
Abstract
A convergent parallel mixed methods design with qualitative data collection embedded in a quasi-experimental study was developed to examine the potential of three modalities of preparation for hospital discharge of the families of children with chronic diseases in terms of uncertainty levels and management of the disease at home. Caregivers of these children were divided into three groups: two experimental groups and one control group. Two scales were applied: one measured family management, and the other evaluated uncertainties in relation to the disease. In addition, an in-depth interview was conducted. Wilcoxon’s test and the integrated response index were used in data analysis to compare performance between the groups. Inductive thematic analysis was employed for the qualitative data. The data were integrated, comparing the groups before and after preparation for hospital discharge. Twenty-five family caregivers completed this study. Data integration showed that the intervention group, in which the families developed planning to prepare for discharge in a dialogical way with professionals, presented better perceptions regarding care management when compared to structured guide and usual care groups. Participation of families in planning for hospital discharge showed a reduction in uncertainties regarding the disease and better care management of children at home.
Introduction
Family caregivers of children with chronic diseases (FCCCDs) need to be prepared during hospitalization to provide home care (Klein et al., 2021; Kuntz et al., 2021; Bom et al., 2021). However, parents of hospitalized children do not feel prepared after discharge to manage the disease at home (Góes and Cabral, 2017; Klein et al., 2021; Kuntz et al., 2021; Sawin et al., 2017; Smith and Kendal, 2018; Weiss et al., 2017). This is because this preparation for hospital discharge only occurs occasionally and without listening to families’ anxieties and questions. Health professional was focusing on the disease and using traditional teaching based on content transmission and demonstration of techniques decontextualized from the family life context (Góes and Cabral, 2017; Smith and Kendal, 2018).
Difficulties experienced by FCCCDs in managing the disease at home after hospital discharge arise from weaknesses in some areas such as lack of health education process, lack of appreciation of family singularities when preparing for discharge, and lack of attention by professionals on hospital teams in ensuring care follow-up in care networks after hospital discharge of children with chronic diseases (Toomey et al., 2016). Additionally, poor communication between professionals and families and lack of information (LI) support interferes negatively in the relationship (Smith and Kendal, 2018) and minimize questions.
This inadequate family preparation for hospital discharge has a negative impact on how they cope with the disease and on the prevention of new hospital admissions of children (Weiss et al., 2017). One obstacle identified in a study carried out at a university hospital in the southern of Brazil referred to health professionals’ difficulty cooperating with each other for hospital discharge planning, with a predominance of individualized and non-integrated actions (Kuntz et al., 2021). These actions can lead to hasty discharge, without clarifying questions of families about the care of children with chronic diseases, and don’t guarantee safe hospital discharge (Klein et al., 2021). Thus, it is necessary to identify more effective methods to minimize uncertainty about diseases and to improve care management in this population.
Disease management refers to a way in which families actively respond to diseases in different health care situations (Bousso et al., 2017). Disease-related uncertainties can influence this management. Greater uncertainties are, greater difficulties for families to understand the disease process (Madeo et al., 2012; Fedele et al., 2011). This interferes with decision-making and skills to manage care, generating physical and emotional overload in structuring, organizing or predicting the care demands for children with chronic diseases (Barbosa, 2012).
A scoping review identified different strategies for performing hospital discharge preparation in adults (MacDonell et al., 2020). Usual preparations for hospital discharge were evaluated in a study carried out in India that found a significant association between reporting of poor-quality hospital discharge with death and with chronic disease decompensation at 18 weeks of follow-up (Humphries et al., 2020). Preparation for dialogical hospital discharge was analyzed in a Danish study carried out with patients with chronic obstructive pulmonary disease, which identified a strengthening of knowledge and self-management of diseases after hospital discharge (Andersen et al., 2017). Dialogical way is an intervention that embraces specific needs of families, with back-and-forth dialog, in a participative and interactive way, as opposed to a prescriptive approach (Freire, 2015). This discharge preparation strategy can be defined as health coaching (MacDonell et al., 2020).
According to Stephens et al. (2017) and Weiss et al. (2017), there is few studies that investigate interventions for hospital discharge in FCCCDs and the complexity of this preparation. Given the lack of interventional studies, we proposed the following research questions: • How do different modalities of preparation for hospital discharge impact levels of uncertainty and management of the disease by FCCCDs? • When comparing preparation for hospital discharge developed in a dialogical way (Freire, 2015) with families, and preparation conducted by a structured guide and usual care, are there differences in levels of uncertainty and management of the disease by FCCCDs at home?
Preparation for hospital discharge mediated by dialogicity has same results as have usual or structured preparation;
Families exposed to hospital discharge preparing using dialogical way will have higher quality of discharge teaching with reducing uncertainties and better management of the disease by FCCCDs than families exposed to usual hospital discharge or structured preparation.
