
Abstract
The treatment regimen for children with cystic fibrosis (CF) is vast and is usually undertaken in the family home. Managing CF coincides with other important family routines such as children’s participation in education. There is a dearth of research that considers family routines that may influence, and be influenced by how CF is managed. To address this gap, this patient-led study examined how families manage CF alongside children’s education in England. Semi-structured interviews were conducted with 14 participants comprising 5 children and young people with CF, 4 parents, 2 CF nurse specialists and 3 teachers. The results revealed that CF routines were organized to minimize disruption to education, although families experienced challenges in meeting all daily health and education demands. Families chose between children doing their treatments or participating in school activities when doing both were not feasible. Treatments were sometimes a barrier to education participation and children’s learning. Families found treatment routines restrictive upon children’s friendships. Education is a priority for families, which affects how they manage CF. CF clinical teams should consider bidirectional influences between important family routines and families’ management of CF, when planning appropriate treatment regimens.
Introduction
In the United Kingdom (UK), cystic fibrosis (CF) affects over 10,000 people, and approximately 3000 are of school age (CF Trust, 2016). CF has evolved from an illness where children died in their teens to one with a life expectancy well into adulthood (Havermans and De Boeck, 2007). The increase in survival is due to developments in treatments and management of CF (Castellani et al., 2018). Most treatments can take place at home, allowing families to self-manage the condition. Treatments typically entail chest physiotherapy, nebulized and inhaled drugs, medication, high-calorie vitamin-supplemented meals and exercise. The burden of regular daily treatments is compounded by the need for intensive intravenous (IV) antibiotics during chest exacerbations, which can also be administered at home. While it is a remarkable achievement to integrate CF care and treatment into the home environment (Havermans and De Boeck, 2007), a drawback is that managing CF at home is incredibly demanding for families. Parents now provide support with care that was previously given by health professionals (McGuffie et al., 2008). Treatment is time-consuming, tiring and intrudes into family routines and families must manage treatments while continuing to meet daily life demands (Foster et al., 2001). Research has investigated families’ management of CF in terms of caring time requirements upon parents (McCann et al., 2012); family support (Coyne, 1997); parent coping (Wong and Heriot, 2008); and the quality of life of children with CF, siblings and parents (Besier and Goldbeck, 2012; Hegarty et al., 2009). However, there is a dearth of research that considers the influence of other important family routines upon how CF is managed.
Managing CF alongside other significant family routines
For families of school-aged children with CF, a significant proportion of time is dedicated to activities connected to education. The complexities of managing the huge treatment regimen, therefore, coexist with other important family aims and routines (Besier and Goldbeck, 2012). When CF is stable, most care and treatment can be administered before and after school, to allow children to attend as usual with their peers and reduce disruption to school life (Foster et al., 2001; Havermans and De Boeck, 2007; Puckey et al., 2006). Children value health professionals’ efforts to organize treatments around school hours to maintain their sense of normality at school (Lightfoot et al., 1999; Taylor et al., 2008; Yates et al., 2010). Arranging treatments before and after school introduces added time pressures for families, which may influence treatment non-adherence. Yet the routine and structure inherent to school days may be beneficial to managing CF, as one study from England found adherence to nebulized therapies is better on weekdays during school term time than at weekends or school holidays (Ball et al., 2013).
Enabling children to have treatments at school may reduce the burden upon families when managing treatment routines. However, research from the UK suggests that there is limited school-based health support for children with chronic illness due to issues of training, funding, teacher liability and staff knowledge and confidence in meeting specific health needs (Hewitt-Taylor, 2009; Hinton and Kirk, 2014; Leyland et al., 2016; Lightfoot et al., 1999). Further, parents may experience anxiety when handing care over to other adults at school (Puckey et al., 2006). These issues call into question the feasibility of administering CF treatments in the school setting.
