
Abstract
Intimate partner violence (IPV) constitutes a hidden health risk for exposed mothers and children. In Sweden, screening for IPV in healthcare has only been routine during pregnancy, despite an increase in IPV following childbirth. The arguments against routine questions postpartum have concerned a lack of evidence of beneficial effects as well as fear of stigmatizing women or placing abused women at further risk. Increased understanding of women’s attitudes to routine questions may allay these fears. In this study, 198 mothers in 12 child healthcare centres (CHCs) filled in a short questionnaire about their exposure and received information on IPV at a regular baby check-up visit. The mothers’ lifetime prevalence of exposure to IPV was 16%. One hundred and twenty-eight mothers participated in a telephone interview, giving their opinion on the screening experience. The intervention was well-received by most of the mothers who reported that questions and information on IPV are essential for parents, considering the health risks for children, and that the CHC is a natural arena for this. Necessary prerequisites were that questioning be routine to avoid stigmatizing and be offered in privacy without the partner being present.
Introduction
Intimate partner violence (IPV) is a major public health problem and one of the most common causes of injuries in women (Campbell et al., 2002). Worldwide almost one-third (30%) of all women, who have been in a relationship, have been exposed to IPV. Abused women risk increased health problems, such as chronic pain, gynaecological problems, depression, post-traumatic stress disorder, anxiety and sleep disorders (World Health Organization, 2013a).
Although it is frequently assumed to be so, pregnancy is no protection against IPV. Prevalence rates of 3% up to 30% of exposure to IPV during pregnancy have been reported (Garcia-Moreno et al., 2006). IPV during pregnancy is associated with detrimental outcomes for mothers (such as obstetrical complications, depression and substance use) and their infants, including a heightened risk of low birth weight, preterm birth and small for gestational age (Alhusen et al., 2015; Bacchus et al., 2004). In addition, the 12 months following the birth appear to be a period with an increased risk of mothers being exposed to IPV (Bowen et al., 2005; Macy et al., 2007). IPV is thus a continuing health risk not only for the exposed mother but also for her children.
Exposure to parental IPV has been shown to increase the risk of adverse health outcomes for children, such as post-traumatic stress symptoms, depression, anxiety and aggressive behaviour (Chan and Yeung, 2009; Evans et al., 2008). The risk of child abuse in families where the mother is exposed to violence has also been shown to be high (Annerbäck et al., 2012). The high risk of negative outcomes in the developing child makes recognition of IPV an urgent preventive matter for healthcare professionals.
Despite the adverse impact of IPV, women are unlikely to disclose the abuse unless directly asked and healthcare professionals therefore need to routinely ask about exposure to IPV (Dagher et al., 2014). Feder et al. (2006) have shown that women who have been exposed to IPV are largely consistent across studies in their support of routine enquiries, as long as the healthcare professionals are compassionate, supportive and respectful and demonstrate in-depth knowledge of IPV. However, routine IPV enquiry has been questioned (MacMillan et al, 2009). Currently, the WHO (2013b) recommends screening for IPV during pregnancy but not postpartum. The arguments against routine questions postpartum concern a lack of evidence of beneficial effects as well as child healthcare nurses’ reluctance, resulting from fears of stigmatizing women or increasing the risk for the abused women (Elliot et al., 2002). The discussion has focused on risks and benefits for the mothers and not for the children (O’Doherty et al., 2015). However, postnatal screening for IPV within healthcare has been implemented in some countries, such as Australia (Hooker et al., 2016). In Sweden, the Swedish National Board of Health and Welfare (Socialstyrelsen, 2014) recommends that all women seeking maternal healthcare be asked about exposure to IPV, but routine questions about IPV postpartum have so far not been recommended. In Sweden, 99% of children aged zero to five years attend a child healthcare centre (CHC) with their parents, mostly their mothers (Blennow and Sundelin, 2014). The CHC offers a promising arena for recognizing IPV, since its role is to promote children’s health by informing parents about health risks to children and ways for parents to avoid these risks. Child healthcare nurses in Sweden are educated in and accustomed to asking and informing women on sensitive matters, such as smoking, the use/abuse of alcohol and signs of depression. In spite of this, the risk of stigmatizing women has been described as a barrier to asking about IPV, in Sweden as well as elsewhere (Feder et al., 2009). Increased knowledge of women’s attitudes to routine questions about IPV when visiting a CHC may help allay these fears and overcome this barrier.
