
Abstract
As a magnetic resonance imaging (MRI) examination lasts about 45 minutes and as the technique is sensitive to motion, children are often given sedation or anesthesia. The aim of this study was to examine whether children aged three to nine years could undergo MRI while awake and achieve adequate image quality if age-adjusted routines were used. A two-group controlled experimental design was used. Thirty-six children were assigned to a control group and underwent MRI with the prevalent routines. Thirty-three children were assigned to an intervention group and underwent the MRI while awake. The age-adjusted routine included a booklet and a story book, a model of the MRI scanner with the MRI sound, and a DVD film during the examination. In the control group, 30 children underwent the examination under anesthesia and 6 underwent the examination while they were awake. All had acceptable examinations. In the intervention group, 33 children had their examination while awake and 30 of them had acceptable examinations. The parents’ satisfaction with the care was assessed to be equal or higher in the intervention group and the costs were calculated to be lower. Thus, many children receiving age-appropriate preparation and distraction can undergo MRI examinations while awake.
Children diagnosed with a brain tumor often undergo repeated diagnostic imaging to check for the progress of the tumor and treatment response (Vezina, 2005). Magnetic resonance imaging (MRI) is often preferable to computed tomography (CT) due to its better visualization of soft tissue (Vezina, 2005) and because no ionizing radiation is used. During MRI, the patient has to lie still in a tunnel inside the scanner and a coil is placed close to the examination area, and during data collection and a loud clicking noise can be heard (Mirowitz, 1999; Westbrook et al., 2005). As each examination lasts for 30 to 60 minutes and the technique is sensitive to motion, children are often given sedation or anesthesia before performing the procedure (Malviya et al., 2000).
Studies showed that the number of children who need sedation or anesthesia can be diminished with adjusted preparation and/or realization of the examination (Hallowell et al., 2008; Harned and Strain, 2001; Pressdee et al., 1997). By referring the children to a play therapist and increasing the information to the children, Pressdee et al. (1997) showed that 99% of the children aged between four and eight years could undergo the examination without general anesthesia. Harned and Strain (2001) showed a significant increase in the count of children (age 3–10 years) who managed to go through MRI examinations without general anesthesia but used an MRI-compatible audio/visual system. For children, prior to the real examination, some studies have used practice MRI in an authentic scanner but without the magnet (Hallowell et al. 2008; Carter et al. 2010; De Amorim e Silva et al. 2006;, and De Bie et al. 2010). They showed that 94–98% of the children aged between 3 and 17 years, who had a successful practice MRI, also had an acceptable clinical MRI. In clinical practice, it is still common that children are given general anesthesia or sedation when undergoing MRI examinations (Arlachov and Ganatra, 2012; Cengiz et al., 2006; Slovis, 2011).
Both the confined space inside the MRI scanner and the loud clicking noise are reported to be the main concerns for adults when going through an MRI (Quirk et al., 1989), but there is a huge variation in experience during the examination among adults (Tornqvist et al., 2006b). In a study by Tyc et al. (1995), both children and their parents reported that the intravenous (IV) injection as the most distressing procedural component. Westra et al. (2011) examined children’s discomfort experiences in relation to unsedated MRI and found that 36 of 40 children reported the IV injection to be more distressful than the examination itself. This study aims to determine whether children who receive age-adjusted routines can undergo MRI without deep sedation/anesthesia and achieve scans with adequate image quality.
Methods
The study was carried out as a cohort design with two groups studied at different time periods. The primary outcome was the number of children who successfully went through MRI without deep sedation/anesthesia. Secondary outcomes were image quality concerning motion artifacts, parents’ satisfaction with the care, and costs. The study was carried out in compliance with the Helsinki Declaration and was approved by the Research Ethics Committee of the Medical Faculty, Lund University, Sweden, 606/2006.
Sample
Generally children with brain tumor undergo repeated MRI and preschool children are often given sedation or anesthesia in order to obtain adequate image quality. In this study, the head or head and spine was chosen for examination. Due to the less count of children with brain tumor, all children undergoing MRI of the head or head and spine were included in the study. The inclusion criterion was children aged 3 to <9 years scheduled for an elective MRI examination of the head or the head and spine. Exclusion criteria were (i) children who underwent an MRI while awake prior to this study, (ii) children with obvious developmental delay, (iii) children of the families who could not speak and understand Swedish, and (iv) children who underwent MRI of other body parts other than head or head and spine. Calculation of the necessary sample size showed that 30 plus 30 (30 each in control and intervention groups) children give a power of 0.80 to prove a difference between the control and intervention groups of 30% unit with a significance of p = .05 (Altman, 1991). Informed consent was obtained from all parents. Children were given age-appropriate information and their assent was obtained.
