
Abstract
The aim of this study was to explore the association of Infant and Young Child Feeding (IYCF) practices with health and nutritional status among children aged 0–23 months and to investigate the predictors of minimum acceptable diets (MADs) using Bangladesh Demographic and Health Survey (BDHS) data. Binary logistic regression models were performed to assess the association between IYCF and child health and to determine the influential predictors for MAD. About 55% mothers reported exclusive breastfeeding; 65% introduced solid, semisolid, or soft foods for their child; and 27% maintained minimum dietary diversity (MDD). About 64% children received recommended minimum meal frequency (MMF) and 23% received recommended MAD. The likelihood of having wasting was .22 times lower for the child who received MDD and MMF, respectively. MDD and MAD were associated with lower probability of experiencing underweight among children (Adjusted odds ratio [AOR] = .73 and AOR= .81, respectively). Early initiation and continuation of breastfeeding were significantly associated with reduction in diarrhea prevalence among young children. The findings of the study generated imperative evidence related to dietary diversity, associated factors, and child health outcomes. Policy should focus on the improvement of IYCF practices and complimentary food diversity by taking initiatives for designing and implementing effective interventions to tackle childhood morbidity.
Introduction
Infant and young child feeding (IYCF) practice is a highly concerned global public health issue for its extensive role on child development, growth, and survival (The United Nations Children’s Fund (UNICEF), 2011). Almost 5.9 million under-five children died in 2015; among them, 45% were directly or indirectly associated with malnutrition, pneumonia, and diarrhea, while more than two-thirds of those deaths were due to improper feeding practices (World Health Organization (WHO), 2003, 2016). An estimated 10 million children are vulnerable due to vicious effects of malnutrition globally (UNICEF, 2013). Childhood malnutrition is appeared as a public health threats in both low-income and lower middle-income countries (LMICs) including Bangladesh (Black et al., 2008). It is also evident that malnourished children are more likely to die by experiencing different illnesses, especially respiratory infections and diarrheal diseases (Black et al., 2008). Proper IYCF practices is crucial for improving nutritional status and health, particularly for the young children aged 0–23 months as nutritional status could be directly affected by the IYCF practices (WHO, 2016). Inadequate IYCF practice has a considerable effect on childhood malnutrition, risk of diarrhea (Arifeen et al., 2001), and respiratory infections (Chowdhury et al., 2016). Little evidence is found considering IYCF practices and the health outcomes of the children in resource poor settings of Bangladesh (Lubna et al., 2015; Zongrone et al., 2012). Study reports indicate that exclusive breastfeeding in first six months of life can avert 1.4 million deaths and 10% of diseases burden among infants and young children in developing world (Black et al., 2008). Further evidence suggest that about 10–15% of global under-five deaths could be prevented by achieving 90% of exclusive breastfeeding (Jones et al., 2003).
WHO recommended to initiate breastfeeding within one hour of birth, exclusive breastfeeding for the first six months of life, introducing complementary food at six months of age, continuing breastfeeding up to two years, no prelacteal feeding, no bottle feeding, and maintaining minimum dietary diversity (MDD) for better growth (Coates et al., 2007). Dietary diversity (DD) is conceptually defined as the number of foods consumption from different food groups over a specified period (Ruel, 2003); nevertheless, in this study, we focused on MDD, minimum meal frequency (MMF), and minimum acceptable diet (MAD). Achievement of the MAD is necessary for better growth and proper nutrition of the children as chronic malnutrition significantly associated with dietary diversity in different settings, especially South-East Asia Bangladesh (Arimond and Ruel, 2004; Rah et al., 2010). This accentuates the emerging evidence of the association between dietary diversity and child nutritional status considering socioeconomic status, maternal education, and hygiene practices in rural Bangladesh (Rah et al., 2010).
Under-five children and pregnant women most vulnerable for nutritional deficiency in Bangladesh (Odhiambo, 2013). Furthermore, various socioeconomic and cultural factors are responsible for inadequate feeding practices that may lead to childhood nutritional deficiencies (National Institute of Population Research and Training (NIPORT) and Mitra and Associates and II 2016, 2014). Several studies conducted in different low- and middle-income countries conclude that children’s nutritional status is significantly associated with IYCF practices (Fekadu et al., 2015; Reinbott and Jordan, 2016). The frequency of breastfeeding would contribute to reduce malnutrition, childhood morbidity, and thus could able to reduce 22% of neonatal deaths in Bangladesh (Bhutta et al., 2008; Edmond et al., 2006). The literature reveals some association between feeding practices and child health outcomes (i.e. nutritional status or morbidity) by focusing on single indicator of IYCF practices (Arifeen et al., 2001; Lubna et al., 2015; Rah et al., 2010). Therefore, examination of the association between IYCF practices and child health considering all IYCF indicators for Bangladesh would lend valuable data. As such, this study intended to minimize the information gap of IYCF practices in relation to the nutritional status of Bangladeshi children. This study also focuses on the predictors of dietary diversity and we considered MAD as this indicator composes both MDD and MMF.