The primary aim of this study was to explore mothers’ experiences of and thoughts on being asked about exposure to IPV at a CHC. A second aim was to investigate the prevalence of exposure to IPV among the mothers.
Methods
Study design
A mixed-method study design was used to explore the prevalence of IPV and attitudes to routine screening among postnatal women attending 12 CHCs. The prevalence of exposure to IPV was calculated from questionnaires completed by the mothers at the CHC. The mothers’ opinions on the screening intervention, given in a semi-structured telephone interview following their CHC visit, were documented in a prepared fill-in form and then analysed.
Setting and participants
The nurses at all 59 CHCs in two counties in Sweden were invited to participate in the study. Thirteen child healthcare nurses from 12 clinics, 6 in each county, volunteered. The 12 clinics represented the demographic spread in the counties, being situated in both major cities and rural areas and in low- as well as high-income neighbourhoods. The clinics varied in size, with the number of newborns in year 2014 ranging from 35 to 362 and the total number of enrolled children (aged zero to five years) ranging from 189 to 2065.
During the inclusion period (July 2014 to May 2015), 338 babies were born in the participating nurses’ geographical area, with boys and girls being equally distributed. The mothers were predominantly of Swedish origin (86%), with 4% of European and 10% of non-European origin. Most of the babies lived with both biological parents (95%), and most parents had joint custody (97%). For 39% of the mothers, the baby was her first child.
Swedish CHCs offer all children aged zero to five years and their parents regular health controls, with health-promoting information and vaccinations, in about 16 visits. During the inclusion period, 221 (72%) of the 338 eligible mothers attending a CHC for the five- to six-month baby check-up were informed about and invited to participate in the study by their nurse. Only 9% of mothers who were informed declined, and 90% (198) of the mothers who initially consented to participate were finally included. Of the 198 mothers who took part in the screening part of the study, 65% (128) accepted and took part in the telephone interview one week later. No significant differences regarding parental origin, gender of child or custody were found between the study sample (198) and the population, but no mothers in need of an interpreter took part in the telephone interviews (128) even though the support of an interpreter had been offered. The Regional Ethical Review Board in Uppsala, Sweden, approved the study (2014/463).
The intervention
The project was initiated by the participating healthcare organizations and supported on all organizational levels. As part of the study, the nurses participated in a training programme on IPV and its effects on exposed women and children, with lectures (12 hours) and workshops (5 × 2 hours) led by child healthcare psychologists. A detailed plan set out how the nurses were to act if they recognized an exposed mother. The child healthcare psychologists within the geographical area took part in the training so that they would be able to give appropriate support.
During the eight-month check-up, the mothers were asked to fill in a short questionnaire (the Violence in the Family (ViF) questionnaire) comprising four questions about exposure to IPV. If the mothers had been exposed to violence, they were asked to fill in an additional questionnaire (the Conflict Tactics Scale – Brief [CTS-B]) to further map their exposure. The nurses responded to questions and reactions by the mothers. The mothers’ partners were not present.
Instruments
The ViF questionnaire
The ViF is a self-report questionnaire consisting of four questions regarding the occurrence of violence in current and former partner relationships; it was developed from the partner violence screening instrument (Feldhaus et al., 1997). The questions are as follows: (1) Have you (as an adult) been hit, kicked, punched or otherwise hurt by someone? If so, by whom? (2) Have you (as an adult) been ridiculed, threatened, harassed or otherwise hurt by someone? If so, by whom? (3) Do you feel safe in your current relationship? and (4) Is there a partner from a previous relationship who is making you feel unsafe now? The ViF, which takes one to two minutes to complete, has been shown to be easily administered and well-accepted (Broberg et al., 2015).