The importance of education for children with CF
Given the ageing population of individuals with CF, achievement in education is crucial if those with the condition are to gain financial independence through employment. Indeed, research in the United States and France has shown a significant predictor of employment in adults with CF is educational attainment rather than disease severity or disability (Burker et al., 2004; Laborde-Castérot et al., 2012). However, it is not known what affect following a huge treatment regimen has upon the educational outcomes of children with CF. Children with chronic illness do experience worse school outcomes when compared to their peers, which has been attributed to increased school absence causing children to fall behind, and a lack of focused support from schools in both the English and Australian context (Asprey and Nash, 2006; Bailey and Barton, 1999; Lightfoot et al., 1999; Yates et al., 2010). The social aspects of school are particularly important for children with chronic illness, as they are more likely to experience disconnected peer relationships (Bolton, 1997; Lightfoot et al., 1999; Yates et al., 2010). As Closs (2000) suggests, the time available to establish intimate friendships is limited for children who follow medical treatment regimens. These issues highlight the importance of education to children with CF. Family routines associated with children’s schooling may therefore influence the way that families manage the condition.
Bidirectional interactions between managing CF and children’s schooling
The relationship between managing CF and children’s schooling is bidirectional and interactional. Therefore, it follows that both these important aspects of family life influence each other. There is a need to recognize interconnected and interactional factors that shape how families mange the considerable CF treatment regimen. A key framework that takes into account of these factors is the biopsychosocial model, which is fundamentally ecological and holistic, making it capable of capturing the complexities of family experiences (Engel, 1982). The model is used in this article to explore interactions between biological or health factors related to CF, the school and home environment and social and emotional factors at play in children and families’ lives. Identifying the biopsychosocial influences involved in the management of CF is critical to understanding how families cope with negotiating daily health and education obligations and to provide effective family support (Hegarty et al., 2009; Hinton and Kirk, 2014; Rosland and Piette, 2010).
This article is drawn from a broader study that explored the educational experiences of children with CF. Two major study aims are considered here. The first aim is to examine how families manage CF alongside children’s schooling from an ecological and interactional perspective. The second aim is to consider the possible implications for the care and education of children with CF, in the light of the interactions between families’ management of CF and children’s schooling. The research was conducted by the author who herself is an adult with CF.
Methods
Sample
The sampling approach was taken in respect of the interconnections between health and education, to explore the influence of the interactions between families’ management of CF and children’s schooling. School-aged children from a large regional paediatric CF centre in England volunteered to be interviewed along with their parents, following children’s completion of an earlier questionnaire. All children and parents approached for the research agreed to take part. My position as an adult with CF created a sense of ‘connectedness' with children and parents, which appeared to be a motivating factor in their decision to participate. A purposive sample of children who had undergone home IV antibiotics, had been in hospital or had not experienced either of these in a period of 12 months prior, was selected to take into account of varying treatment regimens and the heterogeneity of children with CF. Since young people who have left school more readily discuss their medical condition and education, having less fear of negative issues being passed on (Cavet, 2000; Yates et al., 2010), a post-school-aged young person from the regional CF centre was also identified. Children and parents were asked to nominate an education professional who could be invited to participate, although one child asked not to involve the school in the research. CF nurse specialists from the regional centre connected to the children and young people were approached for their participation. The sampling approach enabled the ‘multiple truths’ about how families manage CF to be examined (Denzin and Lincoln, 2017).
Interviews
Semi-structured interviews were conducted once with all participants to allow in-depth discussion of their experiences and further questioning of research-related issues. Creating the constructs that informed the interview schedules was an iterative process. First, themes and issues within relevant literature were established. Overlaps and repetitions were collapsed into individual areas of concern and gaps were identified, to produce an initial list of constructs and interview questions. Second, an ‘expert group’ including qualitative researchers, health professionals and members of the CF community were consulted about the suitability of the constructs and interview questions. No subsequent changes were made to the constructs that are the focus of this article. Two key constructs were used to examine bidirectional influences involved with managing CF alongside children’s schooling, namely, (1) CF routines and treatments (e.g. impact on school activities, differences on school days, difficulties encountered) and (2) significant school activities (e.g. impact on CF routines, children’s participation, exclusion, restrictions). The schedules for all participants were based on the same overriding constructs.
Online interviews took place with children and young people to avoid cross-infection between the researcher and this group of participants. Photovoice, vignettes and fantasy wish questions (Asprey and Nash, 2006; France et al., 2000; Hazel, 1995) were used to promote discussion and maintain interest and engagement throughout the online interviews. Face-to-face interviews were conducted with parents and professionals where possible. However, some parents and professionals opted for telephone interviews, either to suit their busy work schedules or because no cross-infection free interview space was available. With participant consent, interviews were recorded and transcribed. Transcriptions were shared with participants and their amendments and further comments were invited.