The sample consisted of consecutive series of children scheduled for MRI and their accompanying parents assigned to a control group (36) for 13 months (February 2008–March 2009) and an intervention group (33) for 14 months (May 2009–June 2010). The control group included all children requiring head or head and spine examinations for diagnostic reasons. The intervention group included children requiring head or head and spine MRI examination for diagnostic reasons (17) and children, born full term and preterm, being assessed for brain development (16).
Settings
The study was carried out at a pediatric day care unit and the radiological department at the Skåne University Hospital in Lund, Sweden. Two MRI scanners (Intera 1.5 T and Intera 3T, Philips Healthcare, Netherland) were used for the examination.
Routine care
Children in the age-group between three and nine years are traditionally scheduled for MRI examinations by administering deep sedation/anesthesia. The parents receive the appointment date together with brief information about the examination (for adults) and a booklet for children about preparation for anesthesia, which should be read by parents and child together. The child is appointed to the day care unit two hours prior to undergoing the MRI examination. Every child receives Emla® and is examined by a pediatrician. When called, the child (accompanied by parent(s)) is transported to the MRI department in a bed. The anesthetist prepares the child with intravenous catheter (IVC), sedate or anesthetize (usually Propofol® is used) and takes care of the child from the time of arrival until he/she is moved to the recovery ward. After a recovery period of about one hour, the child is returned to the pediatric day care unit, for another couple of hours, before the family goes home. If the child is scheduled for an MRI examination while he or she is awake, the family receives the same brief written information as for adults and is invited to visit the MRI department prior to the examination. For a child to undergo an MRI while awake, it has to be proposed by the parents or the doctor and then agreed by the parents, the child, and the doctor. In this study, no one influenced the decision regarding whether or not the children in the control group should undergo MRI while awake or not.
Care according to intervention design
In the intervention group, all children underwent the same intervention and all received extra preparation in three ways. (1) A booklet and a storybook were sent home to the families, which was to be read together by the parents and child. (2) A ‘doll-size’ model of an MRI scanner made with an MP3 player with the MRI sound recorded was shown to the child at the day care unit. (3) The child watched a DVD film while undergoing MRI. The sound of the film was transferred through the headphones. The parents were asked to decide whether the child was to undergo the MRI with or without anesthesia. The appointment was booked thereafter with or without the support from anesthetist. All parents were informed that if the MRI undertaken when the child was awake lacked adequate image quality, then the parents would have to reschedule a new appointment so that MRI could be done whilst the child was under deep sedation/anesthesia. A pilot study was implemented in order to test the instruments and procedures. The pilot study confirmed the use of the three interventions for this larger study.
Instruments
The care given was evaluated in four different ways:
Information was recorded in a protocol drawn up for the study regarding whether the child had deep sedation/anesthesia or was awake, the diagnosis, the number of sequences, duration of events, and whether or not the examination was aborted.
Image quality and motion artifacts were assessed. The motion artifacts were graded as none, mild, moderate, or severe; and if there were artifacts, the number of sequences with acceptable quality was recorded in a protocol (also used in Tornqvist et al., 2006a) by the radiographer conducting the examination. A radiologist was consulted, if there were any doubts as to the quality of the image.
The parents recorded their satisfaction/dissatisfaction with the care of the child in a modified questionnaire called Healthcare Satisfaction Module specific for Hematology/Oncology (Varni et al., 2000). The questionnaire has 20 questions in 6 dimensions (information, communication, emotional needs, technical skills, inclusion of family, and general satisfaction), each with 5 alternative replies. The 1–5 points were transferred to a scale from 0–100 (0/25/50/75/100) where 100 meant ‘very satisfied’.
Costs for the examination were calculated from the price list ‘Local prices and compensations in the Southern Health Care Region, 2010’ (SödraRegionvårdnämnden, 2010), as if the examinations were carried out during the same period. The calculation was made using the price for the most common examination (head with and without contrast medium) and, when anesthesia was used, using the mean time for anesthetic care and time spent in the recovery ward. Costs for information and preparation material were calculated.
