
Abstract
This study aims to assess the family functioning and health-related quality of life (HRQOL) in Chinese boys with Duchenne muscular dystrophy (DMD) and their parents using Pediatric Quality-of-Life Family Impact Module (PedsQL FIM) and Pediatric Quality-of-Life Inventory (PedsQL) 4.0. Findings from 15 families with DMD were compared with 15 unaffected families. The HRQOL, as measured by the mean PedsQL 4.0 Generic Core Scale scores for the boys with DMD were significantly lower than those of age-matched healthy boys, for overall (p < 0.05, parent-report; p <0.001, self-report), physical (p < 0.001, parent-report and self-report), and social (p < 0.05, parent-report) functioning, but the emotional functioning is not affected. The parent–child concordance of our affected DMD families was generally in the moderate-to-good agreement range (intraclass correlation coefficients from 0.51 to 0.73), except for emotional (0.28) and social (0.31) functioning. The PedsQL FIM total score showed an inverse relationship with the affected child’s age (correlation coefficient: −0.55; p < 0.01) and the disease stage (correlation coefficient: −0.63; p < 0.01) confirming that parental HRQOL and overall family functioning worsened as the child increased in age with advancing disease stage.
Introduction
Duchenne muscular dystrophy (DMD) is the most common inherited neuromuscular disorder, with an incidence of approximately 30 per 100,000 live born males. This neuromuscular disorder is caused by mutation of the DMD gene located on the short arm of the X chromosome at the region of Xp21.2 and has an X-linked recessive inheritance (Soltanzadeh et al., 2010). The estimated prevalence of DMD in Hong Kong is 1.03 per 10,000 males aged 0 to 24 years (Chan et al., 2015). Children with DMD usually remain asymptomatic in the first few years of life, followed by gradual onset of progressive muscle weakness and eventual loss of ambulation between 8 years and 10 years. Muscle weakness further progresses to involve the trunk, upper limbs, and oropharyngeal muscles, causing scoliosis, hypoventilation, arm weakness, and feeding problems. Without medical support, death usually occurs in the late teens or early adulthood due to cardiomyopathy or respiratory failure.
In recent years, with the advancement of respiratory and cardiac care and the recommended use of oral glucocorticoid, the course of natural deterioration caused by the disease has been modified, and the survival of patients with DMD has improved (Liang et al., 2018; Moxley et al., 2010). With the increase in survival of patients, it is important to study their health-related quality of life (HRQOL) and the impact of the disease on their families.
Although studies have shown a lowered HRQOL among DMD patients compared with normal control patients, the exact effect, particularly on emotional functioning, is not yet certain (Bendixen et al., 2012; McDonald et al., 2010; Uzark et al., 2012). Past studies comparing the parent report of pediatric quality-of-life (PedsQL 4.0) with the self-report from affected sons in Western countries demonstrated moderate-to-poor agreement between the affected children and their parents (Lim et al., 2014; McDonald et al., 2010). Similar Eastern studies have been scarce. The purpose of this study was to assess the HRQOL in Chinese children with DMD compared with age-matched healthy peers, examine the parent–child concordance, and identify disease factors that may affect parental HRQOL and family functioning.
Methods
Participants
Children with DMD and control group
Fifteen Chinese boys with DMD aged between 2 years and 18 years who were regularly followed up by the Department of Paediatrics and Adolescent Medicine of the University of Hong Kong and Kwong Wah Hospital, and their parents were recruited in this study. A multidisciplinary team of each hospital regularly assessed the children with DMD following the recommended standard of care. All the affected boys had genetically confirmed DMD. Fifteen age-matched boys without DMD or other chronic diseases and their parents were recruited as controls from the mainstream schools (ranging from grade 1 to the first-year university) during the study period.
Procedures
For the recruited boys with DMD, medical information, including age of diagnosis, oral steroid use, motor performance, cardiac and respiratory status, feeding performance and spinal problems, was systematically collected at the clinic consultation. Written consent was obtained from the parents of the participating boys with DMD, and assents were obtained from the affected boys aged 8 years or older. The Chinese version of PedsQL Inventory version 4.0 was administered in person to the children older than 5 years, while the parents completed the corresponding parent proxy report, together with PedsQL family impact module (PedsQL FIM) 2.0. Boys and parents from the unaffected control group completed PedsQL 4.0. This one-year study conducted from September 2014 to August 2015 was approved by the Institutional Review Board of The University of Hong Kong (IRB reference no. UW13-462).
Measures
PedsQL 4.0 was used to evaluate the HRQOL. The 23-item PedsQL Generic Core Scale consists of a self-report questionnaire for three age groups (5–7, 8–12, and 13–18) and a corresponding parent-reported questionnaire for four age groups (2–4 (toddler), 5–7 (young child), 8–12 (child), and 13–18 (adolescent)) that assesses parents’ perception of their children’s HRQOL. The four age groups represent the presymptomatic, early symptomatic, ambulatory, and nonambulatory stages of the disease, respectively. The 23-item scale includes four dimensions, namely physical functioning (8 items), emotional functioning (5 items), social functioning (5 items), and school functioning (5 items). The summary scores of the PedsQL 4.0 Generic Core Scale include the total scale score (23 items), physical health summary score (8 items), and psychosocial health summary score (15 items from the emotional, social, and school functioning scales). Items are reversely scored and linearly transformed from 0 to 100, so the higher the score, the better the satisfaction. The reliability and validity of this scale have been demonstrated in both healthy and patient populations (Varni et al., 2001).
