
Abstract
It is increasingly accepted that children have the right to have their views taken into consideration by healthcare providers. Children’s opinions and experiences of hospitalisation are essential for monitoring and evaluating the effectiveness of health services provision. In this paper we report on children’s views and wishes about hospital and healthcare professionals. The children held both positive and negative views of hospital and healthcare professionals. Dissatisfaction was caused by insufficient information, lack of involvement, and inadequate play facilities. Their wishes were mainly concerned with the need for more information and more involvement in communication interactions with doctors and nurses. They wished to express their opinions, ask questions and receive information about care and procedures. They recommended that healthcare professionals make a better effort to listen and to take account of their views.
Introduction
My one big wish is that nurses and doctors would explain things better to children (Child, 10 years).
Internationally, there has been a noticeable change in the attitudes towards children with increasing recognition of their ability to contribute to society (Alderson 2008, Department of Health & Department for Education and Skills 2009, Franklin & Sloper 2009). The United Nations Convention on the Rights of the Child (1989) stated the child’s fundamental right to be listened to and to openly express their opinions on issues that concern them. Since then considerable efforts have been made by a number of organisations to raise awareness of children’s rights, particularly in relation to the opportunities provided to children to express their views and preferences (European Association for the Care of Children in Hospital 2010, United Nations Children’s Fund 2003, United Nations General Assembly 2002). Similarly in Ireland, the National Children’s Strategy (2000) aimed to create ‘an Ireland where children are respected as young citizens with a valued contribution to make and a voice of their own’ (Department of Health and Children 2000, p4).
It is a key principle of hospital standards that hospital services are child-centred, and that children’s views are taken into account in matters affecting their lives (Department of Health 2003). Eliciting children’s views and preferences are essential if we are to provide services that are responsive to their needs. However in the past, parents and healthcare professionals’ views have been sought on children’s care and experiences, instead of the child’s perspective (Sommer et al. 2010). Hospitalised children are at risk of having their rights overlooked or disregarded due to the perception that they are immature and/or that they are incapable of expressing their views and opinions (Nova et al. 2005). Children are capable of providing new perspectives and ideas on the delivery of healthcare services, so their views should be sought (Coad et al. 2008).
Background
There is a growing body of research into children’s experiences of hospitalisation. Although experiences of hospitalisation may vary from child to child, the research highlights particular areas of hospital life that concern many children. These areas include unfamiliar hospital environment; separation from family and friends; intrusive investigations; needles and blood tests; communication with healthcare professionals; and acknowledgement of children’s opinions (Carney et al. 2003, Coad & Houston 2007, Coyne & Conlon 2007, Pelander & Leino-Kilpi 2010). The research suggests that children’s views are seldom elicited or considered in the development and implementation of hospital policies and the delivery of health services (Curtis et al. 2004). Yet children’s opinions and experiences of hospitalisation are essential for monitoring and improving the quality of health services provision (Vessey 2003). There is increasing interest in exploring children’s views on hospital environments and services (Coad & Coad 2008) but less studies into children’s preferences for participation in decision-making (Coyne 2008, Martenson & Fagerskiold 2007). Clearly there is a need for information on children’s experiences of hospital life and participation in healthcare matters. Therefore we conducted a study to elicit children’s perspectives on participation in information-sharing and decision-making and the data from the interviews are reported elsewhere (Coyne & Gallagher 2011). In the same study we used participatory techniques to elicit children’s wishes and views on hospital and healthcare professionals and these data are reported here.