Data collection
Data were collected in connection with the child’s examination. If the child had deep sedation/anesthesia, the parents were asked to complete the questionnaire when the child came back to the day care unit and not directly after the examination. The costs were prospectively recorded and calculated when the study was completed.
Analysis
The statistical software SPSSTM was used for statistical evaluation using the Mann–Whitney U test for comparison between the groups. For nominal data, a chi-square test and Fisher’s exact test were used. The effects on costs for the control and intervention groups were calculated. A p value of less than .05 was considered statistically significant.
Results
Patient recruitment and characteristics
All 36 children and parents who were invited to participate in the control group agreed to participate in the study. Of the 26 children undergoing MRI for diagnostic reasons and their parents who agreed to participate in the intervention group, 9 parents chose to let the children undergo MRI with deep sedation/anesthesia, thus not participating in the study. All children (n = 16) undergoing MRI for assessment of brain development and their parents who were asked to participate also accepted to participate in this study. Patient recruitment and characteristics of the children and the examinations in the two groups are shown in Figure 1 and Table 1.
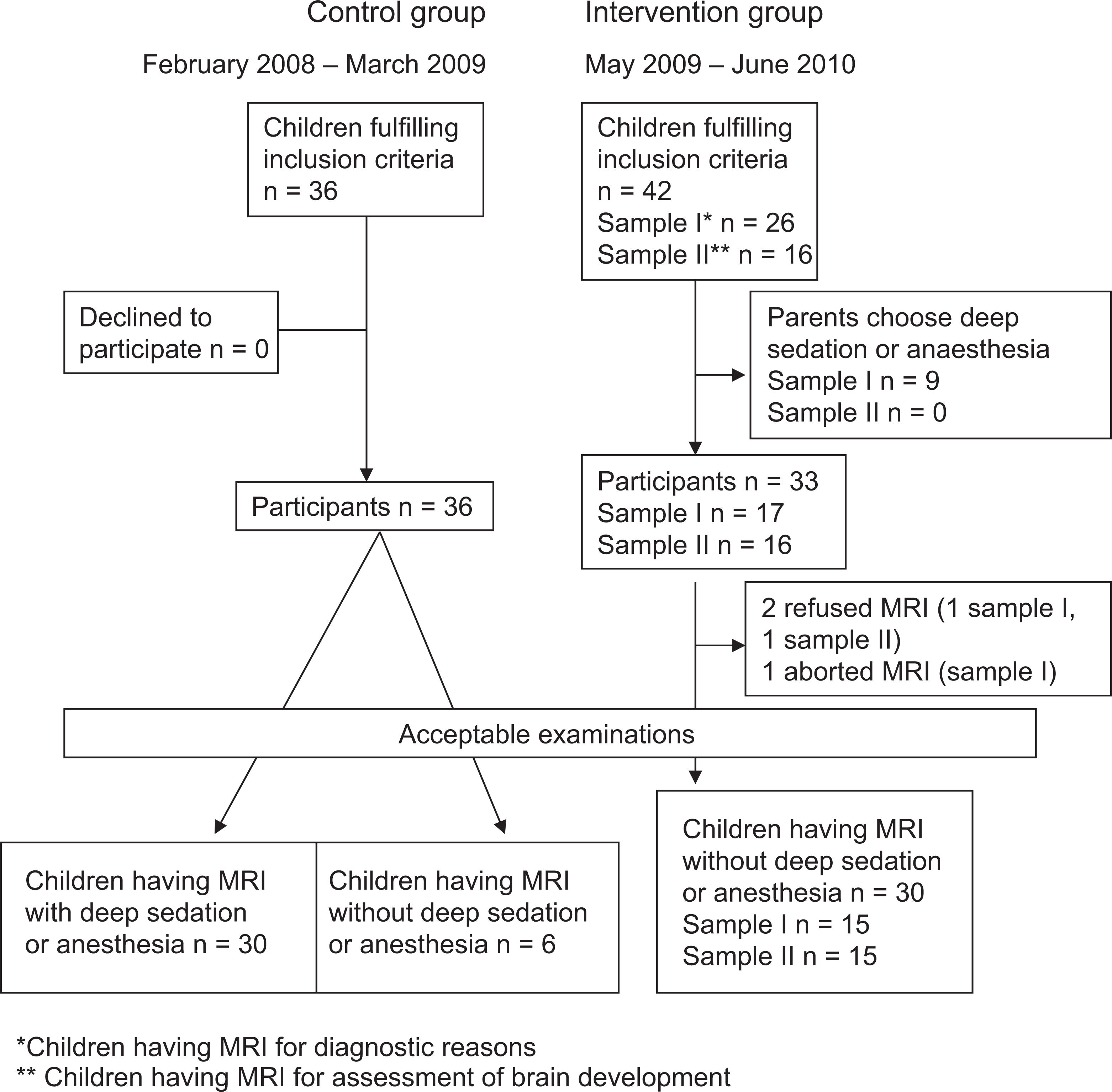
Overview of patient recruitment and MRI examinations. MRI: magnetic resonance imaging.