Data analysis
Analysis of the interview transcripts combined elements of grounded theory (Glaser and Strauss, 1967) and thematic analysis (Braun and Clarke, 2006; Saldaña, 2013). The respective approaches were chosen to provide the flexibility needed for a priori and a posteriori coding of the data set and to facilitate a systematic approach for identifying, analyzing and reporting patterns and themes (Braun and Clarke, 2006; Saldaña, 2013). First, familiarization took place whereby transcripts were read repeatedly. Transcript data were subsequently broken down into segments of text and given a code name. Then, several iterations of code mapping (Saldaña, 2013) were undertaken, involving sorting and comparing codes to look for replications and to determine codes that grouped together. At this point, some codes were discarded and others formed themes. Next, themes came together under superordinate themes where they captured something important about the data and were related in meaning to other themes. Five superordinate themes were consistent throughout the data analysis and are the focus of this article. Themes were independently checked across a sample of the data set and no subsequent changes were made.
Ethical considerations
Ethical approval was granted by the Yorkshire and the Humber – Leeds Bradford Research Ethics Committee (13/YH/0342). Research and development approval was given by the local NHS Trust. Informed written consent was gained from all participants. Children and young people provided their own consent/assent and were not expected to take part if they did not want to. The right not to participate and withdraw from the research was reaffirmed at the start of each interview. It was explained that pseudonyms would be used in research outputs to protect anonymity.
Results
Fourteen participants were interviewed for the research, comprising five children and young people with CF aged between 9 and 17 years (3 male, 2 female), 4 of their parents (all mothers), 2 CF nurse specialists and 3 of the children’s teachers. Characteristics of the children who took part, along with the parents and professionals connected to them, can be found in Table 1.
Characteristics of children, connected parents and professionals.
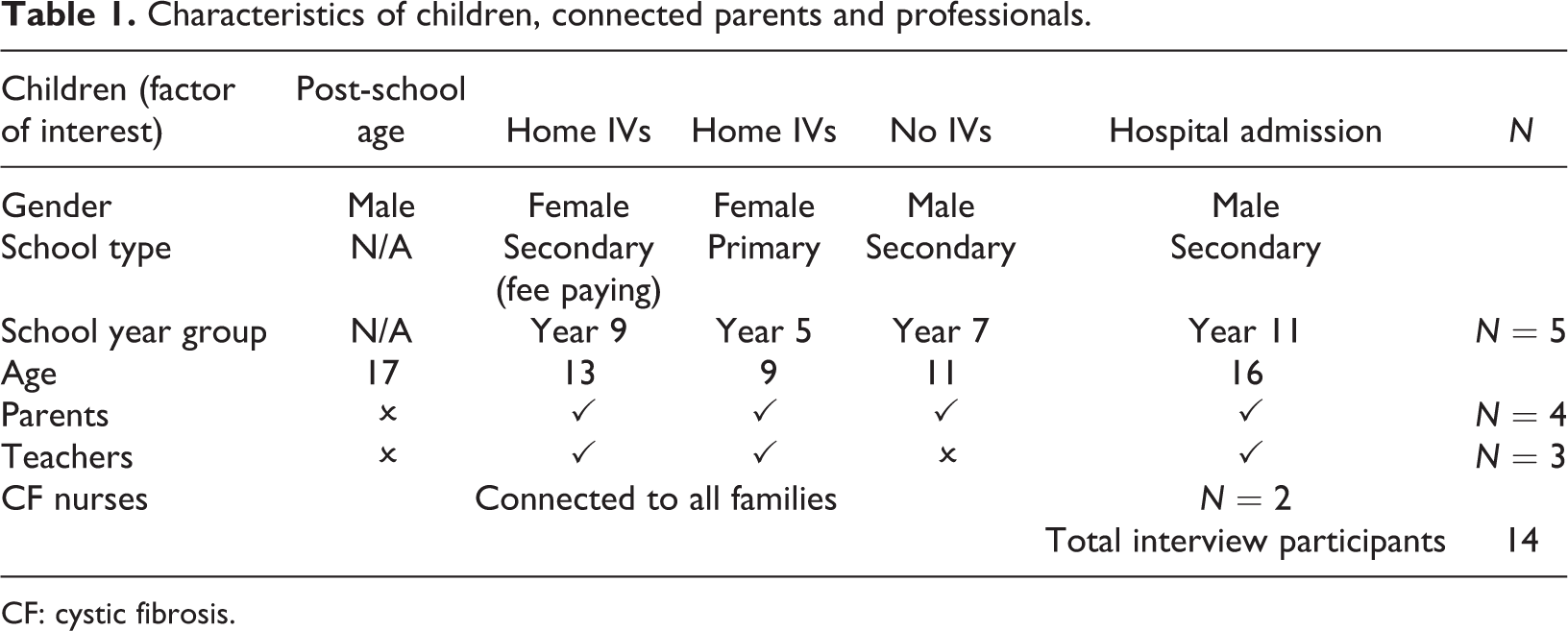
CF: cystic fibrosis.