PedsQL FIM 2.0 was used to evaluate the impact of DMD on the families and consists of a 36-item questionnaire with eight dimensions to produce a PedsQL FIM total scale score. It also produces a parental HRQOL summary score that includes physical, emotional, social, and cognitive functioning subscales (20 items), a family functioning summary score that includes daily activity and family relationship subscales (8 items), a communication subscale score (3 items), and a worry subscale score (5 items). Items are reversely scored and linearly transformed to a 0–100 scale (0 = 100, 1 = 75, 2 = 50, 3 = 25, and 4 = 0), so the higher the score, the better the family functioning (Varni et al., 2004).
Clinical stages of DMD
We categorized the DMD boys according to the four clinical stages determined by ambulatory status. These stages included stage 1: presymptomatic (n = 4, age: 2–4.5 years); stage 2: early ambulatory (n = 4, age: 5–8 years); stage 3: late ambulatory (n = 4, age: 8–13 years); and stage 4: nonambulatory (n = 3, age: 14–18 years).
Statistical analyses
To explore the QOL differences between DMD group with the healthy controls, paired t-tests were used for the PedsQL 4.0 Generic Core Scale. To study the differences in family impact between the DMD group and other neurological conditions, paired t-tests were used for the PedsQL FIM 2.0 scores. To study the correlation of age and clinical stage with QOL, Spearman’s rank correlation coefficients were calculated. Spearman’s correlation ranges from −1 to +1, with −1 indicating perfect inverse linear correlation, +1 perfect linear correlation, and 0 no linear correlation. The Spearman’s correlation was used instead of Pearson’s correlation because it provides a more accurate inference for ordinal variables such as clinical stage. To address the potential of false positive among multiple tests, the p values of the correlations were adjusted using the Holm–Sidak method (Aickin and Gensler, 1996).
