et al., 2004). Validated in Turkish (Kahil & Palabıyıkoğlu, 2018) and translated in Arabic, the STSS asks participants how frequently they have experienced a listed emotional situation as a result of working with Syrian refugees using a 5-point Likert scale: (0) Never – (4) Always. Scores were added, ranging from 0–68. In accordance with previous studies, a cutoff score of 38 or more was used to determine presence of STS (moderate-to-severe STS symptoms) (Bride et al., 2004; Duffy et al., 2015). Cronbach's alpha estimating internal consistency among our sample was good (α = 0.88).
Support Systems
Social Support: the Multidimensional Scale of Perceived Social Support (MSPSS) is a 12-item scale to measure support from three sources: family, friends, and significant others (Zimet et al., 1988). Validated in Turkish (Eker et al., 2001) and Arabic (Merhi & Kazarian, 2012), the MSPSS asks participants how they feel about their source of support through a 7-point Likert scale: (1) very strongly disagree – (7) very strongly agree, with higher scores representing higher levels of perceived social support (Eker et al., 2001). Cronbach's alpha estimating internal consistency among our sample was good (α = 0.81).
Organizational Support: the Survey of Perceived Organizational Support (SPOS) is an 8-item scale to measure employees’ perception to which their organization values their contribution and cares about their well-being (Eisenberger et al., 1986). Translated in Turkish and Arabic, the SPOS asks participants’ opinions about working at their agency through a 5-point Likert scale: (0) strongly disagree – (4) strongly agree; where higher scores represent higher levels of perceived organizational support. Cronbach's alpha estimating internal consistency among our sample was good (α = 0.89).
Professional Experience
Years worked in profession: we asked participants the number of years they worked in their profession (1) up to 1 year; (2) 1 to 5 years; (3) 6 to 10 years.
Sociodemographic
We included sociodemographic characteristics such as self-identified gender (male or female) and average weekly client caseload (continuous) as adjusted covariates, as previous literature has linked gender and caseload size with the mental health of service providers (Baum, 2016; Hensel et al., 2015).
Data Analyses
We used descriptive statistics to examine the sociodemographic characteristics (age, gender, nationality, level of education, agency type) of service providers, the frequency/type of traumas disclosed to service providers, as well as the frequency distribution of VPTG and PTGI scores. Independent sample t-tests were used to calculate significant mean differences for continuous variables between the dependent and independent variables, while Chi-square tests were used to calculate significant differences between categorical variables of the dependent and independent variables. The winsorization method was used for the covariate average client caseload due to the presence of outliers (Kwak & Kim, 2017). Outliers (average client caseload of 90, 90, 130, 150) were replaced with the largest upper bound values in our observation (average client caseload of 80).
A multivariable logistics regression model was used to examine the association between greater exposure to indirect trauma (proportion of clients who disclose trauma, secondary traumatic stress), greater support systems (perceived organization support, perceived social support), and length of time as a professional (years in profession) on VPTG. Adjusted covariates for the multivariable models include gender and average client caseload. All analyses were completed using STATA (version 15.1) (StataCorp, 2017).
Results
Characteristics of the Sample
Characteristics of service providers enrolled in our study are presented in Table 1. A total of 104 service providers were recruited throughout Istanbul; 73 were recruited from civil society agencies and 31 from public institutions. The average mean age was 28.56 years (SD = 5.08), close to half identified as male (49.04%), and the majority were Turkish nationals (82.69%). Most service providers completed the survey in Turkish (89.42%), followed by English (6.73%), and Arabic (3.85%). Three quarters of service providers had a 4-year university degree (75.00%).
Characteristics of Service Providers Working with Syrian Refugees in Istanbul, Turkey (N = 104).
