
Abstract
Adequate early childhood development is critical for later-life success. Developmental profiles of specific populations are required to support implementation of early intervention services. Three hundred fifty-three caregivers of children with mean age 17.9 months (SD = 10.5) were selected from a primary healthcare clinic. Overall positive identification of signs of a developmental delay, with the Bayley Scales of Infant and Toddler Development III, was 51.8% (n = 183). Logistic regression analysis determined the effect of age and gender on results. Prevalence of developmental delay increased with age from 33.1% for children under 12 months to 61.7% and 66.3% for children between 13–24 months and 25–36 months, respectively. Females were 1.82 times (95% CI [1.16, 2.85]) more likely to have had no signs of developmental delay; 2.30 times (95% CI [1.14, 4.65]) in motor and 2.06 times (95% CI [1.23, 3.45]) in adaptive behaviour domains. One-third of children presented with low levels of adaptive behaviour functioning. One hundred and one (28.6%) participants across age groups displayed superior social-emotional ability, possibly due to familial structures and relationships. One-third of children presented with poor adaptive behaviour function, attributed to cultural differences. This study contributes to information on developmental characteristics of children in South Africa.
Introduction
Two hundred fifty million children below 5 years of age in lower-middle-income countries (LMICs) are not reaching their developmental potential (Rasheed and Yousafzai, 2015; Zablotsky et al., 2017). A large proportion of young children in South Africa are negatively impacted by a range of social and economic inequalities, undermining their development (Atmore, 2012; Hsiao et al., 2017). Poverty and socio-cultural context increase young children’s exposure to risk factors that affect their development (Carter, 2018; Joshua et al., 2015; Tran et al., 2017). Children residing in poverty-stricken contexts are at significantly higher risk for behaviour, social-emotional, physical and cognitive problems as well as later academic difficulties (Cairney et al., 2016; Garcia et al., 2018).
Recent prevalence estimates of children not meeting developmental outcomes in LMICs are 35% (Miller et al., 2016) compared to 7% in a high-income country like the United States (Zablotsky et al., 2015). An estimate of 474,000 children in South Africa are living with severe delays and many more with mild to moderate delays (Bridge, 2016). About 40% of delays affecting young children result from preventable causes (Bridge, 2016).
Accurate data on children not reaching their developmental potential are important for policy and resource allocation, as well as for tracking progress toward meeting global goals such as Sustainable Development Goals (SDGs) (Black et al., 2017). The SDGs aim to ensure that all women, children and adolescents have an equal chance to thrive, and not simply survive (Urke et al., 2018). National plans, in all countries, to support children to thrive must ensure that early child development (ECD) is prioritised to inform policy and programmatic implementation and achieve the SDG target (Bushnell et al., 2016). Global commitments to ECD are growing, as the number of countries with national ECD policies has increased, of which 45% are low- and middle-income countries. In 2020, 87 countries – four more than in 2019 – have established a national ECD policy or action plan. Some 117 countries, up from 105 in 2019, have government-owned multisectoral ECD programmes, which focus on promoting stimulation and nurturing care for young children (UNICEF, 2021). In South Africa, the National Integrated Policy for Early Childhood Development (ECD) represents government’s commitment to making quality ECD services available to young children (Bridge, 2016). Despite this policy, financial and capacity constraints result in inadequate implementation of services outlined in the comprehensive policies that are in place (Desmond et al., 2019). Inequity, marginalisation and a lack of access to quality early intervention services remain a barrier (Camden et al., 2020; Joshua et al., 2015; Murphy et al., 2020; Samuels et al., 2012).
Studies on ECD in South Africa have previously investigated risks and protective factors for development (Donald et al., 2019) and developmental outcomes of children of mothers with depression (Christodoulou et al., 2020). Other studies conducted have described relationships between a child’s cognition and later educational outcomes of children in rural South Africa (Cortina et al., 2019), and the cognitive and physical development of HIV-positive children (Sherr et al., 2018). These and other studies have focussed on at-risk populations with existing conditions in rural poverty-stricken areas, rather than a broader overview of developmental characteristics in LMICs (Ballot et al., 2012, 2017a; Wedderburn et al., 2019). General developmental outcomes of children in LMICs are thus unclear.