Two methods were used to examine the agreement between parent- and child-reported QOL, firstly, by Pearson’s correlation coefficient and, secondly, by intraclass correlation (ICC). The interpretation of Pearson’s correlation is similar to that of Spearman’s correlation. ICC ranges from 0 to 1, indicating the percentage of variance that cannot be explained by reporter difference. The statistical significance of correlation coefficients and ICC were examined by the two-tailed p-values, indicating the probability of generating the observed data under a null hypothesis (i.e. correlation and ICC = 0). All statistical significance was defined with two-tailed p values <0.05. R and IBM’s SPSS 22 were used for statistical analysis.
Results
Patient and family characteristics
Fifteen parents of 15 boys with DMD participated in this study. The 15 boys came from 13 families and included two pairs of twin brothers. Most of the affected boys were in the ambulatory stage (n = 12; 80%). Two-thirds of the boys studied in the mainstream school (n = 10), while one-fifth attended special schools (n = 3) and two children had not yet started school. All of the parents of the 15 DMD boys were married couples (n = 15), and over 90% had received education at the secondary level or above (n = 14 for both fathers and mothers). Demographic characteristics of the 15 boys with DMD and their parents are presented in Table 1.
Demographic characteristics of the 15 boys with DMD and their parents.
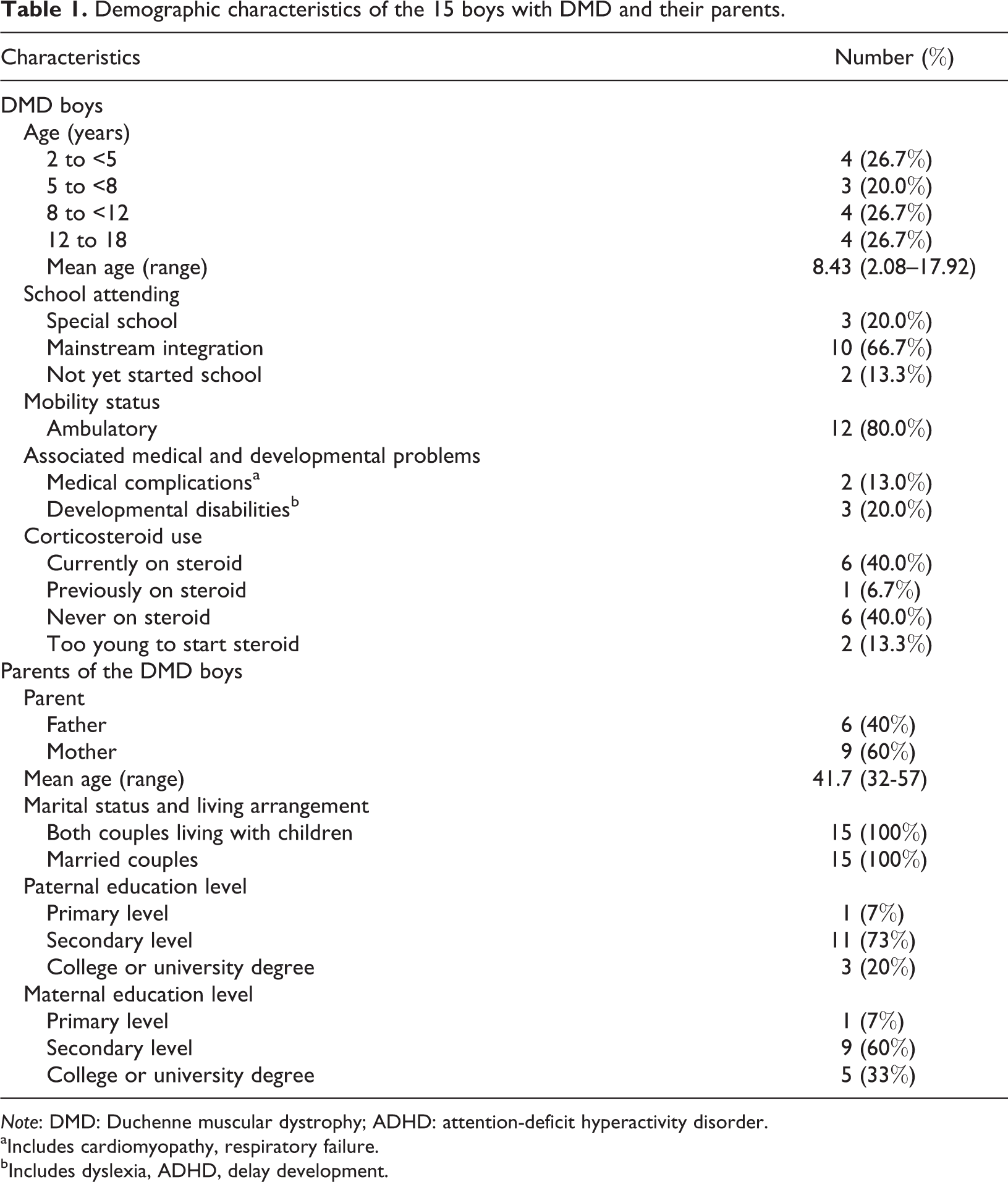
Note: DMD: Duchenne muscular dystrophy; ADHD: attention-deficit hyperactivity disorder.
aIncludes cardiomyopathy, respiratory failure.
bIncludes dyslexia, ADHD, delay development.
Comparison of HRQOL and psychosocial functioning of boys with DMD with an age-and-gender-matched control group measured by the PedsQL 4.0 generic core scale
