
Abstract
This study’s aim was to describe: (a) How life-sustaining treatment (LST) decisions are made for critically ill children in Italy; and (b) How these decisional processes are experienced by physicians, nurses and parents. Focus groups with 16 physicians and 26 nurses, and individual interviews with 9 parents were conducted. Findings uncovered the ‘private worlds’ of paediatric intensive care unit (PICU) physicians, nurses and parents; they all suffer tremendously and privately. Physicians struggle with the weight of responsibility and solitude in making LST decisions. Nurses struggle with feelings of exclusion from decisions regarding patients and families that they care for. Physicians and nurses are distressed by legal barriers to LST withdrawal. Parents struggle with their dependence on physicians and nurses to provide care for their child and strive to understand what is happening to their child. Features of helpful and unhelpful communication with parents are highlighted, which should be considered in educational and practice changes.
Introduction
Advances in paediatric critical care have improved survival rates for complex medical problems in children. These advances sometimes result in ethical dilemmas regarding the use or withdrawal of life-sustaining treatments (LSTs). LSTs commonly refer to assisted ventilation, chest compressions and inotropic support of circulatory function, but can also include other supports of vital functions, such as renal replacement therapies, parenteral or enteral nutrition or hydration, extra-corporeal membrane oxygentation, as well as selected surgical interventions.
It is widely held in most Western countries that treatment decisions for children should be based on the child’s ‘best interests’. The treatment option that offers the greatest proportion of benefit in relation to burden is considered to be in the child’s best interests; recognizing that any LST can be withheld or withdrawn depending on the balance of benefits and burdens for the child (AAP, 1994;Carnevale et al., 2007;CPS, 2004;Hubert et al., 2005). However, there is no consensus over which benefits and burdens should carry the greatest weight. The child’s best interests are frequently difficult to determine.
Another issue relates towho should judge what is best for a child. For example, whereas North American standards require that LST decisions be made by the child’s legal guardians, ordinarily the parents (AAP, 1994;CPS, 2004), French standards challenge this view, arguing that parents should be protected from being ‘culpabilized’ for life-support decisions – that physicians should bear the responsibility for such decisions (Carnevale et al., 2006,2007;Hubert et al., 2005).
A statement regarding LST, published by the Italian Society of Neonatal and Pediatric Anesthesia and Intensive Care, states that the physician in charge of the patient’s care and the unit head bear the main responsibility for the final decision, although the participation of other staff and the parents should be sought (Giannini et al., 2008).
European survey research has documented physicians’ reports on how such decisions should or are actually made in Italy, mainly in neonates (Cuttini et al., 2000,2004,2009;Devictor and Nguyen, 2004). Yet, no research has examined decision-makingprocesses and theexperiences of those primarily involved in decision-making: physicians, nurses and parents.
The research questions for this study were: (1) how are LST decisions made for critically ill children in Italy; and (2) how are these decisional processes experienced by physicians, nurses, and parents?
The study was oriented by a cultural interpretive framework (Carnevale, 2005), extending prior research in France and Canada (Carnevale et al., 2007). Medical, nursing, and parental opinions and practices are examined in relation to conceptions of good/bad rooted in the local cultural context.
Methods
Focus group (FG) methodology was used because it: (1) is effective for investigating process phenomena such as decision-making and concepts that are poorly understood; (2) can be used to obtain data that might be limited or costly through individual interviews; and (3) can solicit richer data than approaches such as surveys (Denzin and Lincoln, 2000;Hollander, 2004;Kitzinger, 1994,1995). Participants can share individual viewpoints and discuss points raised by others.
Participants were recruited from two sources: (1) physicians, nurses and parents from the paediatric intensive care unit (PICU) at a general hospital in Verona, Italy (Hospital); and (2) Italian physicians and nurses attending congresses; specifically, the European Society of Paediatric and Neonatal Intensive Care (ESPNIC) congress held in Verona, June 2009, and the Neonatology Congress (NC) held in Verona, March 2010. Congress recruitment ensured multi-site physician and nurse participation.
The inclusion criterion for physicians and nurses was that participants had to be practicing in the care of critically ill children. Hospital-based recruitment was facilitated by the PICU medical and nursing managers. Congress-based participants were recruited through posters placed at the congresses.
Physicians and nurses were interviewed separately. Physician focus groups and nurse focus groups were conducted at the hospital and the ESPNIC congress. The number of ESPNIC nursing participants was small (i.e.n = 4), therefore, an additional nurse focus group was conducted at the NC congress. Combining hospital and congress recruitment, a total of 16 physicians and 26 nurses participated in the study (Tables 1 and 2 ). Most participants worked with both paediatric and neonatal populations, as is relatively common in Italian paediatric critical care.
Description of physician participants (n = 16)

Note: Sample includes physicians from nine different cities throughout Italy.
Description of nurse participants (n = 26)

Note: Sample includes nurses from nine different cities throughout Italy.