The aim of this study was to explore the association of IYCF practices with common childhood morbidities and nutritional status among children aged 0–23 months as well as to investigate the predictors of MADs by analyzing nationally representative data for Bangladesh.
Method
Data source
The study utilized data from the latest Bangladesh Demographic and Health Survey (BDHS) 2014. The survey was carried out in four phases from June, 28 to November 9, 2014 by Mitra and Associates under the authority of the National Institute of Population Research and Training (NIPORT) of the Ministry of Health and Family Welfare of Bangladesh (Mitra and Associates, 2014). The BDHS is a vital source of records on IYCF practices, anthropometric measurements, and morbidity, because it provides information on child health, including newborn care, breastfeeding, immunizations, the occurrence of diarrhea, acute respiratory infections (ARIs), and it assesses the nutritional status of children from a nationally represented sample. Mothers were requested to provide information on consumption of complementary foods during the day or night preceding the interview. IYCF practice-related information collected only for the youngest child of the household who was living with mother, while the respondent was asked to report the number of solid or semi-solid complementary foods were given to the child (Chowdhury et al., 2016; Mitra and Associates, 2014).
Survey design and sampling procedure
The survey was based on a cross-sectional study design, covering the entire population by taking a nationally representative sample using stratified two-stage random sampling procedure from a sampling frame of 2011 (Mitra and Associates, 2014). In the first stage, 600 enumeration areas (EAs) with 207 EAs in urban areas and 393 in rural areas were selected and made the household list from all the selected EAs. In the second stage, 30 households per cluster were selected with an equal probability of systematic sampling procedure from the newly generated household list. A total of 18,245 ever-married women (included widow or divorced) aged 15–49 years were selected, and with a 98% response rate, a total of 17,863 interviews were successfully conducted. Further explanation of sampling design and other related issues is published elsewhere (Mitra and Associates, 2014).
IYCF indicators
IYCF guidelines recommended by WHO was used for this analysis. The selected indicators were early initiation of breastfeeding; exclusive breastfeeding up to six months; continuation of breastfeeding at one year; introduction of solid, semisolid, or soft foods; MMF; MAD; and consumption of iron-rich/iron-fortified food for children up to 6–23 months. The details of these indicators are described elsewhere (WHO, 2003, 2008).
Measurements of nutritional status and childhood morbidity
The measurements of nutritional status of the study children were determined based on the WHO child growth standards by the three indices of stunting (height-for-age Z-score (HAZ)), wasting (weight-for-height Z-score (WHZ)), and underweight (weight-for-age Z-score (WAZ)). The nutritional status of the study children was judged against the WHO child growth standards and defined stunting, wasting, and underweight as being (−2 SD) below the median value for HAZ, WHZ, and WAZ, respectively (Mitra and Associates, 2014). Mothers were requested to provide information whether the child had experienced any diarrheal episodes or any symptoms of ARI within two weeks preceding the survey.
Major explanatory variables
Maternal age was categorized as (‘<20 years’, ‘20–34 years’, and ‘>34 years’), education as (‘no education’, ‘primary education’, and ‘secondary & higher education’), working status (‘housewife/not employed and ‘employed’), childbirth order as (‘first ‘two to three’, and ‘greater than three births’), electronic media access coded as ‘Yes’ if household has a radio/television and ‘No’ if household does not have it, household size (‘≤ 5 members per household’, and ‘> 5 members per household’). Socioeconomic status of the household was measured by calculating the wealth index using principal component analysis and categorized as (‘poorest’, ‘poorer’, ‘middle’, ‘richer’, and ‘richest’) according to BDHS Mitra and Associates, 2014).