Method
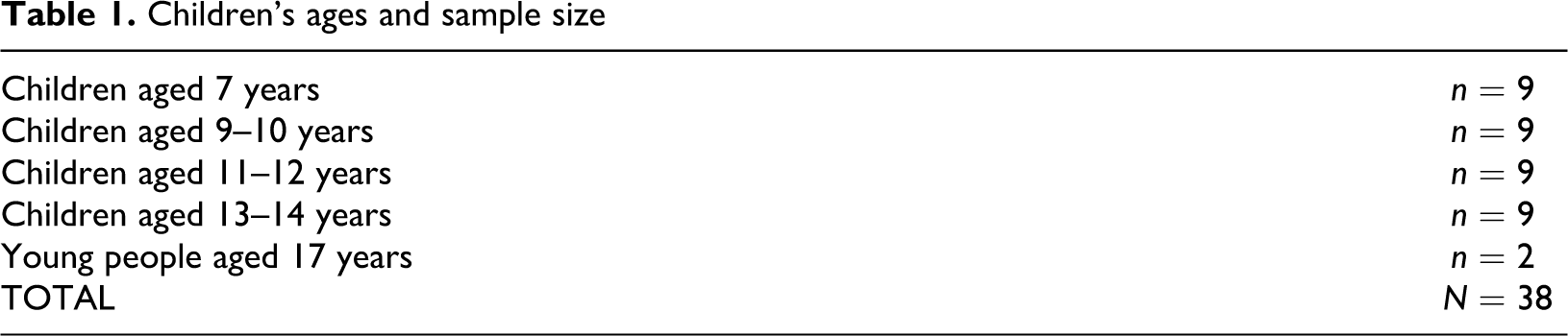
Using a qualitative descriptive approach (Sandelowski 2000), we obtained data from children (n = 55) aged 7-18 years from two children’s hospitals and one district general hospital in Ireland. The sample consisted of children with acute (n = 27) or chronic illnesses (n = 28) who had at least one overnight stay in hospital. Ethical approval was obtained from the ethics committees for each hospital and verbal and written assent obtained from each child and consent from the parent. Interview questions were focused on the hospital environment and facilities; healthcare staff communication; and child’s participation in decision making and care. In addition we used two types of participatory techniques that were: sentence completion and 3 wishes exercise (O'Kane 2000). The participatory techniques were used to assist children in expressing their views through a less formal method of interviewing. Each child was asked to complete three sentences to aid them in expressing their opinions of hospital life. The children were also asked to disclose three wishes based on their stay in hospital. Sentence completion can provide children with the opportunity of expressing their feelings about both negative and positive aspects of care. But the completion technique may be constraining for some and may feel like a form of test. The sentences started with: hospitals are…. ’ and ‘doctors are….’ and ‘nurses are….’ We asked the children prior to or at the end of the interview if they would like to participate in either technique. From the sample there were 17 children who did not wish to participate in either participatory technique and their wishes were respected. Therefore we obtained data using both participatory techniques from 38 children (See Table 1 for sample).
Children’s ages and sample size
Data analysis
The data analysis began with transcribing all the children’s statements verbatim. Using content analysis, the children’s statements and wishes were then examined for meaning and similar statements coded (Hsieh & Shannon 2005). The codes adhered closely to child’s own words. The codes were discussed among the research team until all were satisfied that codes clearly represented the data. The codes were then grouped into key categories. Statements that did not fit into any category were grouped separately as ‘children’s other wishes’.
Results
The children’s statements and wishes centred around the hospital facilities; views of doctors and nurses; communication interactions with doctors and nurses; and participation in decision making.
Hospital facilities
The children held both positive and negative views of hospital and hospital facilities. Most viewed hospital as a place to get better and a place where they could recover and rest. Some children appreciated being able to have familiar items from home such as toys and game consoles. They viewed hospital as a fun place with friendly people. Hospitals are good fun because you can play the PlayStation and your friends can visit you (Child 14 years). Hospitals are scary when you aren’t given enough information about them (Child 9 years). You should visit the hospital first because you will have to see the good and bad points about hospital (Child 10 years). There is hardly any room for the nurses to get in and out. It’s just tiny and we should have our own toilets. We need games, books, somewhere to chill out with a telly and nice sits (couch) because it’s hard being in hospital without anything to do. We need something to take our minds off things instead of staring at the walls all day (Young person 17 years). They should have more things for parents to play with (Child 11years). I would like that there should be a bed for Mams and Dads beside their children (Child 9 years).
Views of doctors and nurses
The children viewed nurses and doctors as the healthcare professionals who help make them ‘better’ and whom provide medication that cures their illness. The doctor was the person who diagnosed the illness and cures the ‘sickness’ as they perform medical procedures, such as operations. Doctors are people who help cure whatever is wrong with you (Child 13 years). Nurses are helpful and kind and always listen (Child 12 years) Doctors are nice and give you medicine (Child 7 years) Student nurses have more time for patients than qualified nurses. If I had a question I would ask a student nurse as I think they have more time (Young person 17 years).