The inclusion criterion for parents was that a parent had a child who had been cared for in a PICU. We sought parents whose child had had a LST decision made, including a mix of parents whose children survived or died, to solicit a range of experiences. Parent participants were identified by the medical and nursing directors of the participating hospital PICU. Focus groups were not used for parents, to explore each parent’s experience more ‘personally’, presuming this was a more vulnerable participant group. Nine parents were interviewed (Table 3 ). In each case the child’s critical illness had occurred within two years prior to the interview, with one exception where the critical illness and death occurred eight years before the interview. This range of timeframes was desired in order to solicit diverse parental perspectives on their experiences.
Description of parent participants and their critically ill children (n = 9)
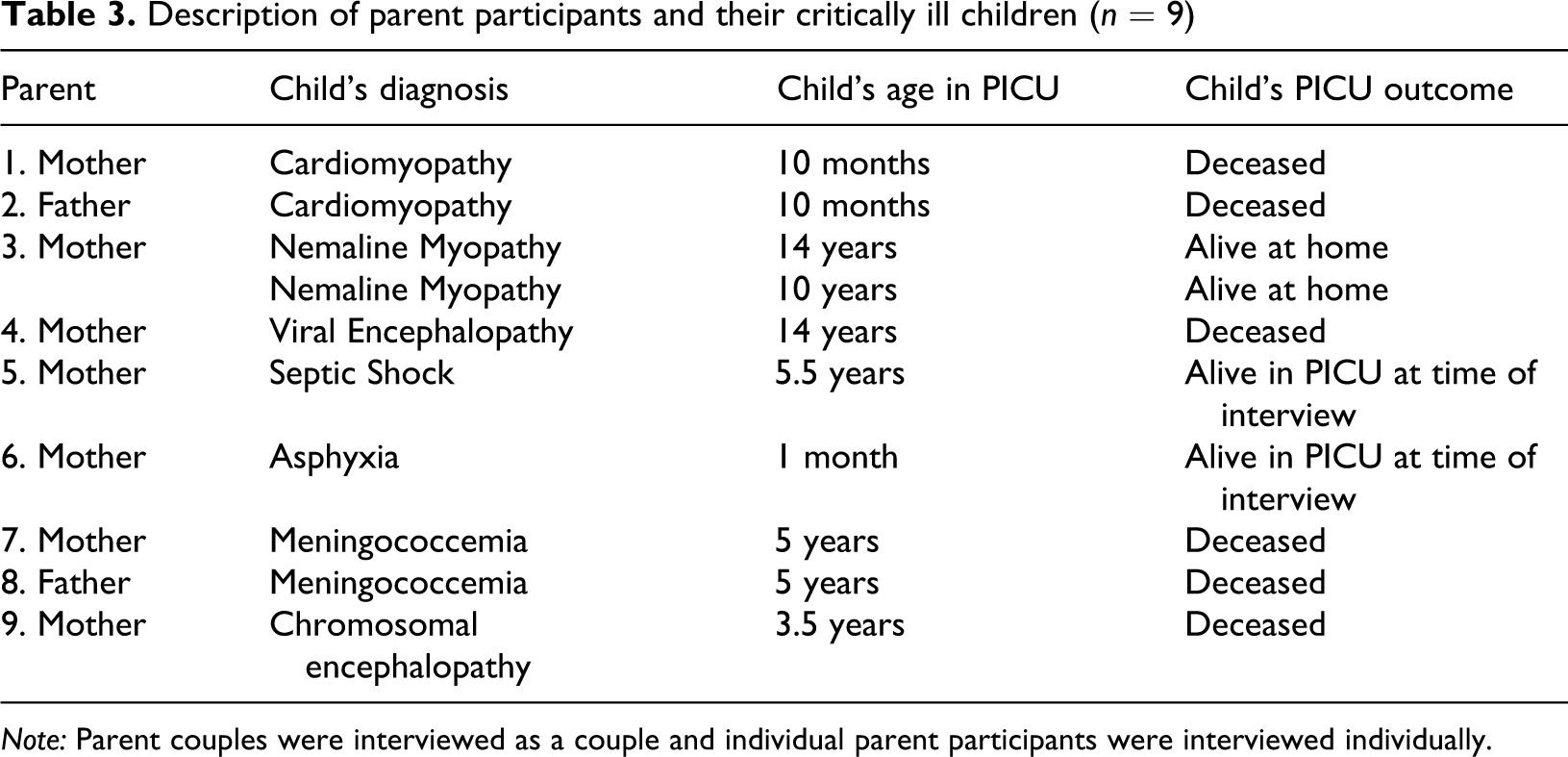
Note: Parent couples were interviewed as a couple and individual parent participants were interviewed individually.
Focus groups and parent interviews were oriented by guiding questions, adapted from the study’s research questions. Focus group guiding questions included (translated from Italian): How are LST decisions made in your unit? Who makes these decisions? What criteria are used to make these decisions? Please describe an example? What ethical challenges do you face in your work? Parent interview guiding questions included (translated from Italian): Please describe a time when a decision was made for your child about a life-sustaining treatment. How was this decision made? Who made the decision? How do you feel about the way this was done? How did you feel about it then? How do you feel about it now?
