
Abstract
Calculating the correct medication dosage for pediatric patients can be difficult for nurses to determine, as the pediatric dose is typically a small fraction of the adult dosage. This study aims to examine the impact of the Triangle Technique on the ability of nursing students to calculate low and high safe dosage ranges in children. To evaluate how this educational tool could improve a nurse’s skill in this area, a quasi-experimental pre-/post-test research design was employed including one hundred fifty-eight third-year nursing students. The Pediatric Medication Administration Form and Pediatric Safe Dosage Calculations Quiz (PSDCQ) were used to measure the effectiveness of the Triangle Technique. While <50% (n < 79) of students gave correct answers to each question in PSDCQ before this intervention, all of the participants (N = 158, 100%) gave a correct answer to one question, and >89.2% (n > 141) of the students correctly answered the other four questions of PSDCQ. The change in scores (pre-PSDCQ median score = 0, IQR = 60; post-PSDCQ median score = 100, IQR = 0) post-intervention was statistically significant (z = 10.633, p ≤ .001), indicating that this teaching technique was effective for improving students’ ability to calculate pediatric safe dose ranges. Nursing students (n = 144, 91.1%) were satisfied with using Triangle Technique. Using the Triangle Technique can increase nursing students’ understanding of how they calculate safe pediatric medication dosages.
Keywords
Introduction
Drug dosage calculation skills for nurses and student nurses are the most critical function for ensuring patient safety (Cheragi et al., 2013; Wright, 2012). Errors in drug dosage calculation are the most common medication mistake in pediatric and neonatal units (Cheragi et al., 2013), and this type of mistake plays a key role in threatening patient safety, and can cause drug administration error rates, overdose, toxic reaction, and even death (Westin et al., 2015). Calculating correct dosage can be difficult in pediatric patients, as they may require only a fraction of the adult dosage (Aneja et al., 1992; Lesar, 1998, 2003; Tisdale, 1986). Unlike adult patients, distribution of medication may be altered in infants and young children due to several reasons, including: higher gastric pH relatively during the neonatal period, increased gastric emptying and shorter intestinal transit time in neonates and young infants, decreased plasma protein in newborns and early infancy, a higher percentage of body water than adults, faster extracellular fluid exchange, decreased body fat, decreased amount of plasma proteins for drug binding, and undeveloped blood-brain barrier, allowing permeation by medications, increased hepatic blood flow due to larger liver relative to body mass which cause highly metabolized drugs, and delayed maturation of glomerular filtration rate which cause reduced renal clearance (Stucky ER, 2003; Hodges, 2018; Woo, 2004). Thus, children respond to pharmacodynamics and handle pharmacokinetics medicines differently and they are more sensitive and prone to possible medication errors (Wright, 2006).
Correct pediatric dosage calculation is a major component of medication administration, and a systematic literature review found that median rate of medication administration errors in children was 14.6 per 100 medication orders and between 6.4 and 9.1 per 1000 patient-days (Ameer et al., 2015). To calculate the correct dosages for pediatric patients, two methods are used: the more common one is based on the unit of drug per kilogram of body weight, while the other uses body surface area (Wong et al., 2019). Using body weight method alone increases the risk of drug miscalculations, leading to subsequent medication administration errors. This shortcoming of the method has been documented (Lesar, 2003), suggesting that nurses should be trained to calculate the low and high safe dosage range.
Literature
Mathematical competence and accurate drug dosage calculations are essential to providing a safe healthcare environment, which includes preventing medication errors (Simonsen et al., 2014). In literature, there are various studies focused on nursing students’ drug calculation skills and different strategies for developing them.
Although there are studies on pediatric safe drug dose calculations in the literature, there are few studies on techniques used in teaching this subject to students. There is a need for studies in which teaching techniques that will provide effective learning are tested. Most of the studies indicate that nursing students’ drug dosage calculation skills are generally poor (Brown, 2002; Caboral-Stevens et al., 2020; Mansouri et al., 2013; Özyazıcıoğlu et al., 2018; Ramjan et al., 2014; Westin et al., 2015; Wright, 2006). In a study by Brown, whose sample was composed of 118 nursing students, student math skills were inadequate (Brown, 2002), and in a study by Grandell-Niemi et al., which included 282 nursing students, the results showed that instructions for drug dosage calculation were insufficient (Grandell-Niemi et al., 2006). Harvey et al. found that only 19% of 304 incoming nursing students passed a competency test that assessed basic math abilities, including arithmetic, decimals, units, and fractions (Harvey et al., 2010). A study by Özyazıcıoğlu et al. (2018) found that most failed areas have found out to be related to the problems of safe dose, drug dosage calculations, and four operations. In the same study, 30.4% of the students failed to calculate the safe dose range. Mansouri et al. (2013) stated that nursing students make errors in dosage calculations (17.4%–37.7%).