Communication interactions with doctors and nurses
Children suggested that healthcare professionals should speak to them using child-friendly language and shorter sentences. A doctor should explain things to you in a way that you’ll understand. Like if you have to fast ask why you have to and what it has to do with your sickness instead of using words you don’t understand. Like I didn’t understand appendicitis (Child 9 years). It is better if the doctor tells you things stage by stage instead of telling you in one big sentence (Child 13 years) Doctors should be able to tell you what is going to happen before it happens not after (Child 11 years). I think that doctors should tell them straight away what is wrong with them and what they are going to have to do to make sure the child is ok with everything that is going on (Child 13 years). Some doctors would ignore you and tell you nothing. When I ask questions I would like to be listened to because if I am not listened to it makes me feel disappointed and upset (Child 11years). Doctors don’t give you enough time to talk to them because they are always busy going to other patients (Young person 17 years). Doctors are alright but don’t explain what’s happening to you. They don’t really talk much (Young person 17 years) Sometimes you might not be able to ask questions because you might be worried of what the doctor/nurse will say. For example they might say that you have done something wrong to your body (Child 13 years) My comment would be for doctors not to get annoyed with children asking questions because they just want to know what’s going to happen to them (Child 13 years). You should listen to them no matter how silly the questions are. You should keep everyone informed and answer all questions (Child 13 years). If doctors and nurses work in a children’s hospital they should be able to talk to children in a language that children can understand (Child 11 years). My wish is that doctors and nurses talk to me (Child 7 years). I think that they should explain the important parts to children instead of saying it in long words to the parents (Child 11 years). Doctors and nurses should tell us stuff before our parents because it is us in the hospital with something wrong and not them. Doctors should talk to you as well as your parents (Child 10 years). When a doctor tells you to leave the room and talk to your parents it makes me scared and I think he should include me (Child 11 years). If it is about me I should be part of the conversation not doctors taking my Mam to another room (Child 12 years)
Views on decision -making
One young person preferred her mother to communicate on her behalf as she was not ready to make decisions on her own. At 17 I don’t feel ready enough to make decisions on my own so I prefer my mum to ask and answer questions for me (Young person 17 years).
Some children thought that the doctors were ‘smart’ and therefore should make most decisions for them. I feel that doctors should make most decisions (Child 11years). It is my decision because I will be the one in the operation (Child 10 years) I think that children or teenagers have the right to make their own decisions and be independent if they were brought up to be allowed to make their own decisions. Also if they are responsible and mature enough to make their own decisions (Child 13 years). There shouldn’t be an age group when it comes to making decisions. The doctors should explain it to all age groups and they explain it very well and they make you feel included (Child 14 years) Children are very important as well. Don’t judge them because they are young and help the ones that are in need. Always include children in decisions. (Child 13 years) My wish is for children to get a say. Decisions should not be made without children’s say (Child 12 years) Doctors and nurses should let you make your own decisions if you are fully mature and informed. For preparing older children (11+) they should be told exactly what’s going on because if you’re fully informed, you can make better decisions (Child 13 years).
Children’s other wishes
Most children wishes were that they would recover quickly and that their stay in hospital would be as short and as enjoyable as possible. Children were aware of good outcomes from being in hospital such as getting better, being helped and going home. My wish is to make children better. My wish is to make medicine work for children (Child 7 years). I’d wish that children would be o.k. and they wouldn’t be scared. If the doctors were nice to them I’d be happy about little kids being in hospital (Child 7 years) My wishes: I would never like to be alone. I would never like to be hurt. I would never like to be sad (Child 8 years) My wish is that the children would not have to go to hospital (Child 10 years) To know: Why does God make children sore and sick? (Child 7 years)
Discussion
The findings show that hospitals are places that could be fun as well as threatening. However some children experience hospital as a ‘scary’ place due to fear of unknown, lack of information and inadequate preparation. Feeling safe, having parents nearby, and having familiar objects from home help children cope (Coyne 2006b, Forsner et al. 2005). The importance of preparation in reducing uncertainty is well known (Justus et al. 2006) yet children continue to report inadequate information and lack of preparation (Carney et al. 2003, Smith & Callery 2005). Despite recognition of the need for better play facilities and areas for socialisation for hospitalised adolescents, these unmet needs continue to be reported (Children in Hospital Ireland 2000, Curtis et al. 2007). Hospitals should be designed to accommodate children of all ages, and should include spaces for socialisation, access to computers, movies and games, and therapies such as pet and music. Preparation programmes should be available for all planned admissions. Information booklets or videos could be used for unscheduled admissions. These interventions will help reduce anxiety when children know what happens in hospital and what to expect.
