
Abstract
Research has shown mixed findings about the relationship between parenting style and child lifestyle outcomes. This paper describes a cross-sectional study that aimed to clarify the relationship between ineffective parenting and childhood obesity by using multiple measures of child and family functioning. Sixty-two families with an obese child (aged four to 11 years) were matched with 62 families with a healthy weight child on key sociodemographic variables. Significant differences were found on several measures, including general parenting style, domain-specific parenting practices, and parenting self-efficacy (d = .53 to 1.96). Parents of obese children were more likely to use permissive and coercive discipline techniques, and to lack confidence in managing children’s lifestyle behaviour. In contrast, parents of healthy weight children were more likely to implement specific strategies for promoting a healthy lifestyle.
Introduction
Parents’ knowledge, skills, confidence, and behaviour affect children’s language development, intellectual ability, social skills, behavioural competence, and physical health (Collins et al., 2000). However, most of the research evaluating the impact of parenting on child development has focussed on children’s aggressive and disruptive behaviour, and far less research has evaluated the impact of parenting on children’s health behaviours. Overweight and obesity are recognised as significant population health problems and up to a third of children are classified as overweight or obese (Wang and Lobstein, 2006). There is increasing evidence that parents play a critical role in shaping children’s dietary and activity patterns (Davison and Birch, 2001); however, clear support for a link between child overweight and parenting style has not yet been established, and ‘the literature remains conflicting regarding the role of parenting in the genesis of childhood obesity’ (Wake et al., 2007: p.e1526).
Parents can influence child lifestyle patterns via multiple pathways, including direct modelling and reinforcement (Epstein, 1996), arrangement of the family food environment (Benton, 2004), provision of activity options (Gustafson and Rhodes, 2006), and parent–child interactions over food and activity (Golan and Crow, 2004). Parents have typically demonstrated a lack of awareness about the dietary and physical activity guidelines for children (Hesketh et al., 2005), and reported a lack of knowledge about effective strategies for managing children’s weight, and difficulty in monitoring and controlling children’s eating behaviour (Borra et al., 2003). What is more, societal messages about what constitutes healthy, unhealthy, fit and active are often ambiguous, inconsistent, and confusing for parents (Hesketh et al., 2005). Therefore, it is not surprising that many parents lack confidence in managing their children’s lifestyle behaviour (West and Sanders, 2009).
Different aspects of parenting have been examined in the childhood obesity literature, including global parenting style (e.g. permissive versus authoritarian parenting); domain-specific parenting style (i.e. parenting style in the context of feeding) (Hughes et al., 2005); and specific parenting strategies in the feeding context (e.g. promising dessert in exchange for eating vegetables) (Ventura and Birch, 2008). Authoritarian or coercive parenting styles have been associated with a higher risk of overweight (e.g. Berge et al., 2010; Rhee et al., 2006; Sleddens et al., 2011) and with less self-regulation in children’s eating (e.g. Joyce and Zimmer-Gembeck, 2009). However, some studies have not found a link between child overweight and parenting style (e.g. Hennessy et al., 2010; Wake et al., 2007). Similarly, permissive child feeding styles are more common in parents of obese children than parents of healthy weight children (e.g. Moens et al., 2007; Rhee et al., 2006). The focus of research to date has been on specific parenting feeding behaviours (Hughes et al., 2005; Rhee, 2008), and some studies have found a relationship between these specific feeding behaviours and child overweight, but not between a more general parenting style and child overweight (e.g. Brann and Skinner, 2005; Moens et al., 2007).
In addition, methodological considerations hamper conclusions about the relationship between parenting style and child overweight. Studies have typically involved very small samples, which may not be representative of the general population. Few studies have adequately matched their healthy weight and obese groups, or included appropriate statistical controls for multiple comparisons. There has also been inconsistency in measures and definitions of parenting style in the literature. One final criticism of the literature is that generally studies have not reported effect sizes nor gauged the clinical importance of significant differences.
Aim and hypotheses
The aim of this study was to clarify the relationship between ineffective parenting and childhood obesity by identifying whether parents of obese children use different disciplinary practices and fewer health-promoting strategies compared to parents of healthy weight children. To address some of the shortcomings of previous research, a widely used and well-validated measure of parenting style was employed, as well as a lifestyle-specific measure of parenting practices. Hypotheses were as follows: (a) parents of obese children would report more frequent use of ineffective discipline practices, (b) parents of healthy weight children would report more frequent use of health-promoting strategies, and (c) parents of obese children would report lower self-efficacy. To explore possible family correlates in families with obese children, several measures were administered in addition to the parenting questionnaires. These measures assessed predictors of child body size and parental competence.