There are published studies looking at the techniques for teaching dosage and calculation to nursing students (Coben and Weeks, 2014; Middleton, 2008). Nurses need to graduate with adequate medication competence, so to improve this skill, it is necessary to find effective teaching techniques, and to assess them as appropriate for nurse education programmes (Dilles et al., 2011; Grandell-Niemi et al., 2006; Ramjan et al., 2014). Wright (2005) has outlined in a study a spiral method that has explored the most effective strategies for teaching drug calculation skills to student nurses. The stages of Wright’s study are represented as a spiral, which includes the importance of practice and establishes—the need to research, collect, and analyse data; and search for significant patterns and insights to develop hypotheses, followed by gathering more data to—further build on your hypotheses, introduce change in practice, and continuing to gather more data. (Bruner, 1960). A study by Özyazıcıoğlu (2018), was conducted to evaluate the students’ knowledge of pediatric dosage calculations in which they were given open-ended questions, known as classic method. In the same study in which classic method was used, direct expression technique and ratio-proportionality were used in dose calculation.
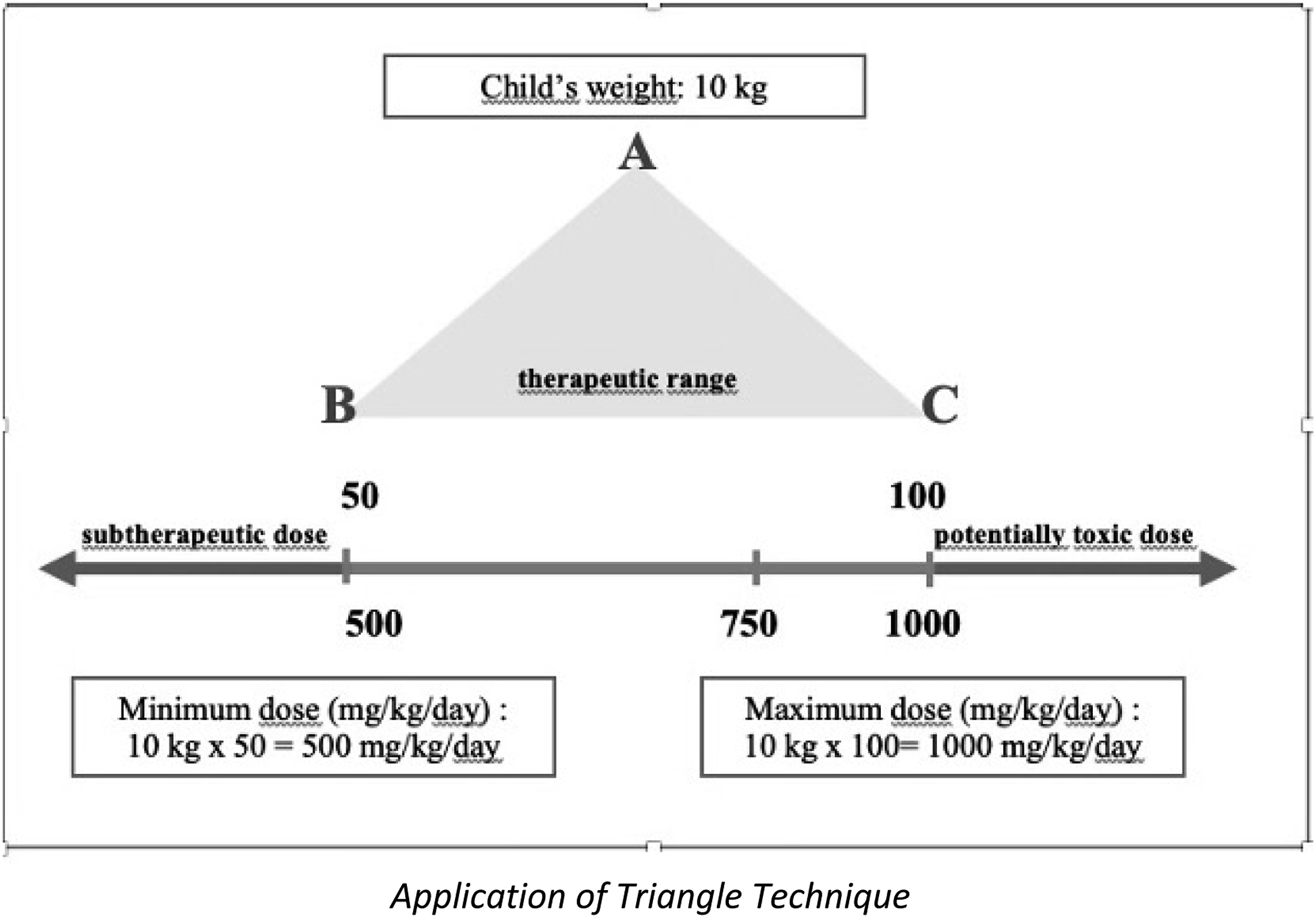
Sredl’s study evaluated the effectiveness of the “Triangular Technique,” in which nursing students were required to use symbolic imagery, where they were asked to enter patient weight at the pinnacle of the mountain, imagine the base of the triangle as a river flowing from west to east (left to right), write the normal therapeutic range on the right and left bases of the triangle, calculate the normal therapeutic range for the child’ weight, and place both values at each end of the line. In this technique, if the value landed on the left side of the river, the students knew that the dose is subtherapeutic; if it landed on the right side of the river, they knew that it is potentially toxic (Sredl, 2006). The study included 30 nursing students; all of which were evaluated before and after the training on their ability to calculate safe pediatric drug dosage intervals. This study showed that students’ ability significantly improved following training in that method (Sredl, 2006).
The Triangle Technique for the computation of safe therapeutic-range medication dose estimates for pediatrics was developed as a response to student concerns about math anxiety and problems performing accurate computations prior to medication administrations (Sredl, 2006). The technique was developed according to evidence-based process by applying the results of research into the nursing student’s learning milieu, learning styles, and learning strategies (Sredl, 2006). Within the learning milieu, educators—especially educators of nursing students—must be sensitive to the learning styles of their students (Wright, 2004). A learning milieu promoting student empowerment by acknowledging competency is likely to lead to greater retention and application of the material.