Sample characteristics.
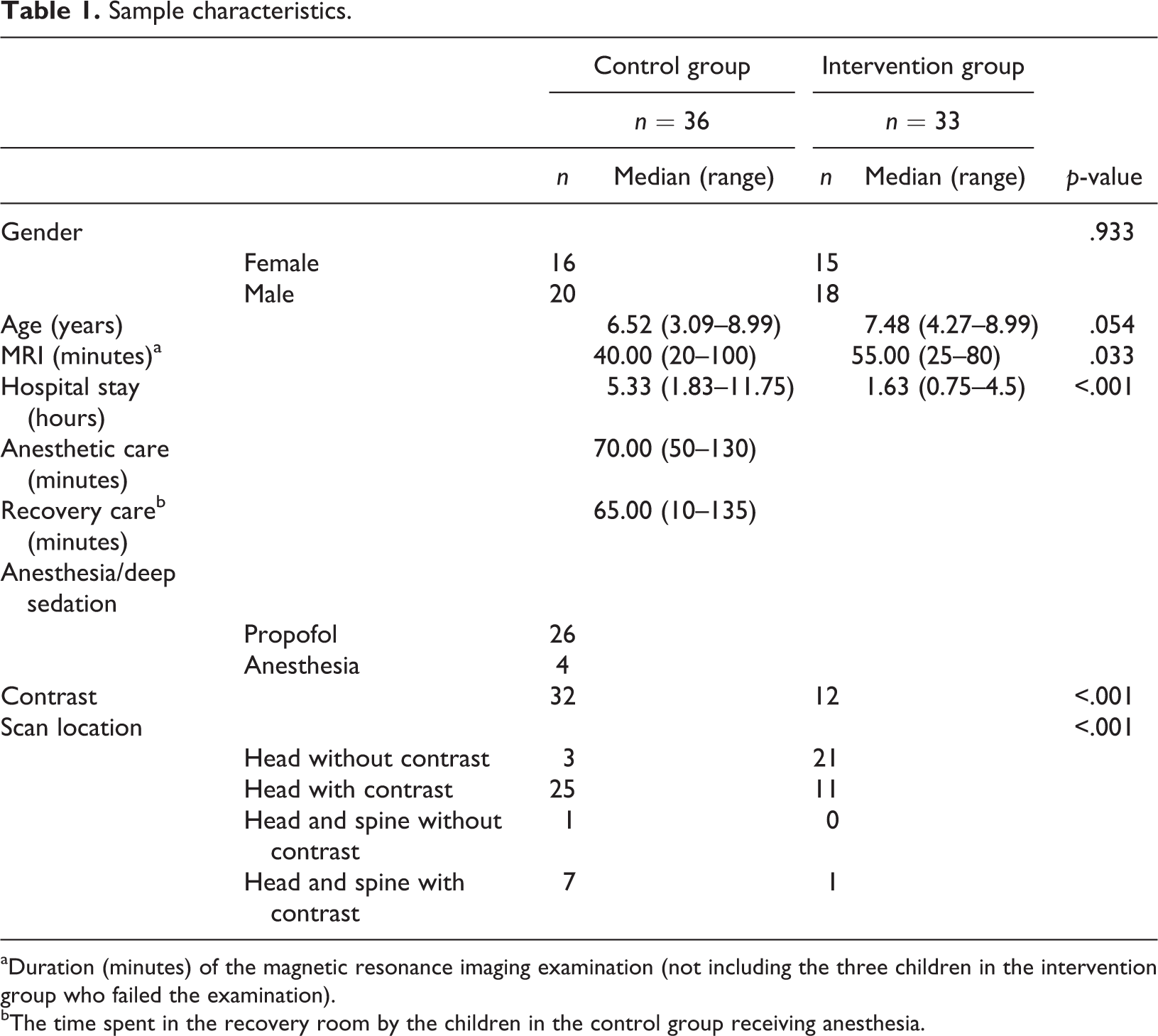
aDuration (minutes) of the magnetic resonance imaging examination (not including the three children in the intervention group who failed the examination).
bThe time spent in the recovery room by the children in the control group receiving anesthesia.