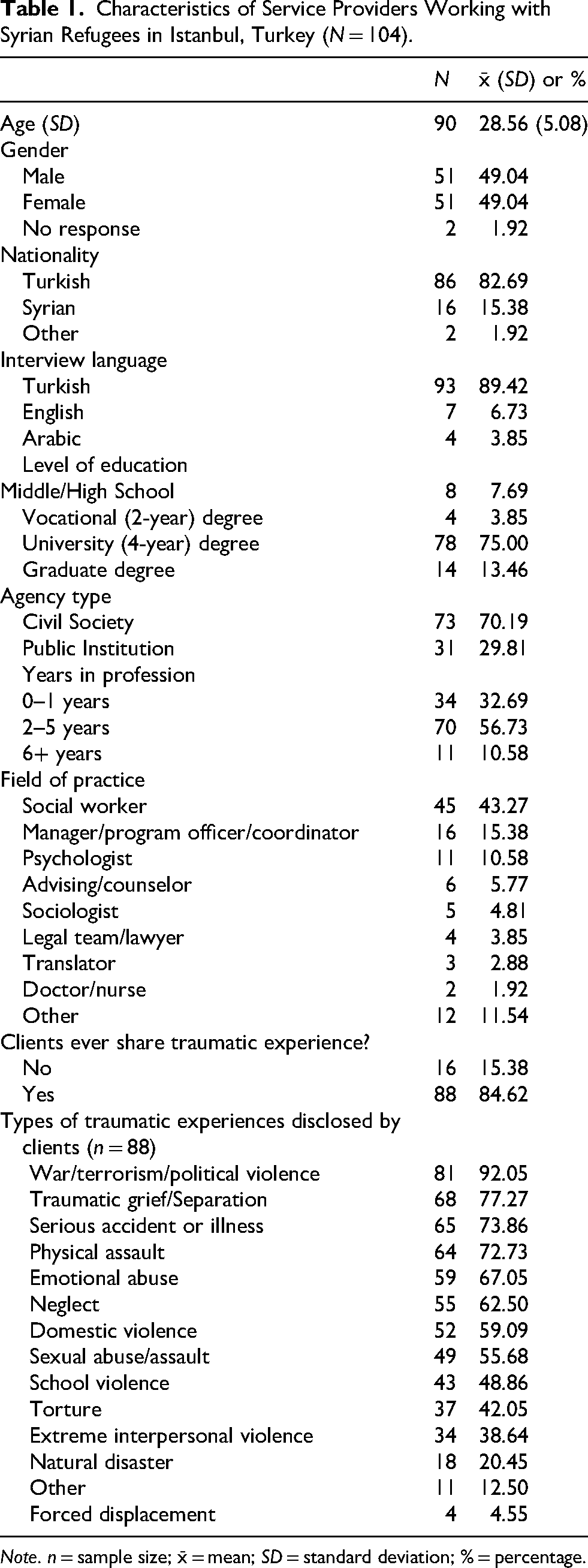
Note. n = sample size; x̄ = mean; SD = standard deviation; % = percentage.
Service providers surveyed reported a wide range of professions, including social worker (43.27%), manager/program officer/coordinator (15.38%), psychologist (10.58%), advising/counselor (5.77%), sociologist (4.81%), legal team/lawyer (3.85%), translator (2.88%), doctor/nurse (1.92%), and other (11.54%). Most service providers (84.62%) reported that their clients disclosed some type of traumatic experiences (Table 1). The three most frequent traumatic experiences disclosed were related to 1) war/terrorism/political violence; 2) traumatic grief/separation; and 3) serious accident or illness, while the least common were 1) natural disaster; 2) other; and 3) forced displacement.
Vicarious Posttraumatic Growth
Less than half of the service providers (44.66%) experienced moderate/high VPTG (Table 2). The total average PTGI item score was 2.80(1.02), which represents that service providers, on average, experienced small/moderate changes as a result of working with refugees. Among the five PTGI subscales, the highest average item scores were Personal Strength and Appreciation for Life, with an average item