As presented in Table 2, the mean score for boys with DMD was significantly lower than that of the healthy controls in terms of overall and physical QOL (p < 0.05) for both the child self-report and parent report. From the parent report, the affected boys’ social QOL was also markedly impaired. The significant difference in the QOL between the DMD boys and the healthy controls also exhibited a large effect size (Cohen’s d > 0.80), suggesting a substantial impact of DMD on the affected boys’ HRQOL from the perspectives of both the parents and the affected children themselves. However, both the parent report and self-report showed similar emotional QOL to that of the healthy peers.
Comparison of the self-reported and parent reported PedsQL generic module 4.0 scores of the DMD and age-matched healthy control groups.
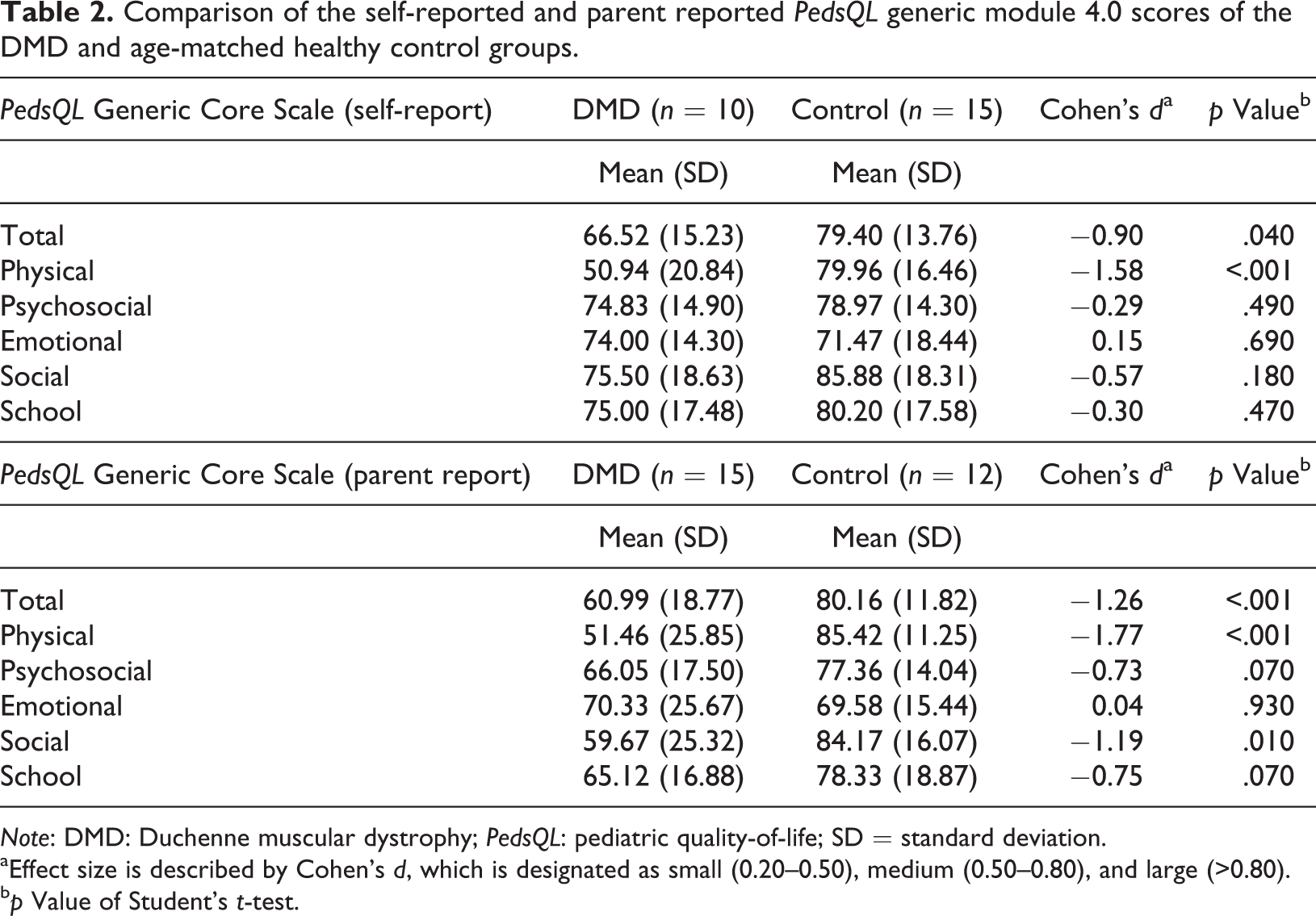
Note: DMD: Duchenne muscular dystrophy; PedsQL: pediatric quality-of-life; SD = standard deviation.
aEffect size is described by Cohen’s d, which is designated as small (0.20–0.50), medium (0.50–0.80), and large (>0.80).
bp Value of Student’s t-test.
Agreement between parent- and child-rated HRQOL
To observe the agreement or differences between the perceptions of the affected children and their parents, the ICC was examined for the PedsQL 4.0 Generic Core Scale. ICC values of <0.4, 0.41–0.6, 0.61–0.8, and 0.81–1.00 were assigned for poor-to-fair, moderate, good, and excellent agreement, respectively (Uzark et al., 2012). As illustrated in Table 3, the agreement in ICC between the children and the parents was good on the total composite, physical health summary, and school functioning summary scores (ICC 0.65–0.73). The means of the parent reports were lower than those of the children’s self-reports on all of the scores, except for the physical health summary scores. In other words, the parents consistently underestimated their children’s non-physical HRQOL. There was poor-to-fair agreement on the emotional (ICC = 0.28) and social (ICC = 0.31) functioning scores. Furthermore, both the mean difference and Pearson’s r were significant for the total composite score and for the physical health and school functioning summary scores. This result indicates that the children’s and parents’ ratings were consistent in terms of rank order, although they did not obtain the same scores.
ICC examined for the PedsQL 4.0 Generic Core Scale (n = 10).
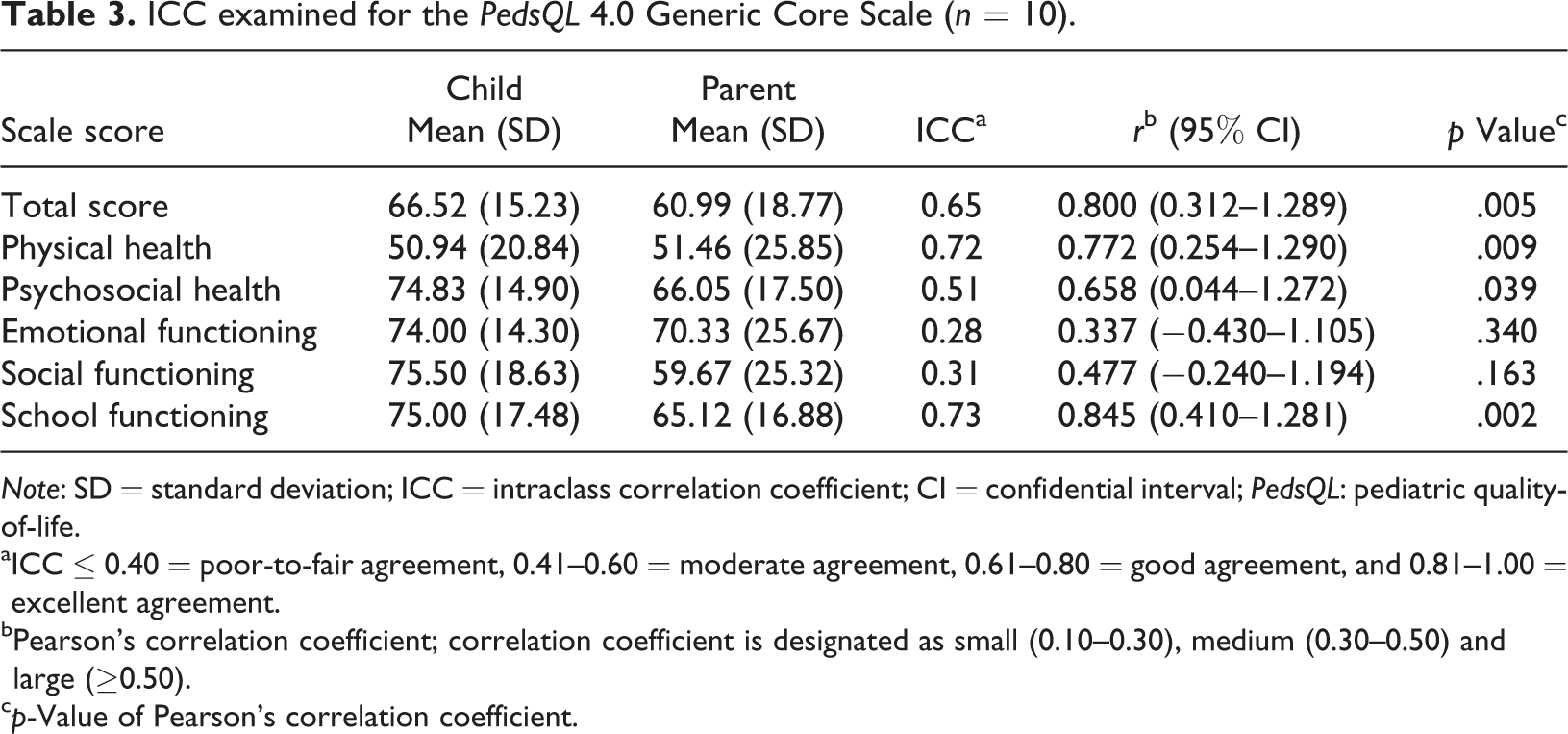
Note: SD = standard deviation; ICC = intraclass correlation coefficient; CI = confidential interval; PedsQL: pediatric quality-of-life.
aICC ≤ 0.40 = poor-to-fair agreement, 0.41–0.60 = moderate agreement, 0.61–0.80 = good agreement, and 0.81–1.00 = excellent agreement.
bPearson’s correlation coefficient; correlation coefficient is designated as small (0.10–0.30), medium (0.30–0.50) and large (≥0.50).
cp-Value of Pearson’s correlation coefficient.
Correlation between clinical disease stage and HRQOL for the boys with DMD
We examined the correlation of the PedsQL scores with four predetermined clinical stages. As explained in Table 4, the clinical stages showed a statistically significant negative correlation (r < −0.50) with the parent-report HRQOL (r = −0.60), psychological (r = −0.54), and social (r = −0.64) functioning on the PedsQL 4.0 Generic Core Scale. Similarly, the increasing age of the DMD boys was significantly associated with lower self-report physical (r = −0.48) and school (r = 0.39) functioning on the PedsQL 4.0 Generic Core Scale.
Correlation coefficienta from Spearman’s ranking correlation analysis of age and clinical staging with the PedsQL 4.0 Generic Core Scale.
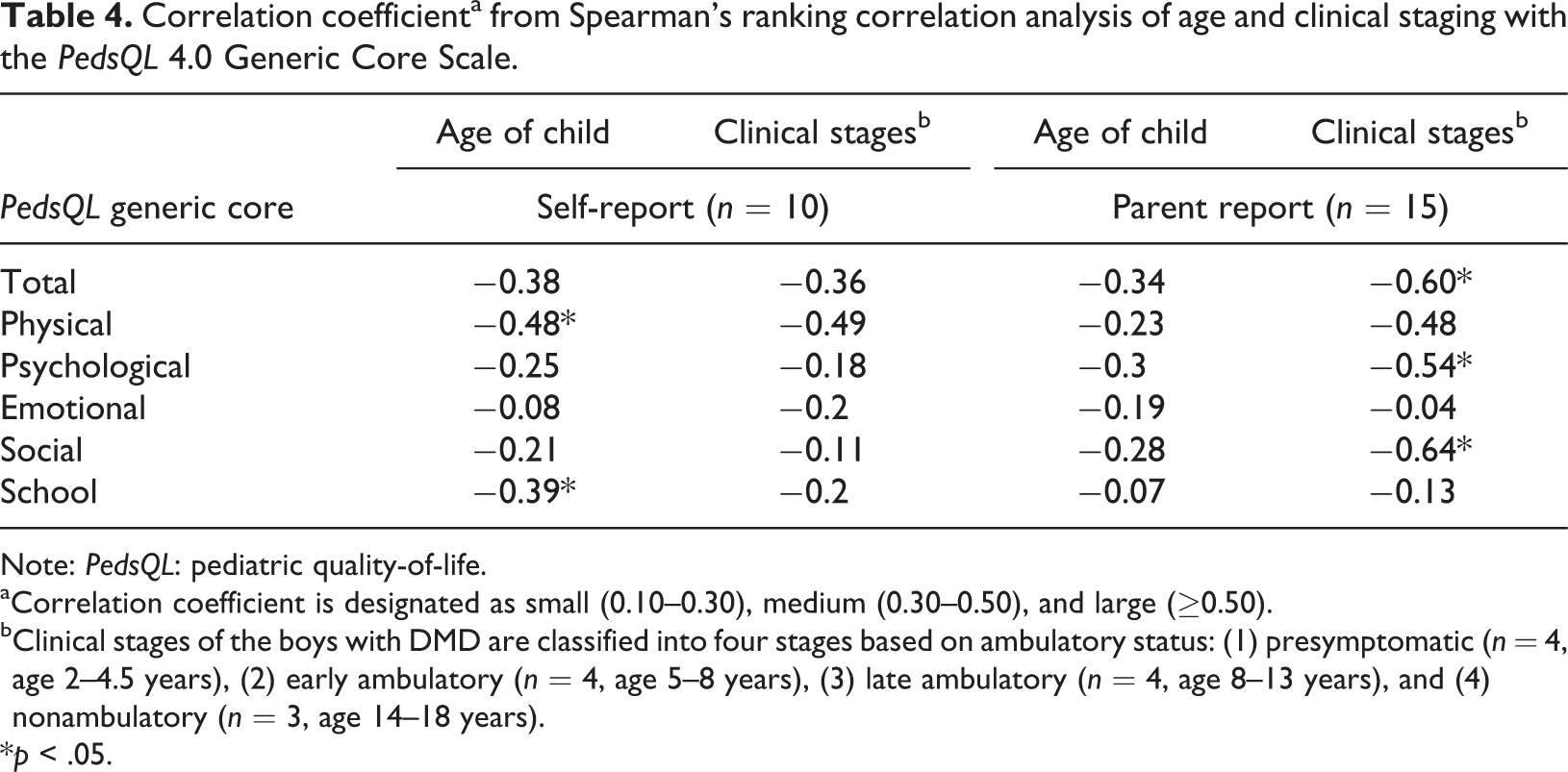
Note: PedsQL: pediatric quality-of-life.
aCorrelation coefficient is designated as small (0.10–0.30), medium (0.30–0.50), and large (≥0.50).