Individuals interpret their environment by filtering information through three main sensory systems: visual, auditory, and kinesthetic (Fleming and Mills, 1992). The instructional design of the Triangle Technique, using visual analogy and imagery in explaining how to solve a mathematics problem while performing the mathematical computation on the blackboard, includes all three learning styles (Sredl, 2006).
Aim
To evaluate the effects of using the Triangle Technique as an educational tool for nursing students, in order to improve the calculation of pediatric dosages.
Research questions asked
• Do nursing students’ correct answers on the PSDCQ increase after teaching the Triangle Technique as an educational tool for calculating pediatric safe therapeutic-range medication dosages? • Is there a correlation between sociodemographics and correct answers on the PSDCQ? • What do nursing students think about the Triangle Technique as an educational tool for calculating pediatric safe therapeutic-range medication dosages?
Materials and methods
Research design and sample
A quasi-experimental single group pre-/post-test research design was employed.
Population/setting/sample size
This quasi-experimental study was conducted between November 2018 and June 2019. The current study employed pre-training and post-training evaluation in .........................The target population included third-year students enrolled in Bachelor of Science in Nursing (BSN) program. Inclusion criteria included students who were able to give consent and/or had pediatric drug calculation lessons to determine the pediatric safe dosage range formula. Exclusion criteria included students who were unable to give consent and/or had already taken the Pediatric Nursing Course and could not speak and understand Turkish very well.
Measures/instruments
The outcome measurements were evaluated using the Pediatric Medication Administration Form (PMAF), Pediatric Safe Dosage Calculations Quiz (PSDCQ), and Satisfaction Form with the Triangle Technique (SFTT), developed by researchers following literature review.
Procedure
We used a three-phase process: pre-education; education; post-education.
How triangle technique works—an example
A child weighing 22 lb (10 kg) is to receive cefuroxime (Ceftin) 250 mg every 8 hours. The normal therapeutic range is 50–100 mg per kg of body weight for children. Write “50 mg” on the line indicating the base of the mountain on the left (B), and “100 mg” on the same line to the right (C). Then draw a line with arrows at both ends just below the base of the mountain. Calculate the normal therapeutic range for a 10 kg child: 10 × 50 mg = 500 mg and 10 × 100 mg = 1000 mg. Place these values at each end of the line. To calculate how much your patient should receive in 24 h, multiply the ordered dosage (250 mg) by the number of times it is to be administered—in this case, three times a day. Three dosages x 250 mg = 750 mg. Apply the result of the calculation (750 mg) to the river at the base of the mountain to see where it fits. It fits between the 500 mg on the left and the 1000 mg on the right. From a quick visual assessment, it is apparent that the dosage is within pharmaceutically accepted parameters and therefore, is safe (Application of Triangle Technique appears in the supplementary material).