Method
Participants
Healthy weight sample
Families with healthy weight children aged four to 11 years were invited to participate in a study investigating childhood obesity. Advertisements were placed in school newsletters in Brisbane, Australia from May to September 2005. A total of 124 parents responded and participated in a standardised telephone interview to assess their family’s eligibility. The inclusion criteria were as follows: (a) the target child was between four and 11 years of age, and (b) the parent described the child’s body size as healthy. Families were excluded from the study if (a) the parent described any of the child’s siblings as obese, (b) the child was taking medication that affects growth or weight control, or (c) the child had a severe developmental delay or disability. Thirty-three families did not meet eligibility criteria, and a further nine parents declined to participate, leaving 82 families (66.1%) for this study.
Obese sample
The obese comparison group was drawn from a childhood obesity intervention study, for which parents were recruited to address their child’s weight concerns (West et al., 2010). These families were also recruited through a community outreach campaign, conducted from September 2003 to October 2004. Families were eligible to participate in the study if: (a) the target child was between four and 11 years of age, (b) the parent described the child’s body size as overweight, and (c) the parent agreed to attend a 12-week intervention. Families were excluded from the study if (a) the child was taking medication that affects growth or weight control, or (b) the child had a severe developmental delay or disability. A total of 205 parents responded and participated in an initial telephone interview to assess eligibility. Of these, 104 families (50.7%) did not meet inclusion criteria, declined to participate, or failed to complete written consent forms. However, only families with obese children (n = 78) were eligible to participate in this study (i.e. families with overweight children were excluded). Only baseline data for this group was utilised in the analyses for this study.
Matched sample
Families in the healthy weight group were matched to families in the obese group on the following variables: child sex, child age, parent sex, and family type (i.e. sole parent or two-parent family). Sixty-four matched pairs were derived and sociodemographic characteristics of the matched sample are summarised in Table 1. There were no significant differences between the groups. The matched sample is typical of the Australian general population in terms of parent age, ethnicity, family composition, family income and father’s employment; but levels of parent education and mother’s employment are slightly higher than national averages. Nearly all parents who participated in the study were mothers (96.8%), aged between 25 and 54 years (M = 39.19, SD = 4.84). Most mothers were married (71.8%) and lived with the child’s biological father (74.2%). Mothers had generally completed some form of post-school education (75.8%) and were employed outside the home (66.1%). Fathers also tended to be tertiary educated (85.7%), and worked an average of 44 hours per week. Total family income typically ranged from AUD$400 to AUD$2000 per week (71.0%). Children were aged between four and 11 years (M = 8.06, SD = 1.70), with 59.7% girls, and the majority were white (91.9%).