Five themes are now presented that exemplify the interactions between families’ management of CF and children’s schooling. The first theme, ‘school day health routines’, describes families’ management of CF specific to school days. The second theme, ‘fitting everything in’, describes family challenges in meeting daily health and education obligations. The third theme, ‘treatment dilemmas’, relates to family choices and priorities around managing CF and children’s schooling. The fourth theme, ‘exclusion from school activities’, describes how treatments can be a barrier to education participation. The fifth and final theme, ‘the importance of friendships’, illustrates the implications of treatment routines upon children’s school friendships and social lives.
School day health routines
Parents, children and CF nurse specialists consistently reported they purposely arranged treatments to fit around the school day, demonstrating a commitment to minimizing education disruption. Treatment routines were more relaxed for families during school holidays and at weekends: I do everything (treatments) in the morning when I’m at school, but on holiday I just do them any time. (Rachel, 13-year-old girl) We consider education to be really important, so anything that needs to be done we get done before and after school. We try to get children on twice daily Flucloxacilin (antibiotic) when they start school so they don’t have to have them through the day. On the whole we try to keep them as normal as possible. (Joanne, CF Nurse Specialist) Sometimes she’ll do her PEP mask in the car on the way to school. We always make a joke that girls multi-task better than boys. She was doing her iNeb (nebuliser) whilst she was drying her hair last night. (Alice, parent of 9-year-old girl) Either she hides it very well, or it (CF) doesn’t (affect her) because she participates along with her peers in exactly the same way. She doesn’t seem to have any issues through the lessons and if she does she doesn’t make me aware of them. (Jackie, teacher of 13-year-old girl)
Fitting everything in
Parents and children explained they get up much earlier in order to complete treatments in time for the school day. Some found this to be difficult, particularly when children were in receipt of additional medications for chest infections: My Cipro (antibiotic) prevents me from having milk at different times. So if I want milk on a morning for my breakfast, I have to wake up at 5 am to have my Cipro first and then go back to sleep. And it’s been like that for a month now. (Joe, 11-year-old boy) It’s more a time management thing trying to get everything done. His Ambisone (antifungal), that’s quite a long time. About twenty minutes that took (to nebulise) and then trying to do his physio after that. Mornings are the worst. We’ve all the time in the world after school. And because we do home IVs quite often, he can’t get to school on time otherwise we’d be getting up at five in the morning. (Nikki, parent of 16-year-old boy) They get nine hours of homework a fortnight, which I think is quite a lot. If you’ve got other things as well, like when he comes home from school he’ll have two nebulisers, he’ll have his medicines, his pep mask or whatever activity we do for physio, and then meal times. When you’ve got to start sitting down and doing homework, I think sometimes he does find it hard to keep up with. (Louise, parent of 11-year-old boy)
Treatment dilemmas
Parents and children described managing CF alongside education as a delicate balancing act. Dilemmas were experienced where parents choose between children doing treatments or attending school as usual, and sometimes doing both were unworkable. When new or additional treatments were introduced, some parents negotiated alternative treatment options to protect children’s participation in education, indicating a need for flexibility from the CF team: They would like him to do another nebuliser before school and we’ve kind of talked our way out of it. It isn’t feasible because of the time thing again. So, ideally he would do one before school, one mid-afternoon, then one when he got home. But we want to make it achievable and don’t want him to start dropping out of doing things. (Nikki, parent of 16-year-old boy) The last time he had IVs he wanted to go to school, but he was on them three times a day. I think if they were just twice a day we’d get him to school. I just know how I feel when I do IVs. I wouldn’t want to give that responsibility to anyone else. Then you’ve got to think he’d have to take his anaphylaxis stuff to school and would they be capable of doing that? It’s a big responsibility to give to somebody else. I think I would prefer to do them at home. (Louise, parent of 11-year-old boy) The school nurse is the first port of call for anything medical really. (Teacher of 9-year-old girl)
Exclusion from school activities