Aim
To examine the potential of three modalities of preparation for hospital discharge of families of children with chronic diseases in terms of uncertainty levels and management of the disease at home.
Materials and methods
Design
Convergent and parallel mixed methods approach was used, QUAL + QUAN (Creswell and Clark, 2017), with integration of results generating a third set of data for final interpretation. We opted for a quasi-experimental study, before-and–after, which made it possible to compare statistical performance obtained before and after preparation for hospital discharge. Descriptive-exploratory qualitative study illustrated and favored identifying aspects of preparation for discharge process that facilitated or hindered FCCCDs’ learning. After a separate analysis, quantitative and qualitative results were mixed for final interpretation (Lorenzini, 2017; Lorenzini et al., 2021).
Sample and settings
A purposeful sampling was applied in this study. Family members were recruited by first researcher on first day of children’s hospitalization. Pediatric Department of a university hospital of regional importance for hospitalization of children/adolescents with chronic diseases in a Brazilian state, with 24 active beds for clinical and surgical treatment and one day hospital ward. All participants were included in the sample following of this inclusion criteria: family members primary caregivers of children with chronic diseases in the age group from birth to 12 incomplete years old; and children hospitalized in the period from November 2017 to November 2018. Exclusion criteria were: family caregivers of children with a non-definitive diagnosis; the children hospitalized for a surgical procedure of ostomy reversion; children hospitalized for over a year; and family caregivers had no telephone contact to schedule a second timepoint of data collection.
All FCCCDs and their hospitalized children were eligible to participate in the study were invited and had 24 hours to decide to accept or not to participate in the research. Three had no interest in participating, and two withdrew from the study (in timepoint 1). Participants were divided into three groups according to hospital admission order: first was the group for which the family intervention was developed in a dialogical way, second was usual care group, and third was the structured guide group, following successively.
Study procedures
All groups received usual care hospital discharge preparation offer by professionals' staff of the Pediatric Department, as described for the UCG. The type of discharge preparation in each group was presented below.
Data collection
Quantitative and qualitative data collection occurred simultaneously in two timepoints, when was applied two scales and interviews carried out as follow: at admission and after hospital discharge. Completion of scales in all groups was mediated by main researcher, who read the items and alternatives based on a Likert Scale (1 - strongly disagree to 5 - strongly agree). Thus, participants could choose the answer that best suited their situation.
Mishel Uncertainty in Illness Scale - Family Member (Mishel) measures the level of uncertainty of FCCCDs. It is subdivided into four dimensions: ambiguity (AM): uncertainties related to decision-making, planning and implementation of the care provided (from 13 to 65 points); lack of clarity (LC): weaknesses in the explanations received or difficulty in understanding them (from 9 to 45 points); LI: LC due to not sharing information about diagnosis and disease with the family (from 5 to 25 points); and unpredictability (UN): family inability to make daily or future predictions for the disease symptomatology or evolution (from 4 to 20 points). Higher score indicates higher level of uncertainty (Barbosa, 2012).
Family Management Measure (FaMM) is subdivided into six dimensions: CDL—Child’s Daily Life (from 5 to 25 points); CMA—Condition Management Ability (from 12 to 60 points); CME—Condition Management Effort (from 4 to 20 points); FLD—Family Life Difficulty (from 14 to 70 points); VCI—View of Condition Impact (from 10 to 50 points); and PM—Parent Mutuality (from 8 to 40 points). PM was only filled out by caregivers who lived with a spouse/partner in the same household. Higher scores in CDL, CMA, and PM indicate greater ease in managing the disease, and CME, FLD, and VCI indicate greater difficulty in doing so (Bousso et al., 2017).
Scales were reliable tools to be applied in clinical practice with this population, based on a satisfactory index of Cronbach’s alpha on the Mishel scale (0.686) and a desirable index (0.9119) on the FaMM, showing its internal consistency and reliability from the measurement to the applied reality (Balbinotti and Barbosa, 2008).
Thus, in timepoint 1 (T1), Mishel and FaMM scales were applied within 48 hours of admission for all recruited families to measure levels uncertainty and disease management before preparation for hospital discharge. In the qualitative study, an in-depth interview was carried out personally with the FCCCDs, conducted by the first researcher. Questions asked to families before preparing for discharge were: “Tell me about your experience and that of your family in daily care of [name of child with chronic disease]. What questions do you have regarding the care of your child?” This data provided support for the planning of hospital discharge for the DIG.
To avoid overlapping interventions of the experimental groups (DIG, SGG), the Pediatric Department was visited daily to identify admission of children with chronic disease, and thus ensure control of the experiment during the hospitalization process, and all groups were visited by the researcher to follow the progress of the case. In timepoint 2 (T2) of the study, which took place two months after children’s hospital discharge, the two scales were reapplied, and a new in-depth interview was conducted. Questions asked were: “How do you evaluate the preparation for hospital discharge performed during hospitalization?” and “What is your perception of your child’s home care after hospital discharge?” Participants were contacted by telephone to schedule day, time, and preferred location for the interview.
