
Abstract
This study compared parental cognitions and relationship characteristics of mothers of children with atopic disease with those of mothers of children without atopic disease. These factors include child-rearing attitudes, parental locus of control, parental sense of competence, attachment security, and maternal sensitivity. Preplanned subanalyses were carried out according to specific disease, mothers’ perception of disease severity, and presence of concurrent atopic diseases. The descriptive comparative study of 233 Korean mothers included 102 mothers of children aged six years or younger with atopic dermatitis, asthma, and/or allergic rhinitis. Data were collected from 2007 to 2008 from local clinics and day care centers. Parental cognitions and relationship characteristics did not differ significantly between groups of mothers, except that mothers of children with atopic dermatitis showed less affection. However, subanalyses showed that mothers who perceived their child’s disease to be severe were less likely to encourage autonomy and had a lower sense of competence, more rejecting attitudes, and an external locus of control. Although we should be cautious in generalizing these results, special care plans are strongly recommended for mothers of children with severe atopic disease to provide support and education, help mothers develop an internal locus of control, and increase parental sense of competence.
Keywords
Introduction
Atopic diseases are the most common chronic disorders in childhood and their prevalence is increasing (Jee et al., 2009; Mortz et al., 2001). Hypersensitivity reactions initiated by immunologic mechanisms underlie allergies, and childhood allergic disorders include allergic asthma, allergic rhinitis, and atopic dermatitis (Alford et al., 2004; Wu et al., 2011). These disorders generally begin in infancy or early childhood and are characterized by a chronic course with frequent relapses, placing an extra burden of care on parents. Atopic disease affects young children during a critical period of physical and psychosocial development. Both disease progression and the child’s physical condition can be influenced by socioemotional states and vice versa (Gil and Sampson, 1989; Hashiro and Okumura, 1997; Lehrer et al., 2002). Therefore, an understanding of parenting characteristics is critical because the quality of parenting is a major factor in the socioemotional milieu for young children.
Numerous studies described the psychosocial difficulties of children with chronic atopic disease (e.g. anxiety, depression, and social withdrawal) and their negative effects on the management and progression of the disease itself (Daud et al., 1993; Dennis et al., 2006; Wright et al., 1998; Wu et al., 2011). In addition, the atopic disease can cause high levels of parenting stress, ineffective family functioning, and poor psychosocial well-being and quality of life for the parents (Chamlin et al., 2004; Emin et al., 2009; Halterman et al., 2004; Hullmann et al., 2010; Warschburger et al., 2004). The tension created by increased parental stress and physical and psychosocial burden has been linked to less secure attachment between mother and child (Cassibba et al., 2004; Kim et al., 2008).
In light of the negative effect of chronic atopic disease on parents’ cognition about their children and the dyadic relationship, a better understanding of parenting and relationship characteristics is needed to develop optimal care plans to ensure the physical and psychosocial development of chronically ill children.
Parental locus of control, self-efficacy, and rearing attitudes can predict the quality of parenting and the family’s ability to overcome challenges such as a child’s chronic illness (Campis et al., 1986; Coleman and Karraker, 1997; Hassall et al., 2005; Kendall and Bloomfield, 2005; Zimmerman et al., 1999). Parental locus of control is used to assess parents’ perceived control in the parent–child interaction (Campis et al., 1986). Parents with a more external locus of control think they have little effect on the child’s behavior and believe that the child controls important aspects of their daily life. These parents tend to have more authoritarian or coercive parenting styles. Parental sense of competence (or parental self-esteem) represents the degree to which parents view themselves as effective in their parenting role (Johnston and Mash, 1989), and the low sense of parental competence is closely related to less optimal parenting behavior in families of children with chronic medical conditions (Reichenberg and Broberg, 2005). Attachment security, which is closely linked with maternal sensitivity, is one of the main indicators of early parent–child relationships (Davis, 2004). Considering the significant role of parental cognitions and relationship characteristics on general parenting practices and management of childhood chronic illnesses (Bugental and Johnston, 2000; Hagekull et al., 2001), the investigation of these variables would be valuable.
Previous studies have reported the negative effect of specific types of atopic disease on parenting and mother–child relationships (Hullmann et al., 2010; Morawska et al., 2008). Disrupted family functioning and ineffective parental discipline are related to poor adherence to medication for children with chronic asthma and poor symptom control for children with severe atopic dermatitis (Lehrer et al., 2002; Morawska et al., 2008; Warschburger et al., 2004). The lack of control makes it difficult to determine the influence of each atopic disease on specific parenting cognitions such as parental locus of control and parental sense of competence and quality of relationship. Although these three atopic diseases share the complex dysregulation of the immune system in the pathology and psychosomatic characteristics (Buske-Kirschbaum et al., 2008; Stone, 2003), previous studies examined children with one specific type of atopic disease and used a single variable of parenting characteristics. Therefore, an in-depth investigation of various parental characteristics of mothers who have children suffering from chronic atopic disease by the type and severity of disease, compared with a healthy control group without specific atopic disease, would be useful to develop care plans and change problematic parenting practices.
The specific aims of our study were (1) to examine parental cognitions and relationship characteristics of mothers who have children with chronic atopic disease (including child-rearing attitudes, parental locus of control, parental sense of competence, attachment security, and maternal sensitivity) compared with mothers of children who do not have atopic disease and (2) analyze these variables according to the specific atopic disease, mother’s perception of disease severity, presence of concurrent atopic diseases, and relevant demographic characteristics.
