
Abstract
Nurses caring for children hospitalised with a serious illness are optimally placed to advocate for truthful health information. This study explored the phenomenon of truth-telling as experienced and perceived by nurses caring for seriously ill children when parents are contemplating a non-disclosure directive. Data were collected through semi-structured interviews and analysed using Interpretative Phenomenological Analysis (IPA). The thematic analysis identified four themes, including, Child’s absence from the health communication conversation, Child and family’s access to health information, Assessment of the child and family’s understanding for the purpose of communicating health information and Nurse communication after physician communication. Despite access to online medical information and the provision of diagnostic results directly to patients, nurses continue to employ self-regulation strategies, upholding traditional practices of disclosure, before employing a supportive role for parents and children. Nurses’ partnership with the child and family can support the implementation of policies and practices allowing participation and shared clinical decision-making through open and honest communication, ultimately contributing to positive care outcomes.
Keywords
Introduction and background
Truth-telling in health care is defined as disclosure of relevant medical information to patients (Muaygil et al., 2025). In contrast, non-disclosure is a deliberate act of withholding, medical information including partial withholding and delayed disclosure (Beauchamp and Childress, 2019; Tuckett, 2004; Zolkefli, 2018). The United Nations Convention on the Rights of the Child affirms a child’s right to access and participate in decisions affecting them, provided it is not harmful (United Nations UN, 1989).
In a paediatric clinical setting, important health information, such as a child’s diagnosis or prognosis, is most typically relayed to parents or guardians first (Limb, 2019). Nurses play a supportive role in assisting parents to then relay this information to children (El Ali et al., 2023). A delicate balance exists between accuracy and comprehensibility when explaining treatments and interventions to children (Grootens-Wiegers et al., 2017). Information for children should be framed in developmentally appropriate ways, for comprehensibility (Grootens-Wiegers et al., 2017), and parents may not feel equipped to do this.
When truth-telling constitutes distressing or bad news, what to tell children becomes more challenging. This can sometimes influence a parent’s decision to impose a directive to withhold health related information from their child (Arabiat et al., 2011; El Ali et al., 2023, 2024). Consequently, non-disclosure may take several forms including, partial withholding, complete withholding, evasion, lying, omission or ‘sugar coating’ (Tuckett, 2004). There are subtle but important differences between these practices, for example, sugar coating the truth, refers to disclosing a difficult truth by adding an aspect of hope which includes presenting bad news while adding reassurances such as, ‘it’s cancer, but there are lots of treatments available’. Conversely, parents may direct nurses to lie - presenting an untruth, such as telling a child who is being palliated that they will be having curative surgery (El Ali et al., 2024).
What is not understood is how nurses practically enact these directives. Understanding truth-telling practices within a non-disclosure directive can promote critical thinking about how nurses can act as advocates for children and subsequently support families effectively (El Ali et al., 2025).
Nurses are integral in the provision of healthcare; however, little evidence is published on how non-disclosure directives, particularly in a digital age impact how nurses practice when they are asked not to tell. A gap was identified in nurses’ experiences of non-disclosure directives, considering the number of hours nurses spend with patients at the bedside.
Aim
To explore the experience and attitudes of nurses’ phenomenon of truth-telling in practice as perceived by nurses caring for seriously ill children.
Methods
Design
Phenomenology, a branch of philosophy interested in the lived experiences from the perspective of the human being living it, is widely used in health sciences, particularly nursing, as it is useful in examining the experience of the human person, which is a central focus for nurses (Moxham and Patterson, 2017). Phenomenology focuses on essential structures that make the lived experience possible challenging traditional subject-object distinctions (Jarrett and Throop, 2021).
Findings of this paper emerged using Smith et al. (2022) Interpretative Phenomenological Analysis (IPA) (Smith et al., 2022), with each step of thematic analysis audited and validated by the research team undertaking data analysis.
Study setting and recruitment
Participants were recruited through purposive sampling where nurses who had cared for seriously ill children within 5 years preceding data collection were eligible to participate. In this paper, the term seriously ill children will reference children with medical conditions requiring hospitalisation or chronic conditions that significantly impact daily life and necessitate ongoing treatment and monitoring (El Ali et al., 2023).