Sociodemographic characteristics of the matched sample (n = 124).
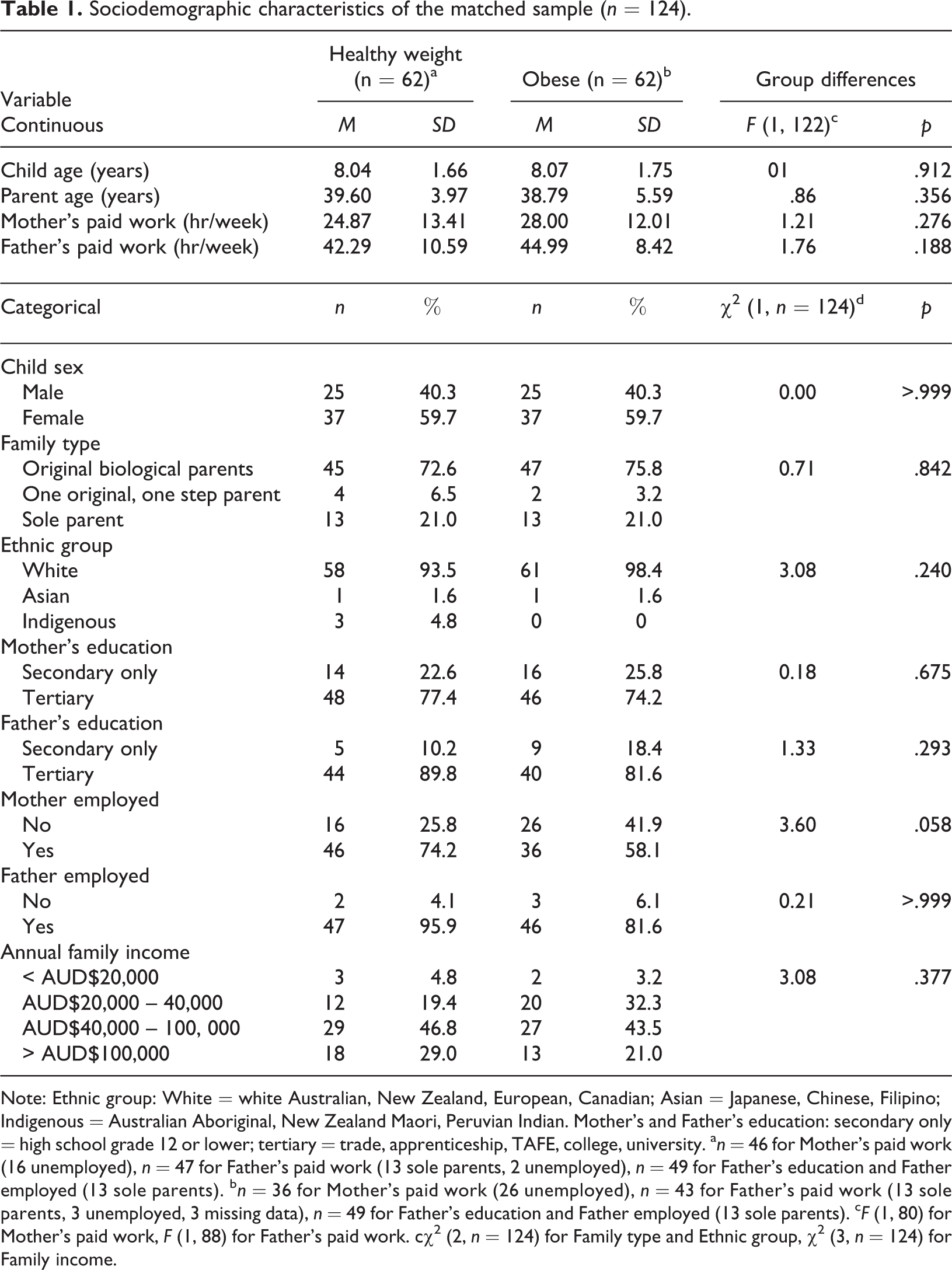
Note: Ethnic group: White = white Australian, New Zealand, European, Canadian; Asian = Japanese, Chinese, Filipino; Indigenous = Australian Aboriginal, New Zealand Maori, Peruvian Indian. Mother’s and Father’s education: secondary only = high school grade 12 or lower; tertiary = trade, apprenticeship, TAFE, college, university. a n = 46 for Mother’s paid work (16 unemployed), n = 47 for Father’s paid work (13 sole parents, 2 unemployed), n = 49 for Father’s education and Father employed (13 sole parents). b n = 36 for Mother’s paid work (26 unemployed), n = 43 for Father’s paid work (13 sole parents, 3 unemployed, 3 missing data), n = 49 for Father’s education and Father employed (13 sole parents). c F (1, 80) for Mother’s paid work, F (1, 88) for Father’s paid work. cχ2 (2, n = 124) for Family type and Ethnic group, χ2 (3, n = 124) for Family income.
Measures
Weight status
One parent and one child from each family participated in a measurement session. Height, weight, waist circumference, and bioelectrical impedance were collected using standard procedures (Davies et al., 2001; PSW Davies, November 4, 2003, personal communication). To ensure consistency, all measurements were performed by the second author. Height was measured to the nearest 0.1 cm using a custom-made portable stadiometer (constructed of a steel pole, wooden base, and metal tape measure), and weight to the nearest 0.1 kg using electronic scales (Metropol 62208, Soehnle, Murrhardt, Germany). Waist circumference was measured to the nearest 0.1 cm using an anthropometric tape (Figure Finder®, Novel Products Inc., Rockton, Illinois, USA) and impedance to the nearest 1Ω using a foot-to-foot bioelectrical impedance device (either Bodystat® 1500, Bodystat Ltd, Douglas, UK; or IMP5, Impedimed Pty Ltd, Mansfield, Australia). BMI was calculated from measured height and weight, and classified as underweight, healthy weight, overweight, or obese using the Australian standard definitions (Australian Government Department of Health and Ageing, 2002). The Centers for Disease Control (CDC) Growth Charts (Kuczmarski et al., 2000) were used to calculate BMI z scores for children (zBMI). Body fat was estimated from measured impedance using Davies and Gregory’s (1991) regression equation and Lohman’s (1989) constants for total body water. The following measures were used in analyses: weight (WGT), BMI (parents only), zBMI (children only), waist circumference (WST) and body fat (FAT).