All focus groups and parent interviews were conducted by one investigator (FAC) to ensure consistency. One of two Italy-based co-investigators (MB or AB) co-facilitated each meeting. Each meeting was audio-recorded and lasted 60–90 minutes. Audio-recordings were transcribed and content analysed, in Italian. The principal data analysis strategies were data coding and constant comparative analysis, both adapted from grounded theory (Strauss and Corbin, 1990). Identified themes were translated into English at the end of the analysis.
Methodological rigor was maintained through recognized criteria in qualitative research (e.g. credibility, fittingness, auditability, confirmability) (Barbour, 2001;Carnevale, 2002;Sandelowski, 1986). For example: the facilitator paraphrased emerging themes in the focus groups to seek participant confirmation; all data were analysed through the same coding procedures to maximize coding consistency.
The study was approved through research ethics review at the participating hospital in Verona, Italy. All participants provided signed informed consent. The focus groups presented a research ethics challenge. Although the researchers ensured that they would respect participants’ confidentiality, the same assurance could not be offered regarding the conduct of other participants. Although participants were asked to respect the privacy of other focus group members, they were also informed that their peers were not held to the same standard of confidentiality as the researchers. They were informed of this potential breach of confidentiality.
Results
Physician and nurse findings are presented first, followed by parent findings, ending with an integration of all findings. Verbatim exemplars of identified themes are presented in Tables 4–7.
Physician and nurse findings
Physician and nurse data, from congress and hospital participants, were pooled to preserve anonymity. Findings are presented thematically. For each theme, commonalities between physicians and nurses are discussed first, followed by between-group divergences. Findings are presented within a three-fold structure, in line with the study’s research questions: (a) decision-making process; (b) decision-making criteria; and (c) significant ethical challenges. Four decision-making process themes were identified (Table 4 ) as well as seven significant ethical challenges (Table 5 ). When referring to both physicians and nurses, the former are listed first. No preferential treatment is intended.
Decision-making process (physicians and nurses)
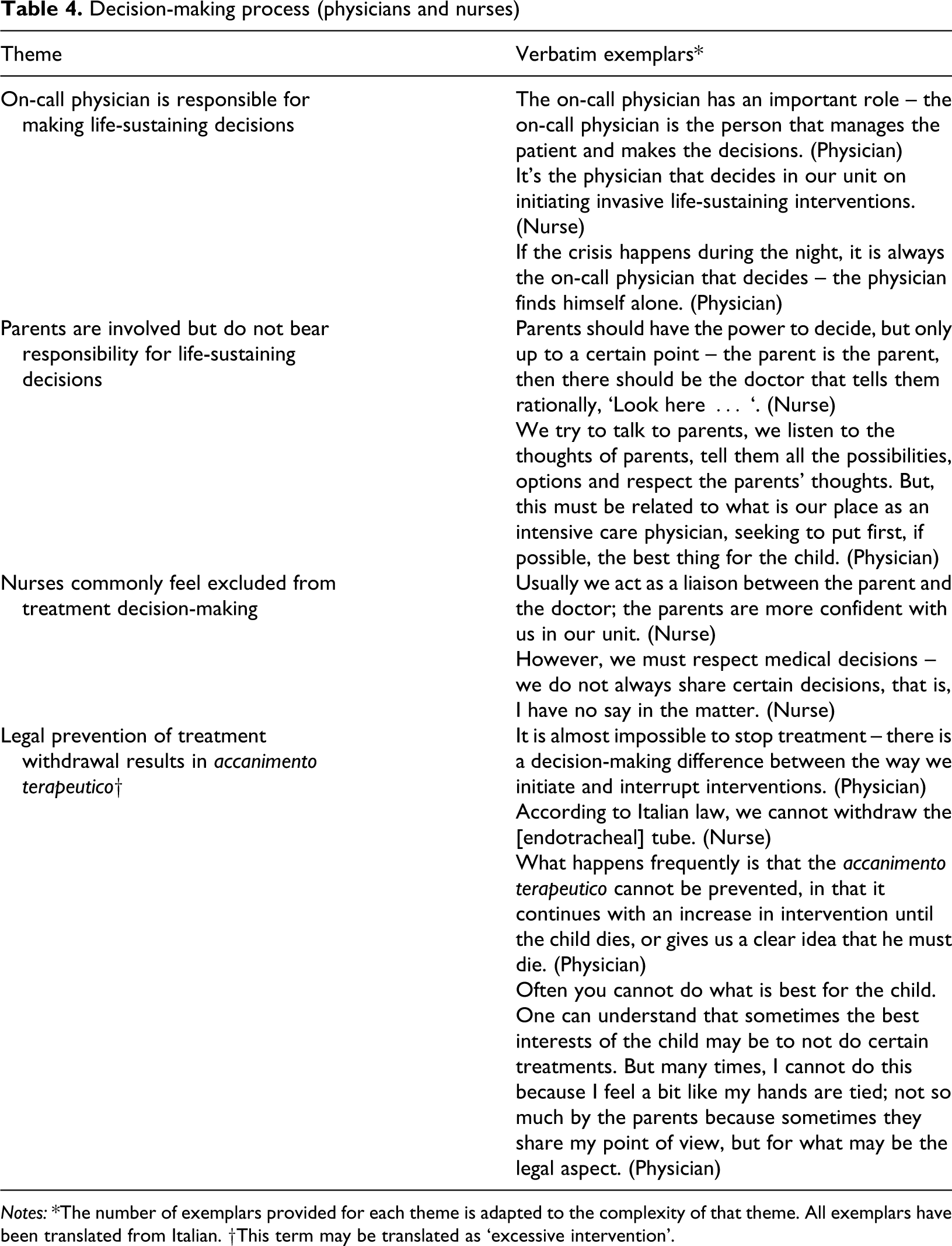
Notes: *The number of exemplars provided for each theme is adapted to the complexity of that theme. All exemplars have been translated from Italian. †This term may be translated as ‘excessive intervention’.
