
Abstract
Holding and restraining children during non-urgent clinical procedures continues to be surrounded by uncertainty and mired in controversy. This review aimed to locate, appraise and map the evidence related to health professionals reported and observed practice of holding and restraining children, from birth to 16 years, for clinical procedures. This scoping review, conducted in April 2022, was based on the Joanna Briggs Institute protocol. Screening and full text review resulted in the inclusion of 30 papers. In total, 14 different terms were used to refer to the act of holding or restraining a child for a procedure, in many papers the action of holding was not defined. Professionals report the main factors influencing their decisions to use restraint and/or holding were the age of a child, with younger children being restrained or held most frequently; a child’s behaviour; and concerns around a child’s safety. Professionals also report that they can perceive pressure from parent/carers to hold or restrain their child and describe how holding practices can be influenced by service and organisational pressures. Health professionals, mainly nurses, continue to report ethical and moral tensions linked to their involvement in the restraint or holding of a child against their will for a clinical procedure. Evidence indicates a need to move practice forward as the issues identified in paediatric practice are long-standing and historical.
Introduction
Children often have to undergo painful and uncomfortable clinical procedures, such as vaccinations, administration of medication, blood tests, and radiological examinations (ISupport Team, 2021). Evidence indicates that they are not always adequately prepared for such procedures (Bray et al., 2019a; 2019b), and may experience anticipatory anxiety and uncertainty (Racine et al., 2016), this can lead children to become distressed and be held against their will whilst the procedure is conducted (Bray et al., 2016; Bray et al., 2019a; ISupport Team, 2021).
Holding children is reported as a common and unquestioned part of paediatric practice (Bray et al., 2016, 2018, 2019a; ISupport Team, 2021; Lombart et al., 2020). However, there is limited understanding of the impact of holding on children, both in the short- and long-term (Demir, 2007; Racine et al., 2016).
Terms such as holding, physical restraint, clinical holding, physical intervention, restrictive practice, restraint and immobilisation are often used interchangeably in practice and in the literature without careful consideration or acknowledgement of their meanings and definitions (ISupport Team, 2021; Lombart et al., 2020; Svendsen et al., 2017). Holding or restraining a child for a procedure continues to be surrounded by uncertainty and controversy, and tensions may arise due to ethical and moral issues, especially those related to protecting children’s rights (ISupport Team, 2021; Lombart et al., 2020).
Despite calls over many years from professionals, academics and researchers to challenge the use of holding and restraint within paediatric practice for non-urgent procedures (Collins, 1999; Hull and Clarke, 2010; Jeffery, 2002; Robinson and Collier, 1997), little progress seems to have been made in reducing the use of physical holding and restraint for non-urgent procedures. There has recently been increased awareness, particularly in the United Kingdom, of the need to reduce the use of restraint with children, specifically children with learning or intellectual disabilities (Government, 2019; Ridley and Leitch, 2021) and those within specialist care settings (Government, 2019). However, there continues to be relative silence in challenging the use of holding and restraint in general paediatric practice.
Recently an initiative by the international iSupport collaboration, has launched the rights-based standards for children having tests, treatments, examinations and interventions which includes definitions and boundaries to the use of holding and restraint within paediatric practice (ISupport, 2021; ISupport Team, 2021). Within these standards a supportive hold is defined as a hold where a ‘child feels calm, secure and settled during a procedure and agrees to the procedure and positioning and/or does not express signs of refusal’, whereas a restraining hold is defined as ‘any action to prevent a child moving freely against their choice or will while expressing signs of refusal’ (ISupport Team, 2021). These definitions aim to provide additional clarity to current descriptions of restraint as ‘any method which involves some degree of direct force to try and limit or restrict movement’ (Ridley and Leitch, 2021). As stated above, the use of holding and restraint for children’s procedures is complex and continues to be surrounded by uncertainty.
There is a need to map the current evidence linked to health professionals reported and observed practice in the use of holding and restraint in order to gain increased understanding of this phenomenon, identify gaps and inform the development of new studies. Previous reviews which have focussed on the holding of children for procedures (Bray et al., 2015) were published 8 years ago, and focussed on an ethical consideration of the evidence from professionals, parents and children. This review adds contemporary consideration of key issues in relation to health professionals reported and observed practice and their views of holding and restraining children for clinical procedures.
Aim
To locate, appraise and map evidence related to health professionals reported and/or observed practice and views of the use of holding and restraint of children for clinical procedures. This review addresses the following questions: ⁃ How is the holding and/or restraint of children for clinical procedures defined and described by health professionals? ⁃ How has the holding and/or restraint of children for a clinical procedure been investigated? ⁃ What factors do health professionals report as influencing the use of holding and/or restraint for children’s clinical procedures? ⁃ What are the gaps in the evidence?
Methods
A scoping review based on the protocol developed by the Joanna Briggs Institute [https://jbi.global/] was performed to map the breadth of evidence on the topic, clarify the concepts/definitions used within the literature on this specific subject, identify key themes and topics within the evidence and identify knowledge gaps to inform the development of new studies (Peters et al., 2021). We paid particular attention to search for all terms used to describe the concept of holding including holding, clinical holding, restraint, immobilisation, restrictive practice, restrictive intervention, therapeutic holding, comfort positioning, comfort holding and supportive holding.