Data analysis
Quantitative data were tabulated and processed in R software, version 4.1.0. Descriptive statistics were used to characterize the FCCCDs; given the small sample size, we used the Wilcoxon test (W) for paired samples to compare performance of each group before and after hospital discharge with the following hypotheses: H0: Scale scores before and after discharge preparation are equal; H1: Scale scores before and after discharge preparation are different. In the intergroup comparison, integrated response (IR) index was applied, in which the UCG was considered a control group for having received only the usual hospital discharge preparation in the Pediatric Department.
A significance level of 5% was used in all tests. A 95% confidence interval (CI) was calculated to analyze statistical trends in the scale dimensions. When calculating the RI index (Sanchez et al., 2013), the mean (X̄) of each item in the subscales was verified, followed by logarithmization of the ratio between the values of the groups, with the addition of one unit, by mean. Overall means and standard deviations were calculated for all groups. Logarithmized values were standardized using the effect size formula for all groups. Baseline was created centered on zero to represent variation of each of the instruments’ questions. Difference between each standardized answer (Zi) and mean of the values of each question in the reference group (Z0) were calculated to obtain the deviation index (A) that determined the effect size in each group studied in its respective timepoint. Values of A were added up determine the IR value for each group by timepoint. In the radar type graph, data by subscale were represented, indicating deviation of the DIG and SGG in relation to the UCG. UCG IR values were considered as reference values to compare performance of the experimental groups before and after the intervention.