Child lifestyle behaviour
Lifestyle-specific problem behaviour was assessed using the Lifestyle Behaviour Checklist (LBC) (West and Sanders, 2009). The LBC lists 25 problem behaviours related to eating, physical activity and overweight. For the Problem scale, parents rate how much of a problem each of the behaviours are with their child, on a seven-point scale from 1 (not at all) to 7 (very much). In the matched sample, the Problem scale had high internal consistency (α = .93).
Parenting
The Parenting Scale (PS) (Arnold et al., 1993) is a 30-item questionnaire measuring three dysfunctional discipline styles: laxness (permissive discipline), over-reactivity (authoritarian discipline, displays of anger), and verbosity (overly long reprimands or reliance on talking). Each item has a more effective and a less effective anchor, and parents indicate on a seven-point scale which end better represents their behaviour. Only the Laxness and Overreactivity scales were used in this study, and existing clinical cutoffs utilised. Factor analyses since the original validation study have supported the Laxness and Overreactivity scales but not the Verbosity scale (Rhoades and O'Leary, 2007). These had adequate internal consistency (α = .87 and .79, respectively).
Parenting self-efficacy was assessed using the Confidence scale of the LBC. Parents rate how confident they feel in managing their child’s behaviour for each of the problem behaviours. The confidence rating ranges from 1 (certain I can do it) to 10 (certain I can’t do it). The LBC Confidence scale had very high internal consistency (α = .97).
The Behaviour Change Checklist (BCC) was administered over the telephone. This checklist lists 10 daily steps parents can follow to promote a healthy lifestyle in their family (e.g. provide children with at least two servings of fruit, ensure 60 minutes of active play, praise or reward healthy behaviours). The BCC was developed to monitor parents’ implementation of strategies during a childhood obesity intervention, but was used in this study as a measure of lifestyle-specific parenting practices. The BCC steps were assessed using open questions and scored as 1 (completed) or 2 (not completed), then summed to give a total score out of 10.
Child adjustment
Child general behaviour was assessed using the Eyberg Child Behavior Inventory (ECBI) (Eyberg and Pincus, 1999), a measure of parental perceptions of disruptive behaviour in children aged two to 16 years. Parents rate the frequency of 36 behaviours on a seven-point scale from 1 (never) to 7 (always) (intensity scale), and identify which behaviours are a problem, using a yes/no format (problem scale). The ECBI scales had high internal consistency (α = .92 and .90 respectively).
Children’s emotional and social adjustment was assessed using the Strengths and Difficulties Questionnaire (SDQ) (Goodman, 1997), a behavioural screening measure consisting of 25 positive and negative attributes. Parents rate how much each attribute applies to the target child on a three-point scale from 0 (not true) to 2 (certainly true). In this study, only Emotional symptoms, Peer problems and Prosocial scales were administered. The internal consistency was fairly low (α = .67, .64, .67 respectively).
Parent adjustment
The Parent Problem Checklist (PPC) (Dadds and Powell, 1991) was used as a measure of interparental conflict over child-rearing. The PPC consists of 16 items, and parents identify which items have been a problem for them with their partner using a yes/no format (Problem scale), and rate the extent of the problem on a seven-point scale from 1 (not at all) to 7 (very much) (Extent scale). The PPC had moderate to high internal consistency (α = .76 and .90 respectively).
Relationship satisfaction was assessed using the Relationship Quality Index (RQI) (Norton, 1983), which consists of five statements about the quality of the relationship and asks respondents to rate their agreement with each statement on a seven-point scale from 1 (very strongly disagree) to 7 (very strongly agree). One additional item assesses global happiness in the relationship on 10-point scale from 1 (unhappy) to 10 (perfectly happy). The RQI had very high internal consistency (α = .96 in the matched sample).
The DASS-21 (Lovibond and Lovibond, 1995) was used as a measure of psychological distress in parents. It lists 21 symptoms of depression, anxiety, and stress, and asks respondents to rate how much each symptom applied to them over the past week on a four-point scale from 0 (did not apply to me at all) to 3 (applied to me very much). The DASS-21 has adequate internal consistency (α = .88, .78, .86 respectively).
