
Abstract
Low adherence is a pervasive issue among youth with inflammatory bowel diseases (IBD), yet our understanding of perceived adherence barriers is hampered by a lack of validated instruments. This study sought to address this by evaluating the reliability and predictive validity of the Beliefs About Medication Scale (BAMS) among youth with IBD. Seventy-six youth (ages 11–18) with IBD who were prescribed a daily oral IBD medication completed baseline ratings of perceived adherence barriers via the BAMS. Parents provided information about patient demographic and disease factors. Subjective medication adherence was assessed via the medication adherence measure. Objective medication adherence was assessed via Medication Event Monitoring System (MEMS) Track Caps. BAMS subscales demonstrated adequate internal consistency (αs = .78–.90) and test–retest reliability (rs = .64–.79). BAMS subscales reliably distinguished between adherent and low adherent groups, though intent to adhere (IA) was the only independent predictor of adherence status. The BAMS holds promise as a tool for assessing adherence barriers among adolescents with IBD. IA may be of particular value in identifying adolescents at risk for low adherence.
Introduction
Inflammatory bowel diseases (IBD), including ulcerative colitis and Crohn’s disease, are incurable diseases affecting the gastrointestinal system that cause significant physical health and psychosocial morbidity (Mackner et al., 2013). IBD affects 1.4 million individuals in the United States, and 20–25% of those diagnosed are under 18 years old (Heaton et al., 2012). Treatment aims to manage symptoms (e.g. abdominal pain, diarrhea, growth failure) and promote disease remission via a multicomponent regimen that often includes daily oral medications.
Although oral medication adherence enhances physical and mental health outcomes in pediatric IBD, adherence is suboptimal, and as many as 88% of adolescents with IBD do not take their medication exactly as prescribed (Hommel et al., 2013). Adolescents are at risk for lower levels of adherence than younger youth, given the rapid cognitive, social, and psychological changes occurring during this developmental period (Hanghøj and Boisen, 2014). In fact, research has identified several barriers to adherence that may be particularly salient for adolescents, including a desire to fit in with peers, difficulty in fully understanding the long-term risks of low adherence, and immature problem-solving and organizational skills (Hanghøj and Boisen, 2014; Stewart and Dearmun, 2001). Moreover, given that adolescence is a time in which teens increasingly gain autonomy from their parents, they may be at risk for lower levels of medication-related supervision than younger youth, which may also negatively impact adherence (Hanghøj and Boisen, 2014; Stewart and Dearmun, 2001).
Low medication adherence among adolescents is particularly problematic, since the health risk behavior patterns that emerge during this developmental period are likely to persist into adulthood (Hommel et al., 2013; Williams et al., 2002).
Among adolescents with IBD, efforts to enhance adherence are hampered by a lack of measures of adherence barriers validated for use with this specific patient population. Specifically, most measures of adherence barriers have not been developed or evaluated specifically in IBD groups, and few of the existing measures have focused on cognitive factors associated with low adherence (e.g. perception that medication causes side effects, belief that medication is unnecessary). However, theoretical paradigms such as the health beliefs model and common sense model highlight the importance of addressing maladaptive cognitions about one’s illness or treatment regimen to promote long-standing improvements in adherence (Janz and Becker, 1984; Leventhal et al., 2003). Moreover, some existing data suggests that attention to beliefs about medication is an important component of promoting medication adherence in pediatric groups (Carter, 2015). Additionally, our recent work suggests that maladaptive cognitions may be particularly salient for adolescents with IBD (Greenley et al., 2017), offering further support for the value of assessing cognitive barriers to medication taking.
The Beliefs About Medication Scale (BAMS; Riekert and Drotar, 2002) is an adolescent-report measure of beliefs about oral medications. The development of the measure was informed by social cognitive theories (e.g. health beliefs model, theory of planned behavior, and self-efficacy theory (Ajzen, 1985; Bandura, 1997; Janz and Becker, 1984)). The measure has demonstrated acceptable internal consistency and short-term test–retest reliability among adolescents with various chronic medical conditions (i.e. asthma, HIV, IBD), and the four-factor structure (i.e. perceived threat of illness, positive outcome expectancies associated with adherence, negative outcome expectancies associated with low adherence, and intent to adhere to oral medications) was supported by confirmatory factor analysis (Riekert and Drotar, 2002). The validation study supported the predictive validity of the positive outcome expectancies, negative outcome expectancies, and intent to adhere subscales of the BAMS for self-reported adherence.