Methods
Study design
This study used a descriptive comparative design to evaluate differences in parenting and relationship variables between mothers of children with atopic disease (atopic disease group) and mothers of children who did not have atopic disease (nonatopic disease group). We also evaluated the parenting and relationship characteristics of mothers according to specific disease, mother’s perception of disease severity, and presence of concurrent atopic diseases.
Sample, setting, and data collection procedure
The participants were recruited from urban areas in South Korea: two local pediatric allergy clinics in Seoul and the Gyeonggi province, two child-care centers in Gyeonggi province, and one university hospital in Daegu. Inclusion criteria were mothers of children aged six years or younger with at least one of the following diseases diagnosed by a pediatrician: atopic dermatitis, allergic asthma, or allergic rhinitis. Mothers of children without atopic disease were recruited from day care centers in the same areas.
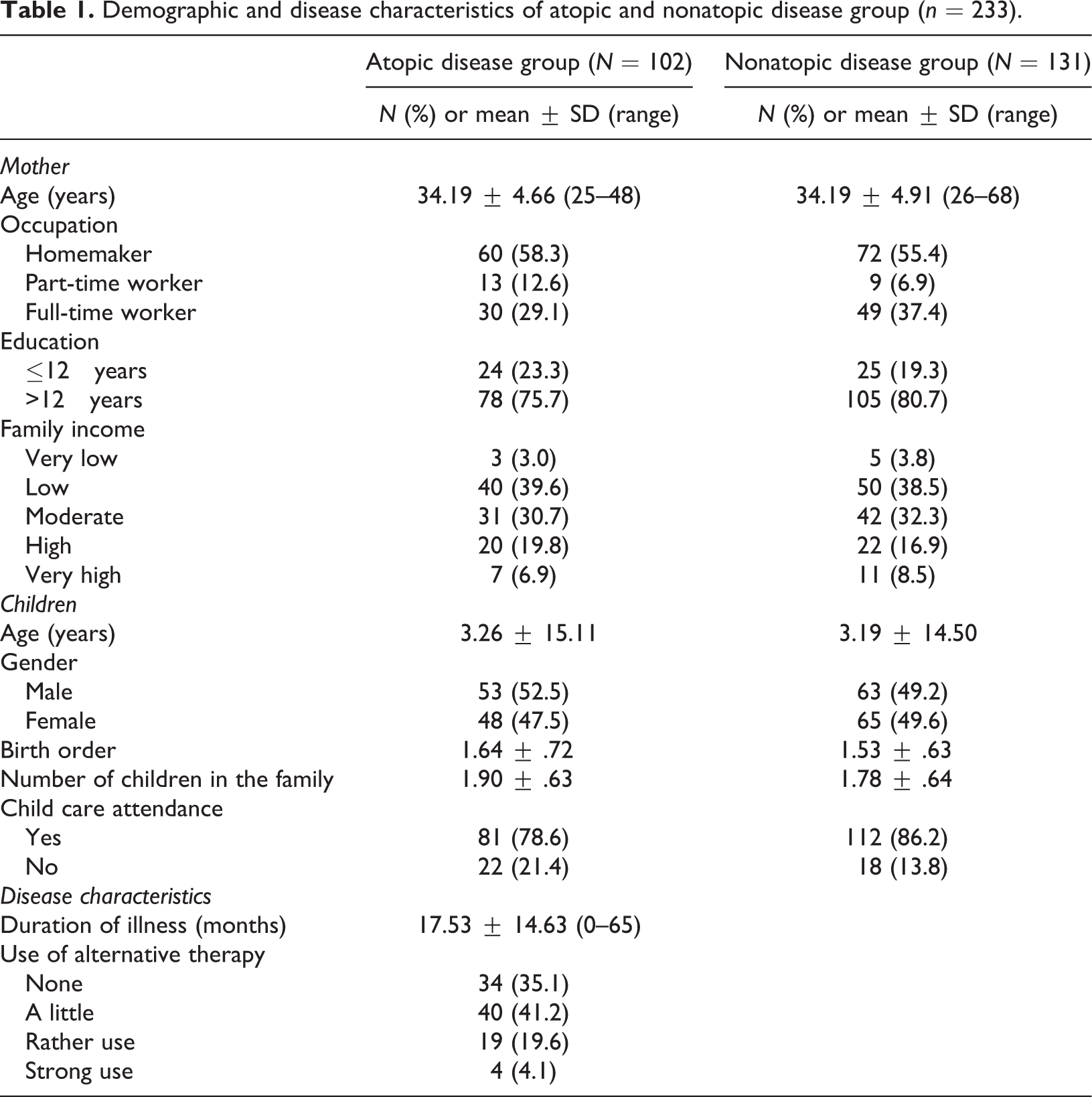
Of the initial 238 mother–child dyads recruited for the study, 233 mothers completed all self-report measures and represent the complete data set (atopic disease group, n = 102; nonatopic disease group, n = 131). Demographic characteristics are shown in Table 1.
Demographic and disease characteristics of atopic and nonatopic disease group (n = 233).
Data were collected from July 2007 to March 2008. The mothers completed the questionnaires at the clinics or at home, taking approximately 30–60 minutes. Mothers were given a gift card (equivalent to US$5) as a token of appreciation for their time. The study was conducted with the approval of the clinics, hospital, and child-care centers. Informed written consent was obtained from all mothers after the purpose, methods, risks, benefits, contact information for any questions, and rights of participants (e.g. participation is voluntary) were explained by the investigators.