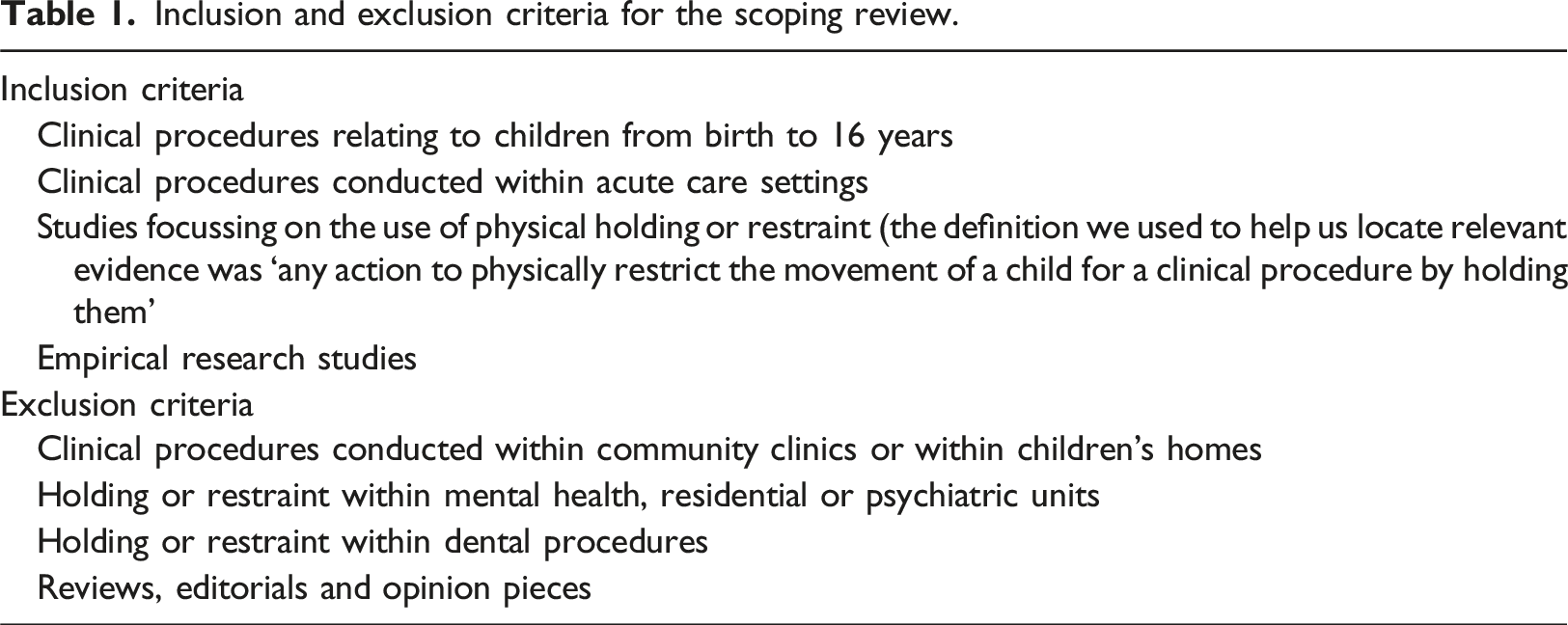
Inclusion and exclusion criteria for the scoping review.
The database search process was operationalised in June 2021, updated in April 2022 and supplemented with an additional search to add terms identified as absent in January 2024 (but still focussing on evidence published up to April 2022).
The search process was conducted in three steps (Peters et al., 2021). In the first stage, the search was limited to analysis of the most commonly used words and terms in the titles and abstracts of the articles in the MEDLINE database; this aided the preparation of the search strategy. In the second stage, searches were performed in MEDLINE, LILACS, Web of Science, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Scopus, ScienceDirect and Embase using the keywords structured according to the PCC framework (JBI); Population (Children), Concept (Holding and restraint) and Context (clinical procedures within acute care services). Thus, for the search of articles in the databases, the following Health Science Descriptors (DeCS) and Medical Subject Headings (MeSH) were considered: Infant; Child, preschool; Child; Adolescent, Teenager, Youth, Young People, Paediatric, Restraint, physical; Immobilization; Critical pathways; and Facilitated tucking, crossed by the Boolean operators AND and OR with the keyword Holding.
In the third and final stage, the references of the articles included in this scoping review were consulted to identify studies that had not been detected in the previous stages. Two reviewers (da Silva, RA and Tordivelli, RS) independently completed the three stages. The third reviewer (Garcia de Avila, MA), who had previous experience in designing scoping review studies, verified any divergences. Any disagreement between the reviewers was resolved through critical discussion with the third reviewer.
The evidence was synthesised by two reviewers who thoroughly and critically read the papers included in this scoping review. For data extraction, a table was constructed, which included the following items related to the study: authors, country, language, study design, study context (procedures, setting) and study participants. The data extraction table also mapped key elements related to the reported practice of holding; the term or definition used to refer to holding or restraint; the reference to any holding or restraint techniques or specific positions; processes around consent or assent for the holding practice; the person/s who undertook the holding practice or restraint and the reported role of parent/s and any factors reported as influencing the decision to hold a child for a procedure. As this scoping review aimed to locate and map the nature of the evidence in relation to the topic, an assessment of the quality of the papers was not required (Arksey and O’Malley, 2005), therefore, formal quality appraisal of the included papers was not performed.
Characteristics of the 30 scientific articles included in the scoping review presented in chronological order.