bClinical stages of the boys with DMD are classified into four stages based on ambulatory status: (1) presymptomatic (n = 4, age 2–4.5 years), (2) early ambulatory (n = 4, age 5–8 years), (3) late ambulatory (n = 4, age 8–13 years), and (4) nonambulatory (n = 3, age 14–18 years).
*p < .05.
Parents’ HRQOL and view of the impact of DMD on the family
The PedsQL FIM was applied to evaluate the impact of DMD on the parents’ HRQOL and family functioning. The total PedsQL FIM score of the parents of children with DMD was compared with previous findings on global developmental delay and traumatic acquired brain injury. The HRQOL and family functioning scores of parents of children with DMD (mean ± standard deviation (SD) 62.84 ± 14.94) were comparable with those of parents of children with global developmental delay (mean ± SD 60.60 ± 13.70; p = .58, |Cohen’s d| 0.16, so small effect size), but the scores were significantly lower compared with those of parents of children with acquired traumatic brain injury (mean ± SD:83.60 ± 16.10) (p < 0.001, |Cohen’s d| −1.3, >0.80, so large effect size). Effect size is described by Cohen’s d, which is designated as small (0.20–0.50), medium (0.50–0.80), and large (>0.80).
Correlation analysis also showed statistically significant negative correlations between the PedsQL FIM 2.0 scale, parental HRQOL summary and communication subscale scores and the age and clinical stage of the boys with DMD—the higher the age or the more severe the clinical disease stage of the boys with DMD, the more negative the impact on the families and parents. Both the emotional and the social functioning of the parents were negatively related to the boys’ age and clinical disease stage. In addition, the more advanced clinical staging was associated with, the more negative physical functioning of the parents (r = −0.57) and the daily activities of the family (r = −0.52) (Table 5).
Correlation coefficienta from Spearman’s ranking correlation analysis of the age and clinical stage with the PedsQL FIM scale, summary, and subscale scores.
