
Abstract
This exploratory study examined the role of satisfaction with support from family and friends on the burden and stress of parents of infants with a congenital anomaly (CA). The effects of social support were examined within the couple (actor and partner effects). A total of 36 couples whose six-month-old infant has a CA participated in this study. The parents completed questionnaires regarding satisfaction with support, burden (Impact on Family Scale – Revised), and parenting stress (Parenting Stress Index). The results showed that fathers directly benefited from the support they received from friends in reducing their burden, while mothers only indirectly benefited from it through the father’s adjustment. The pattern was different for stress: mothers directly benefited from the support they received from their family in reducing their stress levels, while fathers benefited both directly from the support they received from friends and indirectly from the support that their partners received from family. These results highlight that (1) the different support needs of mothers and fathers (due to their different roles during transition to parenthood) and (2) the diffusion of benefits of social support within the couple should be taken into account when developing strategies to promote support to families of six-month-old infants with a CA.
Keywords
Introduction
The first months of parenthood may be particularly demanding for parents who raise an infant with a congenital anomaly (CA). CAs are structural or functional anomalies present at birth that arise during intrauterine development (e.g. congenital heart disease and cleft lip and palate) (Crowley, 2010). In 2010, the estimated prevalence of live births with CA in European countries was 179.81 per 10,000 births (European Surveillance of Congenital Anomalies (EUROCAT), 2012). In addition to the usual caretaking tasks, parents must adapt to the challenges associated with the CA such as surgeries and hospitalizations, increased medical monitoring, and uncertainty about the future quality of life (Mazer et al., 2008). The infant’s CA may have familial/social and professional/financial costs for parents, which may be reflected in the parents’ perceived burden (Hunfeld et al., 1999) and parenting stress (Uzark and Jones, 2003). Given these increased demands, it is important to understand which resources – namely social support – should be fostered to help parents of infants with a CA to adapt to the condition.
Benefits of social support for parents during transition to parenthood
Social support is a type of interpersonal transaction that includes appraisal, emotional concern, information, or instrumental aid (House, 1981). Therefore, social support is a resource to meet the individual’s specific needs in a given period of life (Tak and McCubbin, 2002) and to deal with stressful situations. Social support has been considered an important resource during transition to parenthood among parents of healthy infants (Bost et al., 2002). During this period, the parents’ main needs of support are related to the responsibilities and everyday tasks of parenthood (Bost et al., 2002). Therefore, parents become closer to their nuclear family and more distant from their friends as a way of surrounding themselves with sources of support that appropriately meet their parental needs (social nesting) (Gameiro et al., 2010).
Although the benefits of social support also occur in parents of children who possess a CA (Murray et al., 2007), some specificities make it important to further examine the nature of these effects: (1) this is a period of intense learning related to the diagnosis specificities (Griffin, 2002), so these parents’ support needs may be different (e.g. needs for information) (Sargent, 2009); and (2) parents may have some communication difficulties within their social network concerning the diagnosis, such as sharing the news of the diagnosis (Howard, 2006) or dealing with the reactions from their social network about the infant’s diagnosis (Messias et al., 1995).
Research on the role of social support in the adjustment of parents of children with a CA has focused on parents of older children and shows a positive impact of overall satisfaction with received support on the perceived burden of parents of children (mean age: 8 years) with developmental disabilities (Jones and Passey, 2004) and of parents of children (mean age: 12 years) with intellectual disabilities (Mak and Ho, 2007). Moreover, increased satisfaction with support was associated with reduced levels of parenting stress in parents of infants with cerebral palsy (Britner et al., 2003) and in parents of children (ages between 4 and 18 years) with spina bifida (Macias et al., 2007). Guralnick et al. (2008) found that specific support related to help with childcare or advice about the child’s problems, but not general emotional or instrumental support, significantly contributed to the reduction in maternal stress levels when parenting a child with a disability. Consistently, parents of infants with a CA acknowledged their family (including the partner, their own, and their partner’s nuclear family) as their greatest source of support (Findler, 2000; Hornby and Ashworth, 1994; Jones and Passey, 2004; Tunali and Power, 2002), with the support received from friends being perceived as less helpful (Hall and Graff, 2011). However, it is important to examine the effects of satisfaction with support from different sources on the adjustment of parents of younger children with a CA.
During the transition to parenthood, mothers assume the role of main caregivers of the infant, while fathers are the family’s providers (Katz-Wise et al., 2010), so their support needs may be different. Also, studies have shown that social support seems to be more relevant to mothers’ adjustment than to fathers’ adjustment (Levy-Shiff, 1999). Social support was found to be beneficial for both mothers and fathers of infants with a CA (Macias et al., 2007), while others found benefits only for mothers (e.g. Krauss, 1993), suggesting a distinct effect of social support for both genders. This should be further explored.