Measurements
Demographic and illness-related characteristics
Demographic data collected were the child’s age, gender, birth order, child-care attendance, duration of illness, and the mother's age, occupation, education (years), and family income. The mother was asked to indicate the presence of each subtype of atopic disease (atopic dermatitis, asthma, and/or allergic rhinitis), and the mother’s perception of her child’s disease severity was measured on a 10-point Likert Visual Analog Scale, in which they choose a number to reflect their perceptions. The perceived severity of the disease is considered to indicate its impact on the family (Balkrishnan et al., 2003). Demographic characteristics of the sample are presented in Table 1.
Parenting cognitions
Child-rearing attitude
The mothering attitudes were assessed using the Maternal Behavior Research Instrument developed by Schaefer et al. (1959), which was translated and adjusted into Korean by Lee (1983) and widely used to measure the relative characteristics of child-rearing attitude based on four subscales. The child-rearing attitude measure consists of four subscales: autonomy, control, affection, and rejecting, and the examples of the items were ‘I try to let my child do what she has to do by herself’ (autonomy), ‘I believe a child should follow what parents want to do’ (control), ‘I enjoy the time with my child’ (affection), and ‘I tend to ignore what my child wants’ (rejecting). For the autonomy and affection subscales, higher scores indicate that parents provide more autonomy support and affection toward their children. For the control and rejecting scales, higher scores indicate less controlling and rejecting attitudes. Thus, a high total score reflects a positive child-rearing attitude, with more autonomous, affectionate parenting and less controlling, rejecting parenting. Mothers were asked to rate 50 items on a 5-point Likert scale ranging from ‘strongly agree’ (5) to ‘strongly disagree’ (1). The internal consistency of the total scale measured by Cronbach’s alpha was .72.
Parental locus of control
The Korean version of the Parental Locus of Control – Short Form Revised (PLOC-SFR) (Ahn, 2002), revised by Hassall et al. (2005) from the original scale of Campis et al. (1986), was used to measure parenting control orientation. Mothers were asked to rate items on a 5-point Likert scale. Although the alpha coefficient of the PLOC-SFR has not been reported, Campis et al. (1986) reported an alpha coefficient of .92 for the internal consistency of the total scale. The alpha coefficient for the total scale in this study was .66.
Parental sense of competence
Parental sense of competence, which refers to the degree to which the mother feels competent and confident in handling problems related to her child, was measured using the Korean version of the Parenting Sense of Competence (PSOC) scale used in Yoon’s (2004) research. The PSOC consists of nine items derived from a self-report scale with 17 items developed by Gibaud-Wallston and Wandersman (1978). Mothers were asked to rate items on a 6-point Likert scale, ranging from ‘strongly disagree’ to ‘strongly agree.’ Higher scores indicate a greater parental sense of competence. Yoon reported .85 as the alpha coefficient for the total scale, and the alpha coefficient in this study was also .85.
Relationship characteristics
Attachment stability
The children’s attachment security was assessed with a modified version of Waters and Deane’s (1985) Attachment Behavior Q-sort. The Q-sort was originally developed for a more naturalistic assessment of the attachment relationship and is a behaviorally specific measure that allows valid assessment of attachment security outside the laboratory (Pederson et al., 1990; Waters and Deane, 1985). A 16-item questionnaire was developed by selecting items from Waters’ (1991) revised Attachment Q-set, which were identified by Vaughn and Waters (1990) as discriminating between secure and insecure attachment. Mothers were asked to rate their children on a 9-point Likert scale with anchors and behavioral descriptors that corresponded precisely to the Attachment Q-sort. The questions included ‘If given a choice, my child would rather play with toys than adults,’ and ‘If I move very far, my child follows along and continues his/her play in the area I have moved to.’ Mothers were instructed to report their child’s typical behavior.
Maternal sensitivity
A modified version of the Maternal Behavior Q-set, which was initially developed by Pederson et al. (1990), was used to measure maternal sensitivity. The original Maternal Behavior Q-set consists of 90 items that evaluate a mother’s tendency to recognize her child’s cues and signals or situations that might require her response, to respond promptly to these situations, and to respond appropriately. To enhance the feasibility of the Q-set in our study, we selected 15 items from the behaviors identified by Pederson et al. (1990) that were most likely or least likely to exemplify the sensitive mother. Mothers were asked to rate their behaviors toward their children on a 9-point Likert scale. Higher scores reflect more sensitive, responsive parenting.
Statistical analysis
The power analysis (Faul et al., 2007) using G*Power 3 to calculate the appropriate sample size revealed that the required number of participants for conducting t test were 184 (effect size f = .25, alpha error probability = .05, power = .95), and 111 participants were required to conduct one-way analysis of variance (ANOVA) with three groups (effect size f = .3, alpha error probability = .04, power = .8).
PASW software version 18.0 (IBM Company, Chicago, Illinois, USA) was used for the analysis. Demographic and disease-related characteristics were reported as means, percentages, and SDs. Chi square analysis was conducted to define the differences between the atopic disease group and nonatopic disease group.