Significant ethical challenges (physicians and nurses)
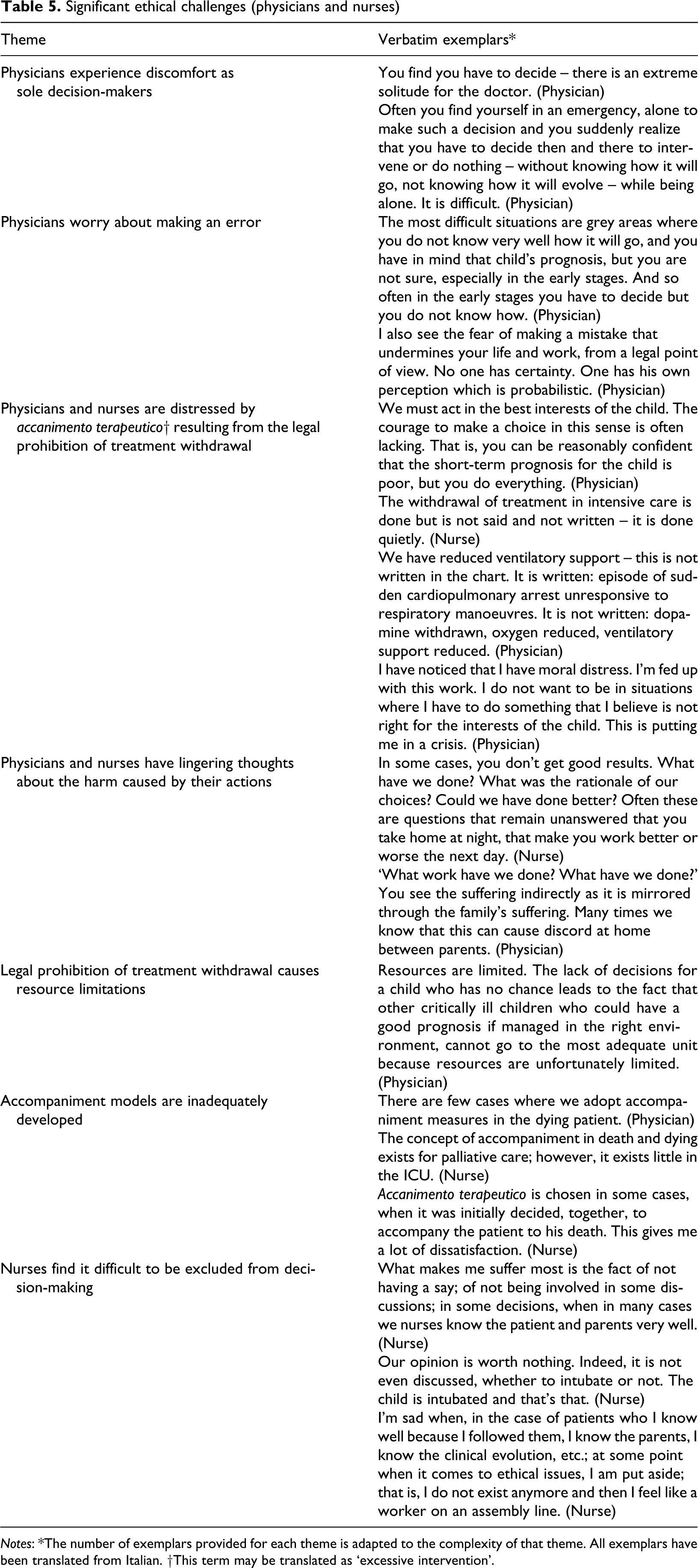
Notes: *The number of exemplars provided for each theme is adapted to the complexity of that theme. All exemplars have been translated from Italian. †This term may be translated as ‘excessive intervention’.