The Actor–Partner Interdependence Model: The benefits of social support within the couple
The Actor–Partner Interdependence Model (APIM) (Cook and Kenny, 2005) is a model of interdependence in dyadic relationships, that is, when one person’s emotion, cognition, or behavior affects the emotion, cognition, or behavior of a partner. Interdependence within the family system has been documented in other contexts, suggesting that the characteristics of one member of the couple influence the characteristics and outcomes of the other member (Barr, 2012; Dorros et al., 2010). As parenting is usually experienced jointly by the couple, this influence may become even more evident (Biehle and Mickelson, 2011). To our knowledge, the partner effects of support in parental adjustment, that is, the effects of one partner’s perceived support on the other partner’s adjustment have not been investigated in the context of raising an infant with a CA. Furthermore, the APIM also suggests that the adjustment of both partners seems to be mutually influenced within the couple (Cook and Kenny, 2005). In fact, Gray (2003) found that fathers sometimes regarded the negative impact of dealing with their child’s disability as an indirect impact that originated from their partner’s distress and suffering. Therefore, it is reasonable to hypothesize that the effect of one parent’s perceived social support influences his or her partner’s adjustment, via an indirect mechanism through that parent’s adjustment (i.e. the individual’s perceived satisfaction with support influence his/her own adjustment which, in turn, influences his/her partner’s adjustment).
Research aims and hypotheses
In accordance with the APIM (Cook and Kenny, 2005), we aimed to investigate the individual (actor) and partner effects of satisfaction with social support received from family and friends in parental adjustment (burden and parenting stress). We also aimed to explore whether the partner effects (the effects of maternal/paternal satisfaction with support on her or his partner’s adjustment) occur indirectly, through maternal/paternal adjustment (Figure 1).
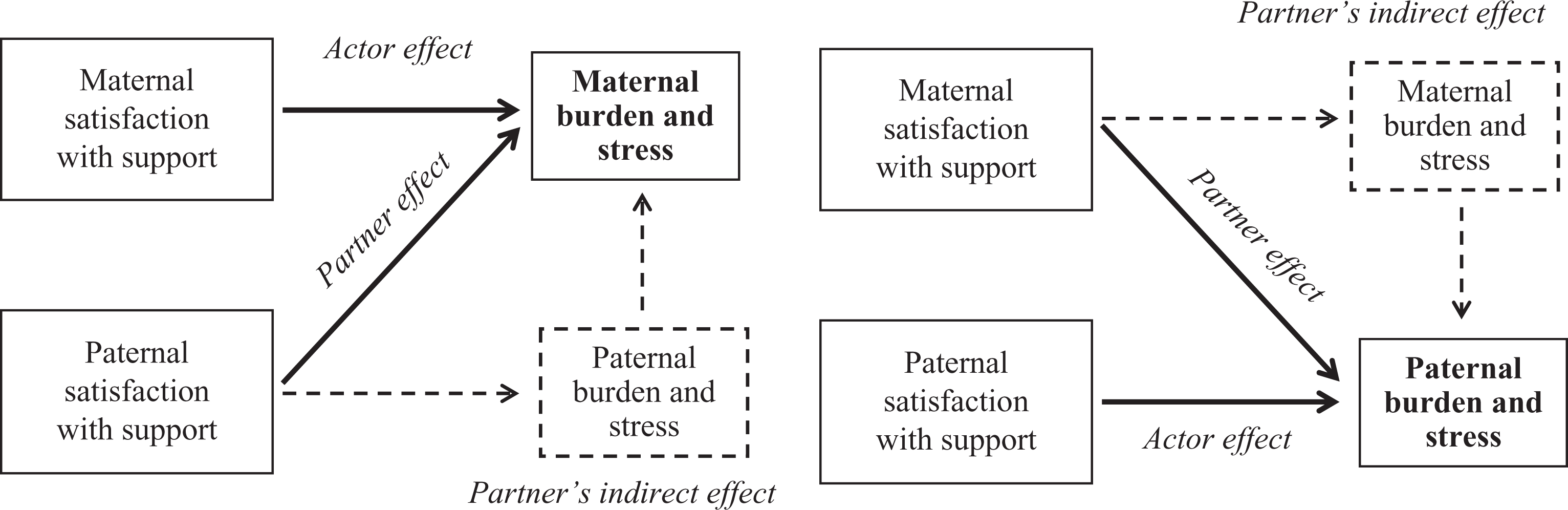
Actor–partner interdependence model: Actor and partner effects of satisfaction with support in parental adjustment.
We established the following hypotheses: (1) increased satisfaction with support from family and friends will predict better individual adjustment; (2) increased satisfaction with support will be positively associated with the partner’s adjustment; and (3) the effect of mother’s/father’s satisfaction with support on her or his partner’s adjustment will be indirect through their own (mother’s/father’s) adjustment.