The CTS-B
The CTS-B questionnaire is a short version of the Revised Conflict Tactics Scales (CTS2; Strauss et al., 1996). The CTS-B comprises 10 statements that assess the types of violence, including physical, psychological and sexual abuse.
The telephone interview
The semi-structured telephone interview format consisted of 17 questions, 8 of them open questions, such as how the mothers perceived being asked about IPV at the CHC, what their views were on the importance of being asked and whether anything was positive or negative about being asked. Seven questions required a yes or no answer and were followed by open probes – such as ‘why/why not?’ – to encourage the mothers to say more about their views. These questions concerned the presence of a partner when talking about IPV, the suitability of the questionnaires, the best time to ask and the quality of the alliance between the mother and her nurse, as well as what the nurses need to consider when asking questions about IPV and if there was anything they had missed out in the intervention. Two questions entailed a visual analogue scale: mothers were instructed to rate their experience on a 10-point scale with the end points defined as extreme values, followed by open probes inviting the mothers to explain their stance. The interviews lasted for 15–20 minutes, and the interviewer (third author P.A.) documented the answers on a prepared fill-in form.
Data analysis
For statistical analysis of the questionnaire data on IPV prevalence (from the ViF and CTS-B questionnaires), and the created numerical categories for the telephone interview data, IBM SPSS Statistics V22.0 software was used (IBM Corp., 2013). Thematic analysis of the women’s open question interview responses was undertaken, informed by the work of Braun and Clarke (2006). Each interview was read several times by the first and third authors separately for their interpretation of the mothers’ explanations and descriptions. The analysis was guided by the aim of describing both the dominant opinions and the variance on each question.
Results
Prevalence of IPV
In response to the question ‘Have you been hit, kicked, punched or otherwise hurt by someone?’ on the ViF questionnaire, 32 (16%) of the 198 mothers stated that they had been exposed to violence from an intimate partner. In 27 cases (13%), the violence was in the past (greater than three years), while 5 mothers (2.5%) had been exposed more recently (one to three years) and 1 mother (.5%) in the past year. The second questionnaire (CTS-B) administered to those mothers who had answered that they had been exposed to IPV revealed that psychological violence was most frequently reported (30 mothers, or 15%). Twenty-one mothers (10.5%) had been physically abused and the other nine mothers (4%) had been sexually abused. All mothers but three reported being abused by a former partner, not the biological father of their newborn child. One mother described feeling unsafe with her child’s father, and two mothers were still fearful of their former partner.
The mothers’ attitudes to the screening intervention
Most of the 128 interviewed mothers (71%) appreciated being asked about exposure to IPV by their child healthcare nurse and described their experience as very positive or positive. Twenty-four percent of the mothers described the experience as neutral, while 5% were doubtful, although not entirely negative.
The mothers who were positive about being asked described it as relevant and natural to bring up IPV in the CHC and reported that they felt safe to talk about IPV there. ‘I think it’s great to bring this up at CHC, it’s important. Some people don’t realize that they are living in a violent relationship before they get children’. The mothers saw it as important that mothers who are exposed to IPV are recognized, and they appreciated that their nurse cared about such matters. They stressed the value of all mothers being given information on the negative impact of IPV on children’s well-being and development and on how to receive help, as this is not common knowledge. The mothers compared this information with what they had been told about other risks of children’s health and development, and they stated that they considered the IPV information to be equally important; ‘Questions about violence need to be asked – the best of the child has to be the primary consideration’. According to the mothers, providing this information could increase the likelihood of an exposed mother eventually talking about her situation. The interviewed mothers (n = 128) deemed the risk of a mother no longer visiting a clinic because of being asked about IPV as low (M = 7.47, SD = 1.76, n = 127, on a 10-point scale, with 1 = extremely high risk and 10 = no risk at all).