Procedure
Ethical clearance for the study was obtained in accordance with the ethical review processes of the University of Queensland and the National Health and Medical Research Council guidelines. Individual measurement sessions were conducted either in the family’s home, or at one of the venues for the intervention. Families received a questionnaire booklet prior to measurement, and were asked to bring the completed questionnaire booklet to their measurement session. Parents were contacted by phone to complete the BCC.
Data analysis
Differences between the healthy weight and obese groups were assessed using a series of one-way between-groups ANOVA (for constructs assessed by a single measure), and one-way between-groups MANOVA (for constructs assessed by multiple measures if r ≥ .30). A Bonferroni correction was applied to all univariate F tests. Additional chi-square analyses were performed on some measures to determine group differences in the proportion of scores falling within the clinical range and odds ratios. Clinical cutoff scores were compared for the ECBI, SDQ, and PS scales; and meaningful cutoffs were devised for the LBC scales (i.e. healthy weight group mean ± standard deviation), and the BCC (i.e. half the steps followed).
Results
Means, standard deviations, univariate F statistics, and effect sizes for the continuous variables are displayed in Table 2. Proportions and chi-square statistics are displayed in Table 3.
Means, standard deviations, univariate F statistics, and effect sizes for the healthy weight and obese groups.
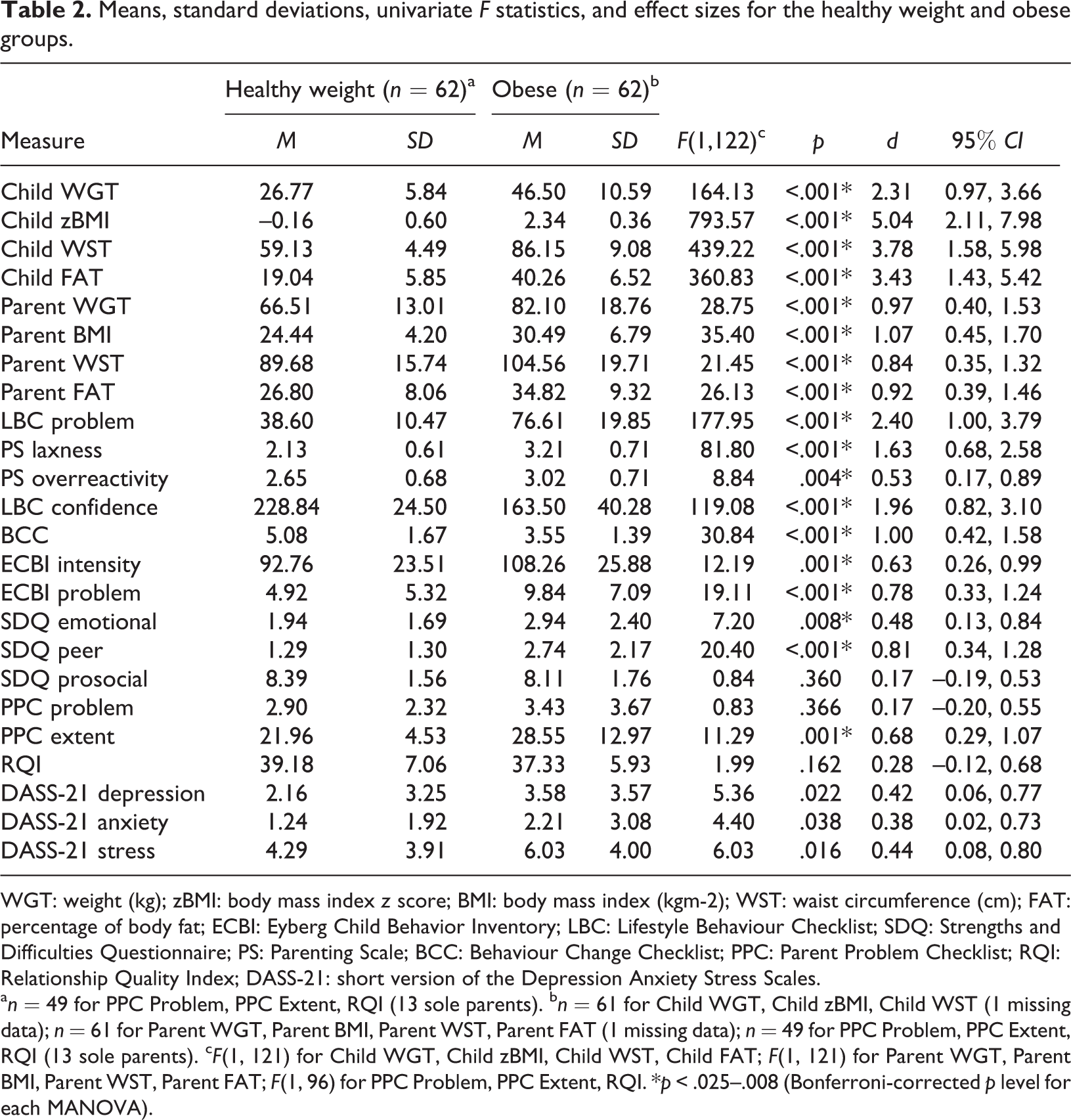
WGT: weight (kg); zBMI: body mass index z score; BMI: body mass index (kgm-2); WST: waist circumference (cm); FAT: percentage of body fat; ECBI: Eyberg Child Behavior Inventory; LBC: Lifestyle Behaviour Checklist; SDQ: Strengths and Difficulties Questionnaire; PS: Parenting Scale; BCC: Behaviour Change Checklist; PPC: Parent Problem Checklist; RQI: Relationship Quality Index; DASS-21: short version of the Depression Anxiety Stress Scales.