Although preliminary data are promising with respect to the value of the BAMS, its psychometric properties have not been specifically examined in a sample of adolescents with IBD. Although youth with IBD share some similarities with youth with other chronic diseases, it remains important to examine the measure’s psychometric properties among youth with IBD specifically for several reasons. First, since IBD is often diagnosed during adolescence (Cuffari, 2009), a time in which cognitive developmental changes allow for improved thinking about the future, cognitive barriers may be particularly relevant to this group. In addition, compared to conditions diagnosed earlier in childhood, adolescents with IBD have limited time to acclimate to regimen responsibilities and fewer opportunities to observe the benefits of long-term adherence or the long-term risks of low adherence. Third, IBD medications focus on long-term remission, and a single/few missed dose(s) have little immediate impact on physical health. Thus, youth with IBD may have lower perceptions of negative outcomes associated with low adherence compared to youth with other chronic conditions (e.g. type 1 diabetes), in which low adherence has almost immediate effects. Finally, given that IBD involves socially embarrassing symptoms (e.g. diarrhea, blood in stool), adolescents with IBD are reluctant to share their diagnosis with peers, creating unique social barriers compared to conditions in which disclosure of illness is more normative (Lu and Markowitz, 2011).
This study sought to provide additional data regarding the psychometric properties and clinical utility of the BAMS in a sample of adolescents with IBD. First, we aimed to evaluate the reliability of the BAMS. We hypothesized that the BAMS would show adequate internal consistency, mean item-total correlations, and test–retest reliability. Second, we sought to evaluate the predictive validity of the BAMS for subjective and objective reports of oral medication adherence. Past work has documented associations between BAMS scores and self-reported adherence (Riekert and Drotar, 2002); however, the predictive validity of the BAMS for objective adherence (e.g. electronic monitor assessment) has not been evaluated. We hypothesized that each of the BAMS subscales would be significant predictors of subjective and objective adherence. In recognition that measure development and validation should occur over multiple studies (Holmbeck and Devine, 2009), our goal was to build upon the preliminary support for the BAMS as a reliable and valid assessment screener for adherence barriers among adolescents with IBD, a group known to be at increased risk for low adherence (Hommel et al., 2013).
Methods
Participants
Participants were part of a randomized controlled trial of the effectiveness of a phone-based adherence-promotion intervention for youth with IBD (Greenley et al., 2015). Data for the current analyses included only baseline assessments prior to the implementation of any intervention. Participant inclusion criteria were (a) diagnosis of IBD, (b) prescribed daily oral IBD maintenance medication, (c) patient 11–18 years old at enrollment, (d) parent/guardian willing to participate, and (e) English fluency. Youth with a cognitive impairment that precluded questionnaire completion or those with a comorbid medical condition that required daily prescription medication were excluded.
Seventy-six of 172 families approached for participation agreed to participate (44%), which was consistent with participation rates of other behavioral health trials (Hommel et al., 2012). Parents and adolescents aged 18 provided written consent for their own participation. Adolescents aged 11–17 provided written assent for participation, and parents provided written consent for minor adolescent participation. No differences in age or sex between participants and nonparticipants were documented. Mean participant age was 14.5(1.87) years. Fifty-one percent of participants were male, and most were Caucasian (87%). See Table 1 for additional demographic and disease characteristics.
Demographic and illness characteristics.