There was no significant difference concerning gender and age between the control and intervention groups. There was a difference in the duration of the examination, with a significantly longer duration in the intervention group (about five minutes), and there was a significantly longer duration of hospitalization in the control group (approximately three hours.). In the control group and intervention group of children undergoing MRI for diagnostic reasons, 23 of 36 and 10 of 17, respectively, had to undergo MRI for the diagnosis of a brain tumor. Contrast medium was used for 32 children in the control group and for 12 in the intervention group (p < .001). For all children undergoing MRI for assessment of brain development, the head examination was done without contrast (Table 1).
Nine children, two girls and seven boys, not participating in the intervention group, had a median age of 5.50 years (range: 3.53–8.97). There was no significant difference in age among children undergoing MRI for diagnostic reasons (p = .349).
Primary outcome
All 36 children in the control group, 30 with deep sedation/anesthesia and 6 without, had acceptable MRI examinations compared to 30 of the 33 children who underwent MRI without deep sedation/anesthesia in the intervention group. For an acceptable MRI examination, all important structures must be visibly sharp in at least one of the sequences to ensure accurate diagnoses. Two children (aged five and eight years) in the intervention group refused to undergo MRI; and in one child (aged five years), the examination was terminated prematurely (Table 2, Figure 1). Three children in the intervention group underwent a total of 10 additional MRIs while awake during the data collection period.
Acceptable examinations, motion artifacts, and parents’ satisfaction with care.
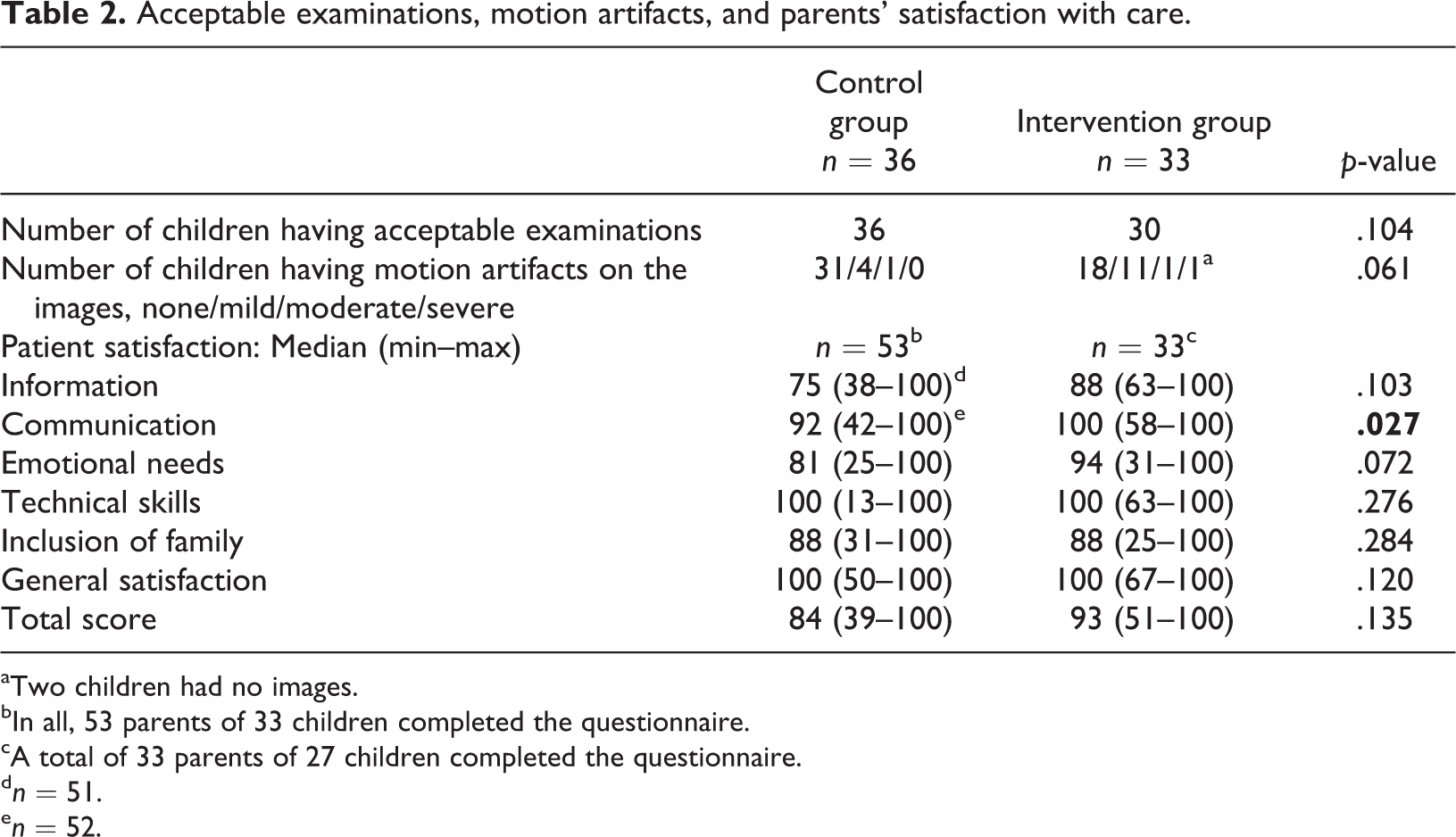
aTwo children had no images.
bIn all, 53 parents of 33 children completed the questionnaire.
cA total of 33 parents of 27 children completed the questionnaire.
d n = 51.
e n = 52.
Secondary outcome