Methods
Participants and procedure
This study is part of a longitudinal study entitled ‘Reproductive decisions and transition to parenthood after a pre- or postnatal diagnosis of a CA,’ which was approved by the Ethics Committees of the Hospitais da Universidade de Coimbra (HUC) and the Centro Hospitalar de Coimbra (CHC), Portugal. Inclusion criteria of an individual for the present study were (1) having an infant who was pre- or postnatally diagnosed with a CA, without the occurrence of perinatal death, (2) being at least 18 years of age, and (3) having a level of literacy (educational level ≥ sixth grade) that allowed for comprehension of the assessment protocol.
The data collection took place between September 2009 and February 2012, in the Obstetrics and Neonatology Departments of HUC and in the Pediatric Cardiology Service of the Pediatric Hospital at CHC. Approximately one month after the disclosure of a diagnosis of a CA, all parents were informed about this study by their medical team at the end of a medical appointment and contacted by the researchers. Those who decided to participate signed an informed consent form and responded to the assessment protocol (time 1). A total of 82 couples were contacted, of whom 22 refused to participate/did not return the questionnaires (participation rate: 73.17%). Parents were contacted again six months after the infant’s birth (time 2). The questionnaires were mailed to the participants along with a prestamped envelope in which to return them after completion; 17 couples did not return the questionnaires (attrition rate: 28.33%) and seven questionnaires were excluded because they had been completed only by the mother. No significant differences in sociodemographical or clinical characteristics were found between parents who returned or did not return the questionnaires at time 2 (data not shown). For the purpose of this study, only the couples who participated at time 2 were considered.
The final sample comprised 36 couples. The sample characteristics are presented in Table 1. Mothers were younger and studied for longer than fathers. The majority of parents learned about their infant’s CA during the prenatal period.
Sample of sociodemographic and clinical characteristics.
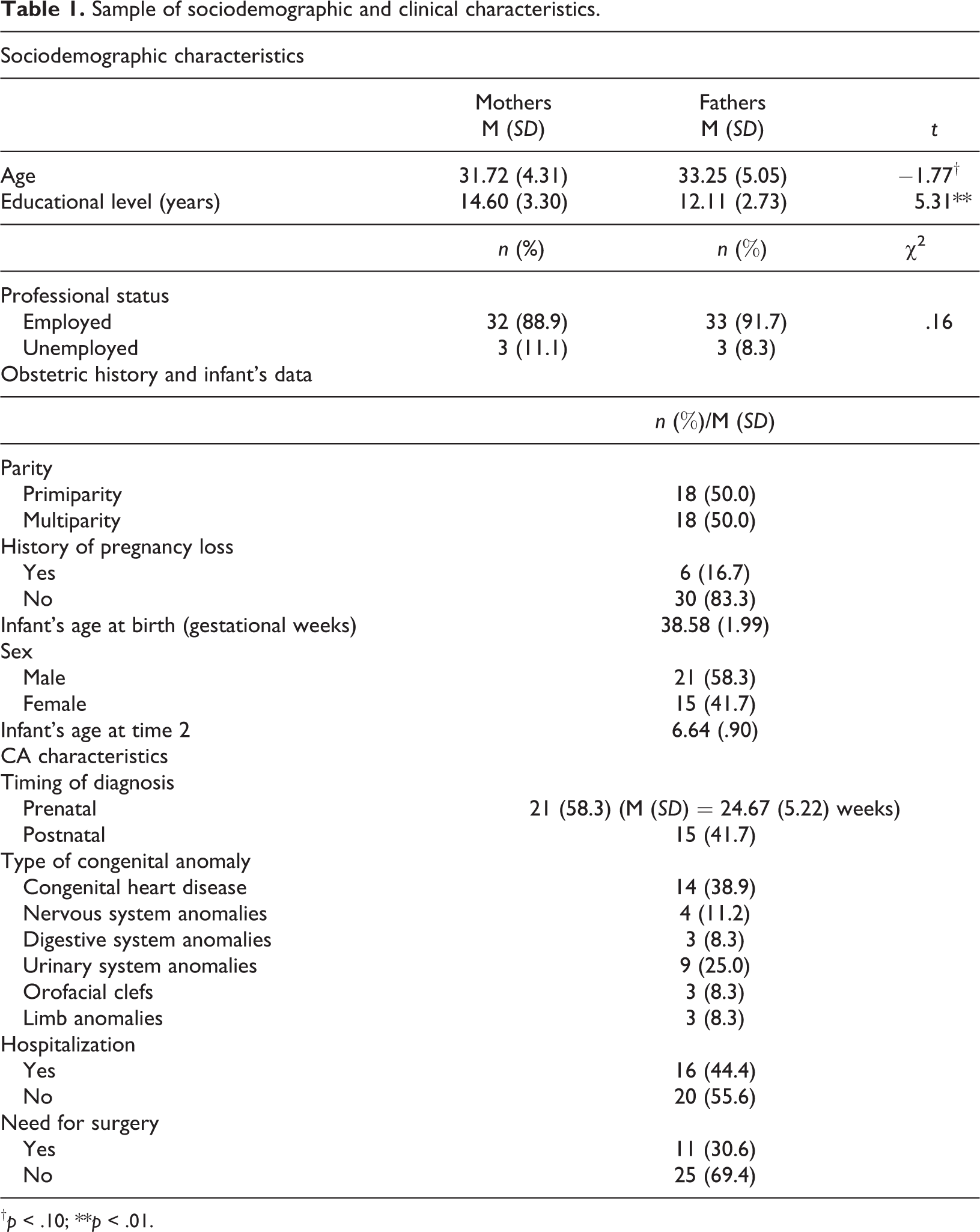
† p < .10; **p < .01.