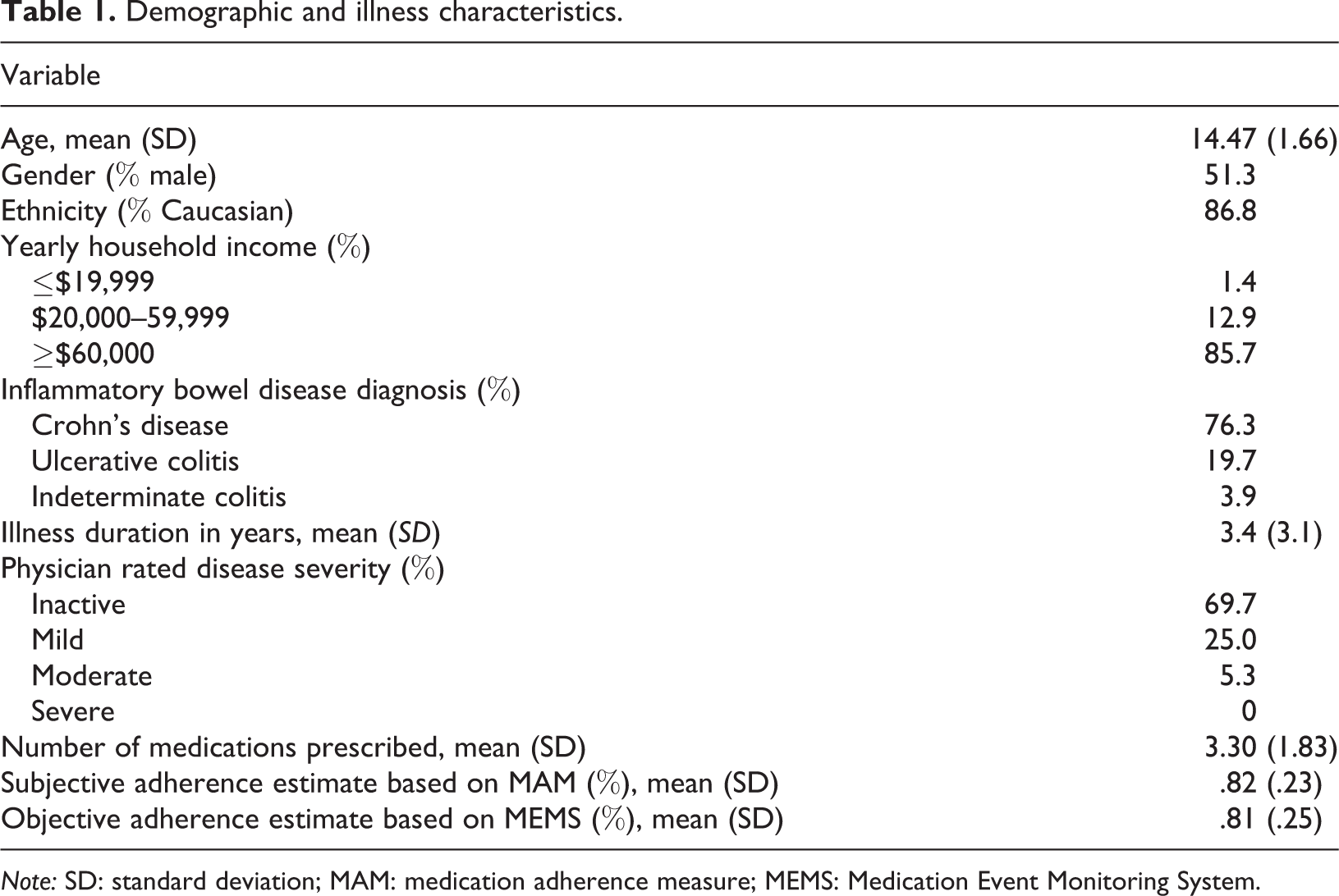
Note: SD: standard deviation; MAM: medication adherence measure; MEMS: Medication Event Monitoring System.