Regarding the qualitative data, six steps of inductive thematic analysis were used: interview transcription for familiarization with the empirical material, initial coding, classification of codes into pre-themes, review of pre-themes, definition of themes, and elaboration of final report (Braun et al., 2019). No software was used for qualitative data analysis. Data were organized manually into analytical tables and the generating themes were identified by any means of chromatic marking.
Qualitative and quantitative data were integrated and organized in a joint display. Qualitative data helped to understand the scores obtained in the group that received usual preparation for discharge when compared to experimental groups.
Ethical considerations
Study was approved by Research Ethical Committee and its implementation followed Brazilian guidelines and norms regulating research involving human subjects. All participants signed consent forms. Before, questions about the study were clarified and the right to accept or deny participation on the study without impacting care, and the right to withdraw from participating were guaranteed. Anonymity of families was guaranteed by using letters and numbers to identify their respective groups.
Results
Sample characteristics
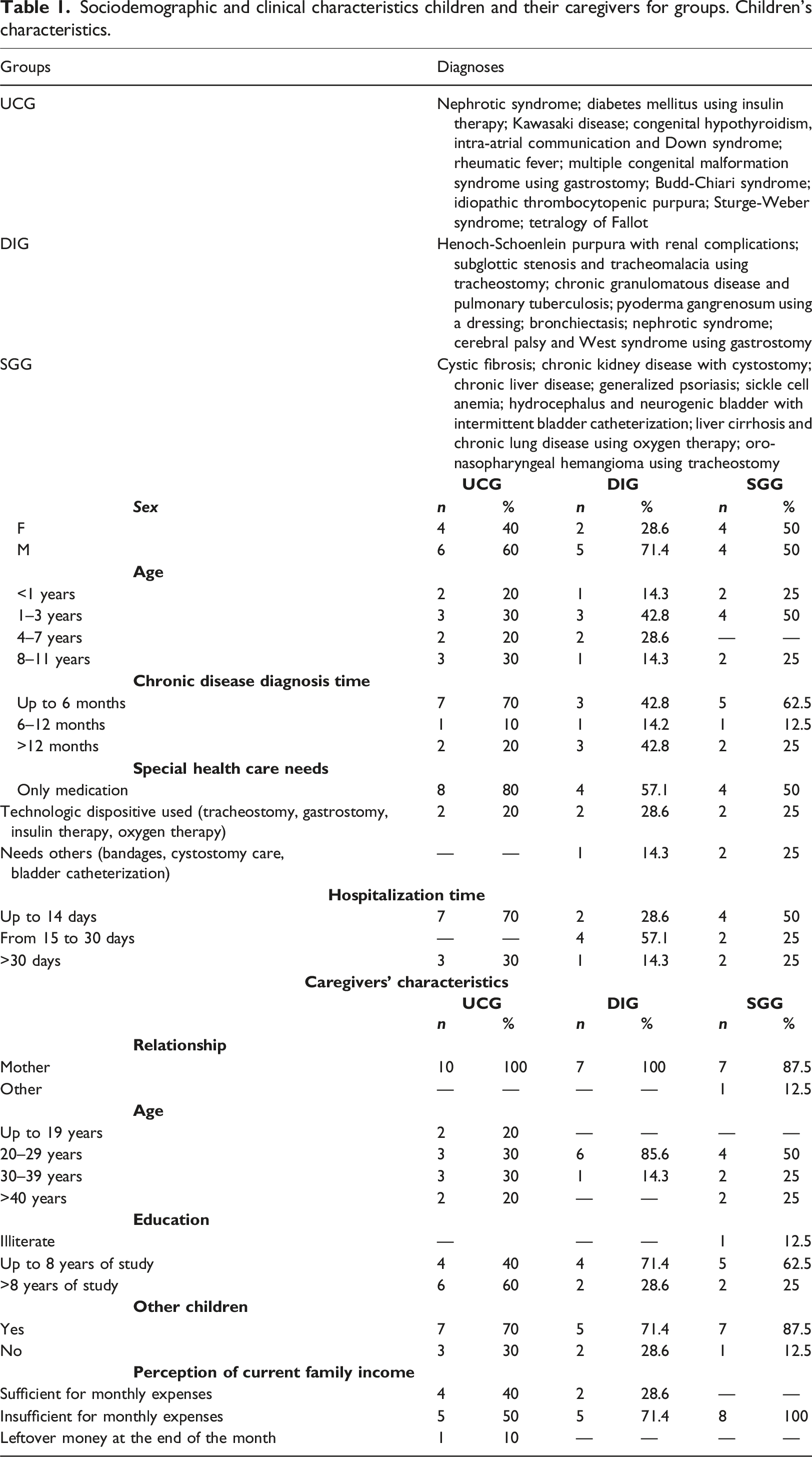
Sociodemographic and clinical characteristics children and their caregivers for groups. Children’s characteristics.
Narratives in the FaMM and Mishel scale before and after preparation for hospital discharge
Joint display comparing quantitative data by dimensions of the Mishel scale and qualitative data with the FCCCDs of the DIG, SGG, and UCG on levels of uncertainty before and after hospital discharge.
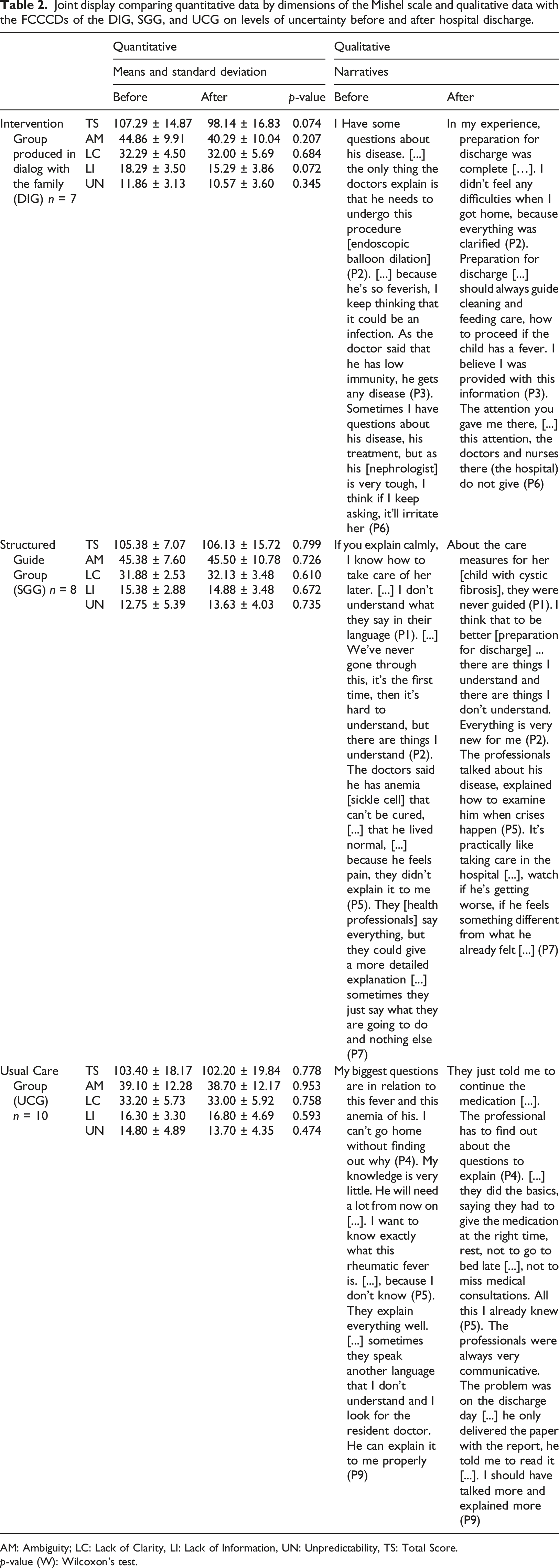
AM: Ambiguity; LC: Lack of Clarity, LI: Lack of Information, UN: Unpredictability, TS: Total Score.
p-value (W): Wilcoxon’s test.