Statistical analysis
Data scrutinizing, cleaning, and checking for any inconsistency were done through the execution of range and influential/outlier value identification. Sampling weight was used to address the survey design, and finally a total of 2911 sample observations were included in the analysis. Descriptive statistics such as frequencies and percentages were calculated for sociodemographic, maternal, child, and household characteristics in case of categorical variables and means and standard deviations (SDs) were determined for continuous variables. Core WHO IYCF indicators were stratified and tabulated by the residence of children to investigate residential disparity. Binary logistic regression models were performed to assess the association between IYCF and child health outcomes nutritional measurements of stunting, wasting, underweight, morbidity diarrhea, and ARI) for addressing the predictors for MAD among respective children. The results were presented in terms of odds ratio (OR) with 95% confidence interval (CI) for both adjusted and unadjusted models. Statistical package STATA (version 13) was used to conduct analysis, and results were measured as significant for a p-value < .05.
Ethical approval
BDHS 2014 is a publicly available data set (https://dhsprogram.com/data/available-datasets.cfm). For conducting the analysis approval was sought from the Measure Demographic and Health Survey (DHS) program to use the data sets that have been accepted by the respective authority. According to the DHS, written informed consent was obtained from all participants before enrolling in the survey.
Results
Background characteristics of study population
Background characteristics including maternal and child health, sociodemographic, and household characteristics of the study participants are presented in Table 1. The mean age of study children was 11.88 (SD ±6.48) months, age distribution showed that 19.92% of children were less than six months, while almost 48% children were less than one year, and 53.10% of children were male among the total samples. Considering nutritional status of the children, approximately 28% were stunted, while 26% and 17% were underweight and wasted, respectively. Mean age of the mother was 23.99 (SD ±5.54) years. Approximately 59% of mothers had educational experience which was secondary or higher level, followed by primary education (28%). Forty-one percent of study children were the first-born child of their parents, while the mean birth order was 2.10 (SD ±1.34). Mean household size was 6.19 (SD ±2.81), and most of the households (60.68%) had no access to electronic media. Seventy-five percent of children had the rural residency and 22.03% were from the poorest community. Considering administrative divisions, most of the children (37.27%) were from the Dhaka division, followed by Chittagong (21.05%), while the lowest proportion was found in the Barisal division (5.72%).
Distribution of sociodemographic characteristics, nutritional status, and childhood morbidities 0–23 months children in Bangladesh (n = 2911).

Note: CI: confidence interval; SD: standard deviation.
IYCF indicators
The distribution of WHO-recommended core IYCF indicators and food group consumptions are presented in Table 2 and Figure 1. About 51% mothers reported that their child was breastfed within the first hour of delivery, which was more frequent in rural areas (53%) compared to urban mothers (45%). Overall, the prevalence of exclusive breastfeeding was 55% for the infants aged up to zero to five months, which is slightly higher among rural mothers (58%). During the period of the survey, 96% of mothers stated that their child was continuing breastfed at that moment and breastfeeding continuation after one year was comparatively more frequent among rural mothers (97.18%) compared to urban (93.21%). Approximately 65% of mothers introduced solid, semisolid, or soft foods for their babies at six to eight months of age. Only 27% mothers were able to maintain MDD (greater than or equal to four food items) for their children as recommended by WHO, while the rest (73%) fed their children with less than or equal to 3 food items within the survey. Similarly, 64% children received recommended MMF, and only 23% received recommended MAD. MDD (34%), MMF (67%), MAD (27%), and consumption of iron-rich or iron-fortified foods (60%) were found among the urban communities, while consumption prevalence were 25, 62, 21, and 54% for rural communities, respectively. The most consumed food groups were grain, roots, and tubers (76%), followed by fleshy foods (44%).
Distribution of WHO-recommended core IYCF indicators and food group consumptions.