Concerning image motion artifacts, 5 children in the control group and 13 in the intervention group had images that were assessed to have motion artifacts (Table 2). One child in the intervention group was assessed as having images with severe motion artifacts and the examination was therefore prematurely terminated. All other children who underwent MRI were assessed to have acceptable images. Three of those children had sequences with unacceptable quality, but the examination as a whole had enough images with good quality (at least 75%).
Comparison of parent satisfaction showed no significant difference concerning the total score, information, emotional needs, technical skills, inclusion of family, and general satisfaction. There was a significant difference concerning communication, with the intervention group scoring higher (Table 2).
The cost for a head MRI (without and with contrast medium) with deep sedation/anesthesia is calculated to be SEK 13,964 and without deep sedation/anesthesia SEK 5258 (SödraRegionvårdnämnden, 2010). The initial costs of the material used in the intervention group were calculated to be SEK 30,200 (Table 3).
Calculated costs for one head MRI examination with and without contrast medium in the control and intervention groups, and initial costs in the intervention group (Costs in SEK).
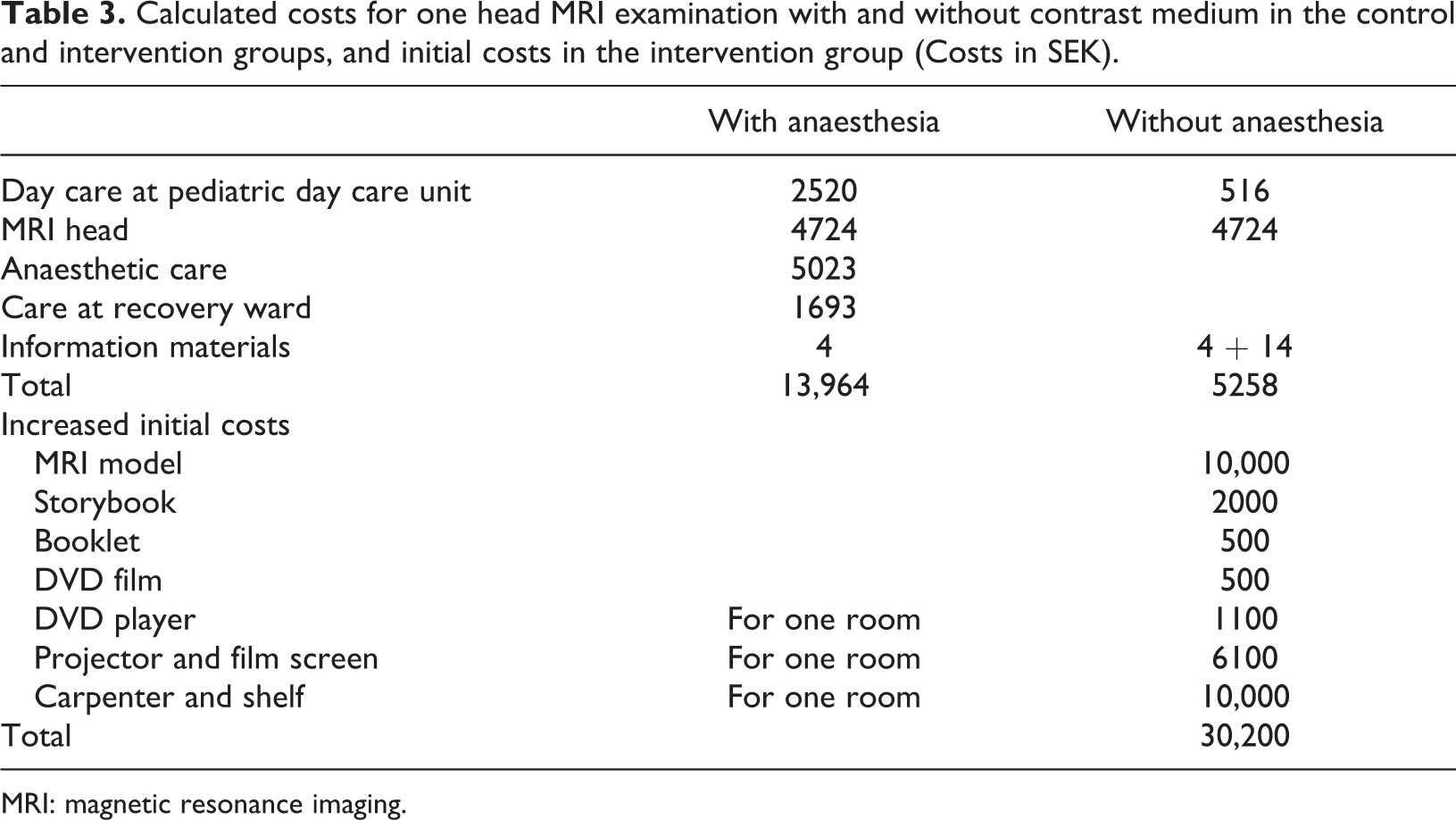
MRI: magnetic resonance imaging.
In the control group, 30 children underwent MRI with deep sedation/anesthesia and 6 without. If we consider that to be a normal distribution (when no effort is made to let more children have MRI awake) the total calculated costs for 30 children with, and 6 without anesthesia are Swedish Krona (SEK) 450,468 in total (36 children) and SEK 12,513 per child.
For children in the intervention group undergoing MRI for diagnostic reasons, nine parents and children preferred the examination in deep sedation. If we assume that also nine parents and children undergoing MRI for assessment of the brain had done the same, we calculate that 18 children were given deep sedation/anesthesia, 33 children were awake, and three children had two examinations (without and with deep sedation/anesthesia).