A description of developmental characteristics provides information on typical and atypical development, and a prevalence of developmental delay across and within specific developmental domains (Chambers et al., 2016; Gasparini et al., 2017). This information may be used to guide implementation of early intervention services (including developmental assessment, surveillance and intervention) to support optimal child development. An outline of developmental characteristics may also serve as an indicator of function, which aids clinicians and parents in setting realistic expectations and facilitating timely interventions (Sumanasena et al., 2019). Describing developmental characteristics of those children who are most susceptible to poor developmental outcomes is necessary to focus assessment and interventions, as well as to improve child health outcomes (Wedderburn et al., 2019). Given that children in sub-Saharan Africa are most at risk to not meet their developmental potential, and there is a dearth of published findings thereof, these findings could have important implications for public health policies (Wedderburn et al., 2019). This study’s purpose was, therefore, to describe developmental characteristics of young children, under 3 years of age, from a low-income South African community using a gold-standard tool. This is necessary in order to create a developmental profile for this population to easier identify the need for early intervention services, as well as the protective factors or assets in the population.
Aim
To describe the developmental characteristics of children aged 3–36 months using the Bayley Scales of Infant and Toddler Development III (BSID-III) in a low-income community.
Method
A descriptive research design was utilised to describe developmental characteristics of children aged 3–36 months using the BSID-III in a low-income community.
Context
Data for this study were collected at Stanza Bopape primary healthcare (PHC) clinic in Mamelodi, Gauteng, South Africa. Mamelodi is one of the largest townships in the Tshwane Metropolitan Municipality, South Africa. More than a third of residents in Mamelodi live below the poverty line (Freedom House, 2017).
Population
A convenience sampling method was employed to select caregiver-infant dyads to participate in this study. Caregivers were invited to participate while waiting in the queue at the baby wellness clinic with their children. A total of 353 caregivers and their children aged with a mean of between 3–36 months (SD = 10.5), with SD representing standard deviation, were included in the study. This age range was focused on, as 1 month to 36 months is the targeted age range of the BSID-III. Caregivers attending the baby wellness clinic, who were proficient in English or Afrikaans, were included in the study.