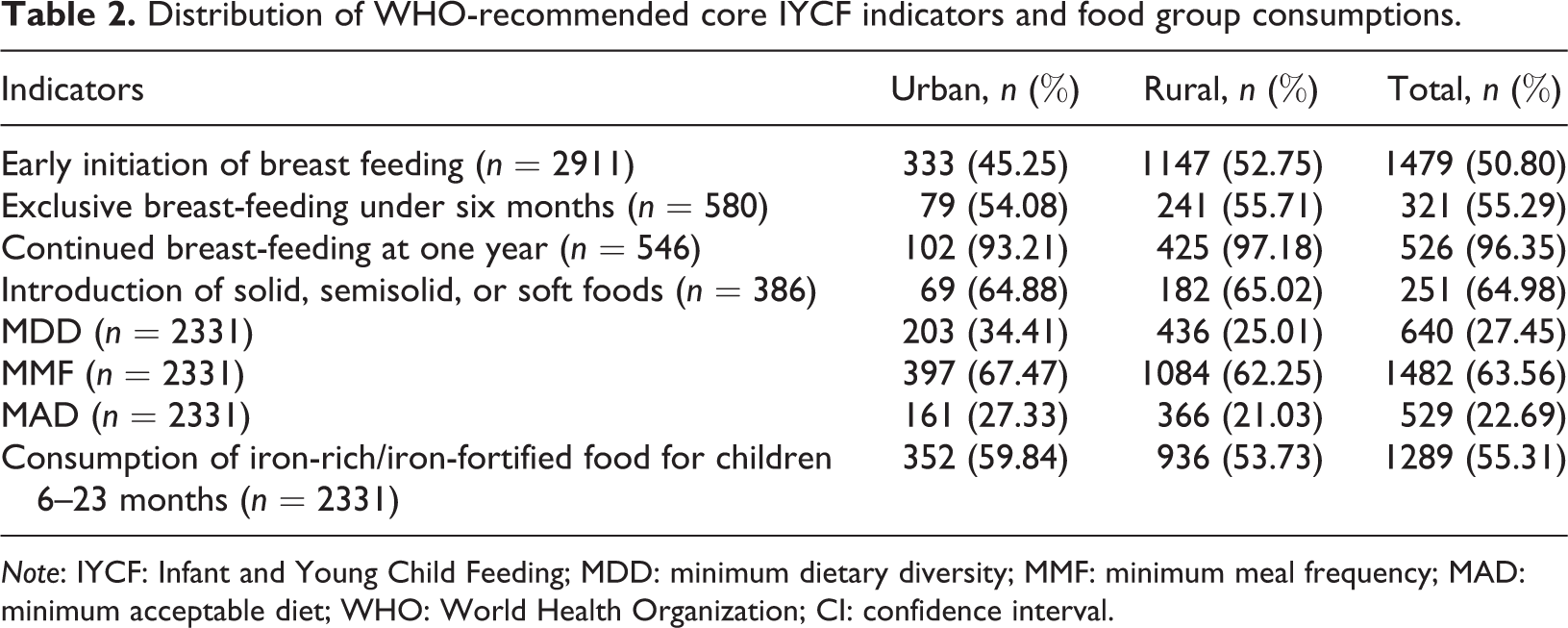
Note: IYCF: Infant and Young Child Feeding; MDD: minimum dietary diversity; MMF: minimum meal frequency; MAD: minimum acceptable diet; WHO: World Health Organization; CI: confidence interval.
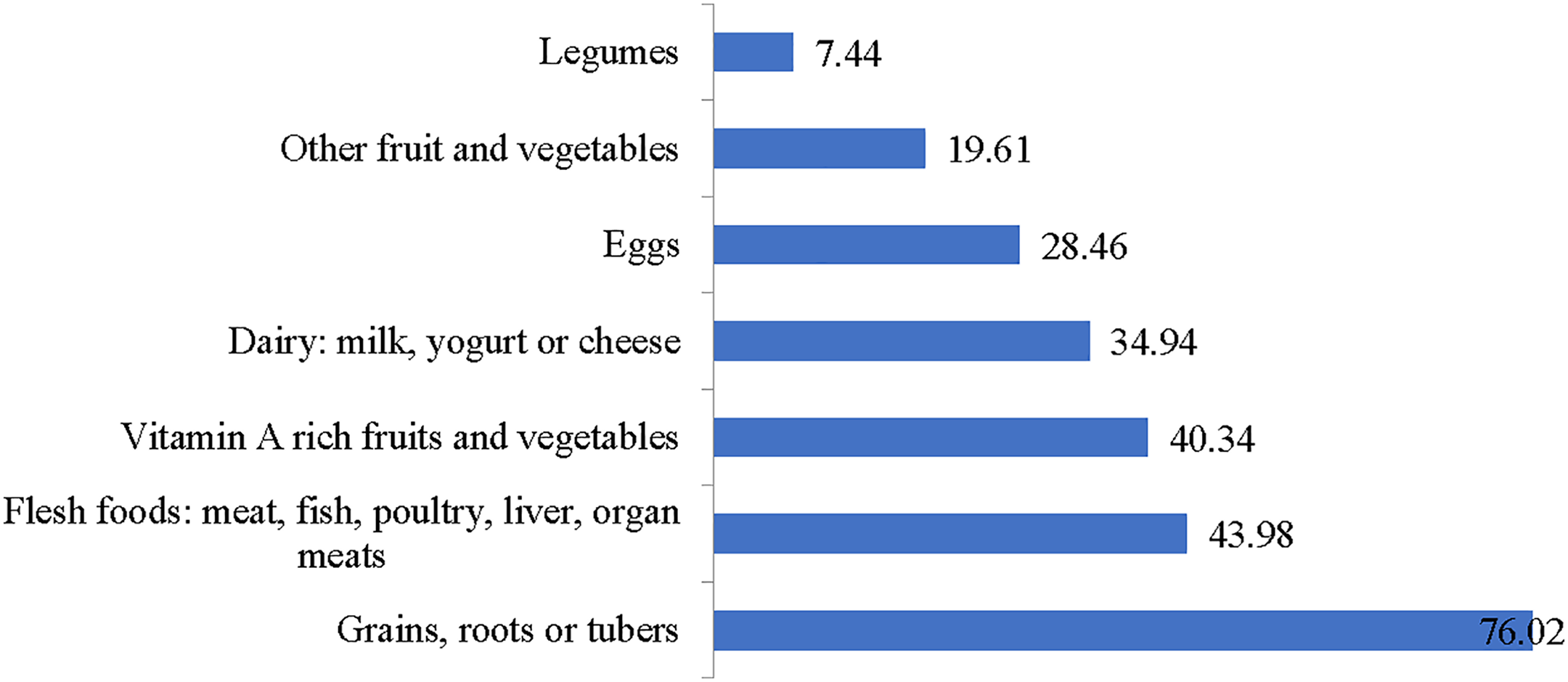
Proportion of food group consumption among study children.
Association between IYCF indicators nutritional status and morbidities
Table 3 represents the association between WHO core IYCF indicators with child nutritional status and morbidities. After adjusting all possible covariates, it was found that achieving none of the IYCF indicators significantly increased the likelihood to be stunted, wasted, or being underweight. Children who achieved MDD and MADs were 32% and 23% less likely of being stunted. The odds of having wasting were .22 times less likely for a child who received MDD and MMF, respectively (adjusted odds ratio [AOR] = .78, 95% CI = .59, 1.04). Similarly, the MDD (AOR = .73) and MAD (AOR = .81) are significantly associated with reduced probability of underweight children. Early initiation and continuation of breastfeeding were significantly associated with reduced childhood diarrhea. Children who achieved MAD were 1.49 times more likely to experience any diarrheal episodes (AOR = 1.49; 95% CI = 1.02, 2.17). However, consumption of iron-rich/iron-fortified food was found as statistically negatively associated with ARI (AOR = .68; 95% CI = .47, .99).