The level of statistical significance used in the actual data analysis was .10 as we wanted a more relaxed threshold to act as an early warning signal of variables. Group differences in parenting and relationship characteristics were determined using the t test, ANOVA, and Bonferroni and least significant difference analysis as a post hoc analysis. The t test and ANOVA were also used to compare parenting and relationship characteristics according to the mother’s perception of disease severity. Pearson’s correlation coefficient was computed to determine correlations between demographic and disease characteristics of the children, and the parenting and relationship characteristics of their mothers.
Results
Maternal parenting and relationship characteristics according to the presence and type of atopic disease
Despite our expectations, no significant differences were observed in parenting attitudes, parental locus of control, parental sense of competence, attachment security, or maternal sensitivity scores between groups (Table 2). Further investigation examining differences among specific disease types revealed that mothers of children with atopic dermatitis had lower mean scores of affection than mothers in the nonatopic dermatitis group. No other significant differences were observed between these groups (Table 2).
Maternal parenting and relationship characteristics by the presence and types of atopic disease.
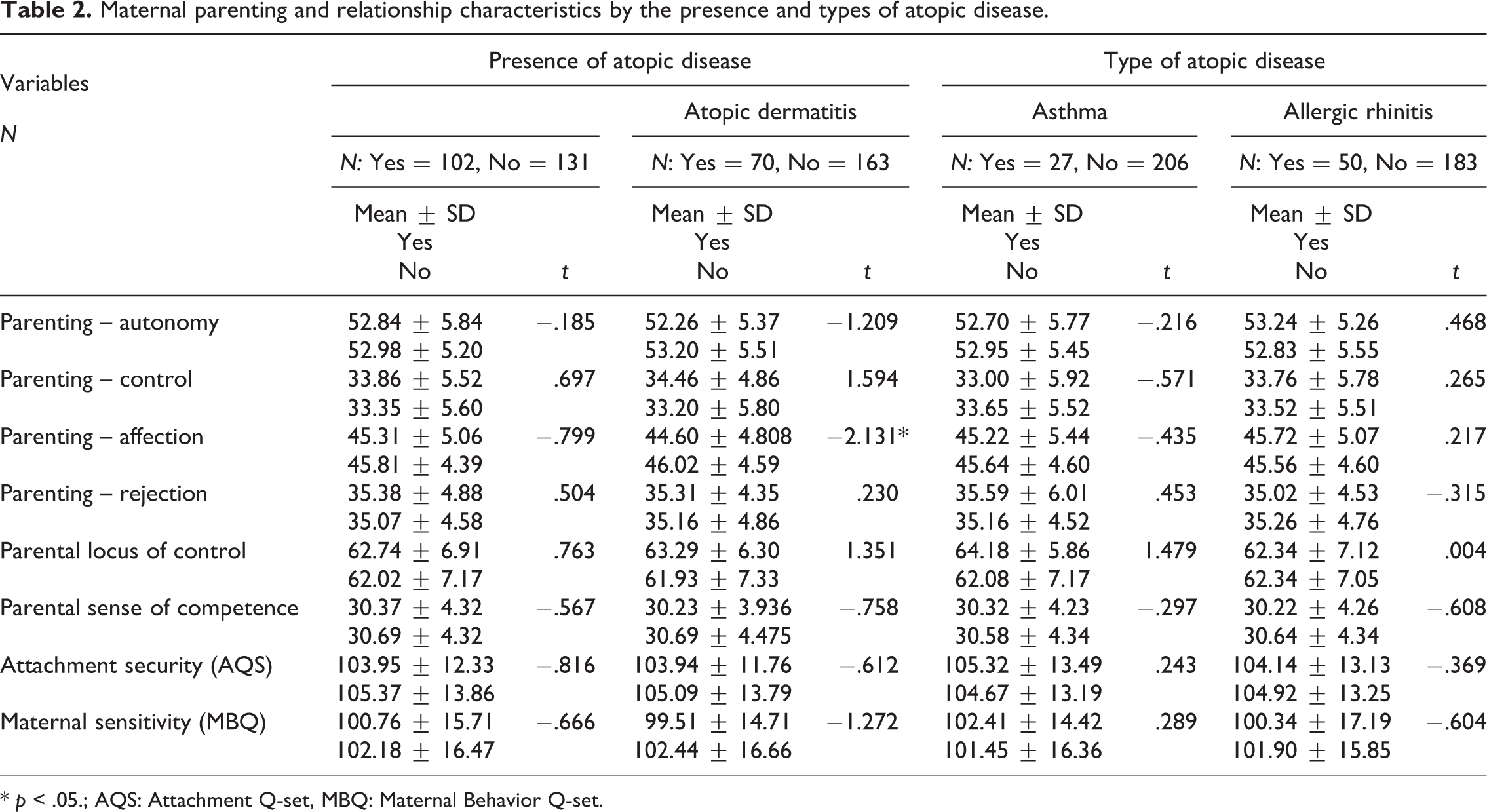
* p < .05.; AQS: Attachment Q-set, MBQ: Maternal Behavior Q-set.
Maternal parenting and relationship characteristics according to perception of disease severity, specific disease, and concurrent atopic diseases
In Table 3, mothers who reported their children’s condition as severe showed less parenting autonomy, more rejecting parenting attitude, more external parental locus of control, and less parental sense of competence compared to those of children having a mild to moderate condition, and specific differences among mild, moderate, and severe groups analyzed by post hoc analysis are presented. No significant differences were observed among these groups regarding parenting control, affection, attachment security, or maternal sensitivity scores.