Recruitment was undertaken through professional bodies (e.g. Australian College of Children and Young Peoples Nurses [ACCYPN]), snowballing and social media platforms (e.g. LinkedIn) (Palinkas et al., 2015).
Inclusion and exclusion criteria
Recruitment was guided through a purposive sampling strategy used to include Australian nurses who were not in their graduate year. This was to ensure responses were based on experienced nurses who were not in the consolidation phase of their career – hence continuing to learn. Post graduate qualifications were included in demographic information as it provided context to the participants clinical expertise, role capability and preparation. The study was interested in nurses who had specifically cared for children aged between 4 and 12 years old who were hospitalised with a serious illness within the preceding 5 years.
Data collection
Sample interview guide.
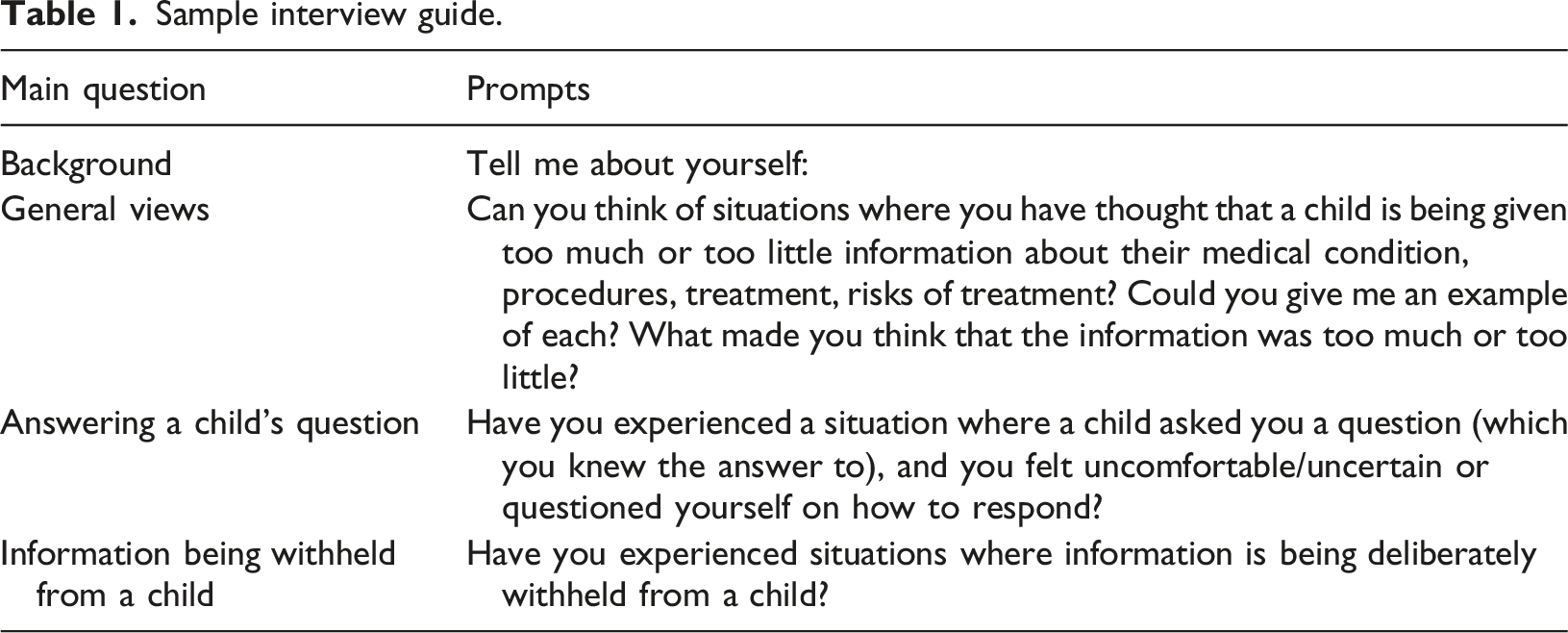
Authenticity in the interpretation of the data was critical to the study. Researcher reflexivity was achieved through the demonstration of the characteristics of good qualitative research which includes the sensitivity to context, commitment and rigour transparency and coherence and impact and importance (Yardley, 2000).