Procedure
Participants were recruited at one of two Midwestern children’s hospitals during outpatient gastroenterology clinic appointments. Forty-five participants were recruited from site 1 and 31 participants were recruited from site 2. Interested families provided written consent/assent. Participants were given a Medication Event Monitoring System (MEMS) Track Cap and bottle at the time of enrollment. Participants prescribed multiple oral medications used the MEMS device for the most complex regimen (i.e. medication requiring the most daily dosings). One month after enrollment, participants completed a baseline assessment involving youth- and parent-report questionnaires, and youth completed a semi-structured adherence interview. Participants were subsequently randomizedinto an intervention group or a wait listcomparison group (WLCG). Twelve weeks later, those in the WLCG (N = 26) completed the same evaluation, which allowed for test–retest reliability analyses. During the 12-week period between the first and second assessments, WLCG participants obtained routine medical care but did not receive any formal exposure to adherence-promotion strategies. Participants were compensated for participation. The institutional review boards at participating institutions approved all study procedures. Full procedural details for the parent study are reported in (Greenley et al., 2015).
Measures
Demographic and disease information questionnaire
Parents completed a questionnaire that recorded demographic information (i.e. child’s age, race/ethnicity, sex, and family income). Additionally, parents reported on the child’s type of IBD, diagnosis date, and prescribed medications.
Physician Global Assessment Scale
Gastroenterologists rated disease activity at the time of enrollment using the Physician Global Assessment (PGA) Scale (Hanauer et al., 1993). Physicians rated disease activity on a 4-point Likert-type scale, in which 0 = No disease activity/clinical remission; 1 = Mild activity; 2 = Moderate activity; and 3 = Severe activity. The PGA is a validated assessment of clinical disease activity that correlates highly with other disease activity indices (Hyams et al., 1991).
Beliefs About Medication Scale
The BAMS is a 59-item self-report measure of adherence barriers (Riekert and Drotar, 2002). Youth rate their agreement with statements about their illness and treatment regimen using a 7-point Likert-type scale, where higher scores reflect greater agreement. The BAMS includes four subscales: Perceived Threat (PT; e.g. ‘I do not think my illness is a serious illness’), Positive Outcome Expectancy (POE; e.g. ‘If I take my medicine theway the doctors says I should, it helps keep me feeling well’), Negative Outcome Expectancy (NOE; e.g. ‘The side effects of my medicine are so bad that I do not want to take it’), and Intent to Adhere (IA; e.g. ‘I want to take every dose of my medicine the way the doctor says I should’). Lower scores on the NOE and PT subscales reflect fewer adherence barriers. Higher scores on POE and IA subscales reflect fewer adherence barriers.
Medication adherence measure
The medication adherence measure is a semi-structured interview in which respondents report on the number of missed/late doses for each medication over the past week (Zelikovsky and Schast, 2008). We examined self-reported adherence to the IBD medication that was being tracked electronically. Subjective adherence was calculated as follows: (number of prescribed doses – number of doses missed or over 1 hour late)/7. Higher scores reflected higher adherence.
Electronic medication adherence monitoring system
At enrollment, each participant received a MEMS Track Cap and bottle for use with his/her primary daily oral maintenance medication. MEMS Track Caps recorded the date and time of each bottle opening. Devices were returned at the completion of the study and data were analyzed via PowerView® software (Aardex Group Ltd.). Adherence data for the four weeks following baseline assessment (prior to intervention) were utilized in the present study. Objective adherence was calculated as follows: (number of actual openings/number of expected openings during specified period; Riekert and Drotar, 2002). Higher scores reflected higher adherence.
Analytic plan
Descriptive statistics were computed to evaluate distributions. All independent variables were normally distributed. Adherence scores were dichotomized into low-adherence (<80%) or high-adherence (≥80%) groups, replicating methodology used in the development paper (Riekert and Drotar, 2002) and based on data supporting the clinical utility (i.e. differentiating between patient health indicators and hospitalizations) of this dichotomization in patients with chronic illnesses including IBD (Karve et al., 2009; Nahon et al., 2010).
To evaluate aim 1 (i.e. BAMS reliability), internal consistency ratings and mean item-total correlations were examined. Cronbach’s α statistics were considered acceptable if ≥.70 (Tavakol and Dennick, 2011). Test–retest reliability scores were calculated for those in the WLCG. Test–retest reliability coefficients were interpreted as follows: 0 to .2 ‘poor’, .2 to .4 ‘fair’, .4 to .6 ‘moderate’, .6 to .8 ‘substantial’, and .8 to 1.0 ‘almost perfect’ (Landis and Koch, 1977).