Apparatus
The Bayley Scales of Infant and Toddler Development III (BSID-III) are norm-referenced measures for assessing development of children ages 1 month to 36 months. It is a valid and reliable tool used for clinical and research purposes (Rademeyer and Jacklin, 2013). The Bayley-III consists of five scales: Cognition, Receptive Language, Expressive Language, Fine Motor and Gross Motor, which are assessed by direct observation; and the Social-Emotional and Adaptive Behaviour domains depend on parental or caregiver report.
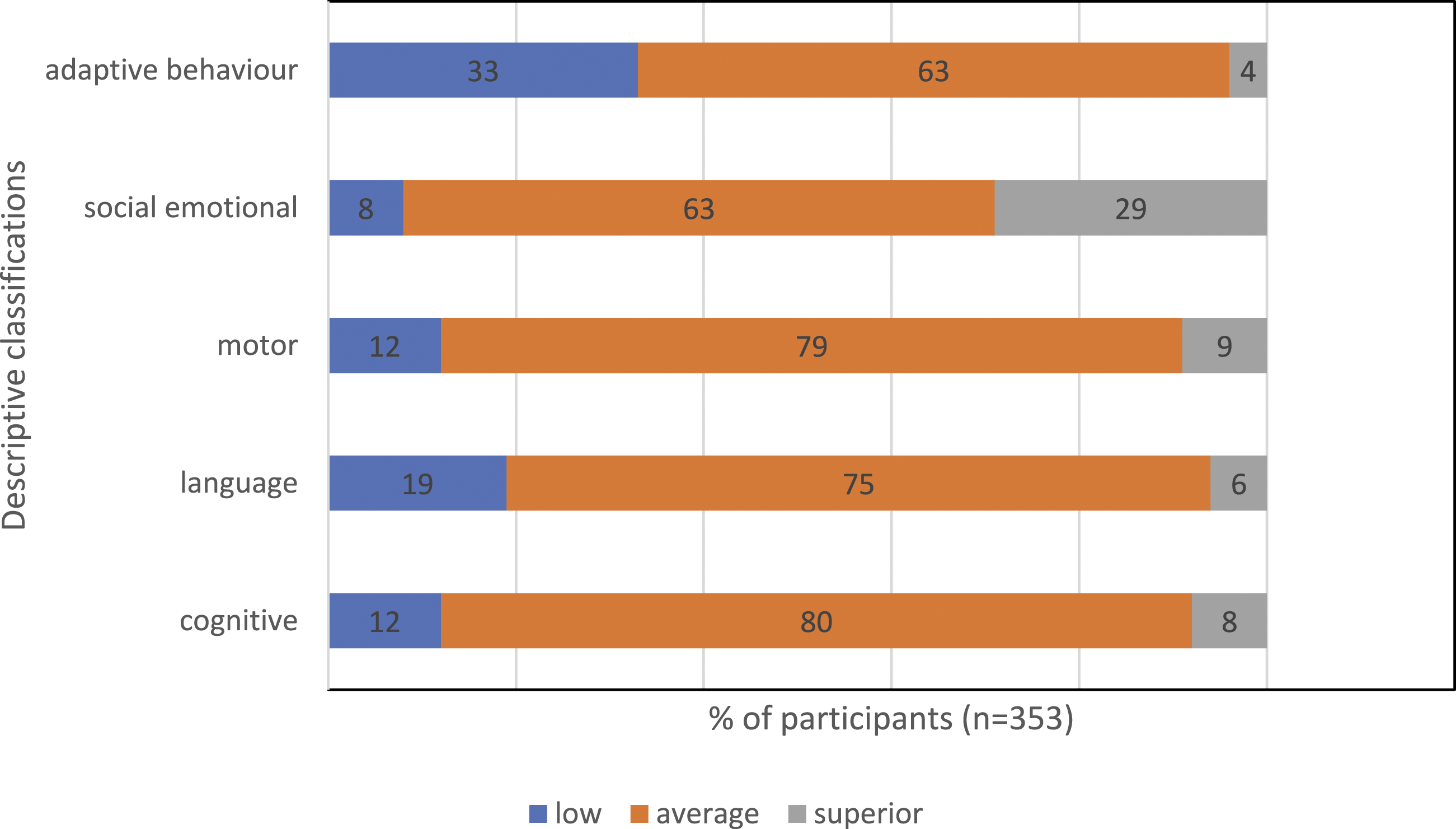
Descriptive classifications of the BSID-III focus on capacities of a child, and define these as very superior, superior, high average, average, low average, borderline and extremely low. Identification of delay in a developmental domain was defined, according to the BSID-III manual, as a score of 70–79 indicating a mild delay (borderline), and a score of <69 suggesting a severe delay (extremely low).
The BSID-III is a gold-standard observational measure of development for children from 1 month to 36 months. It has established content validity, and a panel of experts reviewed the tool to ensure its validity and reliability before it was used in this study. It has been validated for a South African population (Ballot et al., 2012; Rademeyer and Jacklin, 2013) and found to be culturally appropriate without modifications. Thus, the BSID III has been successfully used in South Africa on a similar population group which made this choice of assessment tool a valid choice for this study (Donald et al., 2019).
As the BSID-III has been normalised in developed countries, local practitioners should understand the nuances and should know if these tests and expected performance remain consistent for different ages within the local context (Laughton et al., 2010; Rademeyer and Jacklin, 2013). Previous developmental profile studies in South Africa, using the Griffiths Mental Development Scales, showed a lower developmental profile in children from low socio-economic groups when compared with expected norms (Laughton et al., 2010). Mean scores on assessment measures were significantly higher than British norms in a study conducted in Cape Town, while overall scores were much higher on the BSID-III in South Africa when compared to a sample in the USA (Rademeyer and Jacklin, 2013). It is thus necessary to describe specific developmental characteristics in a particular patient population profile, to appropriately identify signs of developmental delay based on their expected developmental trajectory (Laughton et al., 2010).