a n = 49 for PPC Problem, PPC Extent, RQI (13 sole parents). b n = 61 for Child WGT, Child zBMI, Child WST (1 missing data); n = 61 for Parent WGT, Parent BMI, Parent WST, Parent FAT (1 missing data); n = 49 for PPC Problem, PPC Extent, RQI (13 sole parents). c F(1, 121) for Child WGT, Child zBMI, Child WST, Child FAT; F(1, 121) for Parent WGT, Parent BMI, Parent WST, Parent FAT; F(1, 96) for PPC Problem, PPC Extent, RQI. *p < .025–.008 (Bonferroni-corrected p level for each MANOVA).
Group differences in the proportion of scores falling within the clinical range (n = 124).
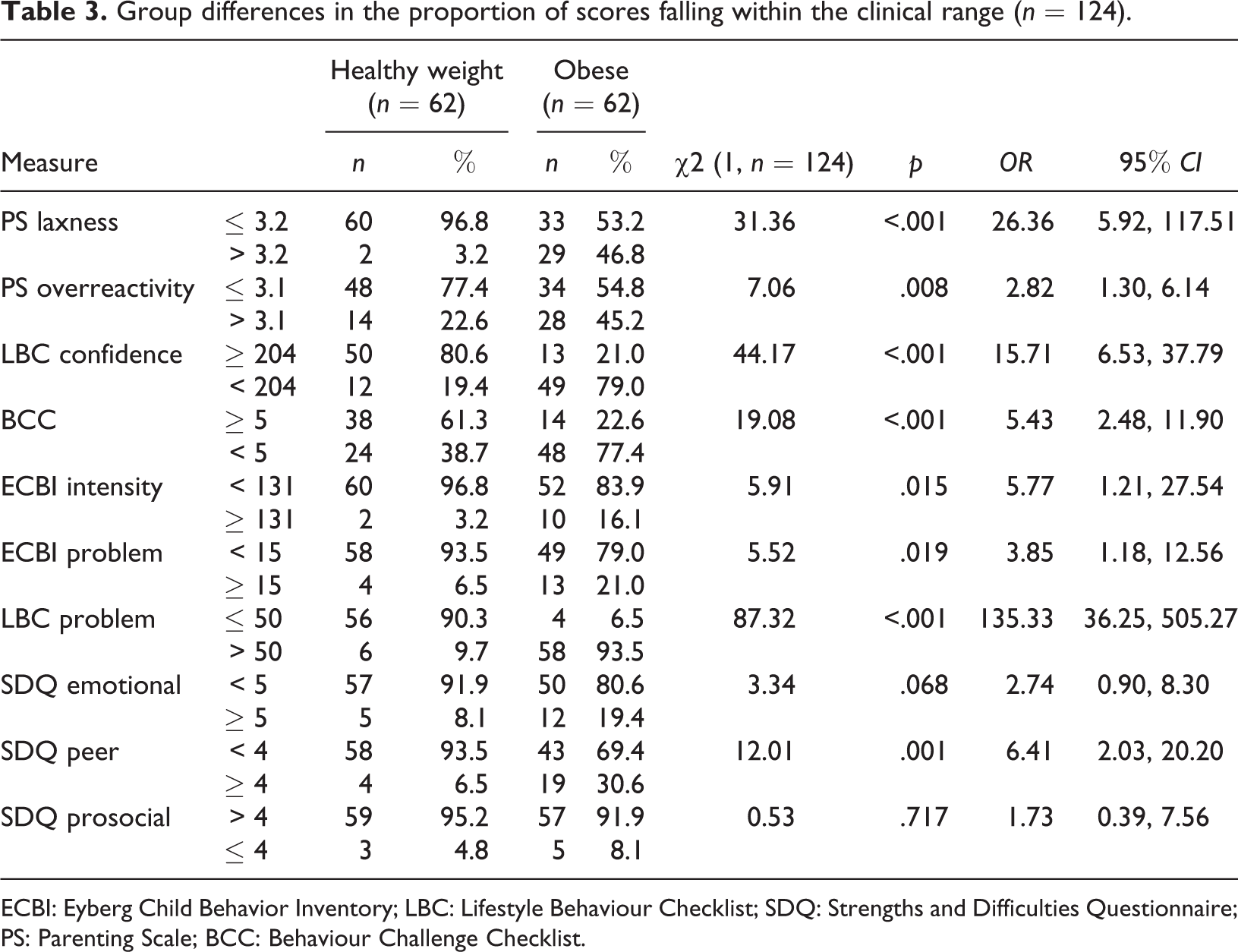
ECBI: Eyberg Child Behavior Inventory; LBC: Lifestyle Behaviour Checklist; SDQ: Strengths and Difficulties Questionnaire; PS: Parenting Scale; BCC: Behaviour Challenge Checklist.
There were significant group effects for both child weight status, F (4, 118) = 261.81, p < .001; and parent weight status, F (4, 118) = 9.27, p < .001. Children and parents in the obese group tended to have larger body sizes (WGT, BMI, zBMI, WST), and a higher percentage of body fat (FAT), than children and parents in the healthy weight group. The BMI of most parents in the healthy weight group fell within the healthy weight range, whereas the BMI of most parents in the obese group fell within the overweight or obese range.
There was a significant group effect for child adjustment, F (6, 117) = 31.18, p < .001. In the obese group, parents reported higher levels of child general behaviour problems, lifestyle behaviour problems, emotional symptoms, and peer problems than parents in the healthy weight group. There was no group difference in the level of prosocial behaviour, and mean scores were in the normal range for both groups on all ECBI and SDQ scales. However, obese children were more likely to have clinically elevated scores on the ECBI Problem, ECBI Intensity, and SDQ Peer problems scales than healthy weight children.