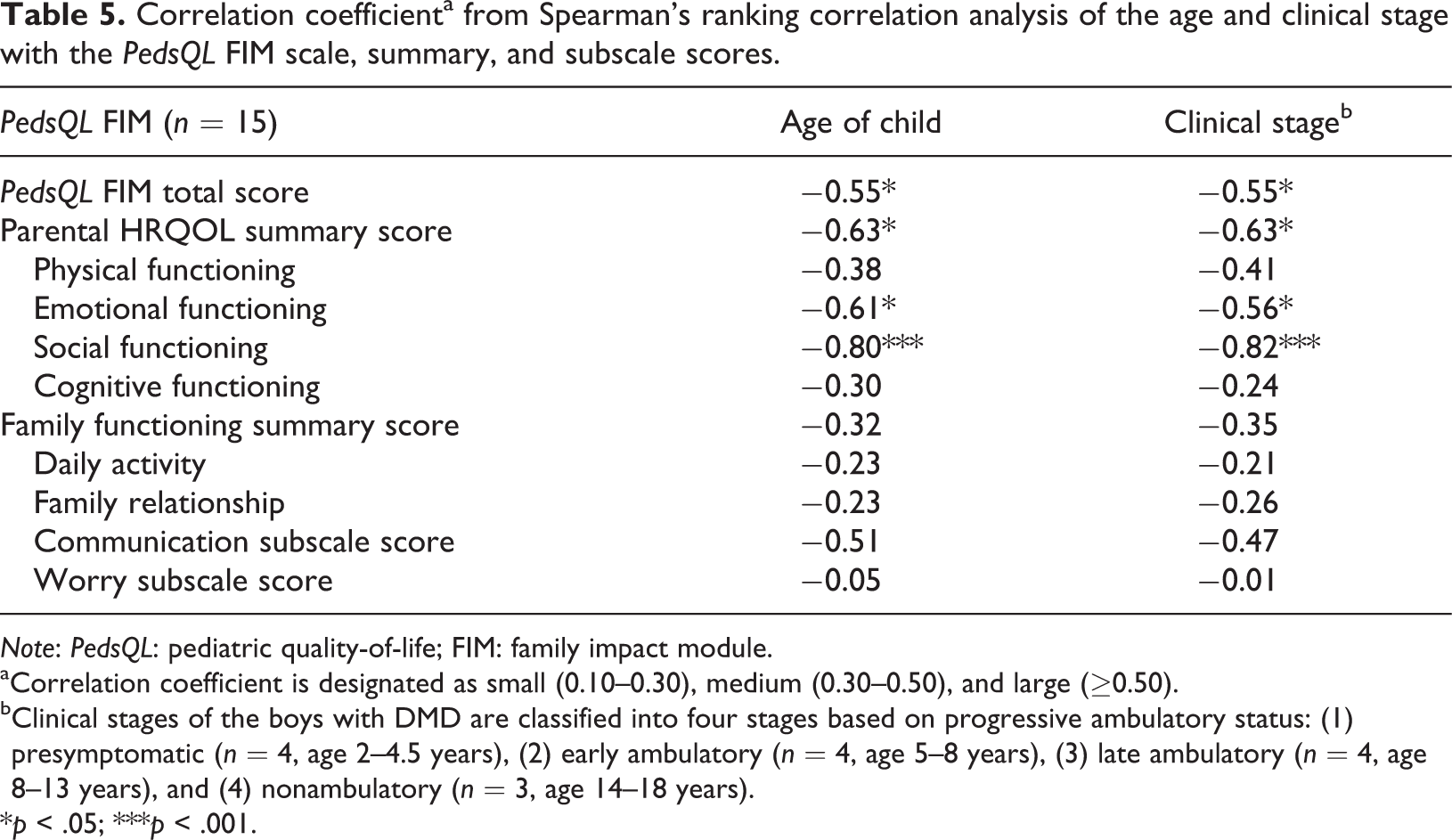
Note: PedsQL: pediatric quality-of-life; FIM: family impact module.
aCorrelation coefficient is designated as small (0.10–0.30), medium (0.30–0.50), and large (≥0.50).
bClinical stages of the boys with DMD are classified into four stages based on progressive ambulatory status: (1) presymptomatic (n = 4, age 2–4.5 years), (2) early ambulatory (n = 4, age 5–8 years), (3) late ambulatory (n = 4, age 8–13 years), and (4) nonambulatory (n = 3, age 14–18 years).
*p < .05; ***p < .001.
Discussion
HRQOL and psychosocial functioning of DMD patients
PedsQL 4.0 has been widely used to evaluate the HRQOL and psychosocial functioning of the DMD population. More than 20 studies have been published overseas using the preceding measurements (Wei et al., 2015), and only 1 study was conducted to determine the reliability and validity of the translated Chinese version of the instrument for Chinese DMD patients (Hu et al., 2013). Consistent with previous studies (Bray et al., 2011; Davis et al., 2010; Henricson et al., 2013; Uzark et al., 2012), the PedsQL 4.0 overall HRQOL and physical functioning of our participants with DMD were impaired compared with those of the age-matched healthy boys recruited for this study. In contrast to previously published results, emotional functioning was not impaired among our DMD patients compared with their healthy peers (Bendixen et al., 2012). The observed difference could be explained by the following contributing factors. Most of the recruited boys with DMD (80%) were still in the ambulatory stage. The easily accessible medical care and special education support helped the children cope better with the changes following the natural disease course. None of the parents of our participants with DMD were separated. An intact family structure probably played an important role in strengthening family ties and providing emotional support for the affected children.