score of 3.10(1.18) and 3.10(1.19), respectively. The lowest average item subscale score was Relating to Others 2.44(1.15). Service providers working in an advising/counselor capacity 4.06(0.41) had the highest level of VPTG, followed by translator 3.59(0.57), and doctor 2.90(0.61) (Table 3).
Vicarious Posttraumatic Growth (VPTG) Inventory Scores.
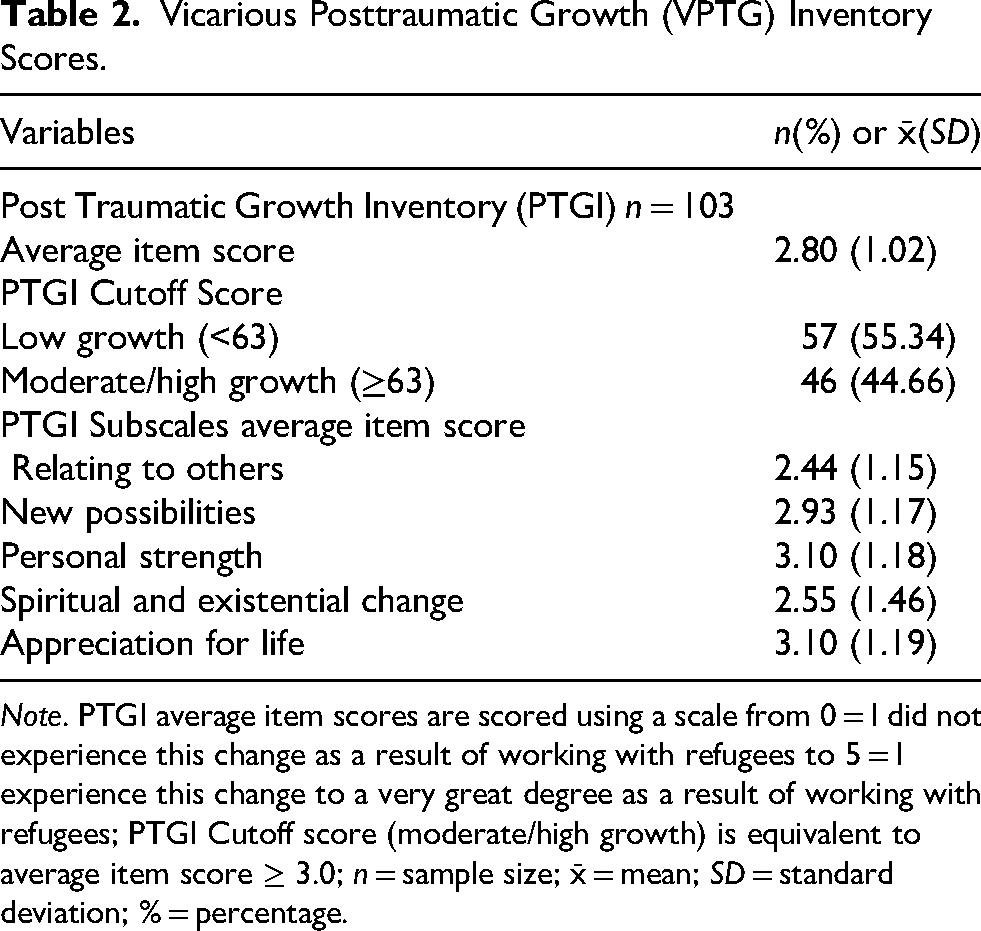
Note. PTGI average item scores are scored using a scale from 0 = I did not experience this change as a result of working with refugees to 5 = I experience this change to a very great degree as a result of working with refugees; PTGI Cutoff score (moderate/high growth) is equivalent to average item score ≥ 3.0; n = sample size; x̄ = mean; SD = standard deviation; % = percentage.
VPTG, Proportion Client Disclose Trauma, STSS, SPOS, and MSPSS Mean Score by Service Provider Profession.
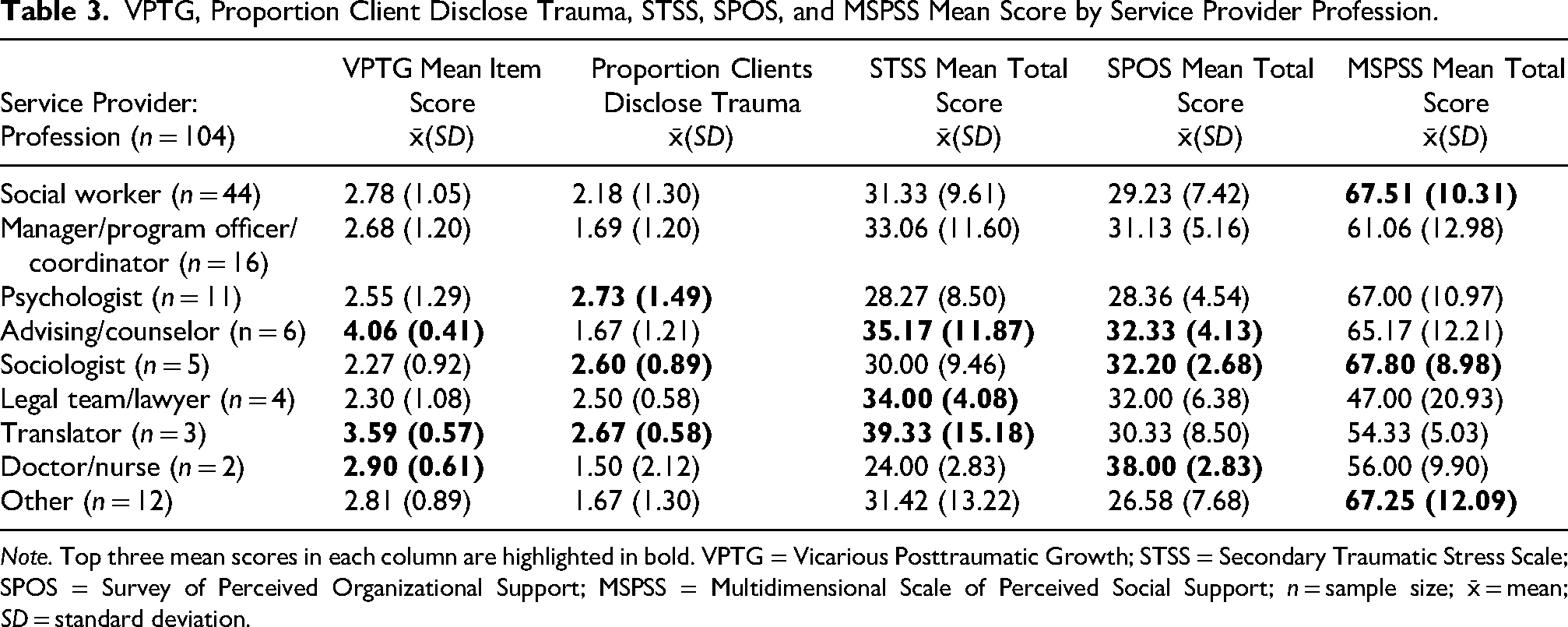
Note. Top three mean scores in each column are highlighted in bold. VPTG = Vicarious Posttraumatic Growth; STSS = Secondary Traumatic Stress Scale; SPOS = Survey of Perceived Organizational Support; MSPSS = Multidimensional Scale of Perceived Social Support; n = sample size; x̄ = mean; SD = standard deviation.