Data analysis
Data were analysed using Smith’s Interpretive Phenomenological theoretical framework. Smith’s Interpretative method of qualitative analysis ‘is informed by hermeneutics, the theory of interpretation’ (Smith et al., 2022: 3) and guides a process of interpreting how participants make sense of their experiences (Smith et al., 2022). This method of analysis prioritises depth and richness of subjective insights (Pietkiewicz and Smith, 2012; Smith et al., 2022; Smith and Osborn, 2015). This study was conducted by an ‘insider researcher’ who interpreted data within the lens of their own experiences as a paediatric nurse – a member of the professional community within which this research was conducted (Greene, 2014: 1; Dwyer and Buckle, 2018).
Several rounds of thematic analysis, sorting and synthesis of the data were undertaken to ensure full immersion and understanding of the findings and the justification of the emergent themes (Creswell and Poth, 2018; Pietkiewicz and Smith, 2012). This was guided by Smith et al.’s, (2022) seven steps for interpretative phenomenological analysis including reading and re-reading the data to support full emersion, note taking for descriptive-Linguistic and Conceptual connections, development of emergent themes, then identification of connections and patterns across themes to present a narrative of the meaning emerging in the data (Smith et al., 2022).
Rigour and reflexivity
Interpretative phenomenology does not hold to the concept of bracketing; however, reflexivity was essential in ensuring any presumptions or biases were addressed. The primary research undertook a pre-interview preparatory self-check, including reflecting on the importance of listening, not volunteering information, and be aware of leading questions. A peer review of data collection processes was instrumental in maintaining rigour during thematic analysis (Hales, 2013; Liamputtong, 2020).
Ethical considerations
The study was approved by the University of Melbourne and the Royal Children’s hospital Melbourne Human Research Ethics Committee [HREC] (37283A).
Non-identifying pseudonyms were assigned to all participants.
Findings
Interviews were conducted online (n = 25) through Zoom or Teams, or face to face (n = 2) in the participants place of employment and ranged between 28 and 68 min in duration. Recruitment commenced prior to COVID-19 allowing initial face-to-face data collection. Researchers were based in Melbourne, Australia and experienced prolonged lockdowns (262 days), necessitating a transition to online interviews. This shift proved advantageous, enabling recruitment of a more heterogeneous sample comprising participants from diverse backgrounds and a range of clinical settings, including rural, regional, remote, and metropolitan locations.
Participant demographics
Twenty-six nurses participated in the study, twenty-four identified as female, two identified as male. Approximately half had between six to 10 years’ nursing experience (50%), 61%, were between 30 and 39 years old, and 81% had cared for both adult and paediatric patients. Participants will be attributed pseudonyms.
Participant demographics.