Discussion
Of the 33 children aged between four and nine years who underwent an MRI examination while awake, 30 managed to complete the examination with acceptable image quality after receiving age-appropriate preparation. More number of the awake children than those in the control group had motion artifacts on their images, although these were acceptable. The parents were equally or more pleased with the care, and the costs were calculated to be lower in the intervention group.
There are some limitations in this study that need to be acknowledged. Although the focus was on children with brain tumor, all children undergoing head or head and spine examination was included in the study. This made the sample more heterogeneous than only the children with brain tumor were included. The children with brain tumor have experienced many ‘hospital visits’, while that may not be the case for those children undergoing MRI for other reasons. However, even the children in the intervention group used to medical intervention had never underwent an MRI while awake. Thus, we had no prior knowledge as to whether the children could undergo MRI without deep sedation/anesthesia. The inclusion of children other than those with brain tumor was done to minimize history bias as we considered it important that the data collection should not last over too long a period as changes in the organization and environment could impair the result. There were significantly fewer children having contrast medium in the intervention group, which might affect the result positively. No children under four years of age participated in the intervention group, and, therefore, we cannot comment whether a three-year-old child can undergo MRI while awake. Children and parents in the control group were not, in this study, encouraged to undergo MRI while awake, they just followed the ordinary routine. Thus, no comparison can be made as to how many of these children could have managed MRI while awake, without the extra age-adjusted preparations and routines.