Indirect Trauma Exposure
The proportion of clients who disclosed traumatic experiences ranged from 0 to 4, with a mean of 2.11(1.28). This represents that on average, over half of clients disclosed traumatic experiences to service providers. Over one-quarter (27.88%) of service providers met the cutoff for moderate/high/severe secondary traumatic stress (STS), while over three-quarters (72.12%) met the cutoff for none/little/mild STS. Table 3 highlights the professions who had the highest proportion of clients disclose trauma, which include psychologists 2.73(1.49), translators 2.67(0.58), and sociologists 2.60(0.89), while those with the highest STS mean score were translators 39.33(15.18), advising/counselors 32.33(4.13), and legal team/lawyers 34.00(4.08).
Significant associations between indirect traumatic exposure factors and VPTG were found in our multivariable model (Tables 4 and 5). In the multivariable model, moderate/high/severe secondary traumatic stress (STS) was significantly associated with increased odds in the unadjusted model [OR: 4.05 (95% CI: 1.37, 12.02)] and increased odds in moderate to high VPTG in the adjusted model [aOR: 3.98 (95% CI: 1.26, 12.59)]. In the bivariate analysis; however, the association between STS and VPTG was trending towards significance (p = .074), which may suggest STS and VPTG have a more complex association when other variables (e.g., level of support, years in profession, etc.) are included in the model. No significant association was found between the proportion of clients who disclose trauma and VPTG. Our hypothesis that greater exposure to traumatic material was partially supported, where higher levels of STS (but not proportion of clients who disclose trauma) were associated with moderate-to-high VPTG.
Bivariate Associations Between Vicarious Traumatic Exposure, Support Systems, and Years in Profession on Moderate/High Vicarious Posttraumatic Growth.
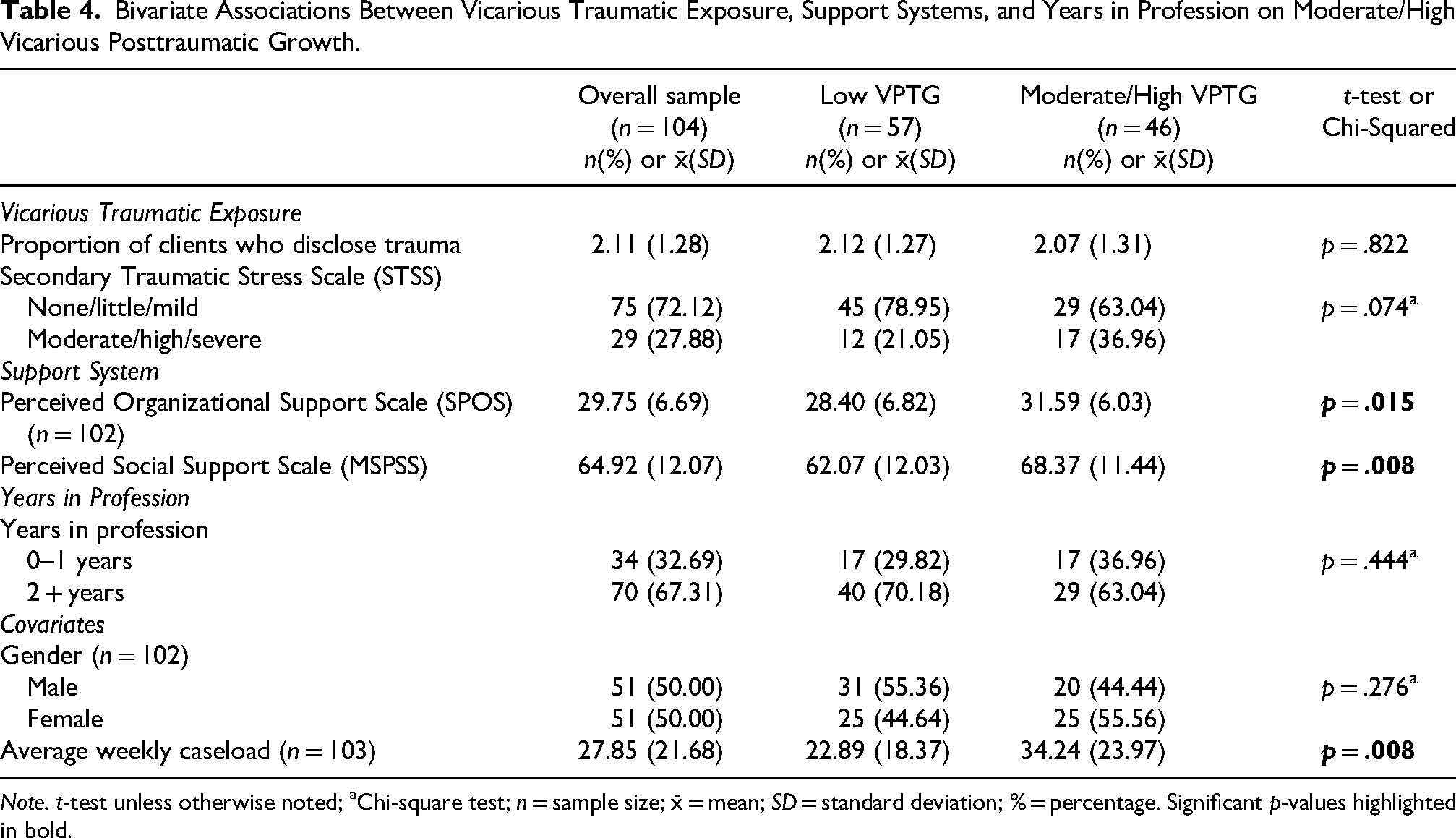
Note. t-test unless otherwise noted; aChi-square test; n = sample size; x̄ = mean; SD = standard deviation; % = percentage. Significant p-values highlighted in bold.
Multivariable Association Between Vicarious Traumatic Exposure, Support Systems, and Years in Profession on Moderate/High Vicarious Posttraumatic Growth.
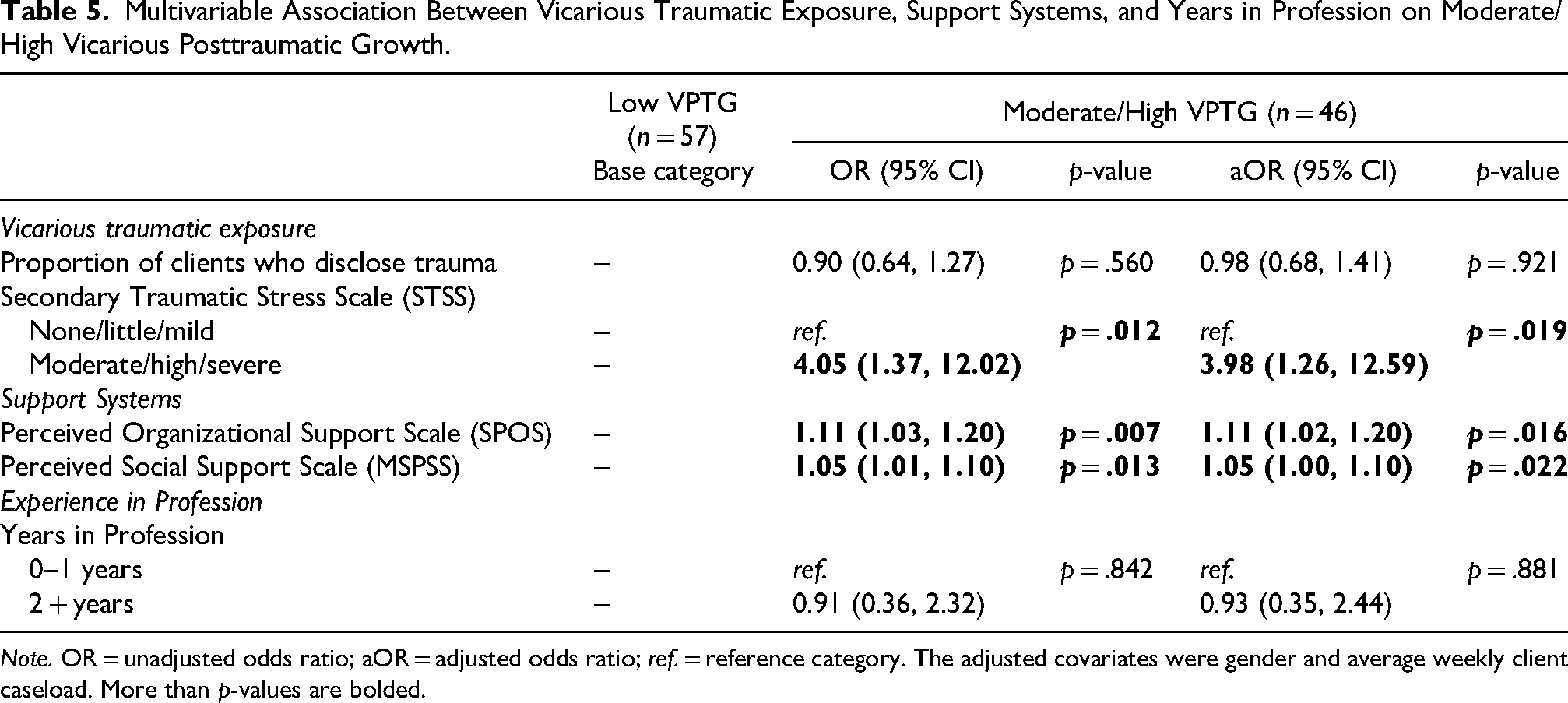
Note. OR = unadjusted odds ratio; aOR = adjusted odds ratio; ref. = reference category. The adjusted covariates were gender and average weekly client caseload. More than p-values are bolded.