In this study, parent–child concordance was generally in the moderate-to-good range except for social and emotional functioning. Such disagreement in the perception of the social and emotional domains between boys with DMD and their parents was not observed in our age-matched control healthy boys, suggesting that such discrepancy was not due to the difference in perception between the two generations. In fact, previous studies also showed that affected boys did not perceive major concerns about their emotional and social functioning as their parents did (Houwen-van Opstal et al., 2014; Lim et al., 2014). The realization of this discrepant perception in both social- and emotional-related HRQOL between the affected boys and their parents allows the parents to better appreciate the positive perceptions and resilience of their child. With a better understanding of their child’s view, the parents could better understand and communicate with their child.
In our study, higher age correlated with lower HRQOL scores according to the parents and the children with DMD, while the loss of ambulatory status also correlated with lower HRQOL scores according to the parents, but not the affected children, of the PedsQL 4.0. The findings are consistent to previous studies reporting the positive association between age and disease severity (Jung et al., 2012; Liang et al., 2018), so a lower HRQOL score is expected. Another important contributing factor could be related to cognitive maturation. When the boys entered adolescence stage, they were able to better understand the different aspects of their QOL and to communicate their thoughts more clearly when reporting their impression and stress on the self-report questionnaires. Deteriorating ambulatory status likely makes the children more dependent in their daily activities, causing more stress for their parents, who are the main caretakers of the affected children, thereby explaining the lower HRQOL scores from the parents in our findings. In contrast to a previous report observing a decrease in the mean patient PedsQL score across ambulatory classes (Landfeldt et al., 2016), the HRQOL scores of our recruited boys are not significantly affected by the ambulatory status. There could be several explanations for this: (1) the recruited boys who were in the late ambulatory and nonambulatory stages in this study were studying in the special schools for children with physical impairment that have an easily accessible and barrier-free school environment, the provision of assistive technology to facilitate their learning, and the allowance for their use of power mobility for their outdoor travel. So, their participation in daily activities was not limited and (2) the small number (n = 3) and relatively young age (<18 years old) of our nonambulatory patients could also contribute to the insignificant difference finding.
Parental HRQOL and functioning of families with children with DMD
This study is the first to use PedsQL FIM 2.0 to study families with children with DMD. PedsQL FIM has been used to study the impact of family on children for whom palliative care teams (Weaver et al., 2018) are monitoring for progress and of other common neurological problems such as global developmental delay or traumatic brain injury (de Kloet et al., 2015; Hsieh et al., 2013). However, it has never been used to study families affected by DMD. A few studies have discussed parental stress and the child- and family-related variables affecting the function of families with DMD patients (Chen, 2008; Mah et al., 2008; Yilmaz et al., 2010). PedsQL FIM assesses the HRQOL of parents of children with DMD and the overall functioning, communication, and worry of the family. It has been proved that parental HRQOL and family functioning are determinants of the QOL and well-being of children with medical diseases (Palermo and Chambers, 2005; Palermo et al., 2014).
We analyzed the correlation between different scale scores in PedsQL FIM 2.0 and the age and clinical disease stage of boys with DMD. The association between increasing age and clinical stages with lower PedsQL FIM Scale and Parental HRQOL Summary scores suggests that the disability level of the affected children is related to the negative impact on family functioning, increases parental stress, and lowers parental HRQOL. Parents who act as the main caretakers of their children worry about the ongoing deterioration of their son’ physical health. They also have less time for their own social activities and rest. These findings contrast with a previous study which mentioned that the disability level of children with DMD did not affect family functioning (Chen and Clark, 2007).
Strength and limitations of this study and future research directions
This study was initiated to assess the use of the Chinese version of PedsQL 4.0, including both the self-report and the parent report forms, to measure the HRQOL of Chinese boys with DMD, and to compare their findings with healthy age-matched boys recruited during the same study period. The current study supported the use of the Chinese version of PedsQL 4.0 as a feasible and reliable measure of the HRQOL of Chinese boys with DMD. This study was limited in that the small number of DMD families being studied affected its statistical power. In other words, the association found to be non-significant in this study can be due to the lack of statistical power rather than the lack of association. We should also note that we have used Spearman’s correlation (instead of Pearson’s) to avoid assuming normality and that the t-test can perform equally well (albeit with lower power) in very small sample size (De Winter, 2013). Other family-related factors such as family income, extended family support, and living area that could affect family functioning, cultural-related factors, such as cultural understanding of the impact of DMD, and developmental factors, such as the impact of adolescence stage on the mental health of the affected children and the change in parental management, were not studied and should be considered in future larger studies.
Conclusion
Overall, the HRQOL, as measured by the PedsQL Generic Core Scale, of the 15 Chinese boys with DMD was significantly lower than that of the unaffected age-matched Chinese healthy boys. The parental HRQOL and overall family functioning as measured by PedsQL FIM deteriorated as the children’s age and disease stage advanced. Contrary to the previous findings of Western studies, the Chinese parents and their affected sons in this study had better overall agreement (moderate to good) on the measures of the perceived HRQOL of affected children, suggesting parents in the Chinese families in Hong Kong have a closer understanding of the perception of the HRQOL of their children.
Footnotes
Acknowledgements
The authors thank Mapi Research Trust for their approval to use PedsQL 4.0 and PedsQL FIM 2.0 in our research. The authors also take this opportunity to thank all the participating families. Without their support and help, this study will not be possible.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.