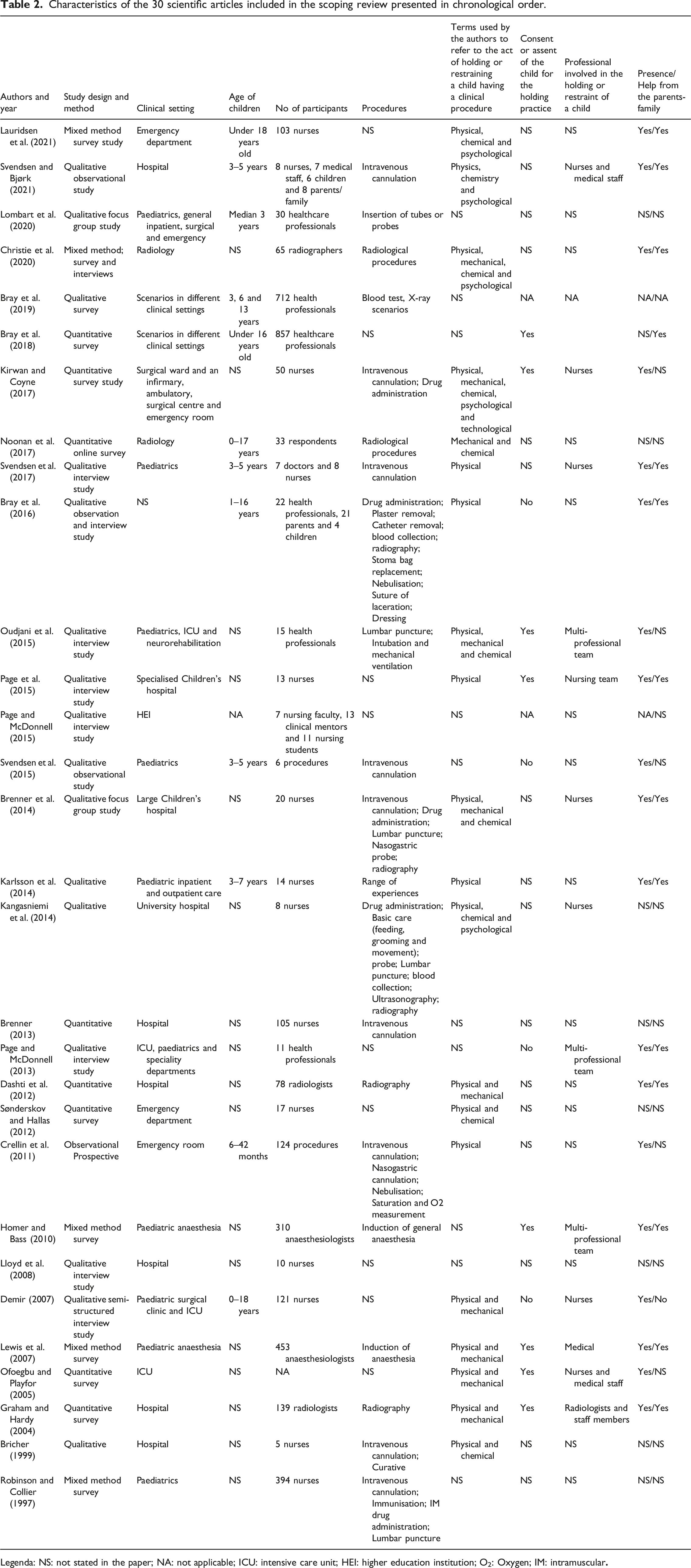
Legenda: NS: not stated in the paper; NA: not applicable; ICU: intensive care unit; HEI: higher education institution; O2: Oxygen; IM: intramuscular
Terms used within the review papers to refer to the act of holding or restraining a child for a clinical procedure.
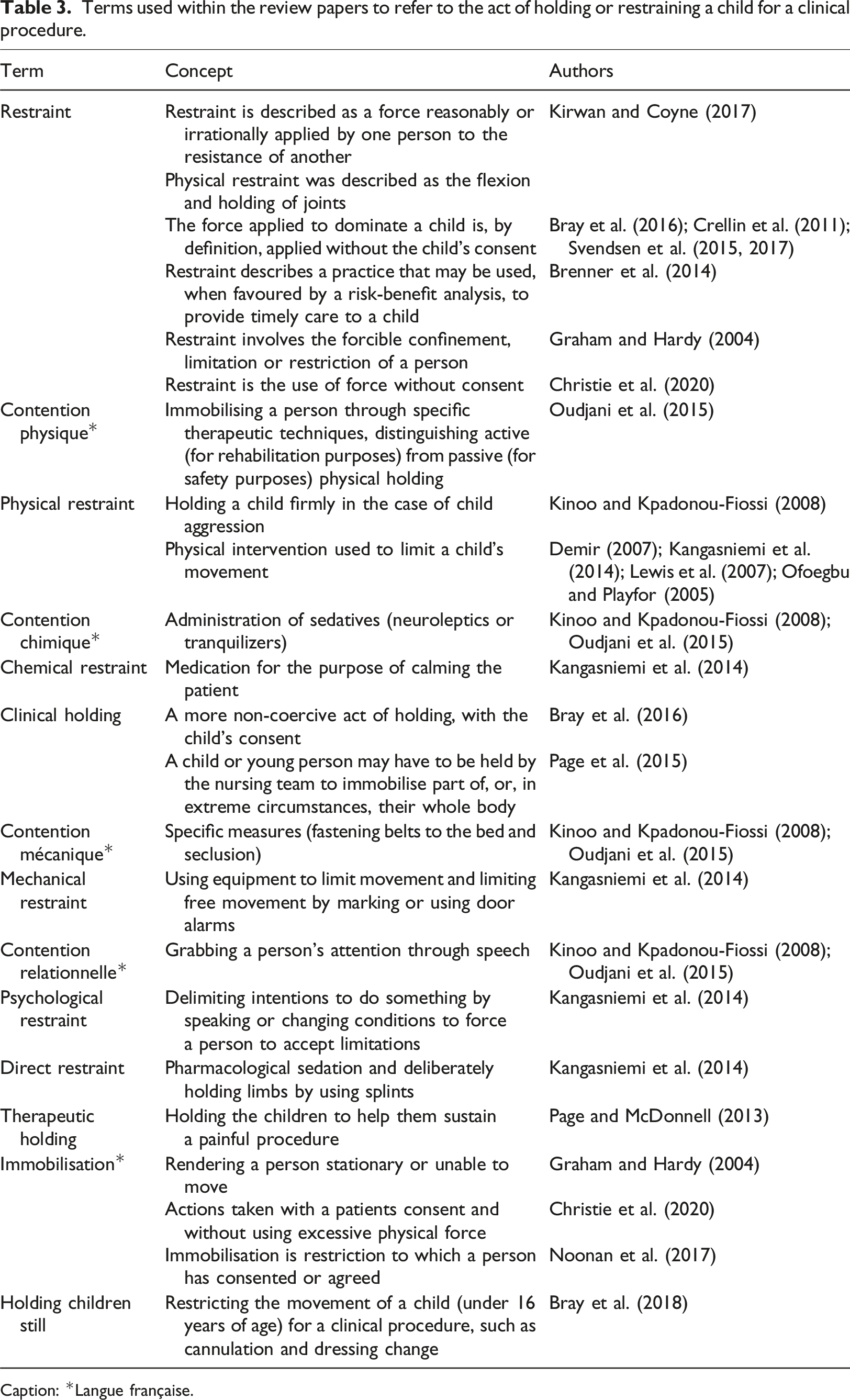
Caption: *Langue française.
Results
Identification, screening, eligibility and inclusion were reported based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) statement (Peters et al., 2021). Overall, 25 scientific articles out of the 7.018 identified were mapped after careful reading of the title abstract, and full text (Figure 1). Following the reverse search, with the consultation of the bibliographic references cited in the 25 articles included, five more articles were added, yielding a total of 30 studies that made up the corpus of analysis. PRISMA-ScR flowchart describing the article search and selection process.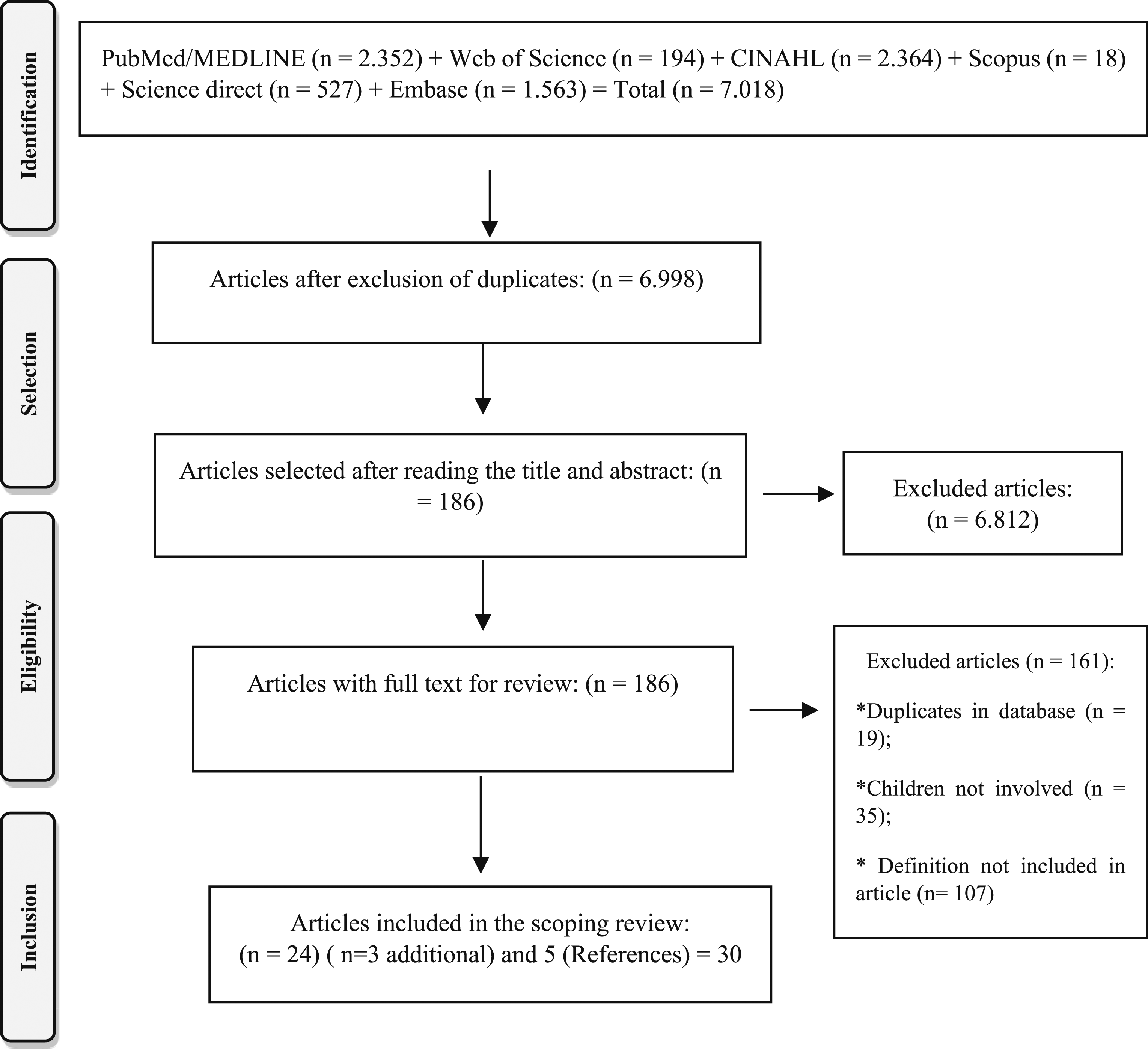
The 30 studies included were published between 1997 and 2021. The number of studies published in relation to this topic has increased over the years, with only 8 (26.7%) published before 2010 and 22 (73.3%) since 2010. Most studies investigated the reported practices and views of health professionals (n = 25; 83.3%). The health professionals who participated across the studies (n = 3.635) included nurses (Brenner, 2013; Brenner et al., 2014; Bricher, 1999; Demir, 2007; Kangasniemi et al., 2014; Karlsson et al., 2014; Kirwan and Coyne, 2017; Lauridsen et al., 2021; Lloyd et al., 2008; Page et al., 2015; Robinson and Collier, 1997; Sønderskov and Hallas, 2012), anaesthesiologists (Homer and Bass, 2010; Lewis et al., 2007), radiographers (Christie et al., 2020; Dashti et al., 2012; Graham and Hardy, 2004; Noonan et al., 2017), and some studies