Procedures
Ethical clearance was obtained from the Research and Ethics Committee, Faculty of Humanities, University of Pretoria (reference number GW20160607HS). Permission was obtained from the clinic management to conduct the study and informed consent was obtained from all participants. Assessments were conducted in a quiet room at the primary health care clinic. The BSID-III was used for developmental assessment. Final year Speech-Language Pathology students (registered with a professional body), who received training to conduct the Bayley Scales of Infant and Toddler Development, assisted with the assessments under supervision. Quality control and monitoring processes were implemented to ensure accuracy. The research ethics guidelines in Ethics in Health Research: Principles, Structures and Processes (Department of Health, 2015) were followed. Compliance with national and international guidelines serve to reassure the public that the rights, privacy, safety and well-being of the participants are protected (Department of Health, 2015).
Scores of the paper-based BSID-III were manually completed and captured. Caregivers whose children were identified as having delays in one or more developmental domains were issued with referral letters to the relevant health care professionals for follow-up.
Data analysis
All quantitative data analysis (descriptive and inferential statistics) was conducted using Statistic Package Social Sciences (SPSS) v 23 (Chicago, Illinois), except for the achieved power analysis that was conducted using G*Power v 3.1.9.4 (Faul et al., 2007). A logistic regression analysis was conducted to determine the effect of gender and age on the overall and domain-specific results. We assume a linear relationship between the predictor variables (age and gender) and the log-odds (also called logit) of the event that the dependent variable is 1 = no signs of a developmental delay. This linear relationship can be written in the following mathematical form (with
Results
A total of 353 children (45.0% females) between the ages 17.9 months (SD = 10.5) were assessed at a PHC facility. Forty-five percent (n = 158) of children were female. Home languages spoken included Sepedi (n = 172; 48.7%), isiZulu (n = 52; 14.7%), Ndebele (n = 34; 9.6%), Setswana (n = 20; 5.7%), Tsonga (n = 16; 4.5%), Venda (n = 12; 3.4%), Shona (n = 12; 3.4%), SiSwati (n = 11; 3.1%), Southern Sotho (n = 7; 2.0%), Xhosa (n = 6; 1.7%), English (n = 5; 1.4%), Shangaan (n = 3; 0.8%), Northern Sotho (n = 1; 0.3%) and Portuguese (n = 1; 0.3%).
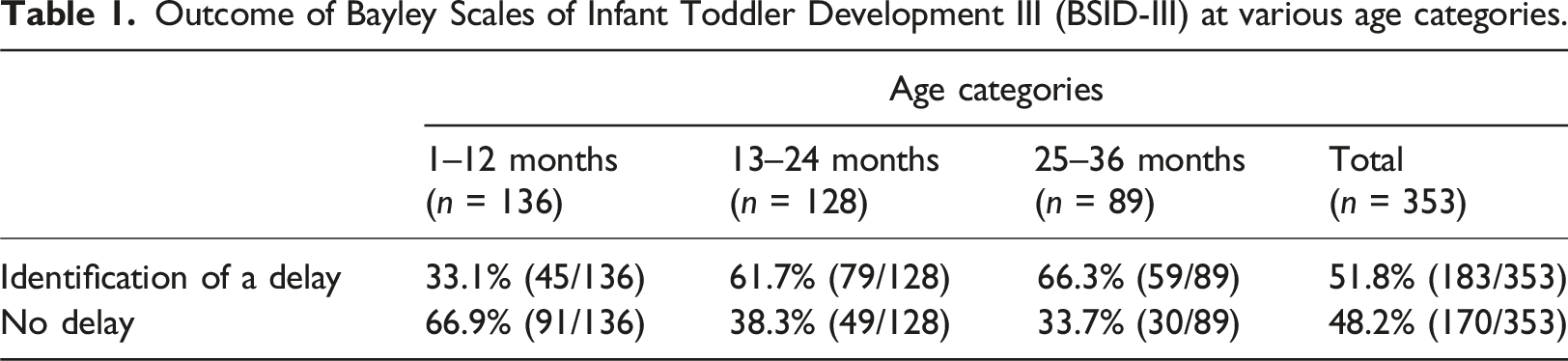
Outcome of Bayley Scales of Infant Toddler Development III (BSID-III) at various age categories.