Some of the mothers who were doubtful explained that it was somewhat depressing to be reminded that some children are put at risk by violent parents, and some were unused to being questioned about such private matters. When probed, 93% of the mothers stated that nothing in the screening intervention was intimidating, while 7% described initial feelings of being negatively judged or viewed with suspicion.
The majority of the interviewed mothers thought that it was essential (M = 9.2, SD = 1.59, on a 10-point rating scale with 1 = not at all and 10 = absolute necessary) to ask about IPV in CHC. ‘Who else could ask? The CHC is important. It concerns the young children’. About 70% of the mothers reported they had never been questioned about exposure to violence before, while 30% had been asked by their midwife during pregnancy. The women varied in their opinions concerning the best way to design a screening procedure (see Table 1).
Women’s opinions concerning the best way to do screening for IPV at CHC (n = 127).
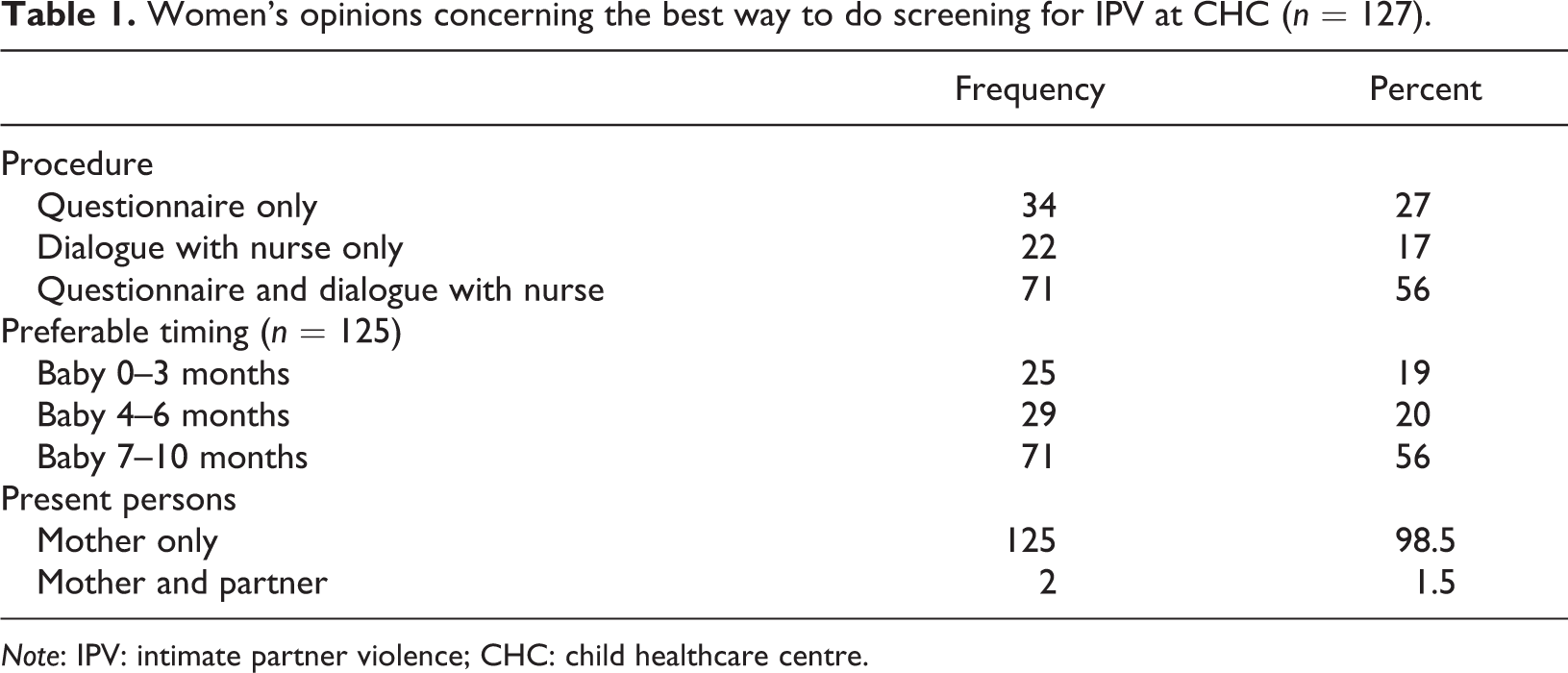
Note: IPV: intimate partner violence; CHC: child healthcare centre.
