
Abstract
Preterm infants are at risk of developing social-emotional and behavioural difficulties. To understand the experiences of their caregivers in day-to-day life, parents (at 2 and 10 years) and teachers (at 10 years) completed a behavioural questionnaire and answered two open-ended questions addressing their concerns and the most positive aspects regarding their child and/or pupil (born <32 weeks gestation). Their answers were analyzed using thematic content analysis. Parental concerns at two years related equally to themes in the clusters Developmental Milestones, Physical Development and Development in Relation to the Self and Others. At 10 years, both parents and teachers reported mainly within the cluster Development in Relation to the Self and Others, but the underlying themes differed. While parents more often mentioned their child’s emotional development, teachers were more concerned about their pupils’ difficulties interacting with their peers, due to a lack of social skills. In-depth qualitative analysis of what parents and teachers experience from day-to-day improves our understanding of the social-emotional and behavioural development of children born very preterm, revealing important topics that should be addressed during follow-up.
Keywords
Introduction
Preterm-born children are susceptible to develop social-emotional and behavioural problems throughout life (Allotey et al., 2018; Aarnoudse-Moens et al., 2009). In early childhood, they are particularly at risk for neurodevelopmental disabilities (Saigal and Doyle, 2008), while school and social-emotional difficulties, including peer relationship problems and anxiety, become more apparent from school-age onward (Linsell et al., 2019; Saigal and Doyle, 2008). Compared to their term-born peers, they are also more prone to psychiatric disorders, including attention-deficit hyperactivity disorder (ADHD) (Johnson et al., 2010). Such disorders may lead to family distress, diminished academic performance and may, later on, have a negative impact on their careers and relationships (Gray et al., 2008; Saigal and Doyle, 2008; Turney and McLanahan, 2015).
Most studies investigating social-emotional and behavioural development in preterm-born children focus on quantitative measures and categorize symptoms according to classifications, for example, attention problems and ADHD or withdrawn behaviour and autism (Aarnoudse-Moens et al., 2009; Johnson et al., 2010). Focussing solely on classified outcomes might fail to consider the full range of caregivers’ main concerns and day-to-day worries, or the aspects they value most in their child after the difficult start of being born preterm. A mixed-method study showed that most parental concerns at 18-months after preterm birth relate to language and motor development (Jaworski et al., 2018). Furthermore, it showed that parents are most content with their child’s personality characteristics, for example, being easy going or curious. These findings would have remained undetected with a quantitative analysis of a behavioural questionnaire, even though they form relevant issues that should be addressed during follow-up assessment of preterm-born children. To our knowledge, qualitative assessments have not previously been conducted in older children.
The use of parents as a sole source of information might not be sufficient, as they, especially as parents of very preterm infants, may be more sensitive to later problems considering their early experiences (Bora et al., 2011). As the role of teachers increases during the daily life of school-aged children, they become valuable additional source of information regarding a child’s social-emotional and behavioural functioning in relation to its peers. Studies comparing the outcomes of parental and teacher questionnaires reported no differences in ratings on internalizing and externalizing behaviour (Aarnoudse-Moens et al., 2009), but this does not necessarily mean that there are no differences in how parents and teachers experience daily behavioural issues at home and in the classroom. To date, qualitative data on parent’s and teacher’s perspectives are lacking for school-aged children, leading to a gap in understanding which topics, both positive and/or causing concern, are predominant for caregivers in their day-to-day experience with children born preterm (Allotey et al., 2018). Insight in these specific experiences will enhance the knowledge of the social-emotional and behavioural development of preterm-born children. Creating a broader understanding of the social-emotional and behavioural development of preterm-born children with regard to the themes parents and teachers struggle with most in daily life and over time is important. It will aid the counselling of parents of preterm-born children today in terms of what they might expect in the future, but also provides insight in topics that should be addressed by clinicians caring for preterm infants and their parents.
Aim
Our aim was to assess aspects causing the most concern in the development of very preterm-born children for parents at 2 years of age and for parents and teachers at 10 years of age. Subsequently, we wanted to identify which aspects of the child are considered most positive.
Methods
Population
This study was part of a larger single-centre, prospective longitudinal study on neuroimaging and outcome after preterm birth. It was conducted in Leiden University Medical Centre, one of the ten hospitals with a Neonatal Intensive Care Unit in the Netherlands. Up to May 2017, the unit consisted of two intensive care units with room for 16 neonates, and one high-care unit that could accommodate nine neonates. Children born <32 weeks gestational age who had been admitted to our tertiary neonatal intensive care unit between May 2006 and November 2007 and underwent a MRI at term-equivalent age were included. Exclusion criteria were congenital anomalies of the central nervous system, severe other congenital anomalies, chromosomal disorders, metabolic disorders and/or neonatal meningitis.
The institutional review board of our centre approved this study, and written parental consent was obtained from both parents (P06.002). For the follow-up at 10 years of age, a waiver was obtained as this is part of the national clinical follow-up program (C15.072/P17.087).