included multi-disciplinary health professionals (Bray et al., 2019a; Bray et al., 2016, 2018; Lombart et al., 2020; Oudjani et al., 2015; Page and McDonnell, 2013, 2015; Svendsen and Bjørk, 2021; Svendsen et al., 2017). Most of the studies used qualitative approaches (n = 16; 53.3%); including observational methods (Bray et al., 2016; Svendsen and Bjørk, 2021; Svendsen et al., 2015), interviews (Demir, 2007; Lloyd et al., 2008; Oudjani et al., 2015; Page et al., 2015; Page and McDonnell, 2013, 2015; Svendsen et al., 2018), focus groups (Brenner et al., 2014; Lombart et al., 2020) or surveys (Bray et al., 2019; Bricher, 1999; Kangasniemi et al., 2014; Karlsson et al., 2014; Noonan et al., 2017; Sønderskov and Hallas, 2012). Some of the studies adopted quantitative (n = 9; 30.0%) designs including descriptive surveys (Bray et al., 2018; Brenner, 2013; Crellin et al., 2011; Dashti et al., 2012; Graham and Hardy, 2004; Kirwan and Coyne, 2017; Noonan et al., 2017; Ofoegbu and Playfor, 2005; Sønderskov and Hallas, 2012). Five studies (16.7%) used a mixed methods design (Christie et al., 2020; Homer and Bass, 2010; Lauridsen et al., 2021; Lewis et al., 2007; Robinson and Collier, 1997). Many of the studies (n = 20; 66.7%) were conducted within a single health care setting (Brenner, 2013; Brenner et al., 2014; Bricher, 1999; Christie et al., 2020; Crellin et al., 2011; Dashti et al., 2012; Graham and Hardy, 2004; Homer and Bass, 2010; Kangasniemi et al., 2014; Lauridsen et al., 2021; Lewis et al., 2007; Lloyd et al., 2008; Noonan et al., 2017; Ofoegbu and Playfor, 2005; Page et al., 2015; Robinson and Collier, 1997; Svendsen and Bjørk, 2021; Svendsen et al., 2015, 2017; Sønderskov and Hallas, 2012).