The majority (90%) favoured the ViF questionnaire, which they described as easy to understand and requiring a reasonable expenditure of time. The CTS-B questionnaire, which was only given to mothers who had indicated exposure to IPV on the ViF questionnaire, was not much appreciated. Only 23% of the 32 answering mothers were positive about the instrument, with the rest of the mothers describing it as unclear and hard to understand.
Some of the mothers who preferred being asked when the infant was younger explained that the conversation on postnatal depression symptoms when the baby is approximately two months old was a time when they were alone with the nurse and thus would be a good opportunity to be asked about IPV. Mothers who preferred being asked later, on the other hand, emphasized that having a new baby is a major change in a woman’s life and eventually she will build a closer alliance with her nurse. Nearly all of the mothers agreed that mothers would need to be questioned about exposure to IPV when seeing the nurse on their own. Otherwise, it would be impossible for them to tell the truth. Several mothers suggested, however, that fathers would also need to be asked about IPV, since men too can be exposed, and stated that fathers also need information on the impact of violence on children’s health and development.
According to the mothers, a prerequisite for introducing questions about IPV in the CHC is that it is done routinely, to avoid any stigmatizing. Nurses also need to be well informed about IPV and capable of handling a situation with an exposed mother who has revealed her situation. The mothers described the need for nurses to be empathetic and humble. Two additional requirements were seclusion and sufficient time. Suggestions for improving the screening intervention included giving mothers more information on IPV, especially on how the violence risks affect children negatively, what the legislation is and where to receive support and protection.
Discussion
This study aimed to explore women’s’ experiences of being asked about exposure to IPV when visiting their CHC. A second aim was to investigate the prevalence of exposure to IPV among the women.
While only a few mothers reported IPV in their current relationship, their reported lifetime exposure to IPV (16%) is close to previously shown prevalence of lifetime exposure in Sweden (14%) (Andersson et al., 2015). Reported lifetime prevalence of IPV seems to be lower in Sweden compared with global prevalence (30%) (WHO, 2013a; Black et al., 2011), and women seem to be more prone to reveal exposure to IPV when asked by healthcare professionals compared with international studies, which overall reports low rates relative to best estimates of prevalence of IPV in women seeking healthcare (O’Doherty et al., 2015).
Most of the mothers were positive about being questioned about IPV by the child healthcare nurse and even described bringing up the topic in the CHC as necessary. In general, the mothers felt cared for by the nurse when she asked about IPV, contradicting the opinion that women would feel intimidated by routine questions about IPV (Elliot et al., 2002; Hultmann et al., 2013). By interviewing all mothers at the CHC, we believe that our results broaden the knowledge concerning women’s experiences of talking about IPV with healthcare professionals. As an example, to the list of recommendations developed by Feder et al. (2006) on the basis of a research review, we might add that mothers stress the importance of being alone when asked about IPV and that asking should be done routinely with all mothers to avoid potential stigmatizing. The risk of stigmatizing was described as negligible, if it was a routine screening procedure. The mothers’ opinions challenge the view and recommendations that only at-risk populations should be asked about IPV (O’Doherty et al., 2015) and are similar to the previous findings in Swedish antenatal care research (Stenson et al., 2001). The mothers in this study emphasized that by asking about IPV, the nurse makes a sensitive topic speakable, thus increasing the possibility of an exposed mother reporting on her situation in the future.