Association between feeding practice dietary diversity with child nutritional status and morbidities in 0–23 months young child in Bangladesh.
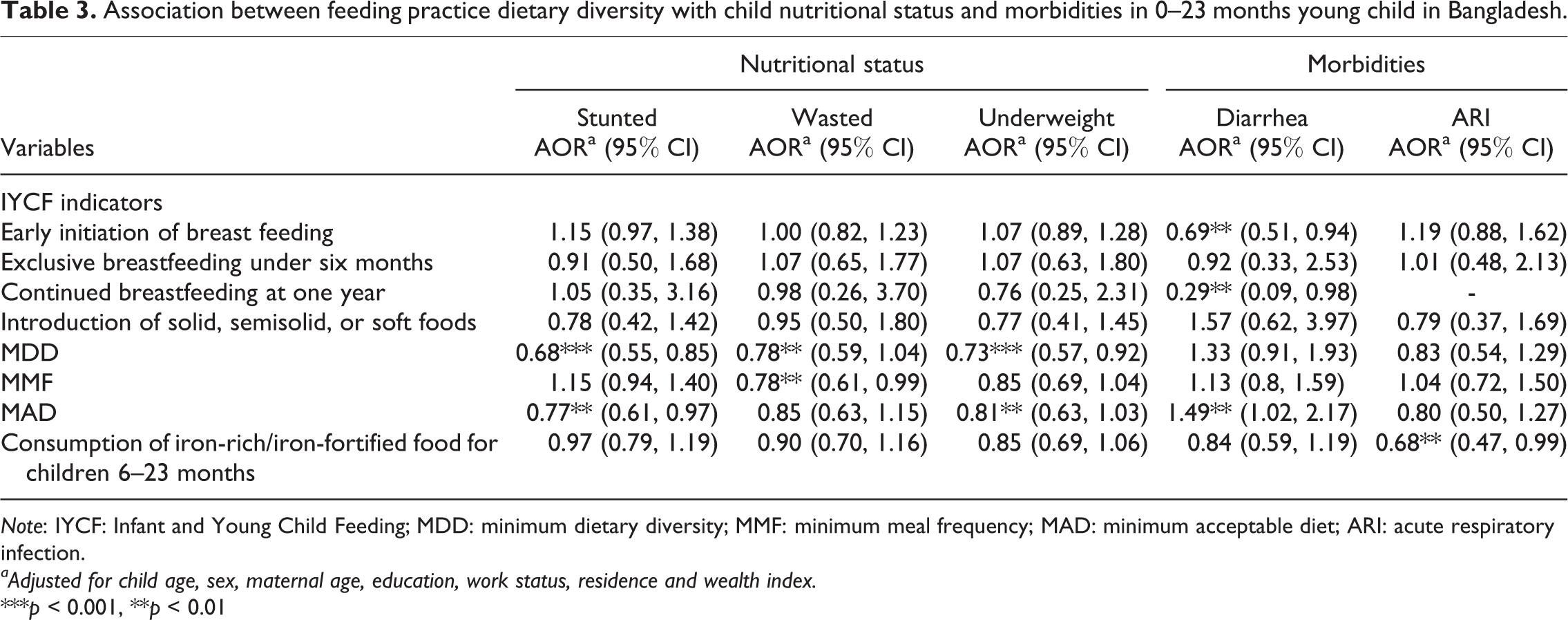
Note: IYCF: Infant and Young Child Feeding; MDD: minimum dietary diversity; MMF: minimum meal frequency; MAD: minimum acceptable diet; ARI: acute respiratory infection.
aAdjusted for child age, sex, maternal age, education, work status, residence and wealth index.
***p < 0.001, **p < 0.01
Predictors of MAD
According to the multivariable regression model, child’s age, maternal age, maternal education, household size, socioeconomic status, and geographical regions/divisions were significant predictors of MAD among children aged 6–23 months (Table 4). Elder child (12–17 and 18–23 months) experienced higher odds of achieving MAD compared to 6–11 months age-group (AOR = 3.01, 95% CI = 2.26, 4.01; p < .001 for 12–17 months and AOR = 4.95, 95% CI = 3.72, 6.58; p < .001 for 18–23 months, respectively). Children were 2.34 times more likely to achieve MAD whose mother’s age was more than 34 years (AOR = 2.34, 95% CI = 1.33, 4.42; p < .001). Also the likelihood of achieving MAD was higher among the children whose mothers had secondary and higher levels of education (AOR = 3.04, 95% CI = 1.97, 4.71; p < .001). The larger household size (>5 members) was