Although no statistically significant difference before and after intervention was found, there was a trend towards a lower overall score for levels of uncertainty in the DIG (p-value = 0.074; X̄1 = 107.29, 95% CI 96.27–118.31 and X̄2 = 98.14, 95% CI 85.67–110.61). Qualitative data showed greater satisfaction about families' expectations being met regarding preparation for the intervention that involved hospital discharge planning produced in dialog with the families. Figure 1 presents the comparison of the IR values calculated for DIG and SGG with the UCG. Integrated response index related to the Mishel scale before (timepoint 1) and after (timepoint 2) interventions evaluated in the DIG and SGG when compared to UCG.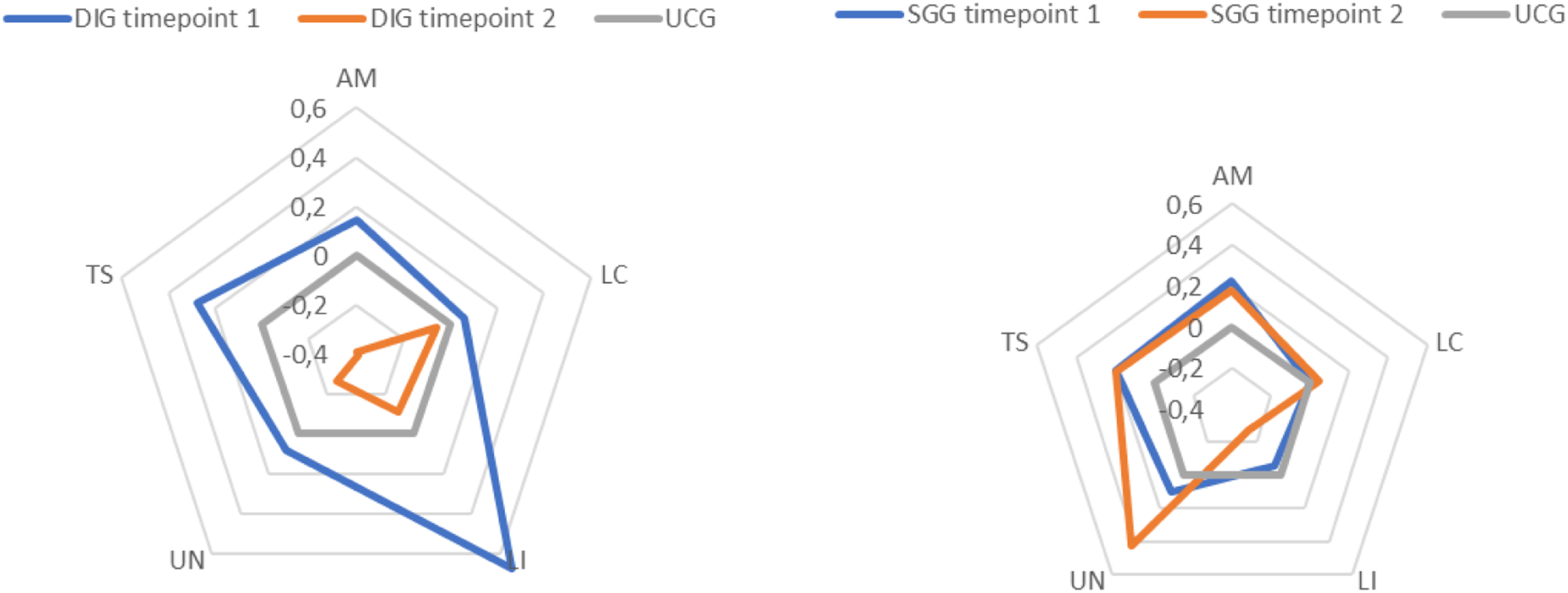
When quantitatively comparing performance of the experimental groups with control group (UCG), a reference for the IR index, the results of the Mishel scale showed a statistically significant difference in the DIG indicated reduction of uncertainties after the intervention, observed with the reduction of all the dimensions (IR1: 1.25 and IR2: −1.23). In the SGG, there was no significant difference in levels of uncertainty in this group when compared to the usual discharge preparation group (IR1: 0.46 and IR2: 0.58).
Joint display with comparison of quantitative data by dimensions of the FaMM scale and qualitative data with the FCCDC among DIG, SGG and UCG on disease management before and after hospital discharge.