Random assignment was not used as it would involve different treatments being given at the same time, which might confuse not only the children and their parents but also the professionals. To impart a sense of security to children and parents, all the professionals needed to be conversant with the procedures and routines used. This was considered to be difficult with two different procedures running in parallel.
No questionnaire was found measuring parents’ satisfaction regarding care concerning radiological examinations. After permission from the creator (Varni et al., 2000), the Healthcare Satisfaction Module specific for Hematology/Oncology was adjusted in order to evaluate a situation including examinations instead of only general care and translated to Swedish. Thus, the questionnaire is not validated and the result must therefore be interpreted with caution.
To help the children to experience control and to become familiarized with the examination situation (Runeson et al., 2002), the preparation for the examination included a booklet, a storybook, and a model of an MRI scanner with a sound recorder. Since children as well as adults take in information in different ways and children develop at a different pace (Pramling, 1983), it was considered to be an advantage that different kinds of information were used.
As shown in our study, as well as in others (Carter et al., 2010; De Amorim e Silva et al., 2006; De Bie et al., 2010; Hallowell et al., 2008; Harned and Strain, 2001; Pressdee et al., 1997), most children can lie still during an MRI examination if they are prepared and/or distracted by film. Not every hospital has the advantage of a practice MRI room (Carter et al., 2010; De Amorim e Silva et al., 2006; De Bie et al., 2010), pediatric occupational therapist (Carter et al., 2010), play therapists, (De Amorim e Silva et al., 2006; Hallowell et al., 2008; Pressdee et al., 1997), and child-life specialist (De Bie et al., 2010). The intervention suggested here can be carried out with ordinary staff and with minor investments, a small MRI model, a storybook, a booklet, and a DVD player with a projector and film screen. Minimal additional time was invested by standard staff to introduce the MRI model and setup the DVD. This additional time spent by staff must be weighed against the benefits for the families and the cost savings.
When the child undergoes MRI while awake, there are advantages both for the child and for her/his family. The child may not need deep sedation/anesthesia with the discomforts and risks that are associated with such procedures (Malviya et al., 2000; Von Ungern-Sternberg and Habre, 2007), the child need not fast, and the hospital stay will be shorter. For the health care system, examinations without deep sedation/anesthesia would be advantageous for logistic reasons since fewer staff members would be needed and patients would not have to wait such a long time for their examination. Also costs may be decreased if enough children succeed in undergoing the MRI while awake. Calculations from our results showed that costs decreased to about SEK 3000 per patient even if 3 children had to repeat the MRI and some children and parents preferred the examination with deep sedation/anesthesia. However, to evaluate the implementation of new routines, a carefully performed health economic evaluation should be done.
However, when undergoing MRI, it is most important that the image quality is good enough for diagnostic purposes. In this study, more children in the intervention group had image motion artifacts than in the control group, although with acceptable quality. Only one child had so many artifacts that the MRI was terminated. Hallowell et al. (2008) showed that 96% of 227 children aged between three and 17 years undergoing MRI without deep sedation/anesthesia had acceptable examinations, although 60% showed signs of movement on the images. Studies (Dantendorfer et al., 1997; Tornqvist et al., 2006a) have also shown that 4–15% of adult patients have motion artifacts on their images.
There will always be a risk that a child undergoing the MRI while awake does not have acceptable images and will need to go for a second MRI. Considerations have to be made with regard to the risk of exposing children who have had a failed MRI while awake and when repeating the procedure with deep sedation/anesthesia. If, on the other hand, the child succeeds in undergoing the MRI while awake, he/she will most probably be able to do so again, as three children showed in this study.
In this study 30 of 33 children could undergo MRI while awake, which may indicate that parents are good predictors of what their child can manage and also ‘no contrast’ may be another possible predictor of a successful awake MRI.
Conclusion
Thus, age-appropriate preparations and film distractions for children and good communication between family and professionals may allow in the realization of many children aged between four and nine years, that is, being able to undergo MRI while awake.
Footnotes
Conflict of interest
The authors declared no conflicts of interest.
Funding
This work was supported by the Swedish Children's Cancer Foundation [grant numbers 06/021, 2007-2009] and the Mayflower Charity Foundation for Children [grant numbers 49, 2007].