Social-emotional and behavioural assessment
All children were invited for follow-up visits at the age of 2 years, corrected for prematurity and at 10 years. Parents completed the Child Behavioural Check List (CBCL) (Achenbach and Rescorla, 2001; Verhulst et al., 1996) during both visits. The CBCL was standardized in a national representative sample of 4–18 year old children, who were enrolled in regular education, without recent professional care. The Dutch committee that provokes the quality of, amongst others, questionnaires (COTAN; Commissie Testaangelegenheden Nederland) has assessed the reliability and validity of the CBCL as at least sufficient.
At 2 years of age, parents completed the CBCL 11/2–5, consisting of 100 items that describe emotional and behavioural issues of pre-schoolers. Each item contains a specific behaviour rated on a three-point Likert scale by either scoring 0 (not true), 1 (somewhat or sometimes true) or 2 (very true or often true). Based on the answers, eight syndrome scales are calculated: emotionally reactive behaviour (e.g. disturbed by any change in routine), anxious/depressed behaviour (feelings are easily hurt), somatic complaints (aches or pains without medical cause), withdrawn behaviour (avoids looking others in the eye), sleeping problems (does not want to sleep alone), attention problems (rapid shifts from one activity to another) and aggressive behaviour (demands must be met immediately). Together the syndrome scales form a total problem scale that is divided into the subscales internalizing problem behaviour (emotionally reactive, anxious/depressed, somatic complaints and withdrawn behaviour) and externalizing problem behaviour (attention problems and aggressive behaviour).
At 10 years, parents completed the CBCL 6–18, while teachers were provided with a Teacher Report Form (TRF) 6–18 (Achenbach et al., 1991; Verhulst and Van der Ende, 2013). Teachers were approached through the parents and were aware of the medical background of their pupil. Each questionnaire consists of 120 items describing the behaviour of school-aged children. Parents and teachers answered the questions on the above mentioned three-point Likert scale as in the CBCL 11/2–5. Based on their answers, eight syndrome scales were calculated: anxious/depressed behaviour (is afraid to go to school), withdrawn/depressed behaviour (there is very little he/she enjoys), somatic complaints (physical problems without known medical cause), social problems (clings to adults), thinking problems (cannot get his/her mind off certain thoughts), attention problems (fails to finish things he/she starts), rule-breaking behaviour (lying or cheating) and aggressive behaviour (gets into many fights). Together the syndrome scales form a total problem scale and two subscales, including internalizing problem behaviour (anxious/depressed behaviour, withdrawn/depressed behaviour and somatic complaints) and the subscale externalizing problem behaviour (rule-breaking behaviour and aggressive behaviour).
At both ages, age-standardized t scores were obtained based on the percentiles of the distribution of the raw scores. Higher scores indicated higher levels of problem behaviour. For the syndrome scales, t scores between 65–70 were considered borderline-clinical and t scores >70 indicated clinical behavioural problems. For the total problem, internalizing and externalizing scales, t scores between 60–75 indicated borderline-clinical and t scores >65 indicated clinical behavioural problems (Achenbach and Rescorla, 2001; Verhulst and Van der Ende, 2013).
Besides the items that need to be answered on a three-point Likert scale, the CBCL and TRF provide parents and teachers with two open-ended questions: ‘What concerns you most about your child?’ and ‘Please describe the best aspects of your child’.
Statistical analyses
Statistical analyses were conducted using SPSS (Version 23.0, IBM, Armonk, NY, USA). To assess whether a selective loss to follow-up occurred, the perinatal factors of children with and without follow-up were compared using chi-square or Fisher exact (when the observed count was <10) tests for categorical variables and the t test for continuous variables. Descriptive statistics were computed as median and interquartile range (IQR) and proportions (n, %). To test whether there were differences in t scores between the two ages and between parents and teachers, a Wilcoxon signed-rank test was conducted, due to the non-normal distribution of the data. A p value <.05 was considered statistically significant. Answers to open-ended questions were analyzed at two and ten years of age through the standard for qualitative research (O’Brien et al., 2014). They were first transcribed and then analyzed using the thematic content analysis method (Hsieh and Shannon, 2005). The statements of parents and teachers were coded inductively by themes, which were originally simultaneous, but independently, developed by two investigators (LJ and JK). Themes and coding definitions were further developed, agreed upon and altered by the same two investigators using the thematic qualitative content analysis method. A third investigator was involved in case of discrepancies between coding and resolved through consensus. When statements contained more than one theme, the themes were coded separately. Frequency was calculated for each theme. Finally, themes were grouped into clusters, capturing the broader scope of a group of themes.
Results
A cohort of 113 very preterm children born <32 weeks’ gestational age who had been admitted to the tertiary neonatal intensive care unit between May 2006 and November 2007 were included. Completed parental questionnaires at 2 and/or 10 years were available for 92/113 (81%) children, including 62 (67%) children at both ages (see Supplementary Material for the derivation of the study population). Teacher questionnaires were available for 75/113 (66%) children. There were no differences in clinical parameters between children with a behavioural assessment and those without. Baseline characteristics of the participating children, of whom 58% were boys, included a median gestational age of 28.9 weeks (IQR: 4.1) and a median birthweight of 1120 g (IQR: 548).