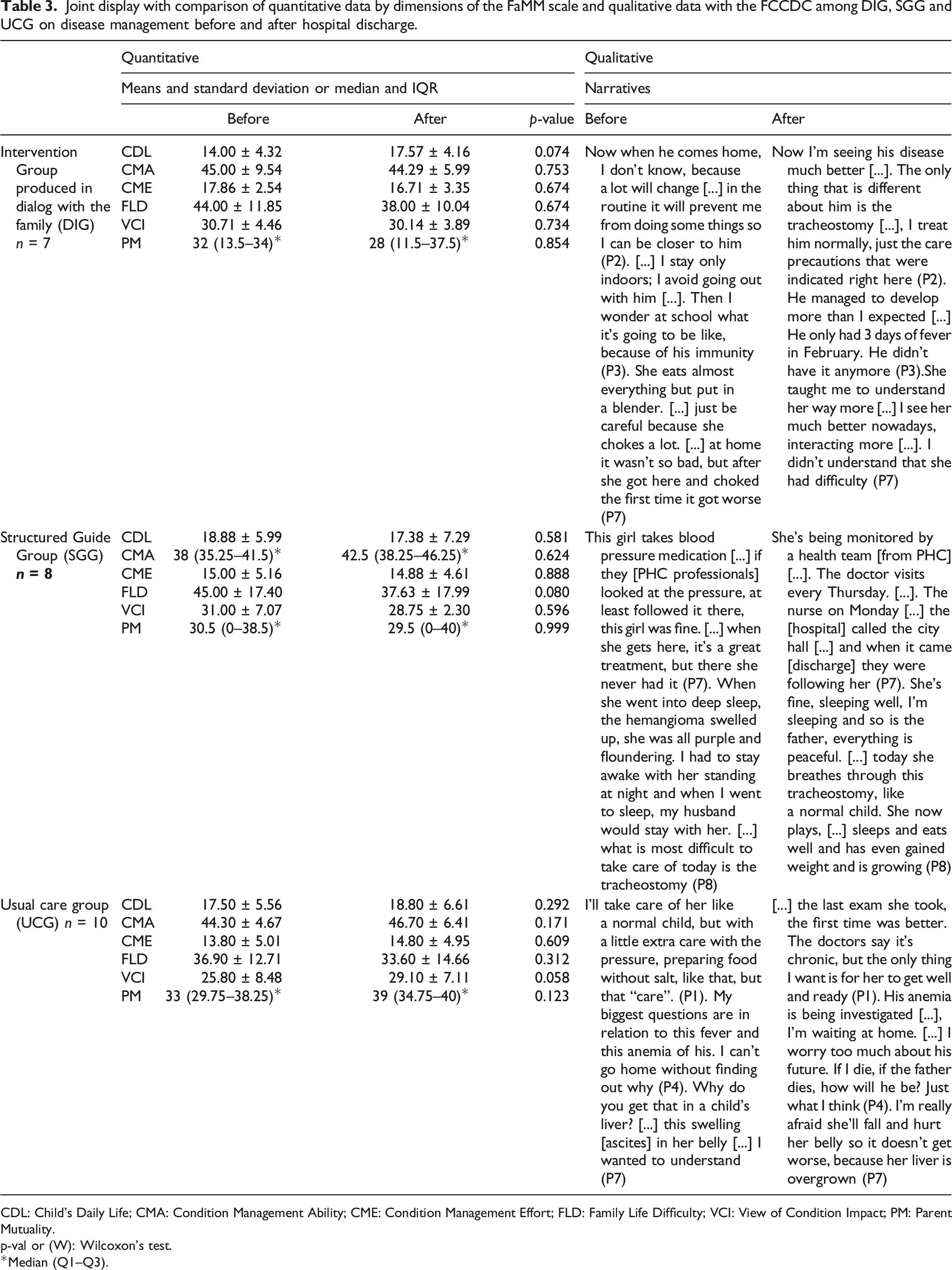
CDL: Child’s Daily Life; CMA: Condition Management Ability; CME: Condition Management Effort; FLD: Family Life Difficulty; VCI: View of Condition Impact; PM: Parent Mutuality.
p-val or (W): Wilcoxon’s test.
*Median (Q1–Q3).