Thematic analysis of parent interviews
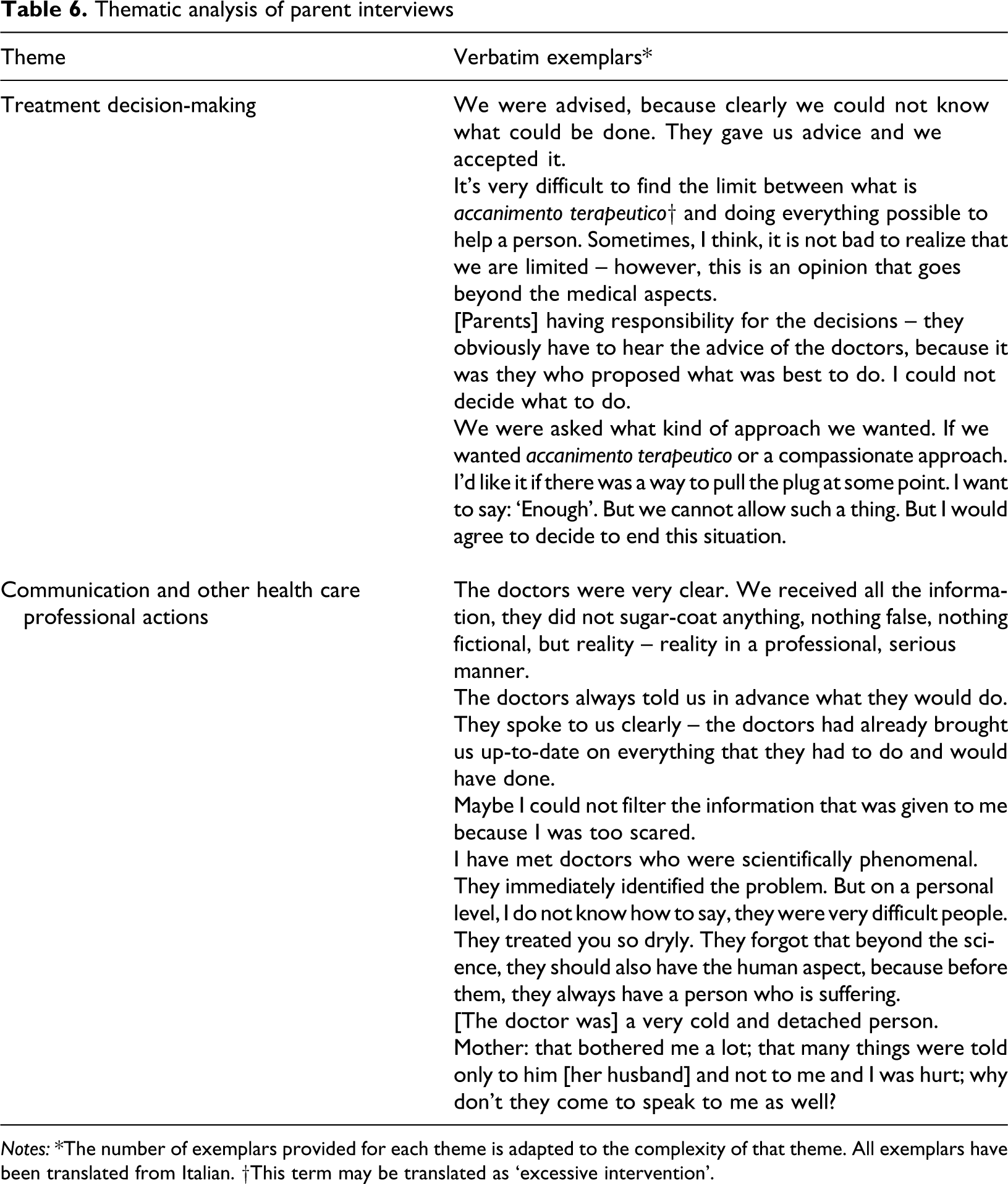
Notes: *The number of exemplars provided for each theme is adapted to the complexity of that theme. All exemplars have been translated from Italian. †This term may be translated as ‘excessive intervention’.
Decision-making process
On-call physician is responsible for making life-sustaining decisions
Participants reported that the principal responsibility for LST decisions rests with the on-call physician. Ordinarily, this physician seeks input from other physicians. Decisions are sometimes made with parents and nurses as well.
Parents are involved but do not bear responsibility for life-sustaining decisions
Parents are regarded as important participants in treatment decisions. Although their views should be considered, participants affirmed that parents should not bear responsibility for these decisions. Responsibility should rest with the physician. Some nurses reported that physicians had a significant influence on parental treatment preferences.
Nurses commonly feel excluded from treatment decision-making
Nurses described the important contributions to decision-making that they could make, given their relationships with patients and parents. Although some physicians discussed the merits of involving nurses in such decisions, nurses reported that they were commonly excluded from decisional processes.
Legal prevention of treatment withdrawal results in ‘accanimento terapeutico’
Participants reported that withdrawal and withholding of LST are regarded differently in Italy – withdrawal of LST is not legally permitted (NB: this complex legal issue is examined in the Discussion). The inability to withdraw LST sometimes results inaccanimento terapeutico. The closest English translation for this term would be excessive intervention; where overly aggressive interventions are given that health care professionals (HCPs) do not believe are beneficial. Once it has been decided to initiate LST, HCPs feel bound to continue until the child dies despite these efforts, regardless of what they think is best for the child.
Other considerations
Additional decision-making considerations included: looking at prior treatment decisions; developing procedures to facilitate decision-making; consulting with an ethics committee; examining the possibility of transfer to another centre; and re-examining the case over time.
Decision-making criteria
In acute situations, the default practice is to provide full LST. However, some children fall within a grey zone, where their condition or prognosis is unclear. When in doubt about the child’s condition, the usual approach is to provide full measures. This becomes difficult as the grey zone becomes larger. The merits of maintaining LST are questioned – despite the legal challenges – when the treating team has assessed that: the child has severe neurological injury, does not respond to therapy, or will not survive treatment; LST will prolong suffering; LST will not ensure the minimal requirements for living; or the parents prefer that LST be discontinued.