Quantitative behavioural assessment
At 2 and 10 years of age, parents reported comparable numbers of children, 17/78 (22%) vs. 16/75 (21%) with borderline-clinical externalizing problems. The number of children with borderline-clinical internalizing problems, however, tripled from 8/78 (10%) at 2 years to 24/75 (32%) at 10 years. This was a statistical significant increase, Z = −2.942, p = .003. Comparing parental and teacher ratings at 10 years, similar mean internalizing and externalizing scores were found, Z = −1.5531.607, p = .120 and Z = −.281, p = .779, respectively.
Qualitative parental assessment of daily life experiences
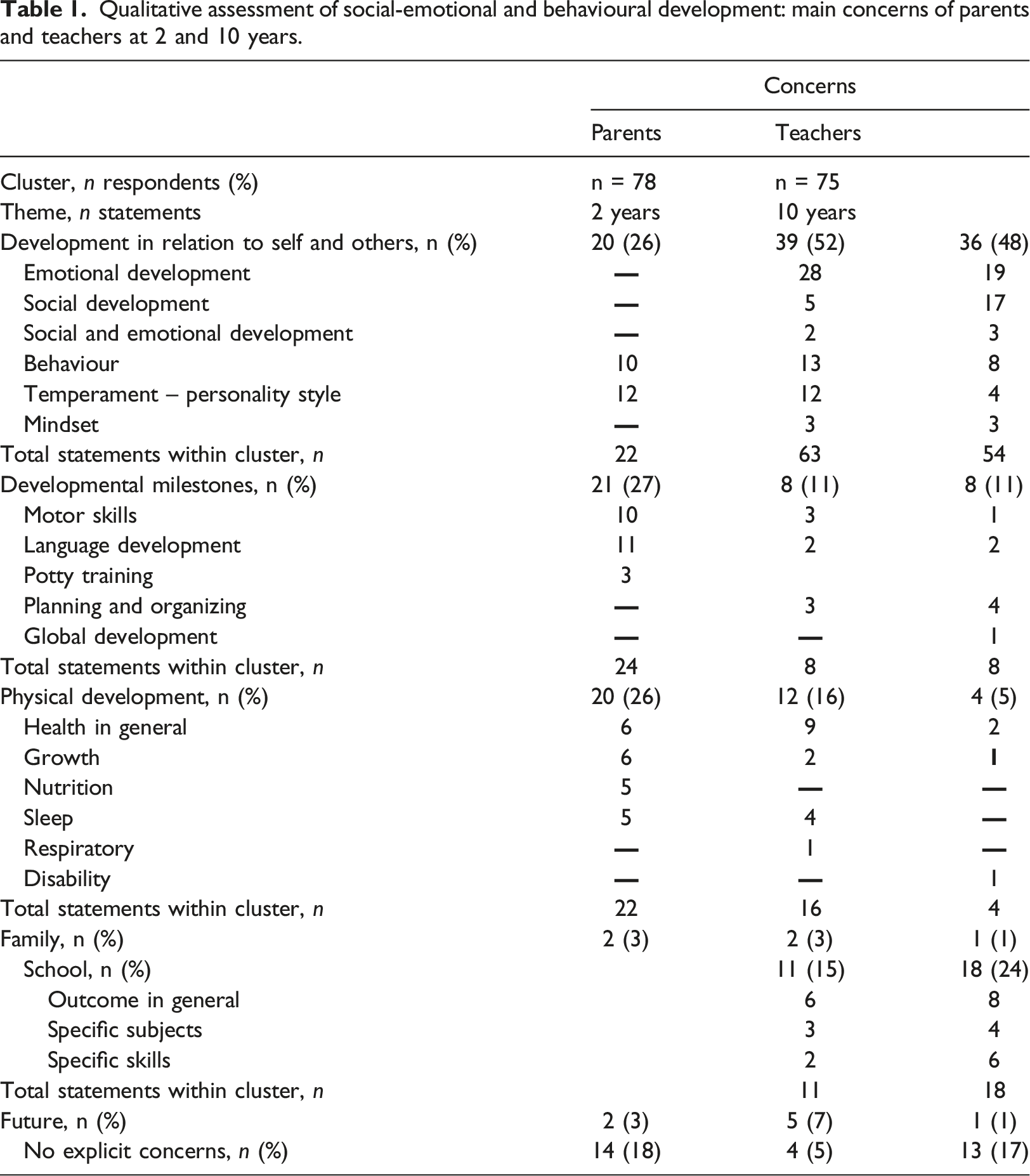
Qualitative assessment of social-emotional and behavioural development: main concerns of parents and teachers at 2 and 10 years.