Ethical considerations
Official permission for the study was obtained from Gulhane Faculty of Nursing, and ethical approval was obtained from the ethics committee (18/294-46418926).
The participating students received written and verbal information about the study. They were informed that all data would be treated confidentially, and to protect participant identity, pseudonyms would be used. Further, because participation or nonparticipation was both voluntary and anonymous, students were assured their course grades would not be affected and were guaranteed that they could withdraw their participation whenever they wanted. The students signed consent forms.
Data analysis
Data were analyzed using the IBM SPSS (Version 23.0, IBM Corporation, Armonk, NY, USA). Median, the Interquartile Range (IQR), mean, standard deviation (SD), percentage, and frequency were used for descriptive statistics. Changes in each of the eight items in the pre- and post-PMAF were evaluated with the McNemar–Bowker Test. Normality for the scores of PSDCQ was checked by using the Kolmogorov–Smirnov test. Answers to individual questions on PSDCQ were coded in SPSS as correct (20 points) or incorrect (0 points). To compare scores of those who had attended traditional high schools versus science-based high schools was calculated using the Wilcoxon Signed Ranks test and Mann–Whitney U test. The level of statistical significance was set at p < .05.
Results
Comparison of correct answers by nursing students pre- and post-PSDCQ (n = 158).

Note: IQR: The Interquartile Range.
aWilcoxon test.
Knowledge and attitudes of students related to pediatric medication administration are presented in Figure 1. Pre-education, 63.3% (n = 100) of students agreed with this statement, “Pediatric drug dosage in children is calculated based on body weight”; 50.6% (n = 80) of them disagreed with “I know how to convert units of measurement”; and 56.3% (n = 89) of them partially agreed with “I know that when calculating the pediatric drug dosage, it should be prepared by taking into account the dry powder volume.” After education, 42.4% (n = 67) of students partially agreed with this last statement, and 29.1% (n = 46) disagreed with it. Moreover, post-education, 93.7% (n = 148) of respondents agreed with “Drug dosage in newborn babies is calculated based on body weight” (Figure 1). Knowledge and attitudes related pediatric medication administration for nursing students (n = 158).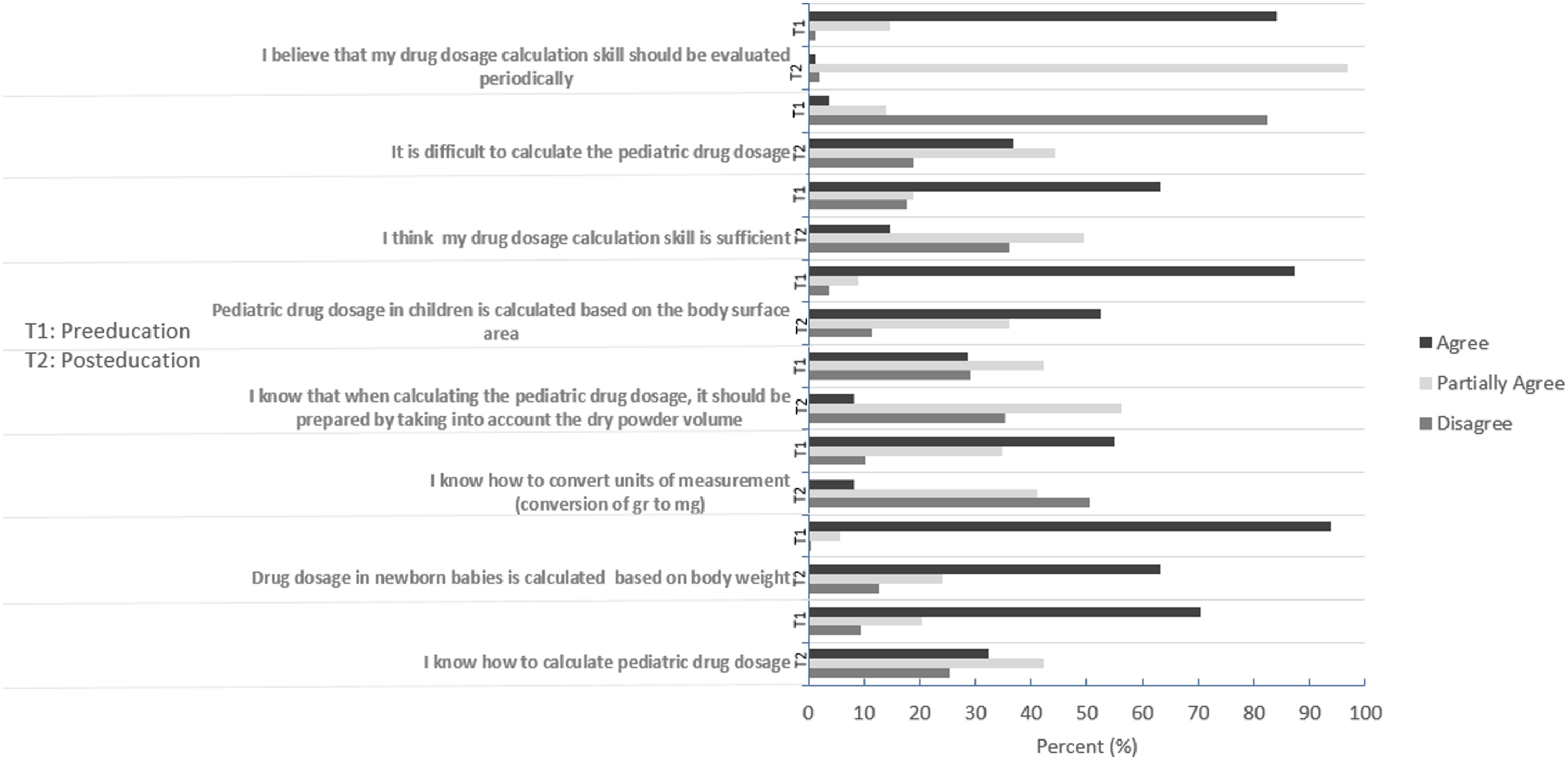
The distribution of quiz’ score across the participant variable and attitude to pediatric dosage calculation ability of the nursing students (n = 158).
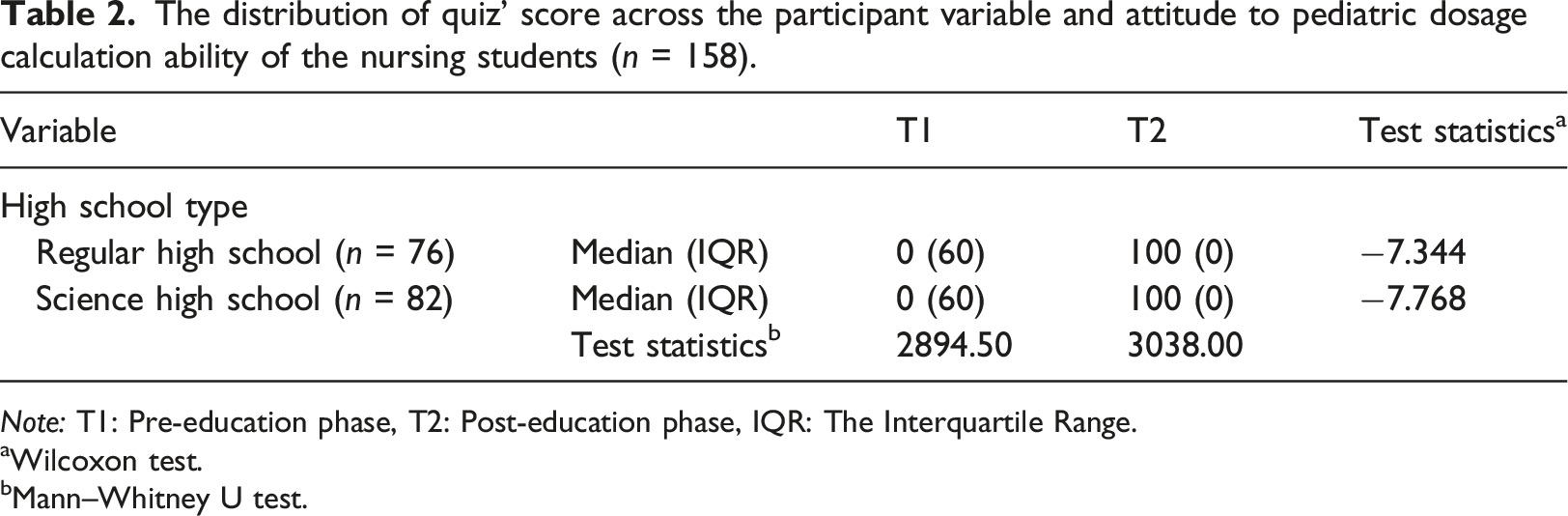
Note: T1: Pre-education phase, T2: Post-education phase, IQR: The Interquartile Range.
aWilcoxon test.
bMann–Whitney U test.