associated with 21% rise in odds of achieving MAD than smaller sized household (≤5 members). The probability of achieving MAD was significantly higher among the richest community compared with the poorest one. Administrative divisions played a significant role to achieve MAD. The odds of achieving MAD was higher among Khulna division (AOR = 1.89, 95% CI = 1.24, 2.88; p < .001).
Predictors of MAD among children 6–23 months (n = 2331).
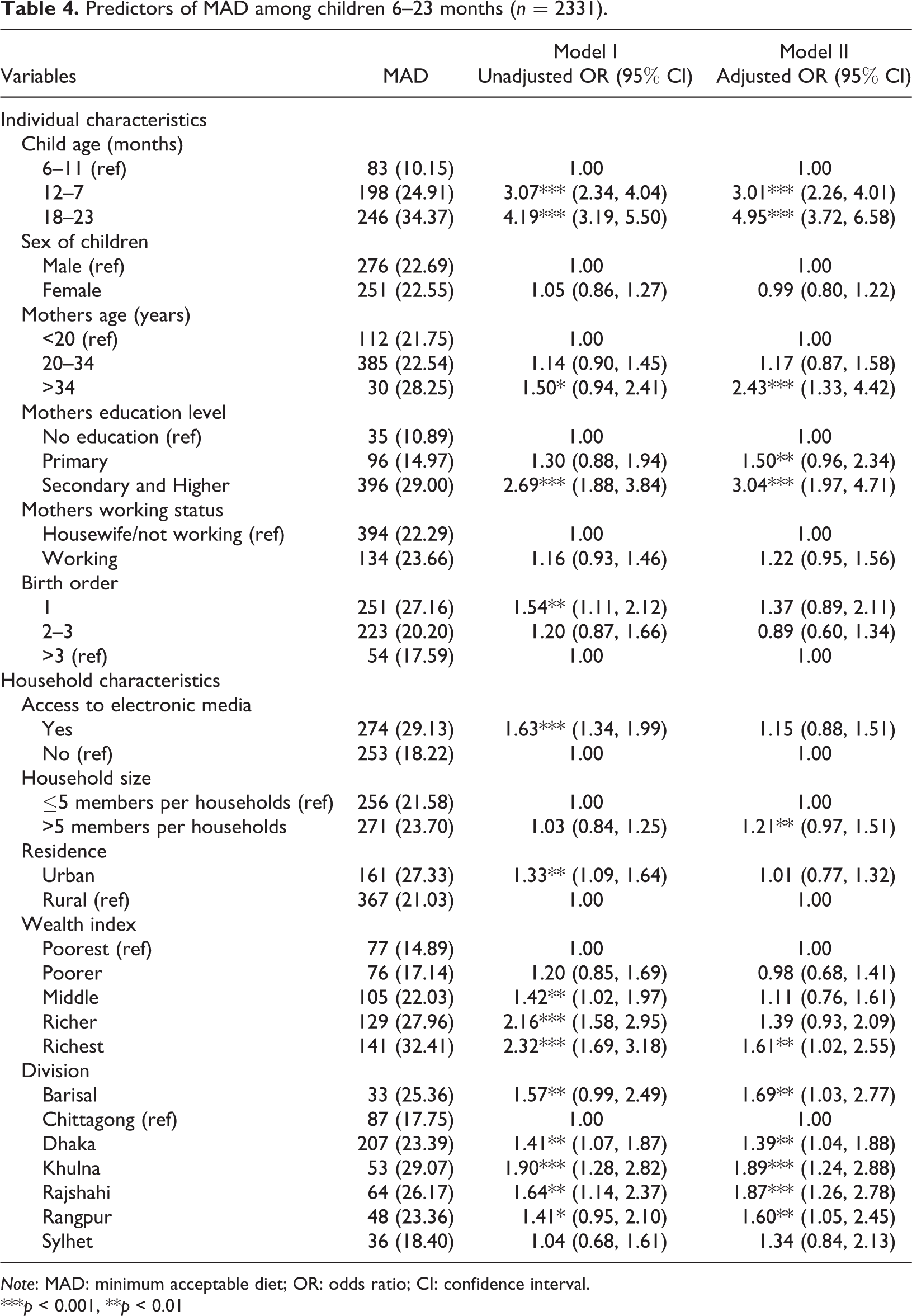
Note: MAD: minimum acceptable diet; OR: odds ratio; CI: confidence interval.
***p < 0.001, **p < 0.01
Discussion
This study provides empirical evidence of the relationship of WHO-recommended key IYCF practice on nutritional status and childhood morbidities using nationally representative household level data set. Our study observed a significant divergence considering IYCF indicators and food consumption among the rural and urban residence, and those who were not able to achieve MAD were more prone to have malnutrition and had more risk of having childhood diarrhea and symptoms of ARIs. These findings indicated a number of factors including age of child, maternal age and education, household size, socioeconomic strata as well as administrative regions were associated with MAD.
Early initiation of breastfeeding is crucial for child survival and the key indicators of IYCF (Mitra and Associates, 2014). It was observed that the practice of early initiation of breastfeeding is comparatively higher among rural mothers. This might be due to a large number of normal deliveries still common in rural setting where as the C-section is comparatively higher in urban mothers. Some earlier studies reported that because of high number of C-sections, urban mothers often unable to initiate breastfed within one hour due to their poor physical conditions (Motee et al., 2013; Mitra and Associates, 2014; Rahman et al., 2014). The similar findings also observed for exclusive breastfeeding, continuation of breastfeeding at one year, and even the timely introduction of complementary feedings is also higher in rural areas than that of urban. Thus, behavior change communication (BCC)-related intervention should be highly encouraged targeting urban mothers. We found about one-fifth of the total children were able to attain MAD, whereas children from urban communities were more likely to attain MAD. Similar patterns were also observed considering iron-rich/iron-fortified food. This might be due to the fact that poor nutritional knowledge and awareness, lower education rate, limited income opportunity, and poor resources are available in rural areas. Therefore, income-generating activities and awareness-building interventions among rural areas may enrich the nutritional status of the children (Kabir et al., 2012).