To examine aim 2 (i.e. predictive validity of BAMS), 8-point biserial correlations were conducted (four with each adherence indicator). In addition, two logistic regressions were conducted to examine the extent to which subscales together accounted for significant variance in subjective or objective estimates of medication adherence, after accounting for relevant covariates. Consistent with the BAMS development paper, age, race/ethnicity, illness duration, and number of medications prescribed were considered as possible covariates; however, none of these variables demonstrated bivariate associations with r values ≥.30, so regressions were run without any covariates.
Results
Preliminary analyses
See Table 1 for demographic and disease information and Table 2 for BAMS descriptive information.
BAMS subscale descriptive statistics, reliability data, and intercorrelations (N = 76).
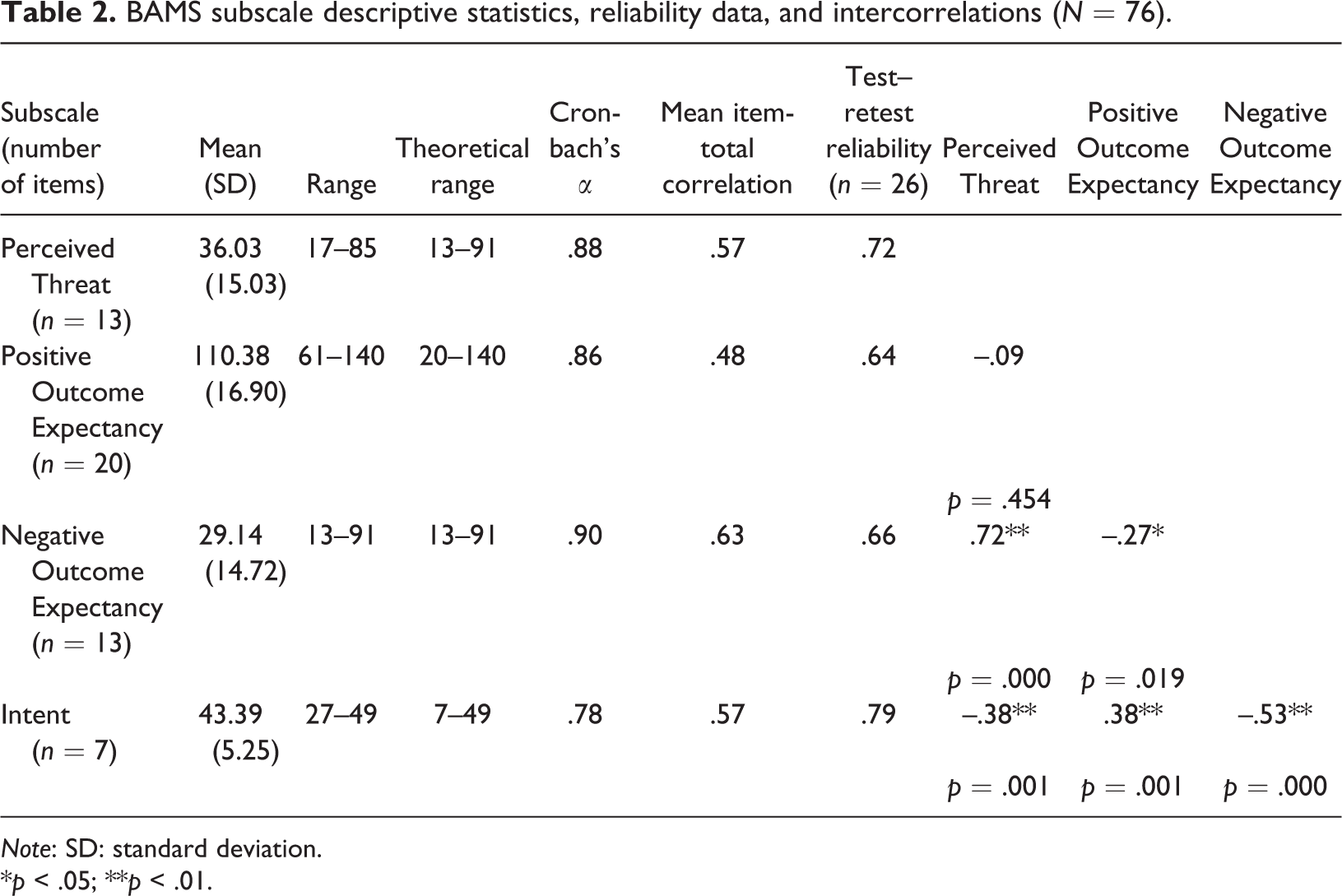
Note: SD: standard deviation.