The results indicate that routine questions about IPV in healthcare settings are appreciated by most women. A small minority of the women in this study were reluctant, although not entirely negative, and no negative effects were described. This finding is in line with previous research (Taft et al., 2015). However, a substantial number of the women declined to be interviewed by telephone. The reason for this is unknown. It may be that women living with ongoing exposure consider that being asked about IPV constitutes a risk. In a Canadian randomised controlled study study of screening for IPV in healthcare, the individuals who were lost to follow-up reported higher scores than the individuals who remained in the study (MacMillan et al., 2009). More research into the effects of routine questions in the healthcare environment is thus needed.
A short self-completion questionnaire for recognition of exposure followed by a dialogue between mother and nurse seems to be a suitable procedure for use in child healthcare, which also has been shown elsewhere (Taft et al., 2015). The ViF questionnaire appears to meet the demand for acceptability in this setting (Broberg et al., 2015).
In this study, the involved child healthcare nurses were offered study-specific training and consultation, and the intervention was supported by the healthcare organization. The implementation of routine questions about IPV needs to be decided on by the healthcare organization in order to secure sufficient support for the nurses; otherwise, the sustainability of the routine appears to be low (Garcia-Moreno et al., 2014).
Despite the established Swedish national guidelines on IPV screening within maternity care, only a small number of the mothers recalled being asked about IPV before. This finding raises questions about the implementation of the routine and the need for more evaluation. National guidelines and the implementation of routine questions about IPV also need to be complemented by a sustainable system of support for and training of the child healthcare nurses. Otherwise the routines appear to deteriorate as a result of a range of barriers, such as the perceived risks for mothers as well as others (Elliot et al., 2002; Garcia-Moreno et al., 2014). IPV is still perceived as shameful, and nurses and midwifes may be reluctant to bring up the topic (Dowd et al., 2002). However, the findings from this study indicate that potential barriers among mothers appear to constitute a minor problem. Individual clinician and healthcare system barriers to asking about violence, as described by others (Hooker et al., 2016), seem to be more of a challenge in addressing the health and safety of abused women and children.
Study limitation
This study has some benefits, as its natural design being integrated into the regular child healthcare service, and from the use of individual interviews, giving women space to express their own thoughts and feelings. However, a severe limitation with the study was that only 65% of the study sample took part in the telephone interview, and no woman required an interpreter. The representativeness of the study is therefore limited to Swedish-speaking mothers.
Conclusion and clinical implications
Routine questions about exposure to IPV are well-accepted by most mothers attending Swedish CHCs but offering a private visit without the partner present is a prerequisite. Information on the risks of IPV for children’s well-being and development was asked for by the mothers in this study and was deemed important for both parents. Routine questions about IPV in child healthcare thus need to be complemented with information on the consequences of IPV on children’s health and neurological development. This demands specific knowledge of the child healthcare nurses and may contribute to their motivation to bring up a sensitive topic. The use of a brief self-completion form followed by a dialogue with the child healthcare nurse seems to be a suitable procedure. This study indicates that the use of routine questions about IPV in CHCs should be further evaluated, as the evidence for universal screening in healthcare settings is still regarded as insufficient (MacMillan et al., 2009; O’Doherty et al., 2015).
Footnotes
Acknowledgements
We thank the participating child healthcare nurses and especially the two head nurses of the child healthcare in the two counties and Christina Gillå and Maria Lind, who made this study possible. We thank the child psychologists who were responsible for developing and conducting the training programme on IPV for nurses in the CHC. We also thank all the mothers for their contributions.
Declaration of Conflicting Interests
The author(s) declared no potential conflict of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was supported by Karlstad University, the County Council of Värmland, and the County Council of Örebro län.