Support System
Significant associations between support system factors and VPTG were found in both the bivariate and multivariable analyses. Service providers with moderate/high VTPG had, on average, a significantly higher perceived organizational support (SPOS) score compared to those who had low VTPG (p = .015). This was also true for perceived social support (MSPSS) scores, where service providers with moderate/high VPTG had, on average, a significantly higher MSPSS score compared to those with low VPTG (p = .022). This significance was also found in the multivariable model, where each additional increase in SPOS score was associated with an 11% increased odds of moderate/high VTPG in the unadjusted model [OR: 1.11 (95% CI: 1.03, 1.20)] and the adjusted model [aOR: 1.11 (95% CI: 1.02, 1.20)], while each additional increase in MSPSS score was associated with a 5% increased odds of moderate/high VPTG in the unadjusted model [OR: 1.05 (95% CI: 1.01, 1.10)] and the adjusted model [aOR: 1.05 (95% CI: 1.00, 1.10)]. Service provider professions with the highest SPOS scores were doctor/nurse 38.00(2.83), advising/counselor 32.33(4.13), and sociologist 32.20(2.68), while the highest MSPSS scores were sociologists 67.80(8.98), social workers 67.51(10.31), and other 67.25(12.09) (Table 3). Our hypothesis was supported as both social and organizational support were associated with moderate-to-high VPTG.
Years in Profession, Gender, and Average Weekly Caseload
Among service providers surveyed, over half worked in their profession for 2–5 years (56.73%), approximately one third (32.69%) worked one year or less, and 10.58% worked 6 or more years (Table 1). No significant associations between years in profession and gender on moderate/high VPTG in both the bivariate analysis and multivariable models were found (Tables 4 and 5). We did not find moderate/high VPTG to have a significantly higher average weekly client caseload compared to low VPTG in the bivariate model (p = .008). Our hypothesis that having greater years of professional experience was associated with higher levels of VPTG was not supported.
Discussion
This paper examines the scope and prevalence of VPTG among service providers working with Syrian refugees in Istanbul, Turkey. We found the rates of moderate-to-high VPTG (44.66%) among our service providers to be similar to other service providers who work with refugee and non-refugee populations. However, the average VPTG item score among our sample of service providers was slightly below a moderate degree of growth, which was lower compared to other studies that examined VPTG among different service providers, including aid workers working with Syrian refugees in Jordan (Rizkalla & Segal, 2020), domestic violence and social service therapists in Israel (Ben-Porat, 2015), psychiatric nurses in Israel (Zerach & Shalev, 2015), and health professionals in New Zealand (Manning-Jones et al., 2016).
One reason why the average VPTG item score in our sample may have been slightly lower is because of the wide variety of service providers we included in our study (e.g., social worker, manager/program officer/coordinator, legal team/lawyer, psychologist, doctor/nurse). In the study sample, service providers who were in an advising/counselor capacity or were translators had a much higher VPTG score, while sociologist or legal team/lawyer had the lowest VPTG score. Differing VPTG scores were also found among a study of health professionals in New Zealand, where social workers had a higher VPTG score compared to psychologists (Manning-Jones et al., 2016). Different VTPG scores between service providers may be associated with the unique training associated with each profession, in addition to the varying exposure to traumatic materials.
Our original hypothesis was that greater exposure to traumatic material, as well as a greater support system, and greater years of professional experience are associated with higher levels of VPTG. This was partially supported. We found higher levels of STS (but not proportion of clients who disclose trauma) and greater support systems (social and organizational support) to be associated with moderate-to-high VPTG. Furthermore, we did not find any significant association between greater years in profession and moderate-to-high VPTG. These findings suggest the important role STS and support systems have on VPTG.