Domain-specific outcomes (cognitive, language, motor, social-emotional and adaptive behaviour) were positive for developmental delays across domains varying between 8% for social-emotional and 58% for adaptive behaviour (Figure 1). A logistic regression analysis was conducted to determine the effect of gender and age on the overall and domain-specific results. Females were 1.8 times more likely to not show signs of a developmental delay compared to males ( Overall and developmental domain-specific positive diagnoses on the Bayley Scales of Infant Toddler Development III (BSID III) (n = 183). Descriptive classifications of development on the Bayley Scales of Infant Toddler Development III (BSID-III) (n = 353) Borderline or extremely low classifications grouped as low and indicate a developmental delay; Classifications that refer to average skills development were combined into one group (average) and those that refer to superior skills were grouped as superior.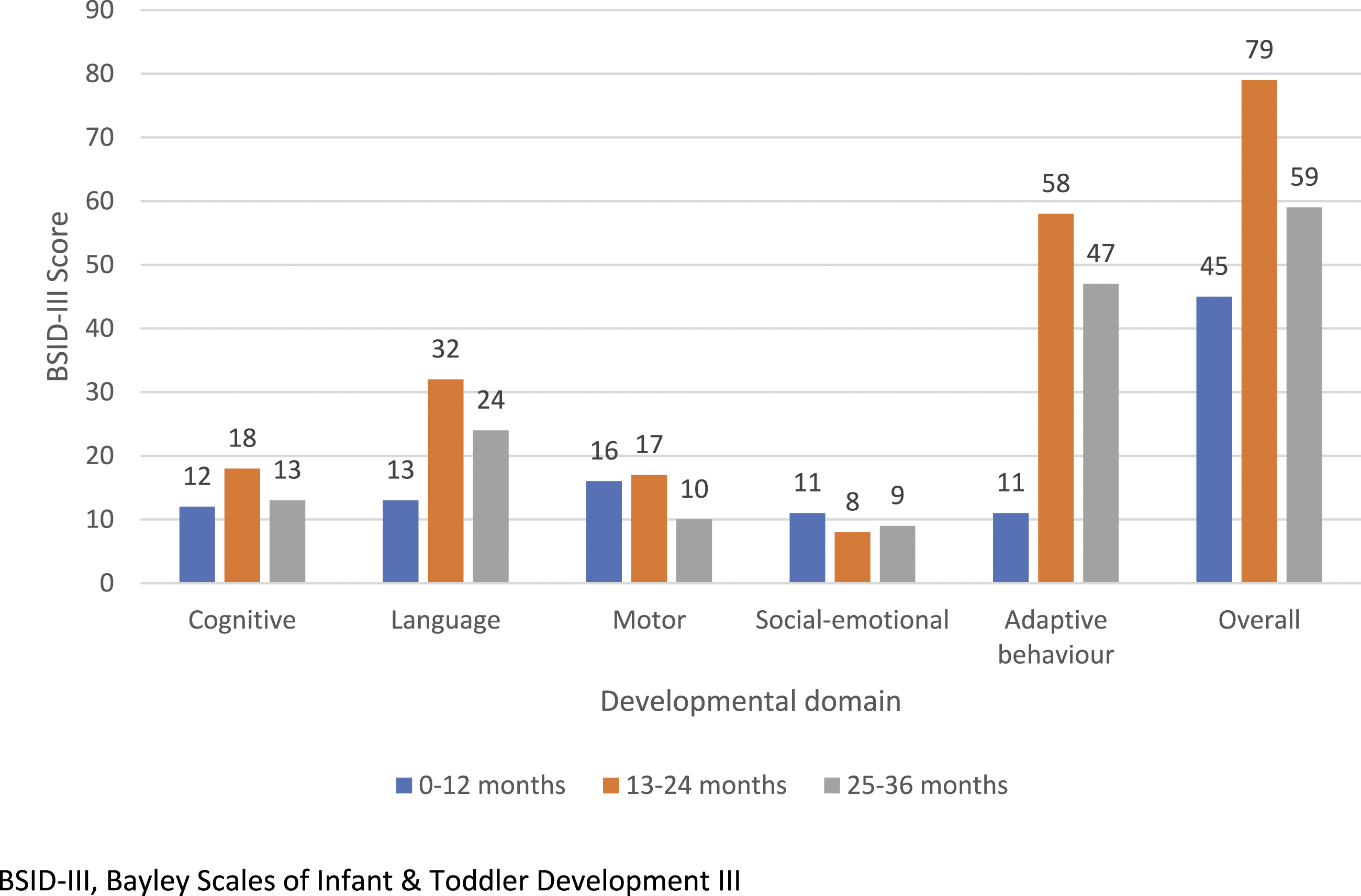
Ages 13–24 months and ages 25< months have significantly more occurrences of no signs of developmental delay than age group 1–12 months. The oldest children in this study have the highest number of overall signs of delay (27.0%). Twenty-eight (7.9%) participants across all age groups had delays in the social-emotional domain, and 101 (28.6%) displayed superior ability in this domain. In the adaptive behaviour domain, ages 13–24 months and 25< months do not differ significantly from each other, with those with delays over 45%; whereas ages 1–12 months differed statistically from them with identified delays of 8.1%.
Discussion
This study’s aim was achieved by describing the developmental characteristics of the study’s population using the BSID-III. More than half (n = 183; 51.8%) of young children (1–36 months) in this study were at risk of long-term developmental difficulties that warrant early intervention (Ballot et al., 2012). Positive overall identification of delays in developmental domains in the current study were greatest in children aged 25–30 months (n = 280; 79.3%) as opposed to younger children. This may be attributed to the fact that it is difficult to identify developmental delays in infants (Fischer et al., 2014). There was a higher incidence of delays in older children compared to younger children (Table 1) with significant differences between the age groups. A similar trend was identified by Ballot et al. (2017b), where the BSID-III was used to