Maternal parenting and relationship characteristics by the severity of atopic disease (N = 102).
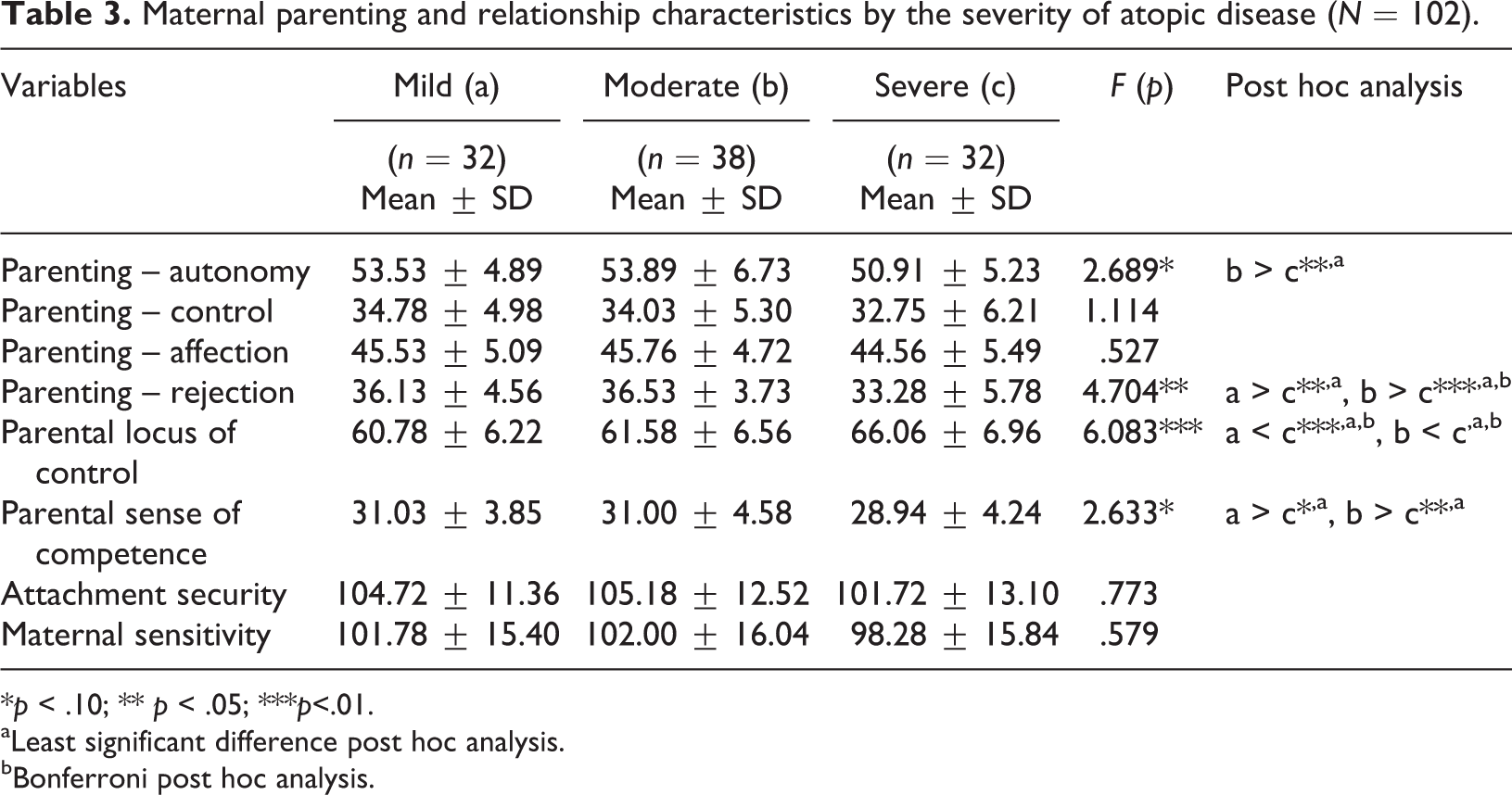
*p < .10; ** p < .05; ***p<.01.
aLeast significant difference post hoc analysis.
bBonferroni post hoc analysis.
Analysis according to perceived severity and specific disease type (Table 4) showed that mothers of children with severe atopic dermatitis were less likely to foster autonomy and reported a more external parental locus of control, lower sense of competence, and lower attachment security than mothers of children with mild to moderate atopic dermatitis. Similarly, mothers of children with severe asthma had lower autonomy scores, a more external parental locus of control, and a lower parental sense of competence than mothers of children with mild to moderate asthma. Finally, mothers of children with severe allergic rhinitis had a lower parental sense of competence score, less secure attachment, and lower maternal sensitivity than mothers of children with mild to moderate allergic rhinitis.
Parenting and relationship characteristics by the perceived severity of each atopic disease.