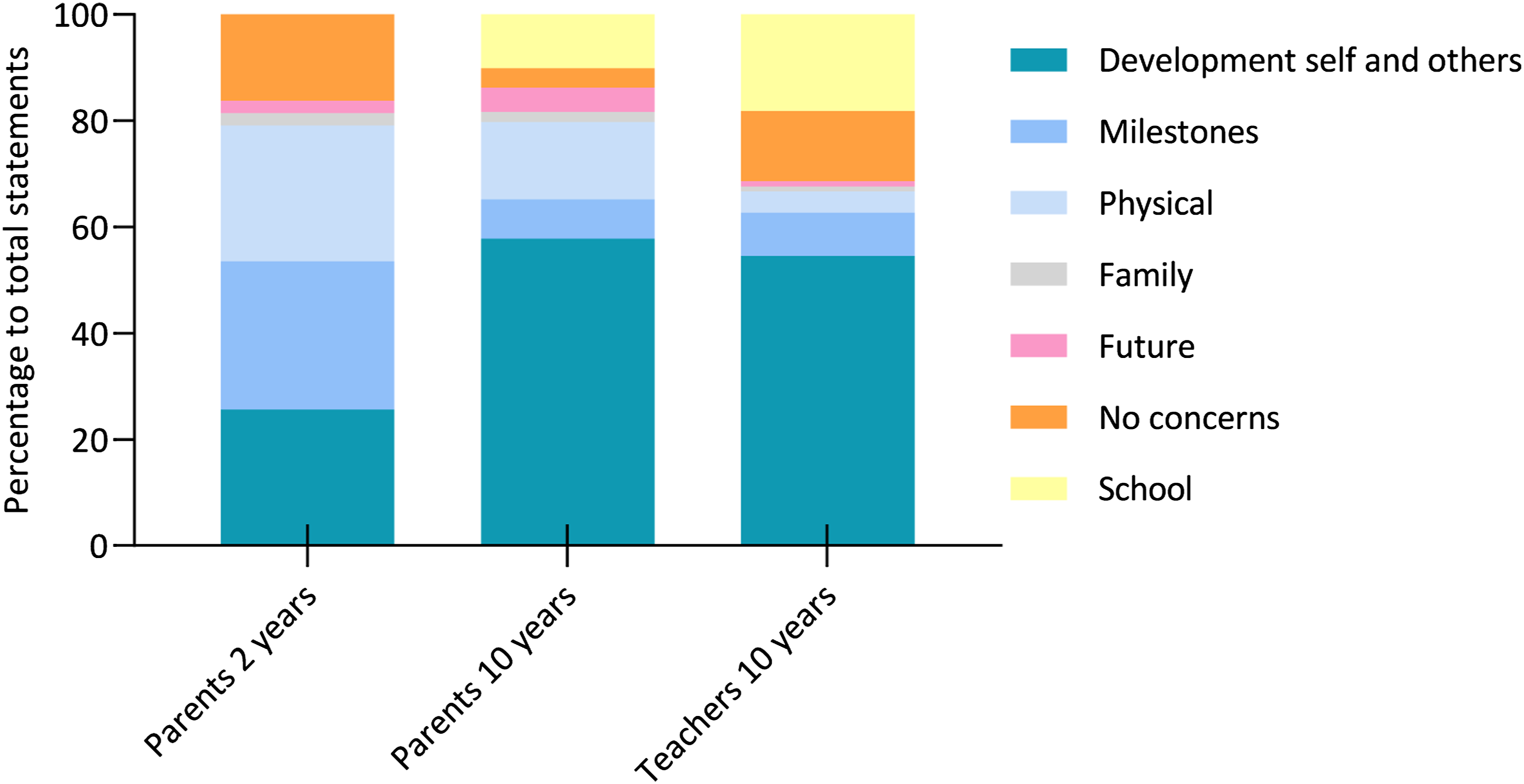
Statements of concern per cluster of parents and teachers.
Parents’ main concerns at the 2-years assessment
At 2 years, 78 parents made 72 statements describing their concerns. These statements were grouped into nine themes and five clusters, which captured the broader scope of a group of themes. Parents reported three main clusters of concern: Developmental Milestones, with 21/78 (27%) parents making 24 statements, Development in Relation to the Self and Others, with 20/78 (26%) parents making 22 statements and Physical Development, with 20/78 (26%) parents making 22 statements.
Developmental Milestones captures three underlying themes that relate to important cognitive and motor milestones in toddlerhood: 11/24 (46%) statements related to language development and were expressed as, for example, ‘He hasn’t started talking yet’, 10/24 (42%) related to motor skills, for example, ‘He still falls a lot while walking’ and 3/24 (13%) related to potty training, for example, ‘He has no interest in potty training’. In the Development in Relation to the Self and Others cluster, parents reported two themes: temperament, with 12/22 (55%) statements describing a child as stubborn, for example, ‘If he wants something, he is very persistent’, and behaviour, with 10/22 (45%) statements concerning tantrums, concentration problems and hyperactive behaviour. The Physical Development cluster captured four themes of concern: health in general (6/22 (27%) statements, e.g. ‘My child is susceptible to catching colds’), impaired growth (6/22 (27%) statements), nutrition (5/22 (23%) statements, e.g. ‘Eats small amounts’) and sleep (5/22 (23%) statements, e.g. ‘Not wanting to sleep on her own’). The two clusters, Family and Concerns about the Future, were mentioned least by the parents and considered the impact of a ‘broken home’ and, for example, ‘His development in the years ahead, will it continue to go well?’