Despite best efforts to manage CF and minimize disruption to education, some treatments negatively impacted children’s participation in school activities. The impact on participation was more pronounced when activities deviated from the typical school routine or when children were in receipt of intensive treatments. IV therapy was sometimes a barrier to children’s participation in physical education (PE): Because my arm is wrapped up in a bandage and because I really like gymnastics, I can’t really do that. So I have to chat or do something else that doesn’t involve hurting my arm in the playground. (Violet, 9-year-old girl) The school trip to the Lakes, he is absolutely adamant he’s not going. I think he’s quite worried about being able to do his medicines, and also he probably wouldn’t eat what they gave him. He won’t take tablets. He’s still on liquid so that would make it harder as well. It would be drawing it up and keeping it in the fridge. I can understand why he doesn’t want to go because it will make him a bit different won’t it? (Louise, parent of 11-year-old boy)
The importance of friendships
The management of CF was influenced by school friendships. Some parents arranged clinic appointments during school holidays to reduce children’s time away from their peer group. Participants recognized the restrictions imposed by treatments upon social activities that allow children to maintain their friendships. The CF nurse specialists explained that during adolescence, the importance of socializing with friends frequently causes young people with CF to rebel and withhold treatment. Indeed, one young person appeared to experience a dilemma between completing his treatments and being with his friends: I mean, sometimes I’m bothered (about doing treatments) because I don’t get to see my friends. But then the other way, I know it’s going to help me with my health. (Joe, 11-year-old boy)
Discussion
The reported themes exemplify the holistic view of schooling held by families through their descriptions of varied activities making up children’s participation in education. Families encountered challenges when negotiating health and educational demands. Organizing treatments around school hours did not always reduce disruption to education as research from England and Belgium has claimed (Foster et al., 2001; Havermans and De Boeck, 2007; Puckey et al., 2006). Time undergoing treatments diminished time for children’s home learning. Therefore, CF treatments may moderate learning opportunities and disadvantage children in education, which further explains the poorer school outcomes of children with chronic illness (Asprey and Nash, 2006; Bailey and Barton, 1999; Lightfoot et al., 1999; Yates et al., 2010).
This study also demonstrated children experience exclusion from activities such as PE and school trips due to aspects of their treatment regime. Exclusion from PE was heightened during IV therapy when IV access needed to be protected from harm. The deviation from the typical school day associated with school trips disrupted the balance involved with managing CF alongside education, presenting barriers to children’s participation, especially when trips involved overnight stays. Barriers may be removed if parents accompany children on school trips, although this may be more practical for parents of primary children. Families may therefore encounter challenges when changes to the typical school day occur through unusual activities, when additional treatments are introduced into the routine or indeed if these circumstances transpire simultaneously.
Fitting in all treatments and educational obligations into the school day was difficult for families. One strategy used was to wake earlier on school days, to allow morning and subsequent treatments to be completed, although some children were late to school when undergoing complex treatments. However, as Ball et al. (2013) suggest, school day structures and routines may support families’ management of CF and facilitate adherence. Certainly, this study demonstrated CF routines are more relaxed during weekends and holidays, raising the possibility that treatments during such periods may go uncompleted.
Confirming the work of Closs (2000), this study illuminated examples of the restrictiveness of treatments upon children’s friendships. The social disconnection experienced by children who follow large treatment regimens may further compounded by illness that prevents them from attending school. For many children with chronic illness, a significant aspect of school may be their friendships rather than their educational development (Closs, 2000). Friendships and social activities may take precedence over children’s treatments. While the adults with CF involved in Besier and Goldbeck’s (2012) Germany-based study reported less satisfaction with their social lives, and higher satisfaction with adherence to treatments, the converse may be true for younger individuals with CF. In this sense, the importance of having a fulfilling social life may be detrimental to adherence, and particularly secondary school students for whom social connectivity is a priority (Yates et al., 2010). This study suggests that issues of non-adherence should be considered alongside the perceived restrictiveness of treatments upon activities children and young people enjoy.