*p < .05; **p < .01.
BAMS reliability
BAMS internal consistency ratings are presented in Table 2. Cronbach’s αs were all in the acceptable range (αs = .78–.90). Mean item-total correlations were equivalent to medium or large effect sizes (PT r = .57 (large); POE r = .48 (medium), NOE r = .63 (large), and IA r = .57 (large)). Twelve-week test–retest reliability for the WLCG indicated estimates within the substantial range: PT r = .72 (p < .001), POE r = .64 (p < .001), NOE r = .66 (p < .001), and IA r = .79 (p < .001).
Relationships between BAMS subscales and medication adherence estimates
Correlations examined associations between BAMS subscales, demographic and disease variables, and adherence are presented in Table 3. IA was positively correlated with subjective (r pb = .29, p = .01) and objective (r pb = .48, p < .001) adherence. NOE was negatively correlated with objective adherence (r pb = –.27, p = .02). In all three cases, greater endorsement of a given barrier was associated with lower adherence. Neither PT nor POE was associated with adherence.
Correlations between BAMS subscales, demographic and disease variables, and adherence.
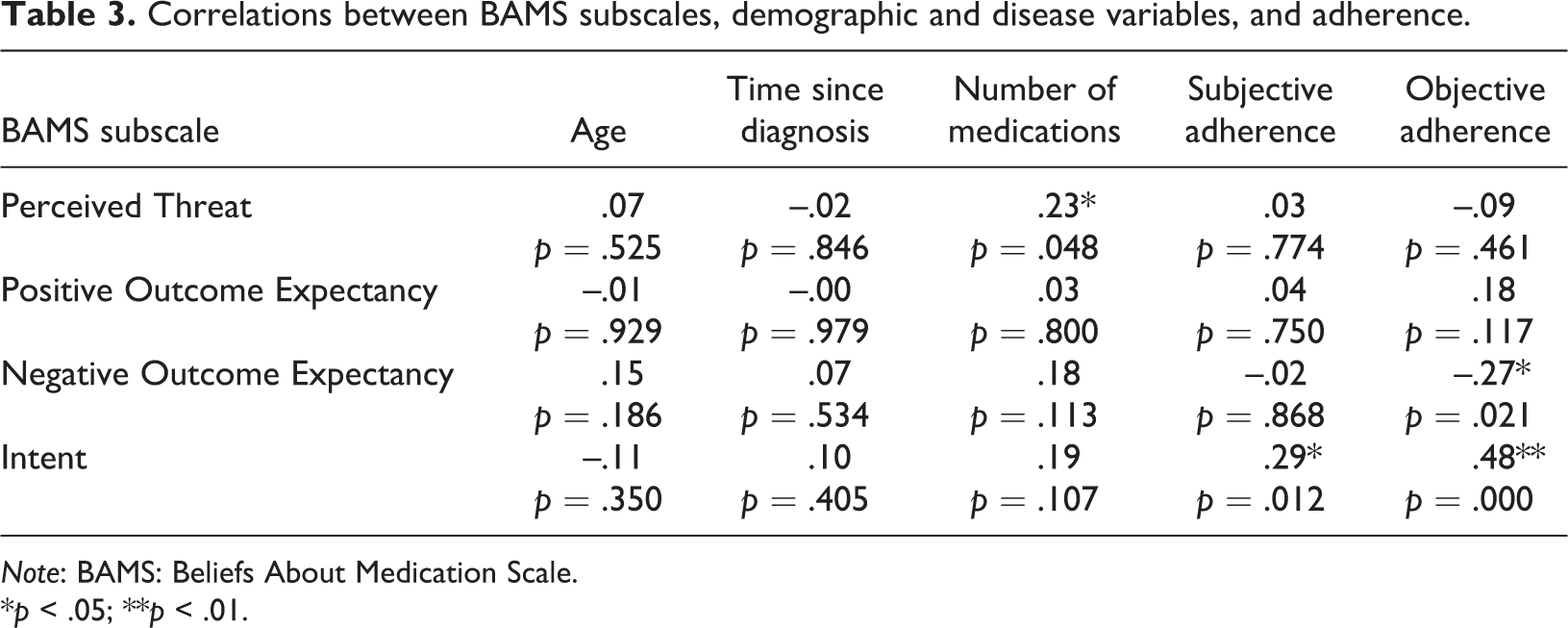
Note: BAMS: Beliefs About Medication Scale.