Parents’ main concerns at the 10-years assessment
There was an increase from 2 to 10 years in the number of parents who explicitly reported concerns regarding their child’s development. While 64/78 (82%) parents expressed concerns at 2 years, 71/75 (95%) expressed concerns at the 10-years assessment. At 10 years, 75 parents made 101 statements that related to 18 themes and 6 clusters. The main cluster of concern was Development in Relation to the Self and Others, with more than half of the parents, 39/75 (52%), reporting on one or more of the six underlying themes in 73/101 statements. This is twice the number compared to the 2-years assessment (20/78 parents, 26%). The underlying theme emotional development (28/73 (38%) statements) included, for example, ‘His insecurity reflects in having many difficulties with his schoolwork’ and ‘His self-image is very low’. Regarding the theme behaviour, concentration problems were parents’ main concern (13/73 (18%) statements), for example, ‘Because of his lack of focus, he is not able to give his best’. Twelve (16%) statements were related to the theme personality style (or temperament, at the 2-years assessment) and included perfectionism, for example, ‘She sets the bar very high for herself and is not easily satisfied with her efforts’ and high sensitivity, for example, ‘She is very sensitive, she doesn’t respond well to loud noises and cries easily’. Fewer statements related to the three underlying themes social development, 5/73 (7%), for example, ‘Making first contact with peers’, (negative) mindset, 3/73 (4%), for example, ‘His negative thinking’ and social-emotional development in general, 2/73 (3%). The Physical Development cluster covered 15 statements that expressed concerns relating to four themes: general health (8/15 (53%), e.g. ‘She often does not feel well’), sleeping problems (4/15 (27%), e.g. ‘Has difficulties going to bed’), growth (2/15, 13%) and respiratory problems (1/15 (7%)).
A new cluster at 10 years, School, contained 11 statements that were grouped into three themes: 6/11(55%) concerned general, 3/11 (27%) concerned specific learning (dis)abilities, for example, ‘Unable to remember math and spelling rules’ and 2/11 (18%) statements regarding their child’s attitude towards school, for example, ‘She doesn’t want to go to school’. In contrast to parents’ perspective at the 2-years assessment, statements of concern within the cluster Developmental Milestones were made less often, 24/72 (27%) vs. 8/101 (8%), respectively. At 10 years, the cluster captured three underlying themes: language development (2/8 (25%), e.g. ‘Has a speech delay’), motor skills (3/8 (37%), e.g. ‘Playing sports’) and the new theme planning and organizing (3/8 (37%), e.g. ‘His ability to independently organize his activities’). As was the case at 2 years, at 10 years, the clusters Family and Concerns about the Future were mentioned least often.
Parents’ perspectives on the best aspects of their child at 2 and 10 years
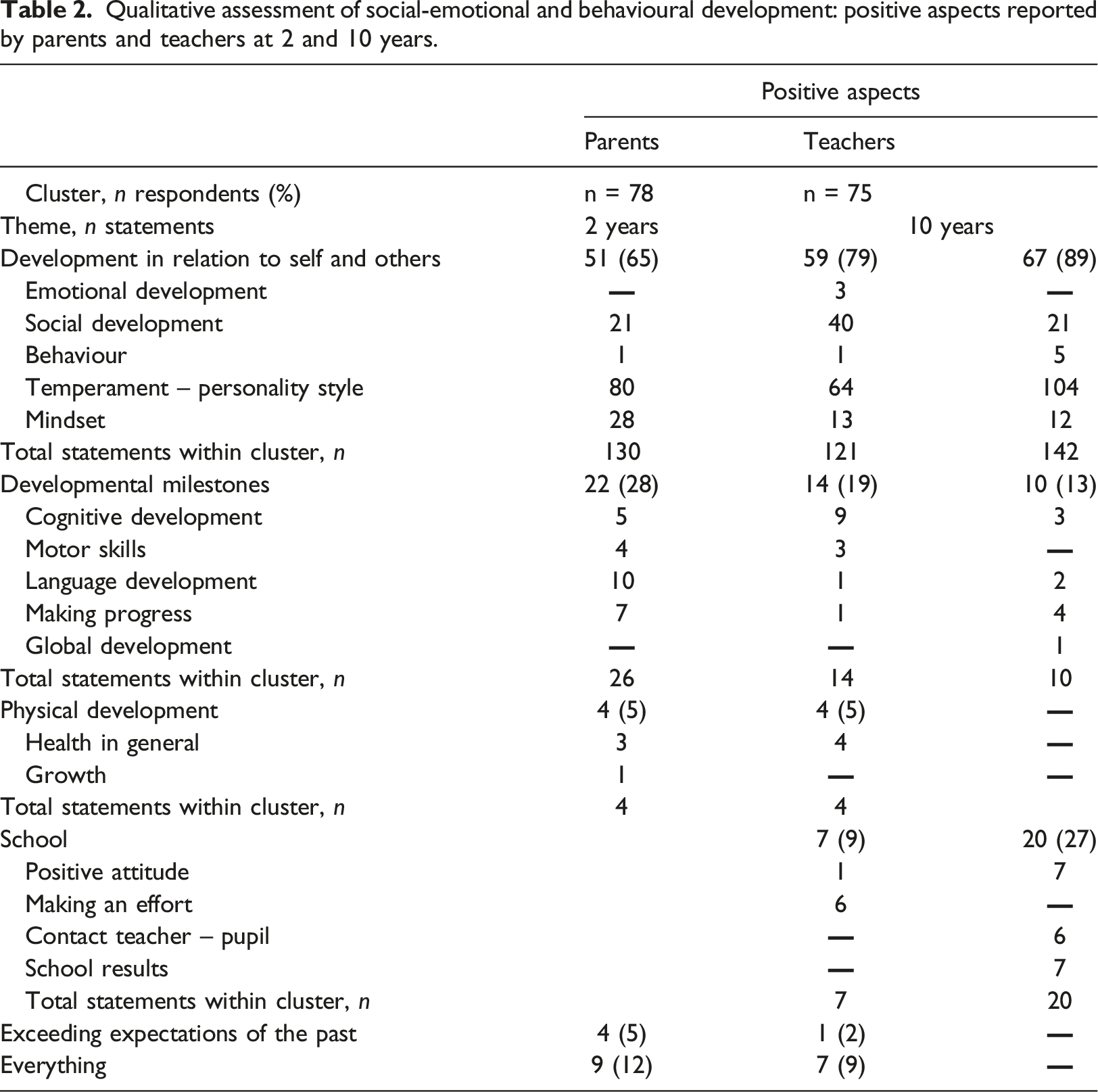
Qualitative assessment of social-emotional and behavioural development: positive aspects reported by parents and teachers at 2 and 10 years.