The clinical procedures that the children underwent were detailed in 21 studies (70.0%) and included intravenous cannulation (Brenner, 2013; Brenner et al., 2014; Bricher, 1999; Crellin et al., 2011; Kirwan and Coyne, 2017; Robinson and Collier, 1997; Svendsen and Bjørk, 2021; Svendsen et al., 2015, 2017), medication administration (Bray et al., 2016; Brenner et al., 2014; Kangasniemi et al., 2014; Kirwan and Coyne, 2017; Robinson and Collier, 1997), insertion of tubes or probes (Brenner et al., 2014; Crellin et al., 2011; Kangasniemi et al., 2014; Lombart et al., 2020), anaesthetic induction (Homer and Bass, 2010; Lewis et al., 2007) and radiography (Bray et al., 2016; Bray et al., 2019; Brenner et al., 2014; Christie et al., 2020; Graham and Hardy, 2004; Kangasniemi et al., 2014; Noonan et al., 2017).
The type of holding or restraint most commonly used or reported as being used by health professionals was physical (n = 19; 63.3%) (Bray et al., 2016; Brenner et al., 2014; Bricher, 1999; Christie et al., 2020; Crellin et al., 2011; Dashti et al., 2012; Demir, 2007; Graham and Hardy, 2004; Kangasniemi et al., 2014; Karlsson et al., 2014; Kirwan and Coyne, 2017; Lauridsen et al., 2021; Lewis et al., 2007; Ofoegbu and Playfor, 2005; Oudjani et al., 2015; Page et al., 2015; Svendsen and Bjørk, 2021; Svendsen et al., 2017; Sønderskov and Hallas, 2012), followed by mechanical (n = 10; 33.3%) and chemical (n = 10; 33.3%). Some of the studies (n = 8, 26.7%) included reports or observations of whether children agreed (assented or consented) to being held (Bray et al., 2018; Graham and Hardy, 2004; Homer and Bass, 2010; Kirwan and Coyne, 2017; Lewis et al., 2007; Ofoegbu and Playfor, 2005; Oudjani et al., 2015; Page et al., 2015). There was wide variability in reported or observed practice in relation to how children were involved in any decisions to be positioned, held or restrained and how they provided assent or consent, and many studies did not include any detail about this aspect of practice.