Measures
Sociodemographic and clinical data
Sociodemographic (e.g. gender, age, educational level, and professional status) and clinical information (e.g. parity; the infant’s data: gender, gestational age at birth, type of CA, timing of diagnosis, and need for surgery) were obtained using a questionnaire.
Satisfaction with support received
The satisfaction with support received from family and friends was assessed by the question: ‘To what extent do you feel satisfied with the support received from the following persons, since your baby’s birth?’ For each source of support (partner, nuclear family, partner’s nuclear family, and friends), the parents classified their amount of satisfaction using visual analog scales (from 0 = Not satisfied to 100 = Extremely satisfied). Individual scores of satisfaction with their partner, their own family, and their partner’s family were averaged to compute an index of satisfaction with support received from their nuclear family.
Perceived burden
Burden was assessed using the Portuguese version of the Impact on Family Scale – Revised (Albuquerque et al., 2011). This unidimensional scale consists of 15 items (e.g. ‘Fatigue is a problem for me because of my child’s illness’), answered in a 4-point scale (from 1 = Strongly disagree to 4 = Strongly agree). Higher scores indicate a greater perceived burden associated with caring an infant with a CA. The Cronbach’s α value in our sample was .93 for mothers and .94 for fathers.
Parenting stress
The Portuguese version of the Parenting Stress Index – Short Form (Santos, 2011) was used to evaluate stress within the parent–child system. The scale comprises 36 items (e.g. ‘I often have the feeling that I cannot handle things very well’) answered on a 5-point scale (from 1 = Completely disagree to 5 = Completely agree) and is organized along three dimensions: parental distress, parent–child dysfunctional interaction, and difficult child. It is also possible to compute a total score of parenting stress, which was used in the present study. Higher scores indicate greater stress. The Cronbach’s α value in our sample was .93 for fathers and .95 for mothers.
Data analyses
Analyses were conducted using IBM SPSS, version 19.0. Data analyses were performed on the couple as a unit. The database was restructured to consider each couple as the subject of the analysis and each partner’s score as a different variable. Descriptive statistics and comparison tests (paired t tests and χ 2 tests) were used for sociodemographic characterization of the sample. Bivariate Pearson’s correlations were computed among the study variables.
Multiple regression analyses were conducted to investigate the effects of social support (satisfaction with support from family and satisfaction with support from friends) on parental adjustment (dependent variables: burden and parenting stress). In accordance with the APIM (Cook and Kenny, 2005), in one set of analyses the maternal outcome variables were regressed on the maternal (actor) and paternal (partner) predictor variables, and in the other set of analyses the paternal outcome variables were regressed on the paternal (actor) and maternal (partner) predictor variables. The sociodemographic and clinical variables were introduced in the first step of the models for control purposes if they were significantly associated with parental adjustment.
When a partner effect on the actor’s adjustment was found, we examined whether this was an indirect effect through the partner’s adjustment. Indirect effects were examined using a procedure that relies on nonparametric bootstrapping, which is indicated for small samples and does not require the assumption of normality of the sampling distribution. The SPSS version of Preacher and Hayes’ macro ‘indirect’ was used (Preacher and Hayes, 2004, 2008). The presence of an indirect effect was assessed with bootstrapping (with N = 5000 resamples). Point estimates and 95% confidence intervals (CI; bias corrected and accelerated CI) were estimated for the indirect effects. An indirect effect was considered significant if zero was not included in the 95% CI.
Post hoc power calculations made for all statistical analyses performed with a significance level of .10 and power ≥ .80 indicated that medium to large effects (f 2 ≥ .30) could be detected (Faul et al., 2007). As a result, significance was defined as p < .05, but marginally significant results (p ≤ .10) were also reported.
Results
Table 2 presents descriptive statistics and the bivariate associations between sociodemographic and clinical variables, social support, and parental adjustment.
Pearson’s correlations between sociodemographical and clinical variables, satisfaction with support, and parental adjustment.