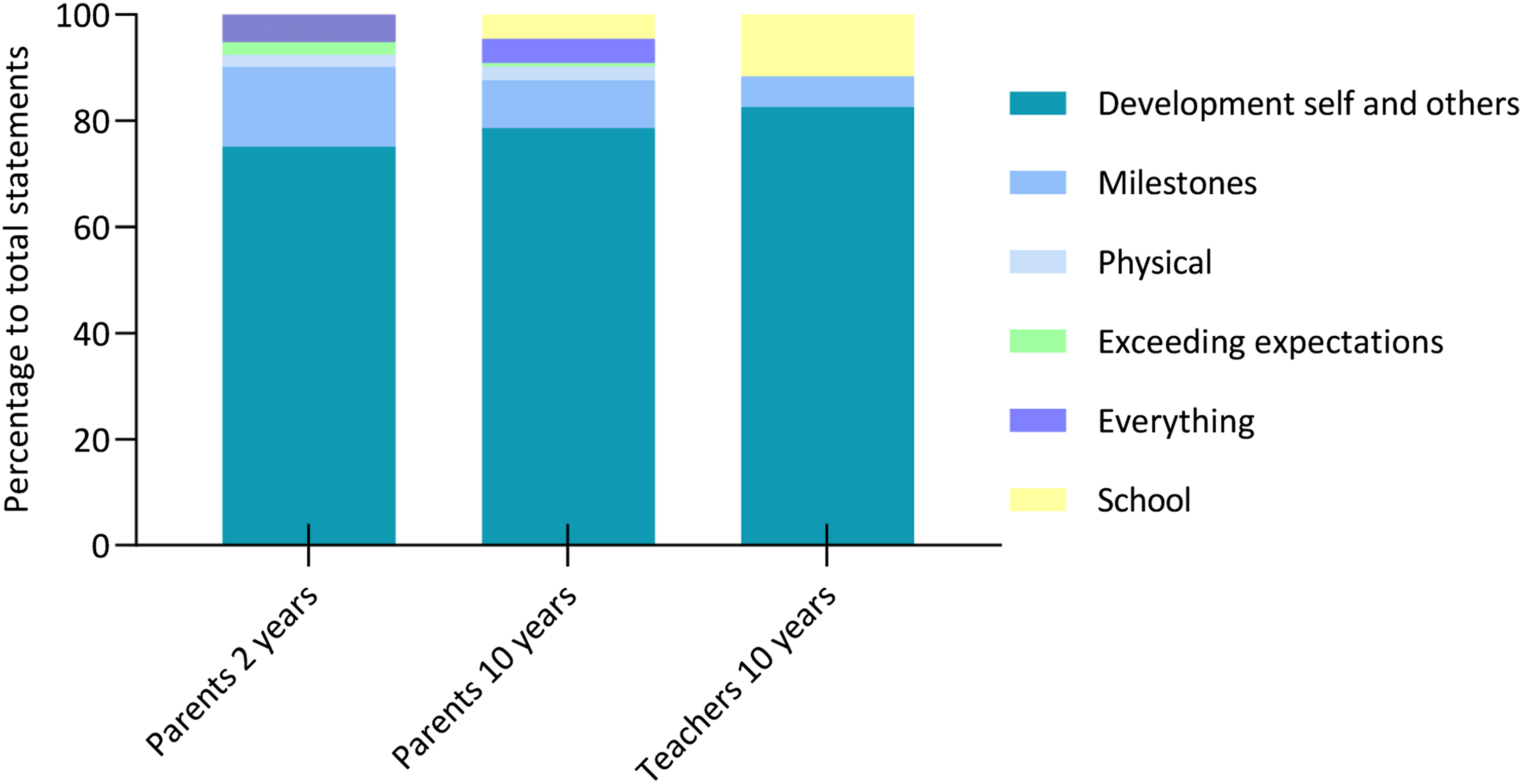
Positive statements per cluster as reported by parents and teachers.