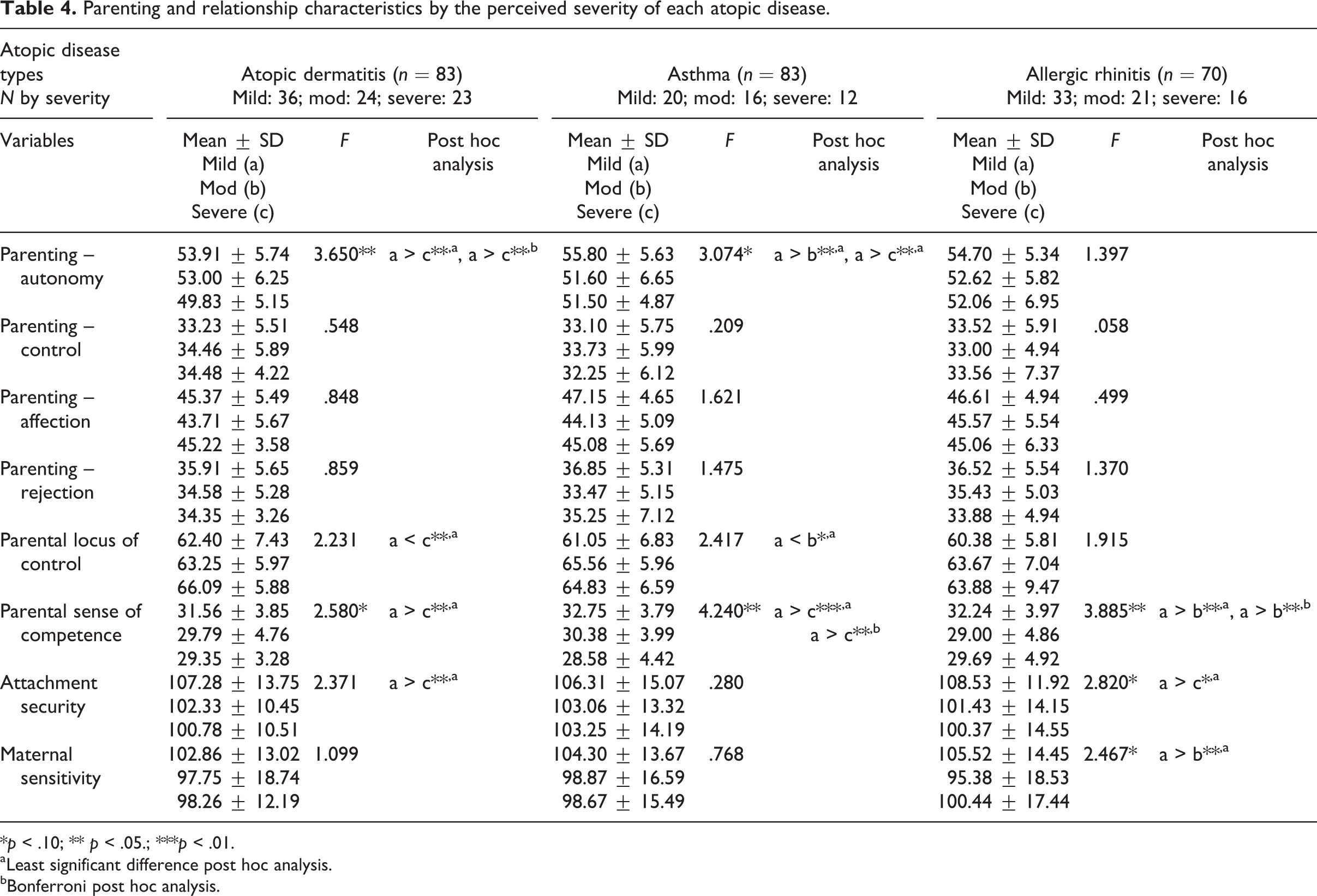
*p < .10; ** p < .05.; ***p < .01.
aLeast significant difference post hoc analysis.
bBonferroni post hoc analysis.
Mothers of children with multiple atopic diseases showed no significant differences in the means of variables compared to those of children having single atopic disease.
Correlations between demographic and disease characteristics and parenting variables
Correlation analysis between demographic and disease characteristics of the children and their mothers’ parenting and relationship variables (Table 5) showed that mothers were more controlling with older children. In addition, older mothers had less rejecting attitudes toward their children. Interestingly, with longer illness duration, mothers were more affectionate and less rejecting. Mothers who perceived their child’s condition to be more severe had a more external locus of control, lower sense of competency, and less secure attachment. In particular, mothers of children with severe atopic dermatitis reported low autonomy scores, high rejecting scores, high external parental locus of control, low attachment security, and low maternal sensitivity. Mothers of children with severe asthma also reported a high external locus of control.
Correlation between demographics/disease characteristics and parenting and relationship variables in the group with atopic diseases (N = 102).