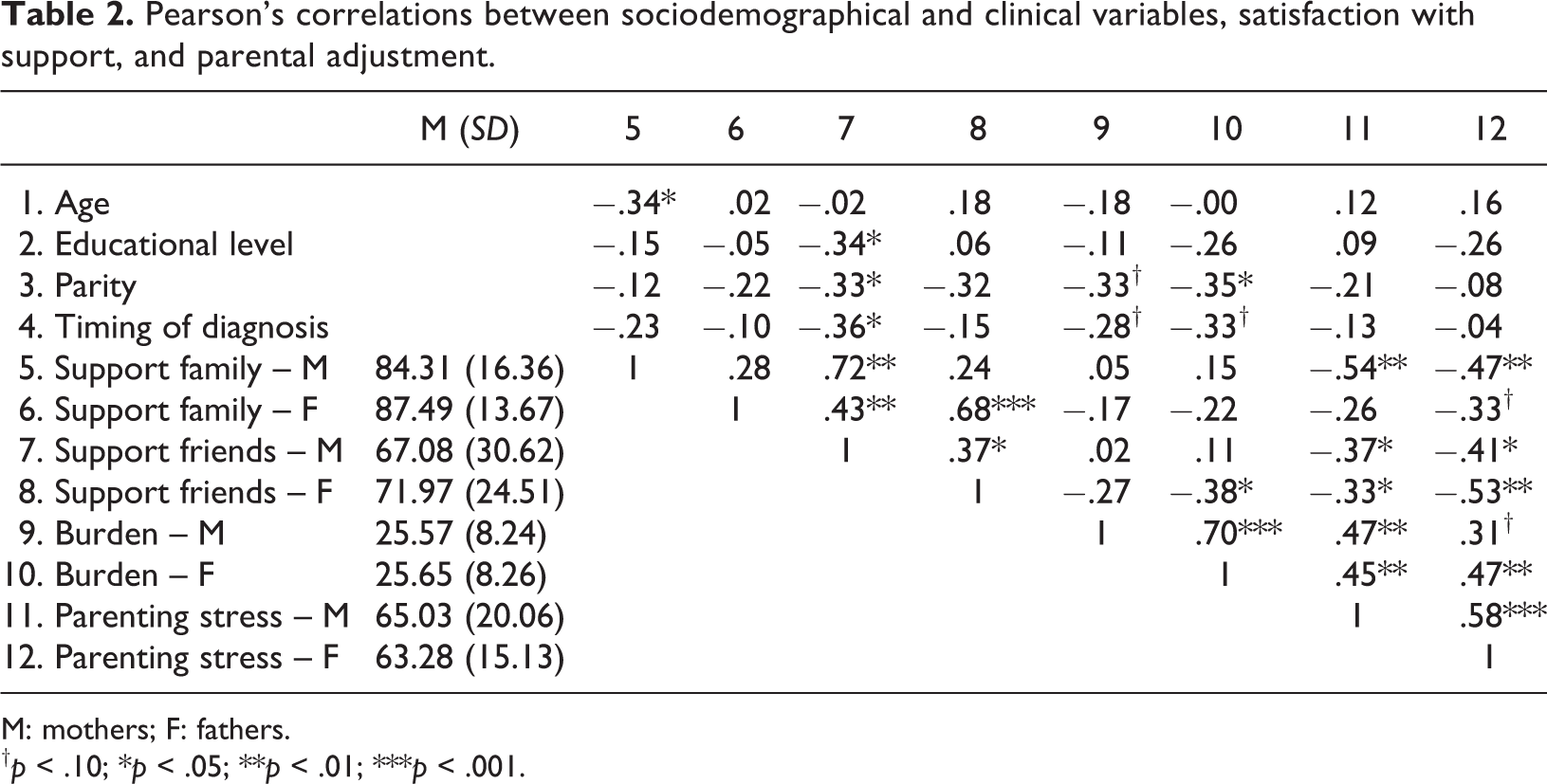
M: mothers; F: fathers.
† p < .10; *p < .05; **p < .01; ***p < .001.
As shown in Table 2, maternal satisfaction with support from family and friends was significantly and negatively correlated with maternal and paternal parenting stress, but not with burden. Paternal satisfaction with support from family was only marginally significantly correlated with paternal levels of stress, while paternal satisfaction with support from friends was significantly correlated with paternal burden and with maternal and paternal stress. Moreover, maternal and paternal satisfaction with support from family was not significantly correlated, while maternal and paternal satisfaction with support from friends showed moderate correlations. Finally, both maternal and paternal adjustment indicators were significantly and positively correlated.
Actor and partner effects of social support on parental adjustment
Table 3 presents the regression models assessing the actor and partner effects of satisfaction with social support in the maternal and paternal adjustment (burden and parenting stress).
Effects of satisfaction with support from family and friends on maternal and paternal adjustment: actor and partner effects.