Comparing parents’ and teachers’ perspectives at 10 years: concerns and best aspects
When comparing the parents’ and teachers’ perspectives (Table 1 and Figure 1 (Supplementary Material)), more teachers explicitly mentioned not having any concerns about their pupils, 13/75 (17%) as opposed to 4/75 (5%) parents. The main cluster of concern for both parents (39/75, 52%) and teachers (36/75, 48%) was Development in Relation to the Self and Others. However, parents’ and teachers’ statements related to different themes. Teachers had more concerns relating to the theme social development, 17/54 (32%) vs. 5/63 (8%) statements and mentioned a lack of social skills, for example, ‘He’s a bit awkward, socially’ and ‘He has trouble reading social cues’, whereas parents were more concerned about their child’s emotional development, for example, ‘Her self-image’ and ‘His insecurity’. Compared to parents, teachers reported more concerns within the cluster School, with 18 teachers making 18 statements relating to three themes. Academic achievement in general was the main theme, for example, ‘He has more difficulties understanding school assignments compared to his peers’ and ‘Her effort and school results do not match’. Concerns relating to the cluster Developmental Milestones were mentioned equally often, 8/75 (11%) by teachers and parents, where teachers were most concerned about their pupil’s ability to plan and organize their schoolwork, for example, ‘Difficulties to start schoolwork and also to finish his work’.
Regarding the parents’ and teachers’ perspectives on the best aspects of their child/pupils (Table 2 and Figure 2 (Supplementary Material)), the main cluster for both parents, 59/75 (73%) and teachers, 67/75 (84%) was Development in Relation to the Self and Others with 121 and 142 statements relating to four themes, respectively. Most statements of both parents, 64/121 (53%), and teachers, 104/142 (73%), concerned the theme personality style. Teachers mainly praised their pupils’ willingness to work hard, while parents mostly mentioned characteristics related to the self, for example, ‘He/she is very sweet/a go-getter’. Positive aspects within the cluster School were mentioned more often by the teachers, 20/75 (27%) vs. 7/75 (9%). Teachers praised their pupils’ positive attitude towards schoolwork and the positive interactions with their pupil more often, while parents mentioned the effort their child made at school more often, for example, ‘He is very serious about school and likes to get good marks’.
Discussion
To enhance knowledge on the social-emotional and behavioural development of children born very preterm, this study provided in-depth qualitative information on what parents experience on a day-to-day basis during two different developmental stages (2 and 10 years of age), including both concerns and positive aspects. Due to the importance of multiple informants, the teacher perspective was incorporated at 10 years of age. At 2 years, parental concerns were equally divided between the clusters Developmental Milestones, Development in Relation to the Self and Others and Physical Development. The main concern at 10 years of age related to the cluster Development in Relation to the Self and Others, for both parents and teachers. However, underlying themes differed, with teachers reporting more social difficulties. Even though the cluster Development in Relation to the Self and Others was the main cluster of concern at 10 years, it was also the main cluster relating to positive statements at both 2 and 10 years of age. These findings add to our understanding of the social-emotional and behavioural development of very preterm-born children, as they give insight in what parents and teachers struggle with most in daily life and over time.
Behaviour in preterm children has been mainly studied through behavioural questionnaires, showing for example, that already at 6 years of age, preterm children have more behavioural problems compared to their term-born peers; a difference that remains stable throughout their school career (Linsell et al., 2019). This leads to a 3-to 4-fold higher risk for a range of psychopathology (Johnson and Marlow, 2011). Currently, the co-occurrence of increased emotional symptoms, hyperactivity/inattention and social difficulties is described as the ‘preterm behavioral phenotype’, in order to distinct the risk, but also the aetiology, from the broader paediatric population (Fitzallen et al., 2020). About 20% of children born preterm experience behavioural difficulties in line with the preterm behavioural phenotype (Burnett et al., 2019). These sorts of behaviours are imaginably challenging for caregivers, but little is known on what they truly experience on a day-to-day basis.
Qualitative research in relation to preterm birth has gained attention over the past decades, especially concerning parental experiences during the period at the neonatal intensive care unit (Provenzi et al., 2016; Arnold et al., 2013) and after early intervention programs (Kyno et al., 2013; Baraldi et al., 2020). Qualitative studies after this period are scarce, potentially leading to missing outcomes that are important and meaningful to caregivers of preterm-born children (Janvier et al., 2016).
In line with Jaworski and colleagues (2018), we found that at 2 years, the cluster Developmental Milestones was the main topic of concern and just as often mentioned as the most positive aspect of (the development of) the child. It might be that, even though parents are worried whether their child will reach age-appropriate milestones, they are also happy with how their child is developing after their stay at the neonatal intensive care (Vohr et al., 2000).
Compared to the quantitative data at the 2-years assessment, externalizing behaviour was reported most by parents. High scores of behavioural traits such as stubbornness and disobedient behaviour might be in line with the normative peak of physical aggressive behaviour, that increases in the second year of life (Alink et al., 2006). However, externalizing behavioural problems were not the main reason for concern at 2 years of age as mentioned by parents. This underlines the importance of looking beyond the numerical outcomes of a behavioural questionnaire.