*p < .05; **p < .01.
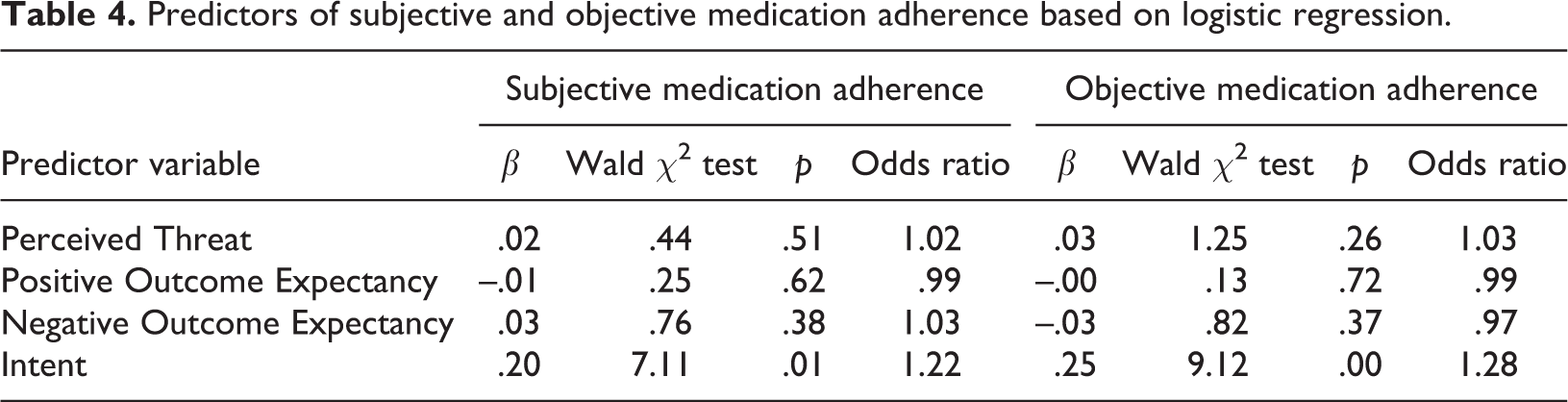
The logistic regression to examine the predictive validity of all BAMS subscales with subjective adherence as the dependent variable indicated that the BAMS subscales together reliably distinguished between the high-adherence and low-adherence groups (χ 2(4) = 9.45, p = .05). However, only IA emerged as a unique predictor of subjective adherence (see Table 4). Youth with greater IA were 1.22 times more likely to be classified into the high-adherence group. Similarly, the logistic regression to examine the predictive validity of all BAMS subscales with objective adherence as the dependent variable indicated that the subscales together reliably distinguished between the high-adherence and low-adherence groups (χ 2(4) = 19.51, p = .001 with df = 4). Again, only IA was a significant predictor of objective adherence (see Table 4). Youth with greater IA were 1.28 times more likely to be classified in the high-adherence group.
Predictors of subjective and objective medication adherence based on logistic regression.