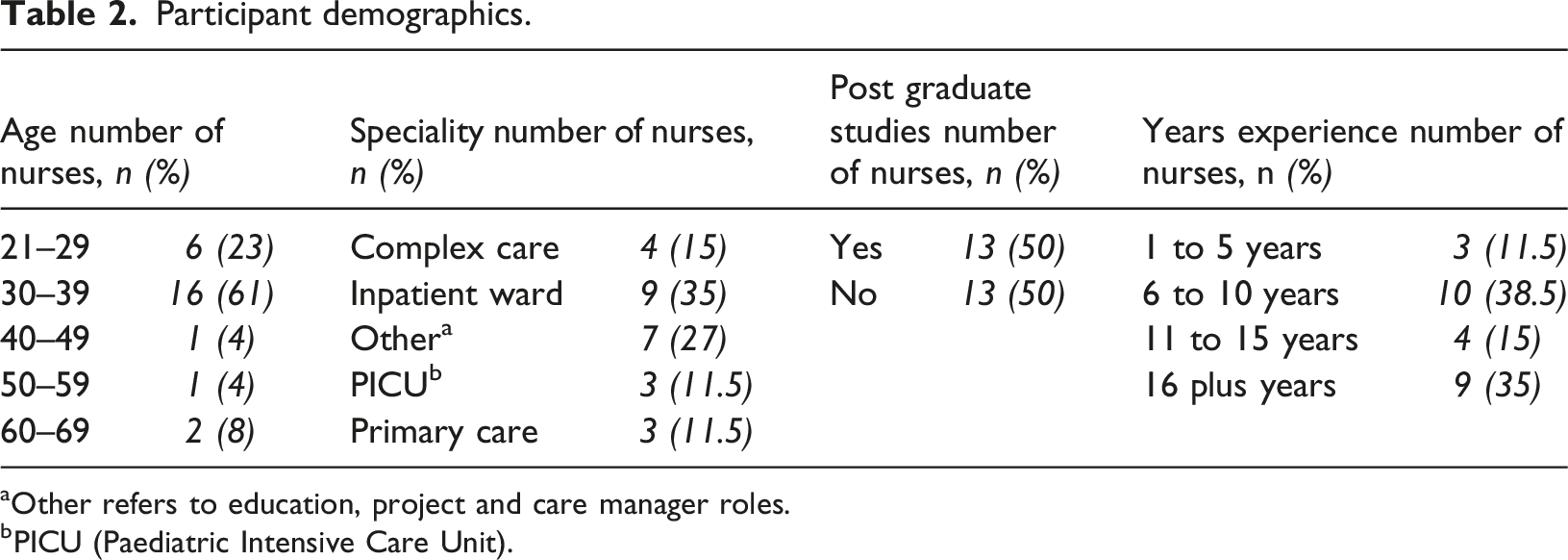
aOther refers to education, project and care manager roles.
bPICU (Paediatric Intensive Care Unit).
Data analysis resulted in four themes
• The child’s absence from the health information sharing conversation. • Child and family’s access to their health information • Assessing the understanding of the child and family for the purpose of communicating health information and • Nurse communication after the information disclosure by the physician.
Themes developed represent how nurses perceive and engage with truth-telling practices in the context of non-disclosure of medical information. A significant insight—one that is acknowledged but underexplored in the literature from the nursing perspective—is that children are typically excluded from the initial health communication discussion, which typically occurs between physician and parent (Carlsson et al., 2021).
The absence of the child from the health communication conversation
Participants described health information sharing, usually initiated by availability of diagnostic information where diagnosis or prognosis was not favourable. Nurses described whispers and withholding of information by health care teams including nurses, until a complete picture of information was available to the physician. This would then prompt a meeting with parents. Initially, nurses articulate that typically children were absent from initial diagnostic conversations to allow parents to process the information. ‘First initial conversation is had where, like, the blood results are abnormal, or we're noticing something on an image… and I noticed that a lot of the time, when that conversation was being had, it was usually with the parents and not the child’ (RNP10)
If a non-disclosure directive was implemented, children would be removed from any further health information related conversation especially if cognitively able to understand the information. ‘I think if we were very, very worried about the child, no, they would take the depending on the child's age. But I think anyone that was pre-teen age, they would take the child would be taken out of the room’. (RNP2)
Nurses justified removing the child as a means to offer initial support for parents in light of a serious diagnosis or prognosis. ‘So, then you take them into like a treatment room, and… it is a bit dependent on the kid… it doesn't make me that comfortable when we have to do it that way, but you kind of have to… just sort of have to explain to parents… what you can offer them in terms of support’. (RNP9)
Children’s absence from the health information conversation was common practice. Participants even described medical rounds as exclusive where health information was discussed in front of children but not directly to children. ‘It's a group of doctors with one computer, and they're in a room talking about a child, but they're not talking to the child. They're talking to each other. And sometimes they will ask a question, or whoever's there with the child, but very rarely, it's almost like a conversation’. (RNP10)
Participants also provided examples of what they perceived as positive health communication, even when communicating bad news. One example was related to a situation where investigations were being undertaken on a young girl for a suspected cancer diagnosis. ‘There was one particular family with a little blonde girl. And they were really great and said that that straw that you've got in your hand… you know how you've been feeling sick, we're going to try and help you feel a bit better by giving you some medications… there were some families who were really great at that communication with their child…’ (RNP10)
The child and family’s access to health information
Participants reported that access to health information by parents and/or patients can occur directly via the healthcare team, through email from pathology or imaging which include pictures and through online searches such as Google.