Thirteen (43.3%) papers provided information as to who was holding or restraining a child for a procedure (Brenner et al., 2014; Demir, 2007; Graham and Hardy, 2004; Homer and Bass, 2010; Kangasniemi et al., 2014; Kirwan and Coyne, 2017; Lewis et al., 2007; Ofoegbu and Playfor, 2005; Oudjani et al., 2015; Page et al., 2015; Page and McDonnell, 2013; Svendsen and Bjørk, 2021; Svendsen et al., 2017). Of these, eight papers (61.5%) specified that holding or restraint was conducted by the nursing team (Brenner et al., 2014; Demir, 2007; Kangasniemi et al., 2014; Kirwan and Coyne, 2017; Ofoegbu and Playfor, 2005; Page et al., 2015; Svendsen and Bjørk, 2021; Svendsen et al., 2017), with the remaining five papers (38.5%) detailing that holding was conducted by multi-professional team members, doctors and radiologists/radiographers (Graham and Hardy, 2004; Homer and Bass, 2010; Lewis et al., 2007; Oudjani et al., 2015; Page and McDonnell, 2013). In 14 (46.7%) of the papers, parents were reported or observed as helping professionals to hold or restrain their child; and parents-family were detailed in 19 papers as often being present during the holding or restraint of their child (n = 19; 63.3%) (Table 2).
The studies were conducted in 12 countries, distributed over five continents, with the European continent having the most publications (n = 23; 76.7%). The studies examining the holding and restraint of children during clinical procedures were mostly conducted in England (n = 7; 23.3%) (Bray et al., 2016; Graham and Hardy, 2004; Lloyd et al., 2008; Page et al., 2015; Page and McDonnell, 2013, 2015; Robinson and Collier, 1997), followed by Ireland (n = 3; 10.0%) (Brenner, 2013; Brenner et al., 2014; Kirwan and Coyne, 2017) and Norway (n = 3; 10.0%) (Svendsen and Bjørk, 2021; Svendsen et al., 2015, 2017). Only five papers (16.7%) examined the use of holding and restraint across multiple countries.
The review identified that there is disparity and a lack of detail and clarity in the terms, definitions, and concepts used in the evidence to describe the practice of holding and restraining children undergoing clinical procedures. In total, 14 different terms (Table 3) were identified across the studies, with a large variability in the practices being described within these terms. This lack of clearly defined and described practice makes it difficult to interpret and draw conclusions across the evidence and has been linked to the continued challenges encountered in transparent practice around holding practices (Bray et al., 2016; Brenner et al., 2014; Svendsen et al., 2017).
The factors reported by health professionals as influencing their decisions to use holding or restraint in order to complete a procedure on a child.
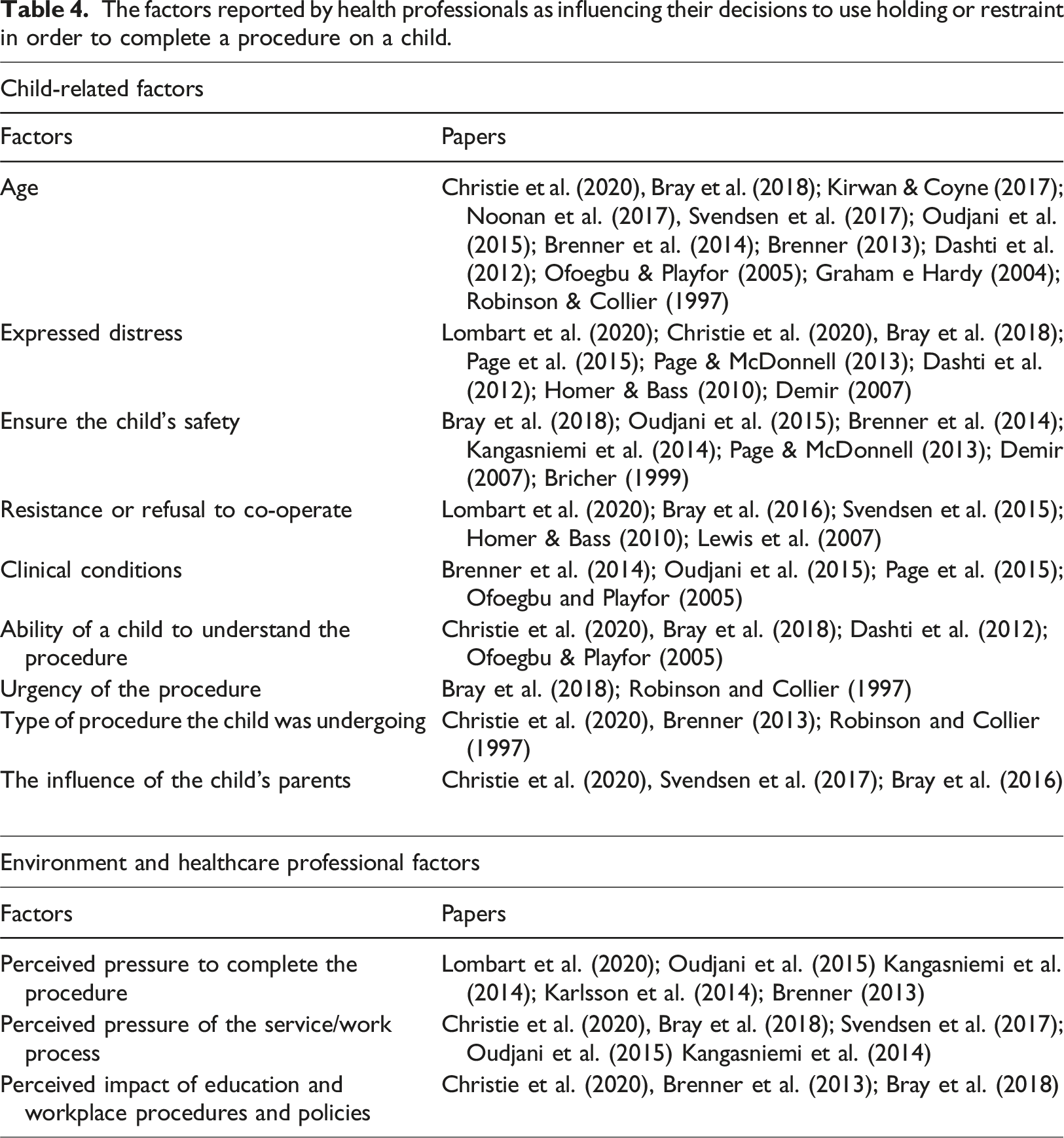
Health professionals reported that their decision to hold or restrain a child to complete a procedure was also influenced by factors broader than an individual child’s characteristics. These factors include the influence of a child’s parent wanting the procedure completed (Bray et al., 2016), parents not being able to persuade their child to co-operate (Christie et al., 2020; Svendsen et al., 2017), the perceived pressure to complete the procedure, to ‘get it done’ (n = 5; 16.7%) (Brenner, 2013; Kangasniemi et al., 2014; Karlsson et al., 2014; Lombart et al., 2020; Oudjani et al., 2015) and perceived pressures within the clinical department or organisation (n = 5; 16.7%) (Bray et al., 2018; Christie et al., 2020; Kangasniemi et al., 2014; Oudjani et al., 2015; Svendsen et al., 2017).