Discussion
This study expanded psychometric support for the BAMS and provided evidence for the clinical utility of IA for adolescents with IBD. Strengths of the study included a focus on a chronic disease group with high risk for low adherence, attention to cognitive adherence barriers, and use of multi-method adherence assessment. Our findings, which were comparable to the findings from the original validation study, provided additional psychometric support for the reliability of the BAMS and its test–retest reliability over a three-month interval. The current results also provided partial support for the predictive validity of the BAMS. Together, all four subscales differentiated between adherence groups, both subjectively and objectively. Since the BAMS is a measure of cognitive barriers to adherence, support for its predictive utility in an adolescent population calls attention to the relevance of this domain of barriers for adolescent patients. The salience of cognitive barriers to adherence in this patient group is consistent with other emerging literature suggesting the relevance of cognitive barriers to adherence for adolescents and young adults (Pai and Ostendorf, 2011), a trend that is consistent with developmental changes including advances in future-oriented thinking and metacognition. In addition, the IA subscale alone differentiated between the high- and low-adherence groups, based on both subjective and objective adherence estimates. Although all BAMS subscales assess illness and medication-related cognitions, the IA subscale includes items that focus specifically on behavioral intention (i.e. one’s intention to take their medication over the next short-term time interval). The finding that behavioral intentions were stronger predictors of adherence than other types of illness or medication beliefs is consistent with health behavior change models, such as the theory of planned behavior, which highlight behavioral intention as the most proximal influence on behavior (Ajzen, 1985). Moreover, these findings also fit broadly within the existing literature which has shown that youth misconceptions about their medications can interfere with adherence (Dawood et al., 2013).
Although the current findings are important, they should be interpreted in the context of several limitations. First, the sample was primarily Caucasian, middle/upper-middle class families, and the majority of participants were in disease remission. Future studies should examine the utility of the BAMS in more socioeconomically diverse samples, since lower socioeconomic status and ethnic minority status are known risk factors for low adherence (Zeber et al., 2011). Moreover, since disease activity may affect motivation to adhere, future research could clarify the utility of the BAMS in predicting adherence among adolescents with higher levels of disease activity. For example, it seems plausible that youth with active disease may perceive a greater threat associated with low adherence or be more motivated to take medications to reduce current symptoms than those with low disease activity. Thus, PT or POE subscales may be more salient predictors of adherence for those with active disease. In addition, recruitment rates were relatively low in the present study, albeit similar to rates of other similar intervention trials (Hommel et al., 2012). The demandingness of the parent study (i.e. a multi-visit intervention trial) may have contributed to low participation rates. Moreover, since recruitment was conducted in an outpatient pediatric clinic, our sample may not be representative of patients who have more difficulty attending regular clinic appointments. Such patient may also have lower rates of medication adherence. Third, although we were able to examine adherence prospectively, our assessment was limited to a one-month interval. Future research examining the predictive validity of the BAMS subscales over a longer time period would be valuable. Given the salience of the IA subscale, future research which examines mechanisms by which behavioral intentions lead to improved adherence behavior and moderators of the link between IA and adherence may also be of value.
The emergence of the IA subscale as a predictor of adherence has important clinical implications. First, efforts focused on enhancing motivation to adhere and/or behavioral contracting to establish short-term goals related to adherence may be of particular value with this group. In addition, the IA subscale may be useful as a stand-alone screening tool in the context of specialty IBD medical care, since it is brief, can be quickly scored, and does not require the presence of a psychologist for administration or interpretation. However, given that all subscales combined contributed more variance to adherence outcomes than the IA subscale alone, administration of the BAMS in its entirety may offer some benefit when a more comprehensive assessment of adherence barriers is possible.
Taken together, findings offer additional support for the utility of the BAMS as a measure of adherence barriers in adolescents with IBD and suggest that the cognitive barriers assessed by the BAMS impact oral medication adherence. Important next steps include documenting that the BAMS predicts longer-term adherence, adherence to other types of IBD therapies (e.g. injection or infusion-based treatments), and key health outcomes. Since promoting adherence during adolescence can lead to improved health outcomes into adulthood (Williams et al., 2002), continued attention to identifying and ameliorating adherence barriers among adolescents with IBD is critical.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the Crohn’s and Colitis Foundation of America (CCFA Senior Research Award #2838; PI: Greenley).