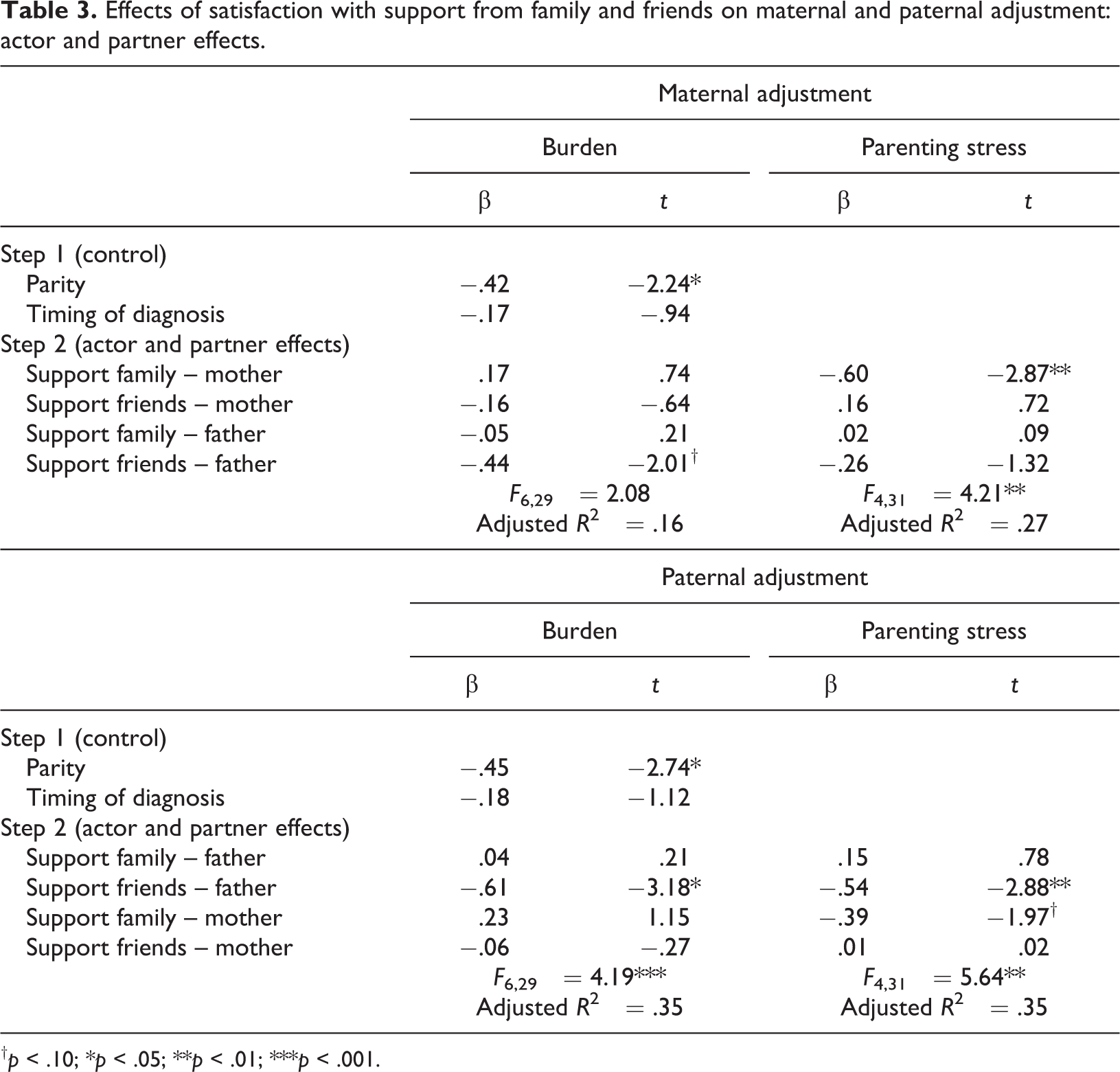
† p < .10; *p < .05; **p < .01; ***p < .001.
Burden
The model predicting maternal burden was marginally significant. As shown in Table 3, the maternal perceived burden was lower when mothers had no other children and when their partners were more satisfied with the support they received from friends (partner effect). Similarly, the model predicting paternal burden was significant. Fathers perceived lower burden when they had no other children and when they were more satisfied with the support they received from friends (actor effect).
Parenting stress
The models predicting maternal and paternal parenting stress were both significant. As shown in Table 3, an actor effect of satisfaction with support from family was found for maternal stress: higher maternal satisfaction with support received from their family predicted lower levels of maternal stress. When considering paternal levels of stress, an actor and a partner effect were found: fathers presented lower levels of parenting stress when they were more satisfied with the support received from their friends (actor effect) and when their partners were more satisfied with the support received from the family (partner effect).
Partner effects: Indirect effects through the partner’s adjustment
Table 4 presents the indirect effects of the partner’s satisfaction with support on the actor’s adjustment through the partner’s adjustment.
Partner effects of satisfaction with support on adjustment: Examining indirect effects.