Significant ethical challenges
Physicians experience discomfort as sole decision-makers
Physicians reported significant discomfort over being the sole decision-maker for critically ill children, frequently feeling alone and unsure about the right course of action.
Physicians worry about making an error
Physicians were stressed by worries over making an error, particularly in the common context of uncertainty with PICU cases.
Physicians and nurses are distressed by accanimento terapeutico resulting from the legal prohibition of treatment withdrawal
Physicians and nurses acknowledged that treatment should be decided in terms of the child’s best interests. But it is their understanding that LST withdrawal is legally prohibited, even if such treatments are considered contrary to the child’s interests. Thus, physicians commonly direct parents towards maintaining life-support. This may result inaccanimento terapeutico. Participants related this problem to the Catholic background of many Italian people, as well as the ‘pro-life’ position expressed by Italian bioethical committees. This results in moral distress and upsetting actions. For example, treatment withdrawal was sometimes undertaken anyway, when it was considered best for the child and with parental agreement, yet this was not openly documented in the medical record.
Physicians and nurses have lingering thoughts about harm caused by their actions
Physicians and nurses are frequently bothered by persistent thoughts about the injuries and consequences of their actions. These include harms to children surviving with significant disabilities and the tremendous impact on families.
Legal prohibition of treatment withdrawal causes resource limitations
The difficulty in withdrawing LST sometimes results in resource limitations; where HCPs are unable to provide adequate care to children with a good prognosis, sometimes transferring them to other centres.
Accompaniment models are inadequately developed
Physicians and nurses reported thataccompaniment models of care for life-limiting illness (e.g. Anglo-American palliative care), have not been adequately developed in Italy.
Nurses find it difficult to be excluded from decision-making
Nurses reported that they commonly know their patients and families well, but felt their opinions were not valued. They believed that their exclusion from decision-making sometimes resulted inaccanimento terapeutico because their input was not considered. Moreover, having an individual physician as the sole decision-maker results in highly variable decisions that nurses believe should be more consistent. Some nurses described situations where their input had a favourable impact on the actions of physicians, reinforcing the importance of their involvement in treatment decisions.
Additional issues
Other issues related to: the optimal involvement and responsibility that parents should have in treatment decisions; nurses struggling with inadequate pain management; working with diverse religious communities; and HCPs managing their opinions where practices may conflict with their personal views.
Parent interviews
Parents were recruited from the same general hospital PICU in Verona from which hospital physicians and nurses were recruited. However, their critically ill children also received care from other hospital centres. Findings include comparative parental reflections relating to all these settings. Nine parent participants were drawn from seven families; seven mothers and two fathers – parents of eight critically ill children (i.e. one parent had two critically ill children). Five parents’ children were living; four parents’ children had died (Table 3).
Parents’ descriptions of treatment decision-making are presented first, followed by comments relating to communication and other HCP actions (Table 6). Additional parental reflections regarding their experiences are outlined inTable 7 .
General parental reflections regarding their experience
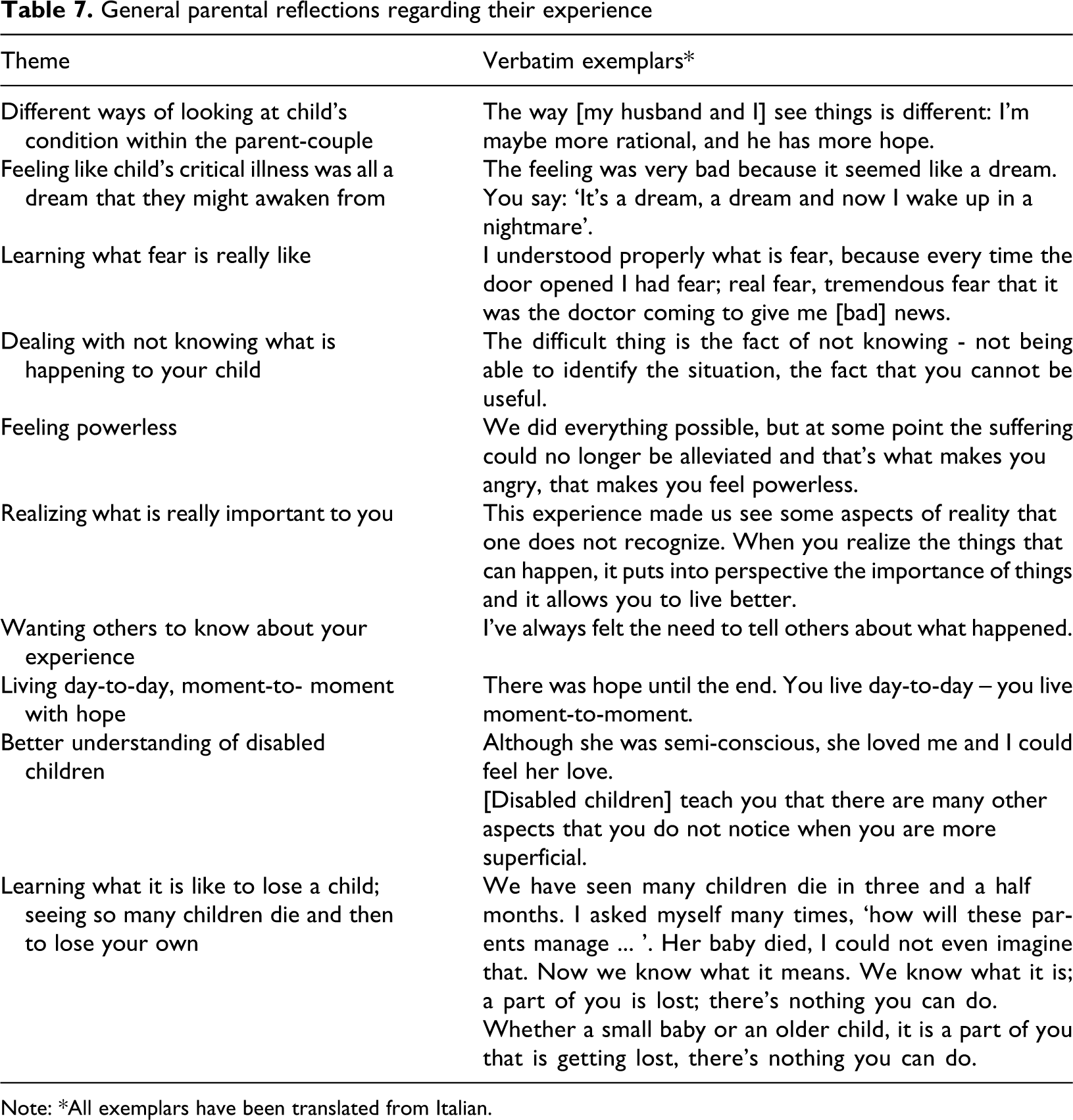
Note: *All exemplars have been translated from Italian.
Treatment decision-making