At 10 years of age, parents reported quantitatively more internalizing behaviour, including anxious and depressed behaviour, which also showed in their answers to the open-ended questions. The mentioned themes became more complex at 10 years and included concerns regarding the child’s emotional well-being, such as a sense of insecurity. Since children generally start their school careers in the Netherlands at 4 years of age, themes related to school were only mentioned at 10 years of age. School is however often not included by behavioural questionnaires, even though behavioural difficulties and school attainment are intertwined (Burnett et al., 2019).
Because of the effect that very preterm birth might have on behaviour and school performance, teachers are a valuable source of information. There were substantial differences in what teachers mentioned as their main concerns and pupils’ best aspects. Not surprisingly, the answers of teachers were more often related to school and academic outcomes. Even though the main cluster of concern was similar to parents at 10 years (Development in Relation to the Self and Others), the underlying themes differed. Teachers were more concerned about a lack of social skills of their pupils leading to difficulties in interactions with their peers. It could be that parents overestimate the social abilities of their child, because they are less confronted with how their child behaves with peers, while teachers have many opportunities to observe their pupils in interaction with others.
In the Netherlands, standardized follow-up of very preterm-born children ends at 8 years. With increasing age, however, there appears to be a continued and perhaps even more urgent need for help and reassurance on whether a child is capable of taking care of itself in the future. For example, Dutch preterm-born adolescents were more often unemployed, not enrolled in any educational program, and boys and girls alike showed more difficulties in establishing social contacts compared to their peers (Bruin et al., 2015). This stresses the need for long-term follow-up, even after school age, to increase the understanding of the difficulties very preterm-born children face, and to provide adequate support.
The underlying themes temperament and social development, of the cluster Development in Relation to the Self and Others, were mentioned most related to the best aspects of a child at both ages. Considering the amount of statements made, it seemed quite easy for parents to recognize and mention the positive traits of their child. There was a clear decrease between 2 and 10 years in how often parents mentioned their child’s positive mindset, with parents describing their child much more often as happy, vibrant and lively at 2 years. High rates of a positive mindset in young children have also been found in other studies (Jaworski et al., 2018).
Limitations
Due to the original design of the study in 2006–2007 (investigating brain imaging findings in an unselected cohort of children born very preterm), no sample size or power analysis was performed for loss to follow-up at two and 10 years of age. Because of the relatively large time interval between the two follow-up points, we decided not to implement multiple imputation for missing variables. This has led to a relative small sample, with data of 62 children available at both 2 and 10 years of age. Another limitation of this study was the lack of a healthy term-born control group to assess whether the themes mentioned by parents were specific to preterm-born children, or more universally related to developmental stages.
Implications for practice
Social-emotional and behavioural development is not always included in follow-up studies after very preterm birth. Having a child without any physical concerns or intellectual problems, but with severe behavioural issues, can be equally challenging to the family in which the child is raised (Janvier et al., 2016). For clinicians working with very preterm-born children, it is important to bear in mind that the numerical outcome of a behavioural questionnaire does not always cover the full experience of parents. Structured interviews might be a valuable addition to the use of questionnaires, as is the use of multiple informants to assess social-emotional and behavioural development to the full extent. Besides generating attention to the reported concerns, it is important to ask parents about their child’s successes and to celebrate these with parents. For future research, it would be interesting to add the perspective of the children themselves. Although studies have shown that self-reports of preterm-born adolescents do not show higher rates of problem behaviour compared to controls (Taylor et al., 2015; Saigal and Doyle, 2008), thematic analysis of their answers to open-ended questions might show more concerns and/or in different areas compared to their peers. Considering the found differences in concern, teachers form a valuable source of information. This study showed that children born very preterm more often experience difficulties with their social skills, making them a possible target group for intervention focused on the development of social skills.
Conclusion
Children born very preterm are prone to develop social-emotional and behavioural difficulties. Parents of very preterm-born toddlers often worry on whether their child will be able to reach age-appropriate milestones, their child’s behaviour and general health. As their child grows older, the concerns of parents shift to a complex field of topics intertwined with personality, behaviour and mindset. For teachers, most concerns are related to their pupils’ emotional well-being, social interaction and academic attainment. This underlines the inability of behavioural questionnaires to cover the full range of experiences of caregivers as well as the importance of multiple informants. The incorporation of parental perspectives regarding their main concern and their children’s best aspects within follow-up assessments will provide valuable information for clinical practice that could lead to a better understanding of very preterm-born children.
Supplemental Material
Supplemental Material - Social-emotional and behavioural issues after very preterm birth: Parental and teachers experiences
Supplemental Material for Social-emotional and behavioural issues after very preterm birth: Parental and teachers experiences by Lisette Jansen, Sylke Steggerda, Monique Rijken, Andrea van Steenis, Linda S de Vries, Cacha Peeters-Scholte, Robert Vermeiren and Jeanine van Klink in Journal of Child Health Care
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Cacha Peeters-Scholte is founder and consultant at Neurophyxia BV. She holds several patents and stocks of Neurophyxia BV. None of this work has a relationship with the current manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Sylke Steggerda received a grand from Chiesi Ltd. for the PROUD study (PReterm brain injury, long-term OUtcome and brain Development study).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.