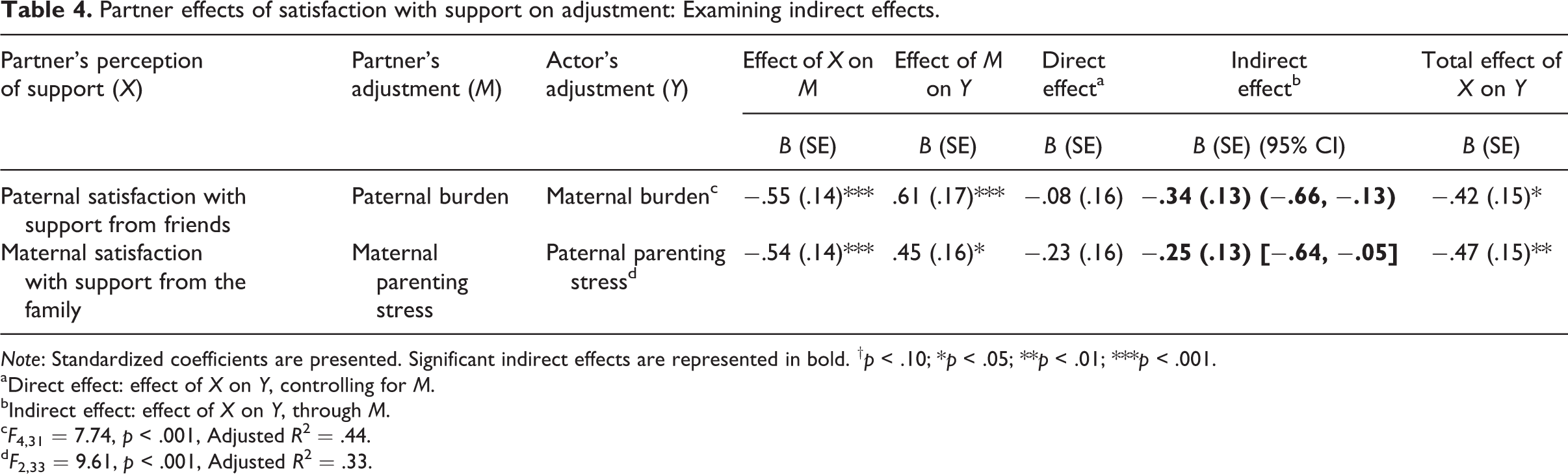
Note: Standardized coefficients are presented. Significant indirect effects are represented in bold. † p < .10; *p < .05; **p < .01; ***p < .001.
aDirect effect: effect of X on Y, controlling for M.
bIndirect effect: effect of X on Y, through M.
c F 4,31 = 7.74, p < .001, Adjusted R 2 = .44.
d F 2,33 = 9.61, p < .001, Adjusted R 2 = .33.
As shown in Table 4, an indirect effect in the relationship between the paternal satisfaction with the support received from their friends and maternal burden was found through paternal burden. When fathers were more satisfied with the support they received from their friends, they perceived lower burden which, in turn, was reflected in lower maternal burden. Moreover, a significant indirect effect was found in the relationship between maternal satisfaction with the support received from the family and paternal parenting stress. When mothers were more satisfied with the support received from their family, they presented lower levels of maternal stress which, in turn, contributed to decreased paternal levels of stress.
Discussion
The main finding of this exploratory study was that both parents of six-month-old infants with a CA benefited from social support. However, the benefits of social support were different when considering mothers or fathers, perceived burden or parenting stress, and family or friends as sources of support. Moreover, social support had a positive impact not only on the individual’s adjustment, but also on the partner’s adjustment, which suggests a diffusion of its benefits.
As shown by our results, mothers benefited directly from the support offered by their family, which reduced their parenting stress levels, partially confirming our first hypothesis. The mothers’ partners and nuclear family (their own and their partner’s) are usually the main providers of instrumental and emotional assistance with usual childcare tasks (Bost et al., 2002), reducing maternal stress associated with the parenting role. Consistent with the study by Guralnick et al. (2008), the most useful dimension of support for mothers of infants with a CA seems to be the support related with help in childcare or advice about the child’s problems. Conversely, and contrary to our expectations, maternal satisfaction with support received was not associated with a decrease in maternal burden. Mothers only benefited indirectly from the support received from their partner’s friends, through father’s perceived burden, supporting the APIM model. It is possible that help with childcare may be useful in terms of emotional consequences (maternal stress), but not in terms of the objective impact of the CA, such as familial routines, financial issues, and interaction with medical services. Therefore, the maternal perceived burden of caring for an infant with a CA may be more effectively reduced with the support from other sources, such as health professionals or social services. This hypothesis should be further explored.
The support received from friends was not beneficial for maternal adjustment. Similarly to mothers of healthy infants (Gameiro et al., 2010), mothers of infants with a CA may distance themselves from their social network (e.g. friends) during the first months of parenthood. This withdrawal may be due to the time spent in providing care to the infant (Lawoko and Soares, 2003) or with some difficulties in communicating about diagnosis-related issues (Messias et al., 1995). The lack of contact with friends may lead to lower maternal satisfaction with the support received from them and also to its lower impact on maternal adjustment.