Parents felt that treatment decisions were directed by the physicians, with the accord of parents. Physicians explained the child’s condition and their treatment plan to parents. Although some parents described themselves as responsible for their children’s treatment decisions, the responsibility was shared with physicians. Several exceptions were also described. In emergency circumstances, physicians decided on their own, on the basis of what would be best for the child. Parents considered this as the right course of action, but were sometimes upset about being excluded. Some parents took the lead in seeking care elsewhere when they were unsatisfied with the care their child was receiving.
Parents favoured treatments that would increase the likelihood of survival and relieve the child’s suffering. They were comforted when they felt their children received all the care they required. Some felt it was acceptable to withdraw LST under some circumstances, but the responsibility for this decision should be shared with physicians. One parent, whose child at the time had significant neurological injury and was projected to have severe disabilities, was distressed because LST withdrawal was not offered for her child.
One couple wondered if their child could have had better chances if they were wealthy. They did not suspect that care for their child was deliberately limited because their modest finances; they wondered how they could ensure their child received every possible treatment.
Communication and other care professional actions
Parents appreciated receiving clear and complete information on a regular basis and when they requested an update, presented in a humane manner. Parents found it helpful when physicians explained what they planned to do in advance.
Parents appreciated it when: HCPs were welcoming to them and their children; HCPs appeared composed in their work; and they could spend as much time as possible with their children in the PICU without feeling negatively judged by staff.
Parents found physician communication problematic when physicians appeared cold, rushed and detached. One mother was upset that physicians tended to provide information primarily to her husband, and not to her. Moreover, given that physicians may provide information differently in different units, parents wanted to know when and how information would be provided in each setting.
One mother pointed out that communication can be compromised by a parent’s emotional state – it can be difficult to understand information when upset about the child’s condition. For another mother, it was important that HCPs (and others) did not express pity or discouragement towards her or her child. One parent was offended when she understood that the HCP had reservations about treating her daughter because of the costs this would entail.
One couple was encouraged to go home to sleep for the night; following a surgical procedure, after they had spent 24 hours per day with their child for several months. Their child died that night. These parents lived with persistent distress from not being with their child during her death.
Additional suggestions addressed how parents’ experience could have been improved, including: staff should understand that parents are sometimes very tired, affecting their behaviour and ability to understand; hospital rules should be flexible (e.g. permitting parents to stay as much as parents think is necessary); and basic facilities (e.g. bathrooms) should be close to the child’s room.
Integration of physician, nurse and parent data
Drawing on a term developed byBluebond-Langner (1978), this study sheds light on theprivate worlds of physicians, nurses and parents. The term ‘private’ is used to highlight the fact that participants’ respective moral concerns are poorly understood by the other subgroups. Physicians struggle with the weight of responsibility and solitude for making life-and-death decisions. Nurses struggle with feelings of exclusion from decisions regarding patients and families they care for. Physicians and nurses are distressed because they cannot openly consider treatment withdrawal and suffer deeply when they feel compelled to engage inaccanimento terapeutico; living with persistent malaise over the consequences of their actions for patients and families. These difficulties are related to the particular challenges of being a PICU physician or nurse.