Evidence shows variability in the impact of policies, guidance, education or training on health professionals’ reported use of holding and restraint within paediatric practice. Professionals identified a need for more training and education in holding practices (Christie et al., 2020). Education and training in holding and restraint has been linked to professionals reporting holding children less frequently (Bray et al., 2018), however, in contrast, nurses were shown to be more likely to restrict a child if they had prior training on safe holding techniques (Brenner, 2013). Professionals report a low awareness of resources such as policies, tools and guidelines to inform the holding of children for procedures within their clinical setting (Bray et al., 2016, 2018; Christie et al., 2020; Dashti et al., 2012; Kirwan and Coyne, 2017; Lewis et al., 2007; Lombart et al., 2020; Noonan et al., 2017).
Health professionals described in the qualitative studies how restraining or holding a child against their will for a clinical procedure caused them to feel moral distress (Bray et al., 2016) and breaches the trusting relationship they have with a child (Bricher, 1999). Professionals also acknowledged the impact of forcefully holding a child against their will could have on the child, ‘scarring them for life’ (Bray et al., 2019) and have negative implications for future procedures ‘in the long run’ (Karlsson et al., 2014).
Despite this the holding of children for clinical procedures is reported as being used very frequently or frequently (Bray et al., 2018; Brenner et al., 2014; Lauridsen et al., 2021; Noonan et al., 2017), across a range of settings. Holding was reported by professionals as a helpful technique when a procedure just needed to be completed quickly and a child was upset and could not be ‘reasoned with’ (Bray et al., 2019) or holding was ‘the only way to manage them’ (Brenner et al., 2014), and the ‘only option for young children’ (Christie et al., 2020). Several papers included reports from professionals that holding or restraining a child for a procedure just happened (Svendsen et al., 2017), was accepted practice or ‘uncontested practice’ (Page and McDonnell, 2013; Svendsen et al., 2017), often inevitable (Bray et al., 2016; Svendsen et al., 2017) or described as a ‘necessary evil’ (Christie et al., 2020).
Discussion
This scoping review aimed to understand how the holding and/or restraint of children for clinical procedures is defined and described by health professionals, what factors influence professional practice in relation to the use of holding and restraint, how holding and/or restraint been investigated and what gaps remain in the evidence. The overarching finding of this review (of the evidence) is that despite the restraint and holding of children undergoing clinical procedures being the subject of research, discussion, conjecture, and investigation for over 20 years, the evidence is still dominated by reports of this practice (restraint and holding) occurring frequently as part of daily practice in paediatric care, with health professionals expressing concern about this practice, especially when children are held against their will (Bray et al., 2016; Brenner, 2013; Lombart et al., 2020). The main findings of the review will be discussed under the three objectives.
Blurred boundaries and unclear practice; how is the holding and restraint of children for clinical procedures defined and described by health professionals?
The evidence highlights that health professionals use a wide variety of terms in their daily work to describe the practice of holding or restraining a child during a clinical procedure (Lombart et al., 2020; Svendsen et al., 2017). The lack of consensus and the variety of terms, evident in the literature can exacerbate the uncertainties of health professionals working in paediatric care regarding the holding or restraint of children for clinical procedures (Bray et al., 2016; Svendsen et al., 2017). This review highlights that without clear boundaried definitions and descriptions of practice, it can be very difficult at times to see where practice ‘tips’ (Bray et al., 2019) from minimal, supportive holding to restraint.