The research findings show families frequently make difficult choices about what to prioritize in terms of the management of CF and children’s participation in education. Families experienced dilemmas, having to choose between children either doing treatments or participating in school activities, when doing both did not seem possible. Parents of secondary school students were prepared to circumvent or renegotiate alternative treatment options to protect school time. However, when children were ill or undergoing complex treatments, families occasionally prioritized treatments above schooling. These approaches are consistent with the ‘balancing act’ described by Bolton (1997) in which children’s health and education needs shift in priority at different times. Families of children with CF clearly experience multiple competing priorities in their lives. It cannot be assumed families will always prioritize CF treatments over children’s participation in school activities. Understanding the important aspects of family life will help clinicians plan optimal treatment regimens together with families and recognize factors that influence perceived treatment failures (Foster et al., 2001). Successful integration of therapy into daily routines is crucial for the life satisfaction of individuals with CF (Besier and Goldbeck, 2012). Confirming research by Ball et al. (2013), this study also suggests that it is vital that some flexibility is applied when helping families incorporate treatments into their schedules and achieve treatment concordance. Where appropriate, being flexible about the treatment regimen, beyond organizing treatments around school hours, stands to increase participation in school activities that might not otherwise be possible.
This study corroborates the view of Puckey et al. (2006) that parents experience anxiety when handing care over to other adults, which may prevent them seeking health support from schools. As other research from the UK has found, this study suggests that parents do not feel when there is appropriate school-based health support (Hewitt-Taylor, 2009; Lightfoot et al., 1999). Allowing CF treatments to be administered at school may enable children to continue education as usual when having complex treatments. However, teachers may require more advice from health services to support children’s medical needs (Hinton and Kirk, 2014; Leyland et al. 2016). The possibility remains that inadequate school-based health support perpetuates the practice of arranging treatments around school. However, the children and young people in this study valued school as a place of ‘normality’, as evidence from the UK and Australia also identifies (Lightfoot et al., 1999; Taylor et al., 2008; Yates et al., 2010). It is conceivable that families prefer to organize treatments at home so children do not experience the sense of difference that may arise from having treatments in the school setting. Certain treatment plans may therefore present a barrier to regular school attendance. Although teacher participants did not perceive children with CF to be different from their peers, families will value additional support when children cannot attend school, by keeping in touch and sending work home. It is vital that education continues throughout absences so children do not fall behind in their school work.
Little attention has been paid to how biology and environment interact to cause challenges in the lives of children with CF and their families. This research has illuminated the ecological, bidirectional interactions between CF and children’s schooling. Children’s participation in school activities represents a significant priority for families with subsequent implications for how they manage CF. Equally, the CF treatment regime presents educationally orientated difficulties for children with the condition. These interacting health and educational challenges require combined responses at both the clinical and school level.
Strengths and limitations
This study was conducted by an adult with CF, which was a strength of the research. Families seemed willing to share their perspectives with ease and candour during the interviews due to ‘insider’ understanding of their experiences. Aspects of CF, such as treatments, medication names and symptoms, were discussed freely without further explanation, which might not have been the case had the study been conducted by a researcher without CF. While this study took account of the heterogeneity of children with CF through their varied treatment regimes, there are limitations in terms of the wider generalization of the findings. The study was located in one geographical area and the small sample chosen cannot be representative of all families of children with the condition. Teacher perspectives on how families manage CF alongside school were somewhat limited. One explanation is that CF is mainly managed away from school, potentially reducing teacher awareness of the respective requirements upon families. Another potential limitation is that the study data were generated at a particular ‘snapshot’ in time for each participant. Children’s needs and challenges are not static and may vary in line with their different experiences of life with CF. A longitudinal study may better take into account of such variations.
Conclusion
This article revealed important insights into how families manage CF alongside other routines. The findings represent novel information of interest to CF clinical teams who must help families manage CF and to nurse specialists who inform schools about the needs of children with the condition. Support for children’s educational needs may moderate any disadvantage arising from the challenges families experience when managing CF alongside school. A degree of treatment flexibility may increase participation in school activities. Further research on bidirectional influences between the management of CF and other family routines is required to highlight and respond to significant areas for targeted support. Supportive responses may cross different agency boundaries calling for interdisciplinary research approaches on family experiences of managing CF.
Footnotes
Acknowledgements
The author would like to thank the families, CF nurse specialists and teachers who gave their time freely to take part in the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Economic and Social Research Council (Grant Number: ES/J500215/1).