Children held both positive and negative opinions of nurses and doctors. Doctors were seen as having a curative role, and were described as clever and friendly. Nurses were viewed as having a caring role and being helpful and kind. Nurses were seen as having more time for listening than doctors. This indicates that healthcare professional’s personal characteristics are important elements in quality care (Pelander & Leino-Kilpi 2004, Schmidt et al. 2007). Although there were positive statements about the healthcare professionals, many children were critical of healthcare professionals’ communication style, felt that they were not given sufficient information and experienced obstacles towards having their voices heard. Children found it difficult to understand doctors’ communication due to medical jargon, medical terms and use of lengthy sentences. They wanted healthcare professionals to use simpler terms and explain information in small amounts. Children wanted time to voice their opinions and ask questions, but experienced difficulty being heard (Beresford & Sloper 2003, Curtis et al. 2004). Being heard and being listened to by doctors and nurses was highly valued and when children felt ignored it made them feel upset. The children stated that explanations and information would help them participate in decisions. Some children aged ten upwards felt that involvement in decisions should not be determined by a child’s age or maturity; instead all children should be included. Likewise Alderson argues that children’s competence should be situation-specific rather than age related and thus should be assessed in each situation rather than assumed (Alderson 2007).
It seemed that the attitudes and behaviour of healthcare professionals influenced the children’s willingness to participate and ask questions which has been reported before (Coyne 2006a, Hallstrom & Elander 2004). Healthcare professionals may be very supportive of children’s participation but be not aware that their communication is unclear. In a survey of Irish nurses and doctors (n = 102), over 90% felt they used appropriate explanations in discussions with parents and children (Migone et al. 2008). But this current study would indicate that the perceptions of children are different to those of healthcare professionals. Therefore healthcare professionals need to critically examine their communication approach with children, and if necessary improve their skills by attending communication skills training and educational updates. They should be careful with usage of complex language and medical jargon, use simple words and tailor the information to the child’s level of understanding. They should continually seek out and listen to wishes, opinions, and choices in each child’s expression. Being busy and lacking time should not be used as justification for brief explanations or non-involvement of the child. Runeson and colleagues found that children who were included from the start in discussions about their treatment actually required less time from healthcare professionals during the actual procedures (Runeson et al. 2001). Children need to feel safe in hospital and being listened to and being heard are essential in helping children feel secure and respected (Coyne & Gallagher 2011). There is evidence that including children in healthcare consultations holds benefits such as better understanding (Boylan 2004), reduced perception of pain (Runeson et al. 2002), feeling valued (Dixon-Woods et al. 2002), feeling prepared and less anxious (Coyne 2006a). The long term benefits include increased sense of control, enhanced self-esteem and a more active role in self-care (for chronic illnesses particularly) (Hanna & Guthrie 2003, Leveton 2008).
Healthcare professionals need to support children’s efforts to participate in healthcare decisions as it is very difficult for children to interrupt or challenge ‘important’ or busy professionals. Simple measures can be used by healthcare professionals to involve a child such as asking if he/she has any questions and giving the child time to respond and taking a child’s opinion into consideration by offering alternative treatment choices. When children experience non-inclusion they can feel rejected, sad and ignored (Coyne 2006a). The adverse aspects of hospitalisation can lead to negative outcomes for some children after hospitalisation such as anxiety, sleep disturbances, sadness and anger (Melnyk 2000). It is essential therefore, that children’s needs for participation are recognised and enabled.
Limitations
The data could have been influenced by the questions in the interview schedule which focused on information-sharing and decision-making. The interview may have raised the children’s awareness of these issues and thus caused them to include them in their wishes.
Conclusion and recommendations for further research
Children prefer to be included in information-sharing and discussions about their care but experience difficulty having their communication needs met. They prefer inclusion as this helps reduce their fears, anxieties and helps them have a more positive experience. Preferences can vary therefore preparation and information needs to be tailored to the child’s preference and wishes. Asking children for their preferences is essential if we hope to improve quality of care provision (Lindeke et al. 2006). It is important that healthcare professionals recognize the benefits of including children in communication and everyday decision-making. Allowing children time to voice their opinions and to ask questions may seem trivial but it can make a significant difference to children’s wellbeing and psychological health. With increasing cultural diversity and global mobility, further research is required to examine the effect of language on the inclusion of children in healthcare decisions. In this era of advanced communication technologies, it would be useful to research children’s preferences on receiving information via technological tools than face-to-face since it is often inadequate. Furthermore follow-up studies with children after discharge would be useful to determine if non-involvement in decision-making leads to negative psychological sequelae. In conclusion it is important that doctors and nurses are cognisant of children’s need and right for inclusion and work towards improving their practices of listening, hearing and involving children in all healthcare matters.
Footnotes
Acknowledgements
We wish to thank all the children and young people who participated in the study, and the nursing and medical staff who kindly facilitated our presence on the wards.
Funding
We gratefully acknowledge the research funding provided by the Office of the Minister for Children, Department of Health and Children, Ireland.