evaluate developmental outcomes of a group of very low birth weight infants (VLBWIs) in Southern Africa, and language scores decreased with age (i.e. identification of delays increased). Gender had a significant effect in this study, with males twice as likely to have delays in motor and adaptive behaviour domains than females. This is in agreement with a multi-country study where a similar trend was reported (Weber et al., 2017).
Almost twice the number of participants in the two older age groups were identified as having a delay in adaptive behaviour skills in relation to other domains (Figure 1). Although the BSID-III has been validated for the South African population and has been reported as culturally valid (Ballot et al., 2012; Rademeyer and Jacklin, 2013), this study found that cultural differences may have impacted children’s performance on the tool. The elevated identification of delays in children aged 13–24 months and in children 25< months in the adaptive behaviour domain were likely attributed to cultural differences. Children’s behaviour is often linked to caregiver expectations, as well as what is viewed as useful or of important influence in the child’s and family’s life. Cultural rearing practices also play an important role in adaptive behaviour of children (Snelling et al., 2019). This sub-section of the BSID-III includes test items that are completed by parents and caregivers with relation to a child’s abilities with regards to skills such as self-care, self-direction, and health and safety. It is important to note that not only the rate of development, but also the activities with which the child is familiar must be taken into account; and both these may be influenced by context (Holding et al., 2008). Children from various cultural groups may not be expected to master certain skills, as they are not culturally valid or acceptable (Semrud-Clikeman et al., 2017). Furthermore, children may not need to develop certain behaviours in their specific contexts (Balton, 2019). For example, in many LMIC settings in southern Africa, children do not have stairs in their homes; therefore, items that assess motor development or adaptive behaviour based on the climbing of stairs may be inappropriate. Another study, which explored the use of the Parents’ Evaluation of Developmental Status (PEDS) tools, also found that children in the low-income context of South Africa have higher referral rates with regards to adaptive behaviour (du Toit et al., 2020).