The evolution of how people source health information over the past 30 years was discussed during the interviews. The participants were clinically current and worked in environments supported by digital technologies. This varied from fully to partially digital. Nurses expressed the challenges of their work environment when patients and their families had access to google searches for answers to health queries, digital results, and diagnostic images as it made managing or controlling the process of information sharing more challenging. ‘The access to information is just incredible at the moment, with internet, I find it quite disturbing that parents will Google information, health information on the internet, and take it as the truth before they've even spoken with doctors…. and you find out they've Googled it …and… they do this because they are second guessing the experts… ’ (RNP11)
Traditionally, diagnostic results and outcomes of examinations were communicated at the will and discretion of the healthcare professionals. Digital information transfer allows patients and families other avenues of accessing diagnostic information. Despite this, nurses were still reluctant to disclose information they possessed about their patients’ medical status. One participant was asked if she would disclose health information given families now have access to their own test results, she responded. ‘They can look it up. I don't think it's my place to give them blood results’. (RNP8)
Where patients sought information through online resources, nurses expressed concern at misinformation they may access, as well as misinterpretation of information in relation to the child’s presenting signs and symptoms. ‘One boy had googled; he wanted to know what a DNR was… so he'd been googling….’ (RNP2).
Despite readily available access to various sources of information, participants described instances where not even parents were given information, let alone children. ‘The parents didn't even really understand. Like, I think this child ended up having to be on TPN [Total Parenteral Nutrition] for a little while. And then, you know, had a lot of issues with refeeding syndrome and things… but …those… interventions were just done without… really explaining to the family what was being done’. (RNP7)
Assessing the child and family’s understanding for the purpose of communicating health information
Participants agreed that children should be given health information and should be told the truth; however, nurse participants felt they had to consider a child’s and families’ language and health literacy capability. One nurse participant emphasised the importance of the nurse’s role in supporting comprehension of health information. ‘… that's where nursing really should bloom… we can be the conduit in the… provide the health literacy… one of the main scopes of nursing because we have more time in theory than someone who's doing a ward round’ (RNP1)
Participants described adjusting their language tailoring to their perception of the child’s understanding ‘So long as that information is given to them in a way that is age appropriate, … you just you have to explain to them, what's going to happen to them in an age-appropriate manner’ (RNP5)
Participants supported transparency in information transfer and spoke with concern about how some families had information withheld from them due to judgements about intellectual understanding of the family or how medical teams perceive certain family units. ‘… I think that we should be perhaps being a bit more transparent … it really depends on the family, though and it needs to be quite individualised. And that's tricky… when you don't have that time to assess… the comprehension level of every individual family when they're first admitted’. (RNP7).
Nurse communication after physician communication
The participants indicated they were often present during health information transfer to parents. They observed that parents often don’t absorb details associated with medical diagnosis, treatment and prognosis. Their role as nurses was to be ready and available for any follow up questions parents have. ‘At critical times, there's a limit of how much information people can absorb so, we often find that we have to have repeated conversations. So, by being there at points of conversation, you can kind of go - remember in the meeting, this was said…’ (RNP8)
In some situations, nurses are left to pick up the pieces following disclosure of a poor diagnosis or prognosis: ‘It takes a bit of time to process that, and kind of come back to it a few times… but because they always say, do you have any questions, and they say no, but then two hours later I have all the questions. Sorry. But I think it's just it's just the nature of tough news and emotion that takes time to process’. (RNP4)
Parents usually required time to process information before approaching their allocated nurse for support in making health information more understandable.