Figure 2 shows the effect size of the FaMM results. Integrated response index related to the FaMM results before (timepoint 1) and after (timepoint 2) the interventions evaluated in the DIG and SGG when compared to the UCG.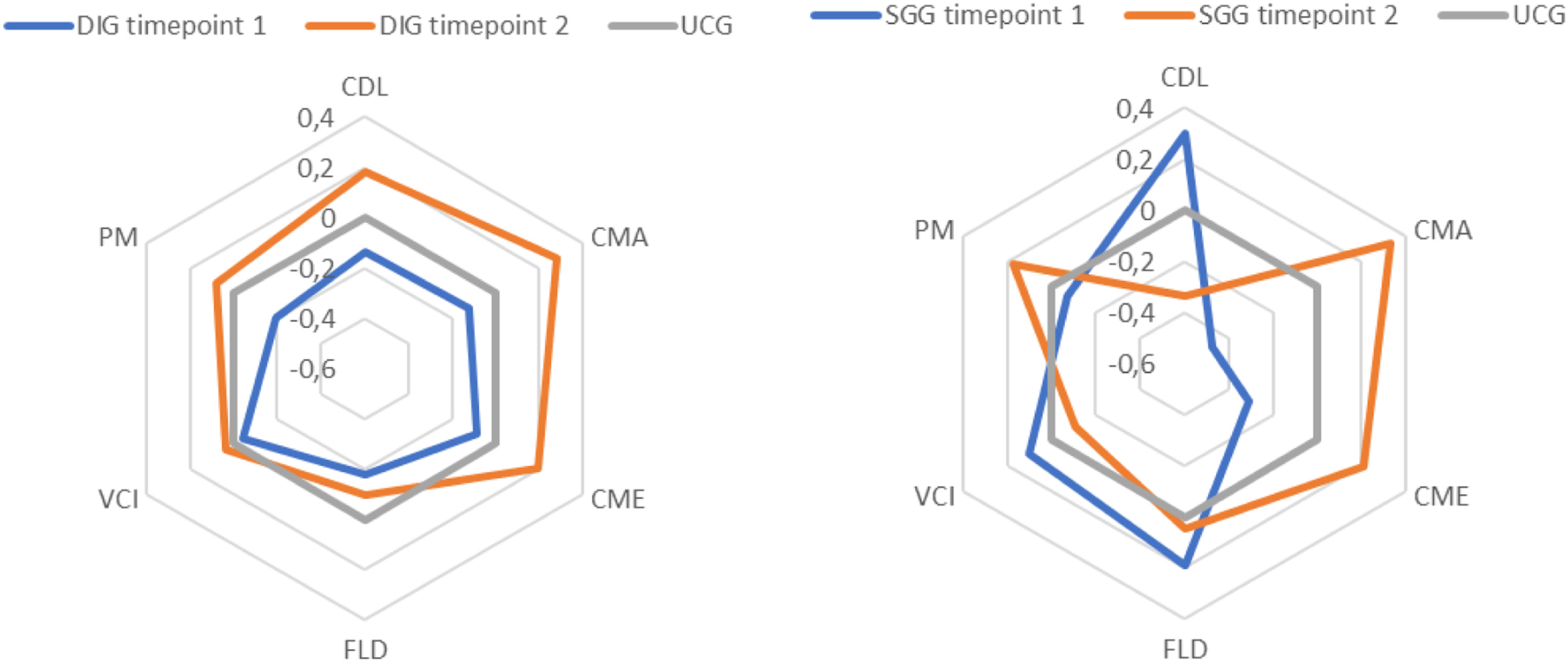
It is evident that SGG was close to the baseline and, therefore, similar to UCG (IR1: −0.24 and IR2: 0.020), with induction of CMA, CME, and PM and inhibition of CDL and VCI. DIG increased in relation to baseline (IR1: −0.15 and IR2: 0.40) with induction in the CDL, CMA, CME, and PM dimensions when compared to UCG.
Discussion
Explanatory evidence for trends found was identified with databases’ integration (Oliveira et al., 2021). DIG tendency to minimize levels of uncertainty can be attributed to partnership between professionals and families in the development of discharge planning. In the joint construction of this planning, knowledge, experiences, and unique demands of the FCCCDs were valued, as well as their life context. Thus, it resulted in greater appropriation of knowledge to carry out home care, strengthening their confidence in decision-making.
SGG and UCG predominated preparation for hospital discharge without family participation in the planning. Actions taken aimed to pass disease-focused information standardized to FCCCDs, to carried with them on returning home, which did not contribute to reducing uncertainties. According to Paulo Freire, this is the “visão bancária do processo educativo” (“banking view of the educational process”), in which “os homens [são] vistos como seres da adaptação” (“men [are] seen as adaptable beings”) to what is imposed on them (Freire, 2015: p. 83). Dialogical approach is an existential meeting between people who seek to reflect on reality in order to transform and humanize it. Therefore, it cannot be reduced to an act of depositing content from one into the other, nor can it become a simple exchange of ideas between people (Freire, 2015).
Education in health through authentic dialog presupposes qualified listening with appreciation of families’ previous knowledge for the reconstruction of reality (Severo et al., 2019). Engaging FCCCDs in learning prepares them to shape knowledge to meet their needs in the home context. This is the central concept of wayfinding, which surpasses simple information transfer (McDonald et al., 2017), contributing to the autonomy of family decision-making.
Preparation for hospital discharge should start from admission and last during hospitalization, and ambience present during this period influences the teaching-learning process of the FCCCDs. Ambience is made up of the physical structure, the actions by the team’s professionals, and the professional-family-child relationships established. When it is favorable, it impacts positively on reception and resolution of their needs (Fontana et al., 2017) resulting in a sense of safety and well-being (Sundal, 2023).
In this study, ambience was disadvantaged when: (i) families did not participate in the planning of preparation for hospital discharge, which resulted in lack of clarification of their questions; (ii) professionals provided little time for preparation and used language that was difficult to understand; and (iii) there was no cohesion between the types of information provided by the multidisciplinary team to the families.