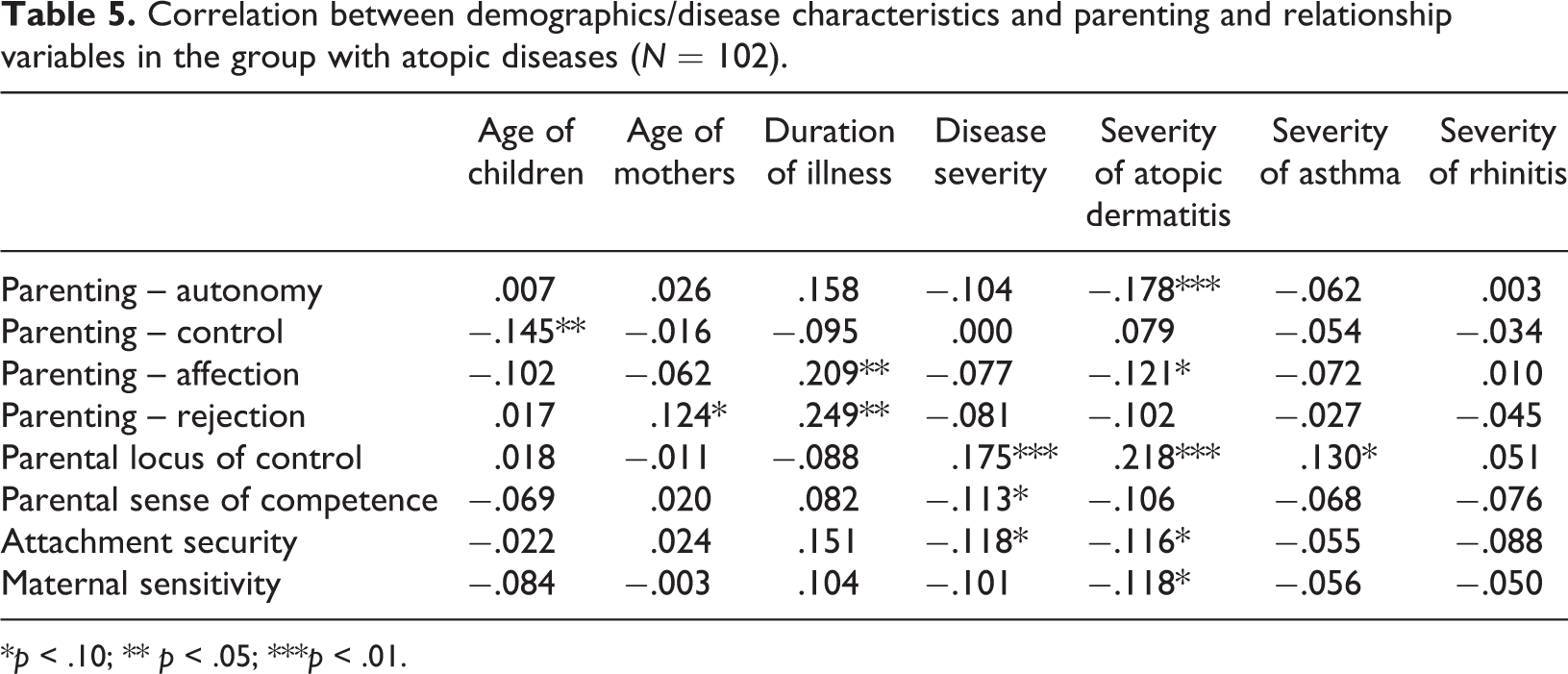
*p < .10; ** p < .05; ***p < .01.
Discussion
This study was designed to compare parental cognitions and relationship characteristics of mothers of young children with chronic atopic disease with those of mothers of children without atopic disease. We evaluated child-rearing attitudes, parental locus of control, parental sense of competence, attachment security, and maternal sensitivity and carried out planned subanalyses according to specific atopic disease, mother’s perception of disease severity, and presence of concurrent atopic diseases.
In our study, we found no significant differences in parental cognitions and relationship characteristics except that mothers of children with atopic dermatitis showed less affection. This finding differed from a previous study reporting that mothers of young children with atopic dermatitis tended to feel guilt and self-blame (Chamlin et al., 2004) and had poorer parenting skills with less effective discipline, significantly more distressed feelings (Daud et al., 1993), and less secure attachment (Cassibba et al., 2004). However, another study reported that the attachment scores of preschool-aged children with atopic dermatitis did not differ significantly from those of healthy controls (Daud et al., 1993), suggesting that health-care providers should not assume that parenting and relationship behaviors are necessarily impaired in mothers of children with chronic atopic disease. Nevertheless, our finding suggests that parent education emphasizing the importance of affection in child rearing may be helpful.
Subanalyses showed that, irrespective of the specific atopic disease, mothers of children with severe disease were less likely to encourage autonomy and had more rejecting attitudes, lower parental sense of competence, and a more external locus of control. Previous studies reported that disease severity, as assessed by a parent or an objective measurement, is an important factor affecting family life (Balkrishnan et al., 2003; Warschburger et al., 2004), parental stress, and parenting style (Pauli-Pott et al., 1999). Given that mothers of severely affected children in our study reported negative parenting traits, it would be useful to determine mothers’ perception of disease severity to identify mothers at risk of poor parenting.
The lower scores for fostering autonomy and higher scores for rejecting attitudes in our study are consistent with previous studies describing the difficulty parents have in disciplining chronically ill children (Hullmann et al., 2010; Morawska et al., 2008). When we analyzed variables according to specific disease and mothers’ perception of disease severity, autonomy scores were especially low among mothers of children with severe atopic dermatitis and asthma, indicating overprotection. Mothers who perceived their children’s asthma or atopic dermatitis to be severe had a more external locus of control, indicating authoritarian parenting, which can undermine the parent–child relationship. A low sense of parental competence was reported by mothers of children with all three disease types when they perceived their child’s condition as severe. Thus, a thoughtfully designed parenting class to reflect on their parenting attitudes and recognize any possible overprotective or rejecting parenting behaviors, and to inform age-appropriate positive discipline based on child’s developmental status, may be helpful for mothers who perceive their child’s condition as severe in order to enhance their child’s autonomy with positive parenting behaviors. In addition, information about the negative effects of parental rejection on the parent–child relationship may be helpful.