The review highlights that the diversification of terms could be linked to a perceived need over time to acknowledge and portray less contentious practice (ISupport Team, 2021). Health professionals have more recently expressed some degree of discomfort with the term ‘restraint’ because it implies implicit violence (Lombart et al., 2020) and sub-optimal practice (Bray et al., 2016) and the restraint of children goes largely unspoken about (Svendsen et al., 2017). Thus, although practice remains mainly unchanged, the semantics used to describe holding and restraint has evolved whilst still being clouded by unclear and varied definitions and terminology (ISupport Team, 2021; Lombart et al., 2020; Svendsen et al., 2017). The authors support the call for increased transparency and clarity of terms to describe holding and restraint within paediatric practice and hope that recent work by ISupport (2021) to delineate ‘supportive holding’ from ‘restraint’ helps to move this challenging part of practice forwards.
Balancing children’s best interests against service pressures; What are the reported factors which influence health professionals’ decisions to use holding or restraint for clinical procedures?
The practice of using holding or restraint to complete a procedure was reported as depending on factors related to the child undergoing the procedures (young age, distressed behaviour and safety), as well as the context health professionals were working within (lack of time, resources and service pressures). Health professionals report justifying holding or restraining a child by the belief that ‘it is best to just get it [the procedure] done as quickly as possible’ (Bray et al., 2019; Lombart et al., 2020). What factors professionals weigh up when deciding what constitutes ‘best’ for a child is complex and seems to be dependent on numerous factors, including work and service pressures. Whilst many professionals work within resource constrained health services, this context, or the best interests or agendas of the adults involved should not drive or define practice to the extent that professionals forcefully hold or restrain a child for a non-urgent procedure. The interests of professionals and organisations should never be prioritised at the expense of a child’s best interests and rights (ISupport, 2021).
The review shows that, despite professional guidance indicating that holding and/or restraint should only be used as a ‘last resort’, this is often not the case, and there is a continued and real need to explore alternatives to the use of holding and promote ways of working to gain the cooperation of the child and parents/family (Bray et al., 2015; Kirwan and Coyne, 2017). Strategies shown to improve children’s experiences of procedures include; ensuring children and their parent/carers are prepared for procedures and are involved in procedural choices, ensuring children are communicated with based on their preferences in a way which develops trust and rapport and ensuring that a child has appropriate analgesia, distraction and is supported by the adults around them who listen to them and act on any expressions of upset or resistance. These strategies should form the basis of health professional education and training, with a need for more robust evidence examining the impact of education on holding practices.
A call for action; What are the gaps in the evidence?
Gaps in the current evidence were identified. Studies published on the subject are centred mainly within European countries, with only four studies gaining international perspectives. It is important that the evidence is expanded to examine reported and observed practices and views from health professionals working in different social, cultural and economic contexts. The majority of the evidence is self-report and drawn from descriptive quantitative or qualitative studies, often from single health care sites. There is a lack of robust large-scale quantitative studies as well as longitudinal studies to map the longer-term impacts of the use of restraint on children, parents and professionals. There is also a need for improved reporting of the age of the children featured within published research, this would help collate and amass evidence and help health professionals to think strategically about the approaches they might use in practice. Evidence focusses on the individual child or professional factors which can lead to the increased use of restraint or forceful holding and there needs to be more evidence relating to organisational factors and responsibilities, including the role of policies and education in shaping practice.
Limitations
The results presented in this scoping review need to be considered critically, because the evidence analysed, regarding the practice of holding and restraining children during clinical procedures, is mostly self-reported by health professionals. This review did not include evidence of the impact of the use of holding or restraint in the short- and long-term for children and parents/family. Although the review included children aged between birth and 16 years, we did not include specific terms such as ‘infant’ and ‘new-born’ within the search strategy which may have influenced the evidence we located.
Implications for practice
This review highlights the need for a renewed focus and critical conversation around the practice of holding or restraining children for non-urgent clinical procedures. Professionals need to be able to identify, openly acknowledge and justify any decisions and actions they make to hold or restrain a child for a procedure. Health professionals need to be educated and aware of strategies to promote children’s positive procedural experiences and alternatives to holding and restraint and be empowered to enact these strategies within their workplace.
For practice to change, national and local policies, organisational systems as well as individual health professionals need to be clear on what constitutes restraint and to be committed to ‘think differently’ to challenge holding and restraint practices. Finally, we emphasise that health professionals need to familiarise themselves with new international standards which aim to prioritise the short- and long-term wellbeing of children and reduce the use of restraint in procedural practice (ISupport Team, 2021).
Conclusion
This scoping review investigated the holding and/or restraint of children undergoing clinical procedures and mapped current issues that require further investigation and reflection.
The results highlight that the use of holding and restraint for children’s non-urgent procedures continues to be reported as common or frequent practice. Younger children, children who resist or refuse procedures, and those who express distress are reported and observed as most likely to be held or restrained. There remains high levels of variability and inconsistency in the terms used within the literature to define and describe the practice of holding children for procedures, creating difficulty in comparing and analysing the evidence.
The review highlights that despite holding and restraint being a contentious issue for many years, professionals continue to report uncertainty and ethical conflict in a similar way to 20 years ago. There is a need for more solution-focussed large-scale research conducted collaboratively with multi-disciplinary professionals, children and parents to begin to move practice forward. There is a need to expand the evidence to include procedural practice within developing countries to explore the use of holding and restraint within different social and cultural contexts.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by Grant No. 28/2019 – CAPES/COFEN. “Tecnologias de Apoio à Sistematização da Assistência e Gestão em Enfermagem: Contribuições do Mestrado Profissional para o Estado de Tocantins” and PROGRAMA DE APOIO A PROGRAMAS DE PÓS-GRADUAÇÃO DA ÁREA DE ENFERMAGEM.