Nurse participants articulated they would not present families with any new information and only repeat what they believed had already been communicated. ‘I will repeat what parents have already been told or things that are very obvious at the bedside… Sometimes you've got families that just want to a medic a doctor to tell them, not the nurse’. (RNP8)
If the news was bad, a conversation may occur between health care professionals prior to approaching families with information to prepare them for the family’s response. One participant described doctors pre-warning nurses when they thought parents would be distressed by a diagnosis. ‘When the parents ready to come in, they might be distressed, upset, whatever. So, if they can, they'll try and give us a bit of a heads up’. (RNP5)
Participants stated quite clearly that it was not their role to disclose information to parents or child for the first time, even if it was not bad news. When asked if she would disclose diagnostic results to a patient and family, RNP10 stated ‘I'm not going to say to them, these look normal, you're fine, I would probably just have this conversation where I'm like, these… look relatively normal. Your child looks well… I'm not concerned at this point, but I… can only give you general advice on what I see on these blood test results, ultimately you will have to speak to the doctor’. (RNP10)
Nurse participants stated they were trained in respect of hierarchical roles within the institution and would be clear on the communication regarding diagnosis and prognosis coming from the doctor. ‘We don't give out those results, unless the doctor has seen them first, and been able to tell us the information about what is going to happen, because it's my personal opinion, I don't know what the other nurses think they may be happy to give out that information I'm not’. (RNP11)
Findings represent a relationship between themes that emerged as a result of an interpretative phenomenological analysis. Participants described their perception of the practice of truth-telling in the context of how the information is passed from one person to another, like a baton in a relay. While parts of the findings align with truth-telling practices in adult settings, consideration of child and family care influences as well as the importance of cognitive assessment from the perspective of the nurse has yet to be explored.