Several reasons may explain our findings that highlight the association between greater exposure to traumatic material and VPTG. In a previous study of service providers working with Syrian refugees, one reason why no significant associations were found with the proportion of clients who disclose trauma is because VPTG may be closely associated with the type and severity of traumatic material, as well as its personalized impact on the service provider (Brooks et al., 2022). This may be the reason why STS—rather than proportion of clients who disclose trauma—may be a better predictor of VPTG, in that STS measures the PTSD-like symptoms associated with the cumulative effects of working and engaging with traumatized individuals (Bride et al., 2004). The direct association between STS and VPTG has also been highlighted in several studies examining VPTG, including a systematic review of VPTG among service providers (Ben-Porat, 2015; Manning et al., 2015). However, the linkage between STS and VPTG appears more complex and nuanced (a curvilinear rather than linear relationship), as previous studies have shown that there may be a plateauing or decline in VPTG at higher levels of STS (Ben-Porat, 2015; Manning et al., 2015).
Regarding service providers’ support systems, we found both higher social support and organizational support were associated with higher VPTG. One explanation is that having greater social support may act as a mitigating factor for indirect trauma exposure, as social support is theorized as a buffer for stressful events (Cohen & Wills, 1985). Having greater social support has also been suggested to decrease isolation, enhance coping and adaptation, and improve overall social resources (Manning et al., 2015). Similarly, greater organizational support may facilitate higher VPTG, as a recent study of aid workers working with Syrian refugees in Jordan suggested organizational support to be crucial in mitigating the negative impact of trauma work, and enabling space for growth (Rizkalla & Segal, 2020). A mixed method study of service providers in Turkey working with refugees found repeated exposure to traumatic stories resulted in diminished interest in activities, and contributed to detachment and estrangement from their existing social support system (Yükseker et al., 2024). This sense of detachment may also be compounded by the fact that public opinion, in recent years, has been more negative towards Syrian refugees (Saraçoğlu & Bélanger, 2019). Furthermore, the study also mentioned both formal- and peer-supervision was often infrequent, and that some service providers felt they had nobody to speak to regarding the traumatic material they were witness to, leading to isolation and avoiding discussion about work altogether (Yükseker et al., 2024).
Lastly, there may be several reasons why greater years in profession was not associated with higher VPTG. One reason is that level of exposure to traumatic material each profession experiences may vary (e.g., social worker vs doctor/nurse vs manager/program officer/coordinator), which may impact the time (i.e., how quickly or slowly) it takes for one to develop VPTG. For example, psychologists and translators in our study had the highest proportion of clients disclosing trauma while managers/program officers/coordinators had the lowest. This means that even with the same years of professional experience, managers/program officers/coordinators are, on average, exposed to less traumatic material compared to psychologist and translators. Furthermore, the time it takes for a service provider to cope with and adapt to traumatic material and to develop VPTG is a personalized process that is dependent on a variety of factors unique to the service provider, which include the unique background and training associated with each profession in managing traumatic material. Mental health services in Turkey, for example, are provided by a range of professionals that include psychiatrists, psychologists, psychological counselors, and social workers, which favor a particular theoretical orientation over another within their respective professions (i.e., cognitive behavioral therapy, system/family systems therapy, versus constructivist therapy) (Savcı et al., 2018).
Limitations
Our study presents the following limitations. First, service providers were recruited on a rolling basis to generate a convenience sample, which limits the generalizability of our results. Furthermore, self-selection bias may have occurred. Service providers who were severely impacted by working with traumatized clients may have not wanted to self-volunteer and participate in the study without being randomly selected and encouraged to do so.
Second, the cross-sectional design of our study limits our ability to draw causal inferences as associations were treated without consideration of temporality. As the name implies, vicarious posttraumatic growth measures service providers’ growth over time as they are impacted by their work with traumatized individuals—a challenging task to measure in a cross-sectional study. This study attempted to mitigate this limitation by including service providers and the years of professional experience in all our analysis. Future studies should focus on the longitudinal aspect of VPTG which, surprisingly, very few studies have done.
Third, this study sample only included service providers currently working in their profession. Working with traumatized clients and listening to stories of despair and grief can be detrimental to a service provider's psychological wellbeing, which may cause certain individuals to leave their job or switch professions entirely. This study sample may include professionals who are incredibly resilient when working with traumatized individuals, or those who have just started their job or profession. Future studies should examine growth associated with professionals who left their jobs and who are no longer working with traumatized individuals.
Fourth, we used validated measures in English, Turkish, and Arabic in our study whenever possible; however, not all measures (i.e., STSS and SPOS) had been previously validated cross-culturally in both Turkish and Arabic. Translation, adaptation, and validation of a measure cross-culturally is a lengthy and complex process that enables an instrument to capture the intended latent meaning of a measure in a different language or cultural context (Cruchinho et al., 2025). Our study team attempted to reduce this risk by having bilingual experts test translated measures to make sure they were appropriate cross-culturally. As cross-cultural validation of a measure requires additional resources and methodological skills, studies should share their validated measures with others.