Many children in this study and more than 50% of children in a study by Ballot et al. (2017b) presented with average skills in all domains. Almost a third of children in this study, however, presented with superior social-emotional skills. Similarly, higher scores in the social-emotional compared to other domains were found in a study conducted in Greece, which is classified as a high-income country (Velikos et al., 2015). In addition to social-emotional ability being derived from the parent-report questionnaires in the BSID-III, the superior social-emotional ability could be linked to strong familial relationships and extended family structures, a characteristic of many South African, especially black African families (Barbarin and Richter, 2013; Huang et al., 2017; Mampane et al., 2019; Singh et al., 2014). Extended families provide social-emotional support for one in three children, or 30%, of children in South Africa (Patel et al., 2017). Previous studies have demonstrated that increased interactions result in improved outcomes (Nuri et al., 2019; Rasheed and Yousafzai, 2015; Romeo et al., 2018).
Study limitations
The current sample does not represent the spectrum of diversity across LMICs but is representative of a low-income community within South Africa; so results cannot be generalised to all children across other socioeconomic, linguistic and cultural groups. Although the BSID-III is valid for use in the black urban African population, further research on the Bayley-III is needed to assess a larger, more diverse group, including all age groups for which the Bayley-III caters (Rademeyer and Jacklin, 2013).
Another limitation of this study is that the BSID-III has not yet been culturally adapted for the South African population. The BSID-III presented with elevated referral rates in this study. This may be attributed to a number of reasons, including the high-risk nature of the population and the young age group. Inaccuracies in parental reporting, most often used with young infants, may have contributed to the under- or over-referral results on the developmental screening measures, resulting in poorer performance than expected when compared to older children. Data for this study were also collected manually, which therefore increases the risk of data being inputted incorrectly. Additionally, while the assessors were trained to use the BSID-III, this study was limited in that no other clinical data was available to substantiate a diagnosis.
Implications for practice
This study’s findings suggest that the BSID-III may be a suitable tool to describe the developmental profile of South African children, which supports previous research (Rademeyer and Jacklin, 2013). The tool has previously been evaluated in studies mostly on HIV-exposed infants and other infants at risk of developmental delay, for example, infants with low birth weight (Springer et al., 2020). Studies have mostly focused on at-risk populations in rural poverty-stricken areas (Wedderburn et al., 2019). As children in sub-Saharan Africa are most at risk of not reaching their developmental potential, understanding their development is important, and further research with a range of cultural and linguistic groups in South Africa is needed.
Clinically, understanding the developmental profile of these children will contribute to guidelines for best practice, especially regarding tailoring developmental assessment to fit the needs of this population. It is clear that the children in this study performed well in the social-emotional domain; however, a concern arose regarding adaptive behaviour functioning. This implies that more cultural consideration is needed in the assessment of adaptive behaviour, even with the use of a gold-standard tool such as the BSID-III. These studies are needed to ascertain the exact nature of expected developmental characteristics, as well as any expected developmental delay with appropriate assessment and intervention measures, across communities and population groups that are greatly influenced by cultural beliefs and practices.
Conclusion
This study contributes to emerging research on the understanding of developmental profiles in young children in LMICs like South Africa. Almost one-third of children in this vulnerable population presented with superior social-emotional skills, possibly due to familial structures and relationships related to the study population. One-third of children evaluated from this low-income South African context presented with low levels of functioning in the adaptive behaviour domain, possibly attributed to various factors including cultural differences. Understanding the course of healthy development and the effect of a child’s settings, customs, and ethno-theories and how they interact is essential for understanding development (Marlow et al., 2019), and this study contributes to that understanding. Furthermore, this study contributes to the adjustment of guidelines regarding the identification of developmental delays in South African children, as it provides an understanding of their developmental profiles. The developmental assessment of these children may be tailored to this developmental profile to suit these children’s needs. Further studies on developmental characteristics of children across LMICs are required to tailor developmental resources and programmes and to inform intervention approaches making sustainable contributions to service delivery that are both family-centred and community-based.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Thuthuka Funding Grant (TTK170512230728) from the National Research Foundation (NRF).
Ethical Approval
Ethical clearance was obtained from the Research and Ethics Committee, Faculty of Humanities, University of Pretoria (GW20160607HS).