Discussion
This research aimed to present an exploration of the experience and attitudes of nurses’ phenomenon of truth-telling in practice as perceived by nurses caring for seriously ill children. Participants provided rich detailed accounts regarding the impact a non-disclosure directive had on their practice.
Nurse participant responses were interpreted to represent how health information is transferred from one point to another. Researchers identified a point of opportunity between the time parents receive health information and the decision to tell or not tell the child. This information transfer was metaphorically represented as a baton in a relay.
When a child and parent present to a hospital the information baton is transferred from family member to triage nurse. This baton is then passed through to the doctor, diagnostics, then back to the doctor before finally being handed back to parents who then decide whether children are allowed to receive the information baton. This is illustrated in Figure 1. The transfer of information ownership.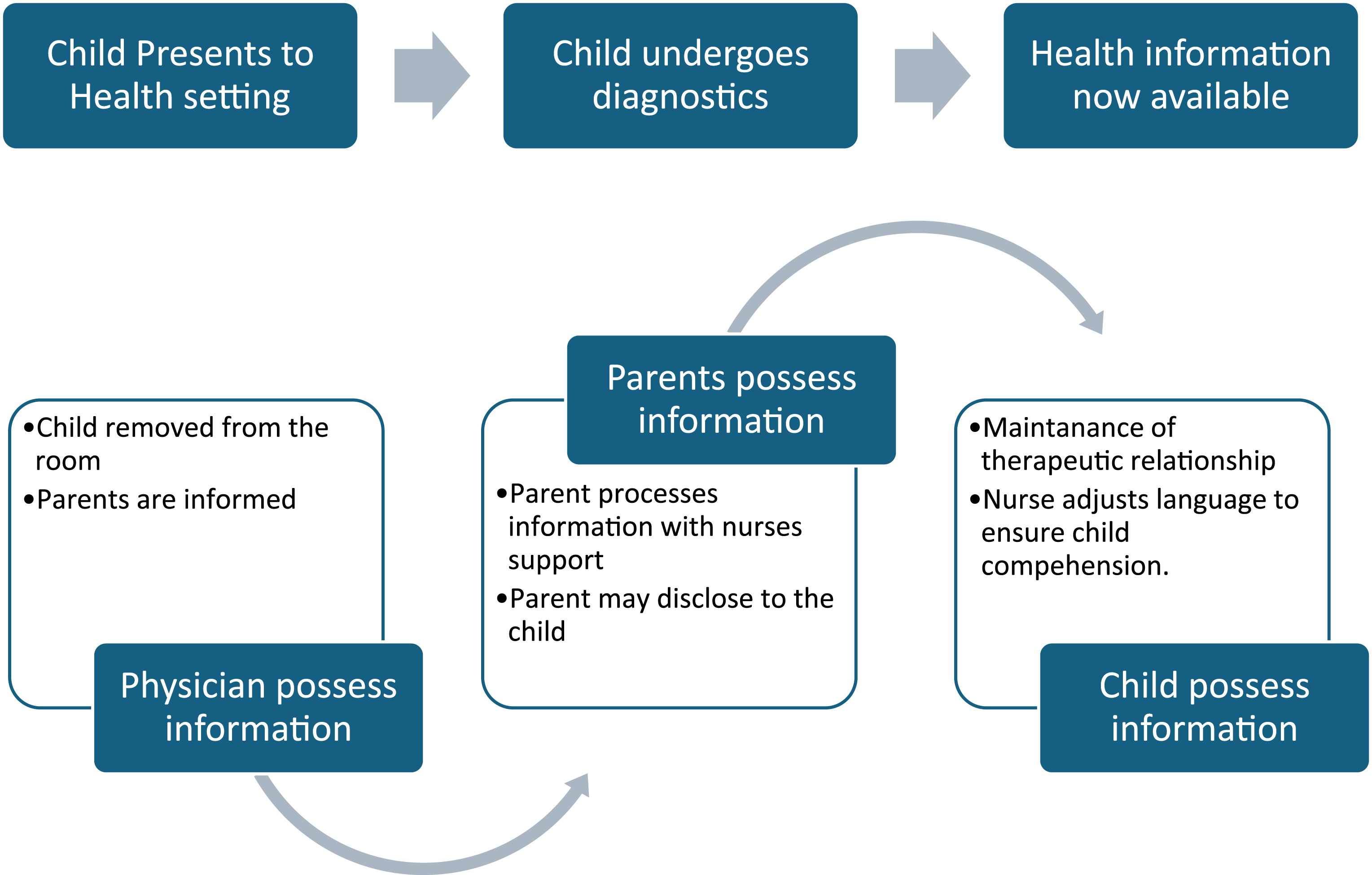
Nurses’ role in this information transfer, as described by the participants in this study, is supportive only (El Ali et al., 2023; Myburgh et al., 2018). This is consistent with literature that puts nurses in a position of picking up the pieces after a physician passes the information baton to parents (Kazdaglis et al., 2010). Participants expressed having to explain and assist parents and children (if they were told) in understanding what doctors had said but confirmed doctors will make initial disclosures. This is also supported by the findings of a systematic review, which demonstrated that nurses position themselves as support persons in health information transfer (El Ali et al., 2023). Interestingly, participants did not observe opportunities to begin conversations on how parents would then pass information to children directly after receiving health information themselves.