Parents struggle with their dependence on HCPs to provide care for their child and strive to understand what is happening to their child. They depend on physicians and nurses for vital information as well as accommodations to remain with their child.
Physicians, nurses and parents suffer tremendously and privately. They know very little about each other’s suffering as they struggle with their respective worries, with the slight exception of physicians and nurses who have some understanding of parents’ experiences because they commonly try to assess parental concerns.
Discussion
Physicians struggled with the weight of decisional responsibility. It is unclear how this has become physicians’ sole responsibility. Italian law recognizes parents as the usual decisional agents for children, as in most Western societies (Cuttini et al., 2009). For LST decisions, Italian physicians appear to practice ‘beneficent paternalism’, as articulated in the French paediatric literature (Carnevale et al., 2007;Hubert et al., 2005). The rationale for this position has not been as thoroughly examined in the Italian literature (Cuttini et al., 2009). Parents did not question the central role of physicians in treatment decision-making, yet they also saw themselves as important participants.
Nurses’ disclosures correspond with those reported elsewhere (Burns et al., 2001;Storch et al., 2004). In recent years there has been a growing recognition of nursing as an autonomous profession. Nurses are responsible for assessing patients’ needs and ensuring their care responds to these needs. This is formalized through legislation and codes of ethics defining legal and ethical nursing obligations (Codice infirmiere, 2009). Nurses in this study expressed distress over their lack of participation in LST decisions, resulting in a ‘caught in the middle’ moral bind (Hamric, 2001). They felt torn between their duty to comply with physician-prescribed treatments and their duty to serve their patients’ best interests, which for nurses are sometimes incongruent.
A major source of distress among physicians, nurses and parents are the reported legal restrictions on LST withdrawal. Participants were largely aware that in other Western settings, where no ethical distinction is drawn between withholding and withdrawing LST, LST can be withdrawn if considered excessively burdensome and without a reasonable prospect of patient benefit (AAP, 1994;CPS, 2004). The resulting distress of Italian physicians and nurses resembles what has been referred to as moral distress: distress resulting from feeling restricted from doing the right thing (Austin et al., 2009). Moral distress among Italian physicians and nurses is predominantly associated with the risk of performingaccanimento terapeutico and living with the responsibility of causing needless harm.
Physicians and nurses appeared to know relatively little about each other’s moral distress. Strategies for strengthening physician–nurse discussion and collaboration should be considered, such as facilitated inter-professional case discussions (Carnevale, 2005;Puntillo and McAdam, 2006).
The legal basis of the prohibition of treatment withdrawal in Italy is unclear. Italian law and medical and nursing codes of ethics indicate that consent is required for care and that treatment decisions for children should be based on the child’s best interests (Codice infirmiere, 2009;Codice medica, 2006;Cuttini et al., 2009;Giannini et al., 2008). Thus, when physicians, nurses, and parents agree that continued LSTs are contrary to the child’s best interests, it would seem legally permissible, if not obligatory, to withdraw these treatments. However, LST withdrawal is not specifically regulated under any written source of Italian law – it is not explicitly permitted or prohibited (Cuttini et al., 2009). This legal uncertainty seems rooted, at least partially, in the juxtaposition of Western ‘quality of life’ values supporting the withdrawal of LST being considered contrary to the patient’s interests and the Catholic ‘sanctity of life’ values espoused by some Vatican doctrine. This was highlighted in the publicized Italian case involving feeding cessation for Eluana Englaro (Donadio, 2009). Some literature corroborates our finding that HCPs sometimes feel compelled to secretly limit, if not withdraw, LST (Smiderle, 2008).
Given this legal uncertainty, HCPs are reticent to openly discontinue such treatments. With the ongoing proliferation of LSTs, legal clarity regarding the withdrawal of LSTs should be urgently established in Italy.
This study also sheds light on how critical care can be adapted to the needs of parents. Communication between HCPs and parents was identified as an important concern. Communication has been gaining attention in the paediatric critical care literature (Eggly et al., 2010;Feudtner, 2007;Levetown, 2008;Meyer et al., 2009). This Italian study highlights the features of helpful and unhelpful communication, which appear relevant for other settings as well. These should be considered in PICU educational and practice changes.
Despite the important contributions made by this investigation, the study had some limitations. First, the study was restricted to the Italian context. Relevance of the findings for other settings may be limited, depending on the comparability of the practice contexts. Nurse participants included women only. Future research should also examine the perspectives of male nurses. Physician and nurse sampling drew participants from various settings to ensure a diversity of perspectives, however, parent sampling was restricted to the Verona region because of logistical considerations. A larger-scale Italian study of parental experiences is needed. Finally, although all findings were supported by multiple participants, a consensus was not sought for each theme. It is acceptable for diverse themes to emerge within a single focus group, revealing the range of perspectives within the group. However, some focus group members may have been reluctant to disclose counterviews in some instances.
This study contributes to a growing body of international investigations of ethical concerns in paediatric critical care. This research enriches our understanding of ethical concerns, both in Italy and abroad, by shedding light on complex matters such as decision-making responsibility, treatment withdrawal, physician–nurse collaboration, as well as physician, nurse and parent roles.