As shown in Figure 2, nursing students mostly expressed positive views on the Triangle Technique. More than 80% (n = 126) reported that they agreed with six of the seven statements that evaluated their opinions. Only the third item—“This approach enhanced my motivation”—had a lower score, with 75.9% (n = 120) of participants agreeing with the statement (Figure 2). Distribution of satisfaction with using Triangle Technique for pediatric safe dosage calculations (n = 158).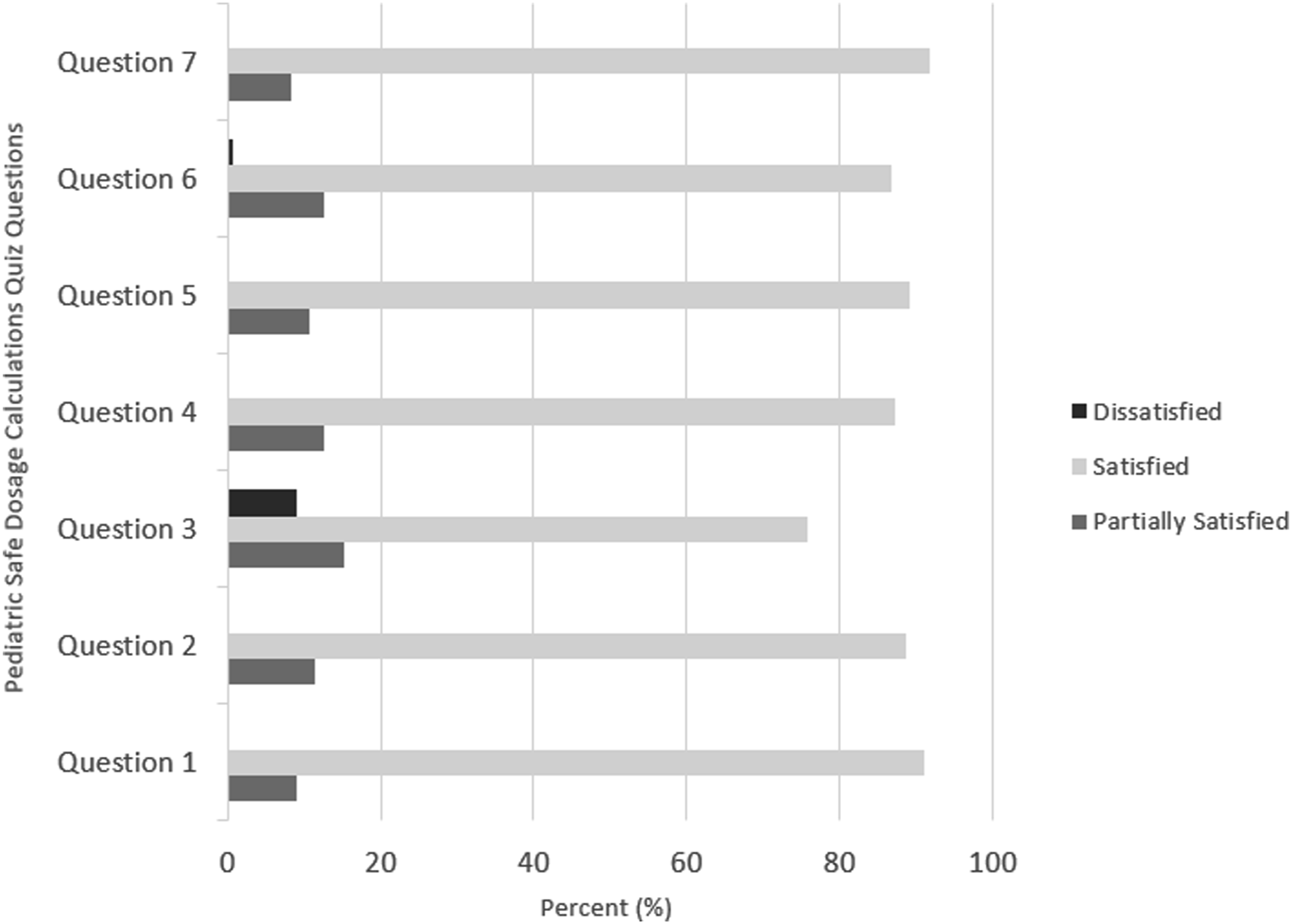
Discussion
This study aimed to evaluate the effect of using the Triangle Technique as an educational tool for nursing students to learn to accurately calculate pediatric dosages. Using the Triangle Technique, students’ ability to calculate pediatric safe dose ranges was improved aligning with the outcomes of the study by Sredl’s study which also used this technique (Sredl, 2006).