To change these negative aspects of ambience, it is necessary for health professionals to take an empathetic posture with regard to needs of families which goes beyond the prescriptive posture, in order to favor the bonding created by a true meeting between families and professionals. This bond gives FCCCDs confidence about expressing their questions, expectations, fears and life context, in addition to favoring feedback of their real knowledge about care. In the DIG, bonding and the clarification of caregivers' questions may have been favored by longer hospitalization time (between 15 and 30 days) when compared to the UCG and SIG, with times up to 14 days.
Family decision-making is also strengthened when continuity of care in the HCN is guaranteed. Integration of network points enhances support for these children, facilitating access to the actions and services necessary for their care after discharge (Klein et al., 2021; Souza et al., 2020).
Children with chronic disease are dependent on the HCN to meet their health demands (Costa et al., 2020). The FCCCDs learned about the network’s support points and acquired autonomy in decision-making to choose therapeutic itineraries, resulting in better quality of life (McDonald et al., 2017). For families with low education, ensuring this support for continuity of care in community services and additional health providers is critical (Phonpruk et al., 2019).
Telephone contact with health departments of the municipalities of origin of the FCCCDs of the SGG resulted in a tendency to minimize difficulties related to disease, although without statistical significance. SGG achieved better results when compared to the strategy of the DIG of delivering summaries to the FCCCDs to be taken to PHC, or of the UCG of delivering the usual hospital discharge medical summaries.
Studies carried out in Canada (Aued et al., 2019), Madrid, Barcelona, Murcia, Seville, Granada (Costa et al., 2020), and Brazil (Röhsig et al., 2019) show that the coordination of care between HCN services performed by nurses through phone calls in preparation for hospital discharge ensured continuity of care. One study also identified promising results in improving the quality of teaching at discharge when nurses used an iPad application in the preparation of hospital discharge (Lerret et al., 2020). This can also, collaborate with systematization of hospital discharge preparation during hospitalization (Sulino et al., 2021).
UCG’ trend identified was unfavorable for disease management because it represents greater concern for the FCCCDs about the future implications of the disease for the children. In the narratives, efforts by UCG professionals to explain the disease and its treatment were observed, but with unidirectional and informative communication. Families considered information and explanations superficial and/or not understandable due to the use of technical terms that were difficult to understand.
Study limitations
A major limitation of this study is that DIG was administered by MDs, SGG by nursing students, and UCG by clinical care nurses. In addition, inclusion of participants was hampered by administrative problems in the Pediatric Department (need for fumigation in the department, lack of supplies such as peripheral venous catheters, interdiction in the nutrition unit) and the truck drivers' strike in the country, which reduced admissions for approximately three months. Due to the reduced sample size, it not enabled to randomize participants and controls to reduce the possibility of confounding bias. Studied variables such as time of diagnosis and length of hospitalization (longer in the DIG), and caregivers’ levels of education (higher in the UCG) presented some disparities. This indicates need of future randomized studies with large sample sizes to better examine these variables. A final limitation was that long hospital stays (24% with more than 30 hospitalization days) resulted in low bed turnover, compromising participants’ inclusion.
Implications for practice
Overall findings from this study support that when communication by health professionals is unidirectional, informative, and irregular, it hinders appropriation of knowledge, weakens FCCCDs' knowledge. Health professionals should implement shared decision-making to be more productive and contribute to development of more effective relationships and communication (Koch et al., 2022).
For the development of discharge planning in a dialogical way with families, it is necessary to pay attention to the impact of the children’s home care on family dynamics (Góes and Cabral, 2017). Recommendations given are more likely to be effective if Health Care Professionals overcome disease-focused care, which is essentially limited, to open up new horizons with the implementation of individualized care. In unique planning of preparation for discharge, there is deconstruction of power asymmetries between professionals and family caregivers, favoring greater awareness of the families’ life histories and ways of caring for them. In this dialogical construction, traditional narration of content is overcome and becomes construction of family-centered care.
Conclusion
This study found that family participation in planning for hospital discharge led to a reduction in levels of uncertainty regarding the disease and better care management of children at home. Discharge preparation intervention with structured guidelines, which included a telephone call for continuity of care in primary care, showed a tendency to minimize the difficulties related to the disease. To give voice to the participants to explain their necessities during a dialogical discharge preparation contributes to the family-centered-care.
DIG participants had a longer hospital stay. Therefore, it is important that new studies be carried out in order to identify whether dialogical hospital discharge preparation have good results in children with shorter hospitalization time.
Integration of qualitative and quantitative data provided a more comprehensive understanding of preparation for hospital discharge carried out by means of different strategies, identifying its strengths and weaknesses of each on, which can support its improvement.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financed in part by the Coordination for the Improvement of Higher Education Personnel– Brazil (CAPES) – Finance Code 001.