Lastly, the small sample size (n = 104) limited the ability to examine nuances between different service providers (e.g., social workers, psychologists, caseworkers, interpreters, managers, etc.). Future quantitative studies should include a larger sample size. Additionally, future studies should include qualitative interviews of service providers and their experience working with refugees and other traumatized individuals to further explore the concept of psychological growth in the Turkish context, as well as in other similar humanitarian situations. Qualitative interviews can also provide insight into the mechanisms behind VPTG as well as the potential facilitators and barriers to psychological growth.
Implications and Conclusions
This study has important implications for the wellbeing of service providers who work with Syrian refugees and other traumatized populations. Although preventing negative psychological consequences such as STS may not be entirely possible among service providers, organizations can play an active role in facilitating social and organizational support to foster the development of VPTG. Focusing on the wellbeing of service providers, in turn, will enhance the quality of care received by the client.
The study findings suggest a close relationship between STS and VPTG. Organizations may benefit from providing general information and psychoeducation to service providers about the negative psychological consequences of exposure to traumatic material, the development of STS, and the growth associated with VPTG. One possibility is to provide some form of trauma-informed training for service providers, such as the four Rs of trauma-informed approach, which help 1) realize the widespread impact of trauma; 2) recognize the symptoms and signs of trauma in clients and staff; 3) respond by incorporating knowledge about trauma into organizational policies and practices; and 4) resist re-traumatization by creating an organization that promotes a trauma-informed approach (US Department of Health and Human Services, 2014). A recent study of healthcare professionals who responded to the aftermath of the 2023 earthquake in Southeastern Turkey found a 1-day trauma-informed care training helped healthcare workers understand trauma, interpersonal relationships, and also significantly reduce burnout (Şimşek & Uğur, 2025).
Previous studies have also emphasized the role of supportive and educational supervision in managing exposure to traumatic material (Reuven Even Zahav et al., 2020). Supportive supervision may include the creation of a reoccurring weekly supervision that is protected from distractions and interruptions from the workplace, and where the supervisee can ask for help from the supervisor regarding administrative (paperwork, productivity, following policies and procedures), educational (address issues that arise with clients and use of clinical theory, skills and intervention), and overall support (encourage, empathize and support supervisee) (Grady & Dombo, 2016). Providing supportive supervision is important among emerging fields in Turkey such as social work, where guidelines and standards for supervision are still developing (Taşğın, 2019).
This study also suggests the need for both social and organizational capacity building. Organizations may benefit from introducing a peer support program, which have been shown to support resilience and well-being, especially after an adverse or emotionally stressful event, and to development of shared organizational responsibility (Shapiro & Galowitz, 2016). Peer support programs may include support following a critical incident or emotionally stressful event, or may provide support that extends beyond the critical incident and include workplace support, managing stressors, as well as personal problems (Donovan, 2022). A review of peer support programs among first responders found peer support can facilitate PTG by providing space to process posttraumatic events and help manage organizational stressors, which can also lead to increased well-being (Donovan, 2022). A study of earthquake disaster responders in Turkey and Syria examined self-care strategies used by disaster responders and found support from colleagues was one of the most frequent self-care strategies used, which indicates the potential benefits of developing a peer support program (Blomberg et al., 2024). Furthermore, as suggested in previous studies (Brooks et al., 2022), organizations can also benefit from developing a constructive feedback loop, where service providers can express grievances and an organization can provide positive feedback to their employees.
Lastly, as working with traumatic materials can contribute to adverse psychological symptoms in some, service providers should be encouraged to seek mental health care if needed (Collis & Long, 2003). In recent years, the mental health system in Turkey has increased accessibility of mental health treatment by following a community-based model that is intended to integrate mental health with primary health care (Bilir & Artvinli, 2021).
This research highlights the need to understand both the positive and negative psychological consequences of working with traumatized communities. It also emphasizes the importance of focusing on service providers’ wellbeing, by minimizing the impact of exposure to traumatic material and by fostering the development of VPTG. Future research should utilize qualitative and longitudinal approaches in understanding VPTG development, so the mechanisms behind VPTG, trauma exposure, support systems, and time can be better understood. One possible future study is to examine service providers who recently graduated and to track how trauma exposure, supports system, and VPTG develop over time. This includes service providers who continue to work within their profession, those who decide to change professions, as well as service providers who experience high levels of STS yet low levels of VPTG.
Footnotes
Acknowledgements
The authors would like to acknowledge and thank the agencies who opened their doors to our study and the participants who took the time to share their stories. Our work would not have been possible without the dedicated research staff who contributed during the study period.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Columbia University President's Global Innovation Fund (2016–2018).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.