The theme and slogan of the 2017 World Health Organizations’s Global Patient Safety Challenge was entitled “Medication Without Harm” (Donaldson et al., 2017). This campaign focused on the fact that unsafe medication practices and medication errors are a major cause of avoidable injury across the globe. Nurses play a key role in ensuring medication safety, so pediatric nurses need to graduate from nursing programs having acquired drug dosage calculation skills for children, including babies (Guy et al., 2003). Differences in the organ development of children (hepatic enzyme systems and renal systems, delays in gastric emptying, decrease in bowel movements) may affect the metabolizing and discharge of the drug, especially in overdose medication. Therefore, it is critical to prevent medication errors.
Pre- and Post-PSDCQ
Nursing care involves not only accurate medication administration, but also knowledge and skill competency in calculating medications (Kohtz and Gowda, 2010). A number of studies illustrated that nursing students often have a poor ability to solve drug calculation tests (McMullan et al., 2010). McMullan et al., in their study with 229 second-year nursing students, found that 92% of students failed the drug calculation test (McMullan et al., 2010). Jukes and Gilchrist’s study with 37 second-year nursing students showed similar outcomes, with only three of them able to score 90% and above, suggesting that generally, students were unable to achieve 90% mastery (Jukes and Gilchrist 2006). Blais and Bath, in their study with 66 first-year nursing students, found that 89% failed drug calculation tests. They also showed that 68% of the errors made were related to conceptual errors (Blais and Bath, 1992).
Özyazıcıoğlu et al. (2018) showed that an exam question on the dosage calculation was based on child’s age, which is the most common method in pediatrics, and which ensures right dosages and drug dilution was answered wrong by 30.4% (n = 45) of nursing students. Wright (2005) found out that 36.7% of the students were not able to answer even half of the questions correctly; Simonsen et al. (2014) pointed that in questions on the administration of medication, error ratio of the students was 25%; and Stratton et al. (2004) revealed that incorrect dosage calculation ratio in the pediatric clinics is 31.4%. Macdonald et al. (2013) reported students answered 67% of the questions as “true” and 6% as “don’t know”; which is consistent with our findings. In their study, Mansouri et al. (2013) stated that nursing students make errors in preparing medicine for injection (11.5%–28.7%), and dosage calculations (17.4%–37.7%). The findings of our study align with these results, which show that prior to training, most of our students’ pediatric safe dosage calculation ability was inadequate.
As described in the literature, many studies have been conducted to develop effective teaching methods for setting up the problem. These methods include Triangle Technique, problem solving approaches, dimensional analysis, didactic methods of teaching, active learning, group activities with instantaneous feedback, PowerPoint, CDs, video instructions, online multimedia learning, and integrative approaches, such as the use of technology, computerized-learning, and in person activities to teach math (Ellis-Monaghan, 2010; Kelly and Colby, 2003; Sredl, 2006). To facilitate learning of pediatric safe dosage calculations and set up the calculation problem as something that could be visualized by nursing students, we used “the Triangle Technique.”
In our study, nursing students had higher PSDCQ scores after the intervention. This finding aligns with Sredl’s work on this technique, which she developed and reported as showing marked improvement in students’ post-test scores (Sredl, 2006). This would suggest that using effective teaching methods can improve pediatric safe therapeutic-range medication dosage calculations in nursing students. As in Sredl’s study, it was determined that the use of the Triangle technique is a valid and reliable method that allows students to get high scores in calculating safe pediatric drug dose ranges.
Acquiring the skill to calculate pediatric safe dosage calculations is vital for nursing students to bridge the gap between theory and practice (Chan, 2002). Wright, who wrote about the national debate on nurses’ drug calculation skills, has suggested that clinical practice should be integrated into theoretical curricula because these skills are best taught in the clinical arena (Wright, 2009). Similarly, Allen and Pappas (Allen and Pappas, 1999), and Wilson (Wilson, 2003) emphasized the link between clinical practice and math competency. In our study, the reasons for improvement stemmed from using the Triangle Technique for calculating pediatric safe dosage. As shown in Figure 2, 86.7% (n = 137) of participants reported satisfaction with using this technique for making these calculations.