A different pattern of results was found for fathers. In fact, fathers benefited directly from the support they received from friends in reducing their perceived burden and parenting stress. Three reasons may explain our results. First, despite participating in some caregiving tasks, fathers usually assume the role of economic providers for the family (Katz-Wise et al., 2010). Thus, as opposed to the mothers’ needs, fathers’ support needs may be more related to assistance with financial or legal issues, or increased flexibility with work issues, so their friends can be a useful source of help. Second, fathers may have more opportunities than mothers for interaction within their social network (friends), given their earlier return to work and to daily routines (Feldman et al., 2004). As suggested by Olsson and Hwang (2006), the greater paternal involvement in the professional responsibilities seems to be associated with better well-being for fathers compared with their partners. It is possible that, due to this involvement, fathers receive and benefit more from their friends’ support. Third, research shows that fathers try to assume the protective role of their partners (Locock and Alexander, 2006), trying not to show their own suffering, as we explain below. Therefore, fathers may rely more on friends than on their family for emotional support to deal with the emotional constraints associated with the parenting experience.
In fact, paternal satisfaction with support received from their family was not reflected in better paternal adjustment. Fathers may be concerned with their partners’ suffering after the infant’s diagnosis of a CA, seeking to direct their efforts to support and to protect them (Locock and Alexander, 2006). Therefore, fathers may neglect their own sufferings and may avoid adequately communicating their support needs to their partner or family or even engage in help-seeking behaviors. Even when fathers receive support from their partner and family, they may be worried about their inability to fulfill their role as protectors. These factors may help to explain why support from family did not prove to be beneficial for paternal adjustment. However, fathers showed benefits in parenting stress when mothers were more satisfied with the support they received from the family, as suggested by the APIM model. This benefit was indirect through the mother’s adjustment. As primary caregivers, mothers may experience more emotional constraints associated with the parenting role (i.e. parenting stress) than fathers. As maternal suffering associated with the impact of the child’s diagnosis is sometimes reflected in fathers’ adjustment (Gray, 2003), the factors that contribute to improve the maternal adjustment – in this case, social support – were also reflected in a better paternal adjustment. In fact, when mothers are more satisfied with the support received from their family, they may perceive fewer restrictions associated with the demands of the parenting role, which reflects in reduced levels of maternal stress. Moreover, these reduced levels of maternal stress were likely reflected in better interactions within the couple (e.g. less conflict and improved communication), which consequently improved paternal adjustment. In sum, our results confirmed the diffusion of benefits of social support within the couple, supporting the interdependence in the dyadic relationships (Cook and Kenny, 2005).
Although the present study represents an important contribution to the field, it has several limitations. The first limitation is the study’s reduced power to detect small effects due to the sample size. Second, the assessment of social support (overall satisfaction with support from different sources were assessed using single items) did not allow for differentiation between different types of support (e.g. emotional and instrumental) provided by each source, which can be examined in future studies. The final limitation is the non-categorical approach to CA (i.e. the inclusion of different types of CAs). Although our goal was to examine the common experience of these parents, future studies may investigate whether these patterns are similar for parents of infants with different types of CA.
The findings of the present study lead to some clinical implications. First, social support is a beneficial resource for adjustment among parents of infants with a CA during the first months of an infant’s life, and this support should be a target of evaluation and should be promoted. However, it should be noted that mothers’ and fathers’ support needs are different and that the effects of support are different for different adjustment indicators. Second, it should be noted that the demands of childcare prevent mothers from activating some sources of their social network (e.g. friends). In addition to the assessment of maternal satisfaction with the support received, it would be important to consider other issues, such as opportunities for interaction and for requesting help from friends who usually provide support. Third, given the diffusion of benefits of social support within the couple, both partners should be included in the assessment and intervention processes, and the mutual influences within the couple as well as the different mechanisms by which they may occur should be taken into account.
Finally, parents who report lower satisfaction with the support received from their network may be at higher risk of poor adjustment and should be targeted for specialized counseling, to help them develop strategies for (1) identifying their support needs and sources in their social network who may provide that support, (2) communicating their support needs with their social network and activating help-seeking behaviors, and (3) communicating with different sources of support about satisfactory and unsatisfactory aspects of the support received to improve satisfaction with subsequent support.
Footnotes
Acknowledgments
The authors wish to thank the services that enabled the sample collection: Pediatric Cardiology Service of the Pediatric Hospital – Centro Hospitalar de Coimbra (parents of babies with congenital heart disease) and the Obstetrics and Neonatology Departments – Hospitais da Universidade de Coimbra (the remaining participants from the clinical group).
Funding
This study is part of the ‘Reproductive decisions and transition to parenthood after a pre- or postnatal diagnosis of congenital anomaly’ research project, integrated in the Relationships, Development and Health Research Group of the Research and Development Unit, Institute of Cognitive Psychology, Vocational and Social Development, University of Coimbra, Portugal (PEst-OE/PSI/UI0192/2011). AF. and BN. are supported by PhD Scholarships from the Portuguese Foundation for Science and Technology (SFRH/BD/47053/2008, SFRH/BD/43204/2008, respectively).