Our study sorted out a number of predictors those significantly associated with MAD of children. MAD is significantly associated with the age of children where the older children had the better opportunity to take diversified quantity of foods (Rasheed et al., 2011). Maternal age and education significantly positive role for child’s dietary diversity (DD). Educated mothers were regularly providing MAD to their children, which emphasize the importance of maternal education for better child health, because they are well informed about adverse event for the malnourished child (Arimond and Ruel, 2004). However, socioeconomic status also demonstrated significant role for ensuring DD and wealthiest quintiles had the better opportunity to access and afford the MAD than poorest (Nguyen et al., 2013). It is evident that poor people do not use the advantages of health-care services if their particular health problem is not severe as they do not have proper financial security (Mahumud et al., 2015). Like earlier study, we observed that stunting and underweight were moderately high among older children, particularly for the children aged above 11 months as complementary foods are introduced after the first six months (Das and Gulshan, 2017). Policy should be focused on complementary feeding practice at weaning period to fulfill the nutritional requirements for all community-based nutritional program. Study found that more than 7% children experienced symptoms of both diarrhea and ARIs, which may be due to their poor immune systems, more contact with contaminated water, and unhygienic utensils between households (Kamal et al., 2015; Sarker et al., 2016). We did not observe any association between breastfeeding practices and nutritional status like earlier study (Meshram et al., 2013); although many studies found such association (Arifeen et al., 2001; Demiss, 2016; Lubna et al., 2015; Zongrone et al., 2012). This might be due to the influence of other socioeconomic indicators such as maternal education, hygienic practices of the household and others (Meshram et al., 2013). Our study also reveals MDD is significantly associated with the child nutritional status which reduces the risk of stunting, wasting, and underweight (Odhiambo, 2013; Rah et al., 2010), as the variety and quantity of food items contain micronutrients. Therefore, the findings of this study emphasize on the intervention programs of food supplementation to reduce malnutrition in Bangladesh.
A significant relationship was found between breastfeeding practices and diarrheal diseases. Early initiation and continuation of breastfeeding confirmed the protective effect against the childhood diarrheal morbidity, which emphasizes universal breastfeeding programs for reducing diarrheal-related morbidities in the first two years of life (Arifeen et al., 2001; Jones et al., 2003; Lamberti et al., 2011; Victora et al., 2008). In addition, we observed that MAD is associated with the occurrence of childhood diarrhea which is contradictory to other studies (Odhiambo, 2013; WHO, 2003). Infants may suffer from diarrhea from other reasons such as poor knowledge on hygiene, feeding, and weaning practices; however, they might also have lower immunity and intake of various types of milk supplements which might cause diarrheal illness (Beyene et al., 2015). The study also observed consumption of an iron-rich/iron-fortified food reduces the symptoms of ARI among child; conversely, a study concluded that iron supplementation alone would not reduce ARI incidence (Beyene et al., 2015).
Limitations
There are some limitations of the study. Data were collected from a cross-sectional study design, while large sample size might provide statistical significance rather than clinical significance thus limiting causal association. All the information related to childhood diarrhea, ARI, and IYCFs was provided by the mothers; therefore, the recall bias on the study results cannot be ignored. Despite this, the study results can be generalized at the country level because the study utilized data from a nationally representative latest household survey.
Conclusions
A number of factors including age of child, maternal age and education, household size, socioeconomic strata, and administrative regions were significant influencing factors of dietary diversity. The study generated practical evidence that can contribute to take initiatives of effective interventions. Policy should focus on the improvement of IYCF and exclusive breastfeeding practices along with progressive addition of complementary foods diversity to tackle childhood malnutrition and morbidity. To reduce IYCFs knowledge gaps, community-based awareness programs should be initiated for better feeding practice to improve child health.
Supplemental Material
Supplemental Material, Definitions_of_IYCF_indicators_(supplementary_1)_(1) - Infant and young child feeding practice, dietary diversity, associated predictors, and child health outcomes in Bangladesh
Supplemental Material, Definitions_of_IYCF_indicators_(supplementary_1)_(1) for Infant and young child feeding practice, dietary diversity, associated predictors, and child health outcomes in Bangladesh by Nurnabi Sheikh, Raisul Akram, Nausad Ali, SM Raysul Haque, Shabareen Tisha, Rashidul Alam Mahumud, Abdur Razzaque Sarker and Marufa Sultana in Journal of Child Health Care
Footnotes
Acknowledgements
ICDDR, B is grateful to the Governments of Bangladesh, Canada, Sweden, and the United Kingdom for providing core/unrestricted support. The authors would like to thank ICDDR, B and Independent University Bangladesh for the time contribution of the authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.