Knowledge and attitudes
Teaching methods on this subject affect nursing students’ self-confidence and self-esteem (Pauly-O'Neill and Prion, 2013; Kapborg and Rosander, 2001). Likewise, in the current study, we found that after the training, most nursing students considered their drug dosage calculation skills to be sufficient. As complex concepts are more easily understood when simplified by using a symbol that fits the problem (Hunter Recell and McCurry, 2013), it is clear as to why learning the Triangle Technique led to greater self-confidence in the majority of our study sample.
Correlation between demographics and outcome variables
Nursing students’ ability for solving drug calculation test is related to various factors, such as pre-college math experiences, teaching methods, clinic educators acting as mentors, and using a calculator (Costello, 2011). There is a limited study by Costello showing the relationship between pre-college math experiences and the ability to solve drug calculation tests. As shown in her study with 44 first-year nursing students, a high math score on the scholastic achievement test, the number of high school math courses, and high school algebra grade were statistically positively correlated with a higher score on the medication calculation test (Costello, 2011). In a similar study, Grandell-Niemi et al. found that among 282 graduating nursing students in Finland, students who performed better in mathematics in high school were more successful in drug calculation tests (Grandell-Niemi et al., 2006). Unlike these studies (Costello, 2011; Grandell-Niemi et al., 2006), in our research, we found no correlation between high school type and success on a drug calculation quiz. It is possible that this result may reflect the fact that pediatric safe dosage calculation does not require complex math ability, such as solving intravenous drug dosage calculations with dry powder volume.
Limitation
There are a number of limitations associated with our study. First, was the lack of a control group and lack of a randomized sample, so there is the possibility of sampling bias due to purposive sampling. As a result, further studies are necessary to compare the outcomes of nursing students receiving training against a control group. The second limitation of the study is that the Satisfaction Form with the Triangle Technique was developed by researchers and was not tested at a pilot group. The third limitation of the study stems from the fact that teaching methods are not compared with one another in our study. Consequently, there is a need to evaluate which teaching methods are in fact most effective: PowerPoint presentation, web-based education, or Triangle Technique for solving pediatric safe dosage calculation for nursing students. The fourth limitation of the study, the fact that all the participants were women; may have limited the study findings. Hence, it would be very interesting to examine effects of Triangle Technique on both female and male nursing students’ ability to calculate pediatric safe dose ranges. Also, the study was limited to a specific institution, and a restricted group of students, which may have been a limitation as well. Hence, the findings of this study should be interpreted with these limitations in mind.
Implications for practice
For pediatrics, incorrect dosing is the most commonly reported medication error (Stucky, 2003). Since medication administration errors are common in children, student nurses should receive a comprehensive training regarding calculation of safe pediatric medication dosages. Nurse educators should use teaching techniques which include visual graphic such as triangle technique for students to learn accurate drug dose calculation. The symbol of an isosceles triangle provided the visual graphic for the conceptual framework. Considering that visualization increases learning, it is recommended to use the triangle technique in drug dose calculations in pediatric nursing.
Conclusion
The findings indicate that nursing students showed a low score on PSDCQ prior to educational intervention. Students’ low scores should be taken seriously as therapeutic-range medication dosage miscalculations could cause subtherapeutic dosage or potentially toxic dosage in children, or even deaths. However, the outcomes post-PSDCQ proved to be statistically significant regarding the TriangleTechnique; as effective in improving the pediatric safe therapeutic-range medication dosage calculations skill among nursing students. Outcomes from the current study highlighted that following the Triangle Technique training, only 17.7% (n = 28) of students claimed that their pediatric safe therapeutic-range medication dosage calculations ability was insufficient. Also, a large majority, 82.3% (n = 130), believed that pediatric safe therapeutic-range medication dosage calculations were not difficult. Overall, the findings indicate that Triangle Technique is effective for improving students’ ability to calculate pediatric safe dose ranges and has a high level satisfaction rate among nursing students.
Supplemental Material
Supplemental Material - Triangle technique: An effective tool for improving nursing students’ ability to calculate safe pediatric medication dosages
Supplemental Material for Triangle technique: An effective tool for improving nursing students’ ability to calculate safe pediatric medication dosages by Derya Suluhan, Dilek Yildiz and Berna Eren Fidanci in ournal of Child Health Care
Supplemental Material
Supplemental Material - Triangle technique: An effective tool for improving nursing students’ ability to calculate safe pediatric medication dosages
Supplemental Material for Triangle technique: An effective tool for improving nursing students’ ability to calculate safe pediatric medication dosages by Derya Suluhan, Dilek Yildiz and Berna Eren Fidanci in ournal of Child Health Care
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.