In this study, mothers of severely affected children were found to have an external locus of control and low parental sense of competence. External locus of control and intrusive interruption may be related to undesirable behaviors in children (Janssens, 1994). In a study of school-aged children with atopic dermatitis, parents’ rejecting attitudes and coercive control preceded their children’s internalizing and externalizing behavioral problems (Kim et al., 2010). In contrast, parents with an internal locus of control used a self-regulation approach in their parenting, were confident in dealing with their children’s asthma, and had a higher sense of parental self-efficacy (Zimmerman et al., 1999). A care plan such as one providing knowledge about child development and parenting skills to support parents in having age-appropriate developmental expectations and affective interactions with their severely ill young children, avoiding harsh and disruptive parenting, and building social support networking to reduce parental burden may be helpful to enhance parental competence and internal locus of control in parenting (Damashek et al., 2005; Hassall et al., 2005; Kendall and Bloomfield, 2005).
We found that the attachment security score was significantly lower for mothers of children with severe atopic dermatitis or allergic rhinitis compared with mothers of children with milder disease. This result is consistent with the higher rate of insecure attachment reported for children with severe atopic dermatitis in the visible skin area like the face or upper arms (Kim et al., 2008). However, another study found no significant difference in psychiatric adjustment and mother–child attachment of preschool children with severe atopic dermatitis compared with normal controls (Daud et al., 1993).
Mothers of children with severe allergic rhinitis showed less maternal sensitivity and low attachment security than mothers of children with milder allergic rhinitis. To the best of our knowledge, this is the first study of parental cognitions and relationship characteristics that included children with allergic rhinitis. However, previous studies showed that maternal anxiety can increase parental stress (Emin et al., 2009) and damage the child’s self-concept, increasing their vulnerability to high-stress situations (Buske-Kirschbaum et al., 2008), which may prevent mothers from building secure relationships with their young children.
Although we found no significant difference in attachment security among mothers of children with severe asthma, a previous study reported less secure attachments in young children with recurrent asthmatic bronchitis (Cassibba et al., 2004). Given the disruptions in the attachment relationship between mothers and children with severe atopic dermatitis or allergic rhinitis, health-care providers should address these issues carefully. Strategies to enhance maternal sensitivity, such as being attentive to the child’s cues, providing timely and consistent response, expressing a warm, positive, and caring attitude, are needed to enhance the quality of parent–child interactions. Those would ensure the dyadic secure attachment and promote the healthy physical and psychosocial development of children (Klinnert et al., 2001; Madrid and Rio, 2006).
In this study, we found no significant differences in the mothers’ parenting and relationship characteristics when their children had multiple atopic diseases. However, an increased risk of psychosocial problems has been reported for children with multiple allergic diseases (Wu et al., 2011), which further supports the need to assess the quality of the mother–child relationship when the child has multiple atopic disorders. Our study has several limitations. First, we used a self-report measure to assess the mothers’ parenting cognitions and relationship characteristics. Weak or inconsistent relationships have been reported between self-reported parental cognition or attitudes and direct observations of actual parenting (Sigel et al., 1992). Despite using a self-report measure instead of multiple assessment tools to capture real parenting behaviors, we believe our results contribute to the understanding of parenting and relationship characteristics among mothers of children with chronic atopic disease. Second, the small sample size and convenience sampling may limit the ability to generalize our findings. Because parenting and relationship characteristics are culturally sensitive variables, a replication of the study with mothers from different cultural backgrounds is needed to confirm our results. Third, there exists the potential of bias due to unmeasured confounding variables such as child temperament and parental personality. In addition, we evaluated mothers at a single time point; therefore, a longitudinal study is recommended to capture the possible change in parenting and relationship characteristics throughout the course of the disease.
Our findings that mothers who perceived their child’s atopic disease as severe showed low autonomous and high rejecting attitudes with low parental sense of competence and more external control in their parenting, were meaningful to expand our knowledge about the health of and parenting for children having chronically ill atopic disease. In order to advance the quality clinical practice, the specialized care plans to encourage autonomy in child rearing and decrease rejecting attitudes and build internal parental locus of control with enhancing parental sense of competence are strongly required, especially for mothers of children with severe atopic disease.
How might this information affect nursing practice?
To promote optimal physical and psychosocial health in young children with chronic atopic disease, we suggest several guidelines for pediatric nursing practice. First, we should be cautious in generalizing our findings that parenting cognitions and relationship characteristics are impaired in mothers of children with atopic disease. Second, a regular assessment of the mothers’ perception of disease severity is needed. This study revealed that mothers who perceived their child’s disease as severe were less likely to encourage their child’s autonomy and had more rejecting attitudes, an external locus of control, and a low parental sense of competence. Various strategies may be helpful, such as (1) providing mothers with an opportunity to reflect on their parenting to decrease attitudes of overprotection and rejection, (2) increasing social support to ease the parental burden and help mothers develop an internal locus of control, and (3) empowering a mother’s sense of competence by teaching effective parenting skills or ways to cope in stressful situations. These approaches can enhance parenting skills and increase the quality of parent–child relationships. Finally, pediatric nurses should provide a comprehensive care plan to ensure the dyad’s secure attachment through enhancing maternal sensitivity, especially for mothers of children with severe atopic dermatitis and allergic rhinitis.
Footnotes
Conflict of Interest
The authors declared no conflicts of interest.
Funding
This work was supported by the Korea Research Foundation Grant funded by the Korean Government (MOEHRD) (KRF-2006-214-E00031; to Y.-J.I.).