Parenting differed significantly as a function of group, F (4, 119) = 40.10, p < .001. Parents in the obese group had higher mean scores for both the PS Laxness and Overreactivity scales, and were more likely to have clinically elevated scores on these scales. For both groups, the mean score for the Laxness scale fell within the normal range; but for the obese group the mean score for the Overreactivity scale fell within the clinical range. Parents of healthy weight children were more likely to have high scores on the LBC Confidence scale and to follow at least 50% of the steps for promoting healthy lifestyles.
For relationship adjustment, there was a significant group effect, F (3, 94) = 4.87, p = .003. Parents in the obese group reported more intense conflict with their partner over childrearing. However, there were no group differences in the number of interparental disagreements, or relationship satisfaction. Parental distress also did not differ between the healthy weight and obese groups, F (3, 120) = 2.53, p = .060. Mean scores on the DASS-21 were well below the clinical cutoffs.
Effect sizes for group differences in weight status and child and family functioning ranged from negligible (.17) to very large (5.04). As shown in Table 2, the largest effect sizes were associated with the measures of child weight status, and the LBC Problem, LBC Confidence, and PS Laxness scales.
Discussion
The aim of the study was to clarify the relationship between ineffective parenting and childhood obesity. All three hypotheses were supported: parents of obese children used different disciplinary practices to parents of healthy weight children, used fewer health promoting strategies, and lacked confidence in managing children’s lifestyle behaviours. These results are consistent with a growing body of evidence that implicates ineffective parenting in the development and maintenance of childhood obesity.
The results indicate that permissive and coercive parenting practices are more common in families with obese children than families without obese children. Nearly half of the obese group reported clinically elevated scores on the PS, compared to less than a quarter of the healthy weight group. In the obese group, over three quarters of parents followed less than five BCC steps. These findings are consistent with the small body of research showing that authoritarian or coercive parenting styles have been associated with a higher risk of overweight (e.g. Berge et al., 2010; Moens et al., 2007), providing more evidence that general parenting style may be a potential target for intervention in preventing and treating childhood obesity. Previous research suggests that child lifestyle patterns (e.g. child energy intake, physical activity, sedentary behaviour) may be less important in predicting child weight status than other variables (e.g. Magarey et al., 2001). These findings highlight the importance of understanding how parenting and child and family functioning impact upon the development and maintenance of childhood obesity, and provide a cogent rationale for addressing parenting in the management of this pervasive problem.
To begin to understand why parents of obese children might know less about managing children’s lifestyle behaviour than parents of healthy weight children, and why they might be using ineffective parenting strategies, several measures were administered in addition to the two parenting questionnaires. The differences observed in child and parent weight status were expected, given that child BMI was the basis of classification into healthy weight and obese groups, and given the well documented link between parent and child obesity (e.g. Whitaker et al., 1997). Because parents of obese children tend to have their own weight problems, they may model ineffective lifestyle patterns and behaviours, and their knowledge of effective strategies for preventing excess weight gain, their success in implementing lifestyle changes, and their confidence in managing children’s lifestyle behaviour is likely to be limited. Parents of obese children were more likely to have low scores on the LBC Confidence scale than parents of healthy weight children; and only 21% were confident in managing their children’s eating, activity, and weight-related behaviours versus 81% of parents of healthy weight children. Low self-efficacy in obese parents may contribute to their use of ineffective parenting strategies (Jones and Prinz, 2005).
The results suggest that a higher proportion of obese children have challenging behaviours, social problems, and emotional symptoms than healthy weight children; but for most obese children, these problems are sub-clinical. In this sample, compared to lifestyle-specific behaviour problems, general behaviour problems and emotional and social difficulties were relatively minor, consistent with previous literature (e.g. Wardle and Cooke, 2005). Given the pervasiveness of challenging behaviours relating to eating, physical activity, sedentary behaviour, and overweight in obese children, it is not surprising that parents lack confidence. Repeated failed attempts to manage children’s lifestyle behaviour are likely to erode parents’ self-efficacy, thereby exacerbating ineffective parenting. Similarly, only limited support was found for an association between childhood obesity and parental adjustment.
The strengths of this study include the assessment of multiple aspects of child and family functioning, thorough evaluation of the importance of group differences, use of measures with established validity and reliability, and a representative and well-matched sample. However, three limitations should be noted. Firstly, attempts were made to attain a large enough sample size to ensure adequate power (i.e. for a medium effect size, power > .80 if n = 64 per group), but only 62 matched pairs were available for analysis. On measures where no significant differences were detected, true group differences are likely to have been masked by high individual variability, and effect sizes were probably underestimated. Therefore, it is critical that future studies exploring family factors and childhood obesity employ sample sizes that allow detection of small (but potentially important) group differences. A second limitation of the study is the cross-sectional design. The results provide convincing evidence that ineffective parenting is related to childhood obesity. However, the direction of this relationship cannot be evaluated with a single point of measurement. Clearly, more prospective research is required to identify whether ineffective parenting is both an antecedent and consequence of childhood obesity, and what other factors might be at play. A third limitation of the study is the method of recruitment. Families in the obese group participated because parents were concerned about their child’s weight and agreed to take part in an intervention to assist with this. Families in the healthy weight group participated because parents believed their child was healthy. It is possible that parents seeking treatment for childhood obesity have lower self-efficacy and use more ineffective parenting strategies than parents not seeking treatment. Parents who believe their child is healthy, or are not concerned about their child’s weight, are more likely to have high levels of self-efficacy. This means that the differences in parenting style and confidence observed in this study between the healthy weight and obese groups may exaggerate true differences. Therefore, the results may not generalise to all families with an obese child, and all families with a healthy weight child.
In conclusion, parents exert a powerful influence over children’s development of healthy lifestyle patterns, and can therefore impact a child’s risk of becoming obese. Childhood obesity is a pervasive problem, with a complex and multifactorial aetiology. Parenting and other family factors may help to explain how obesity develops and is maintained in certain families. There is an urgent need for prospective studies to clarify whether parenting styles are causally related to childhood obesity and to explore the causal pathways between child lifestyle behaviour problems, self-efficacy, and ineffective parenting. The results of these studies would have implications for future management of childhood obesity. Targeting parents’ use of ineffective parenting practices and low self-efficacy may lead to more effective preventive and treatment approaches than are presently available, and have a direct impact on obesity prevalence.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.