These findings which represent how health information is communicated in a paediatric healthcare setting are consistent with published literature (Coyne et al., 2014). Typically, information is transferred from physicians to parents, and not directly to children (Hudson et al., 2019). This doctor-to-parent transfer is significant because it places decision-making power with parents in deciding if, when and what, information children receive (Hudson et al., 2019). When parents initiate a non-disclosure directive; transfer of information to children can be interrupted, as represented by Figure 2 – hence, the health information baton remains in the parents’ possession. This is where nurses can play a significant role in supporting parents to initiate health information conversations to their children. This window presents an opportunity for nurses to intervene where there may be a potential decision to withhold the truth from children by facilitating the health information transfer in a supportive environment (El Ali et al., 2024). The transfer of information ownership (passing the baton) stops with the parents.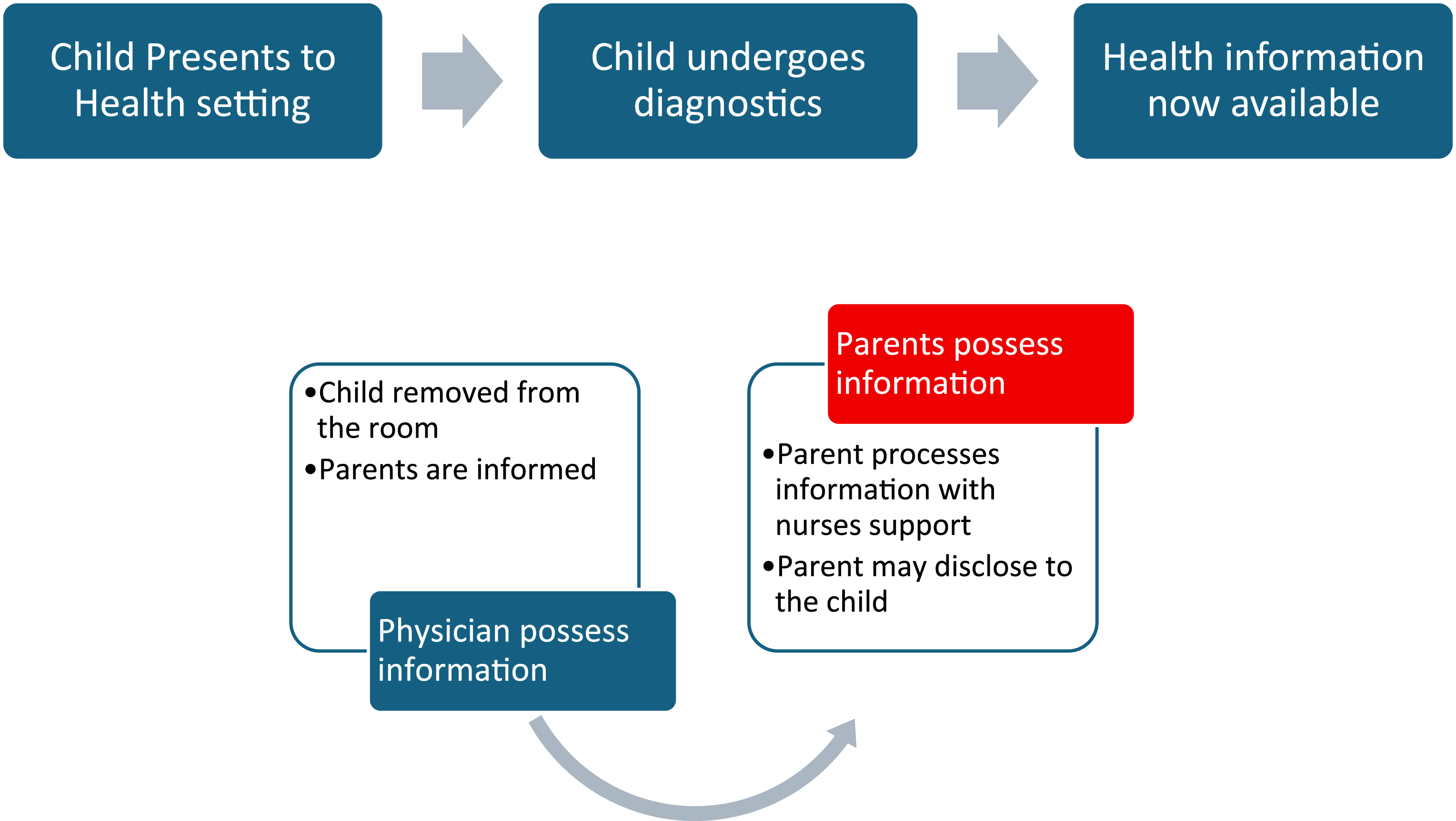
Nurses are well placed to be conduits in initiating how health information will be passed to children (Moura Bubadué and Cabral, 2019). Nurses are generally excluded from conversations where non-disclosure directives are decided (El Ali et al., 2024). Participants believed that physician’s hold significant power in terms of decision-making, referring to hierarchical and systemic structures in health care (Ricciardelli et al., 2022). Empowering nurses to participate in decision-making and truth-telling conversations supports the therapeutic relationship within a child and family centred framework that puts children at the centre of the care encounter, and the family provides integral structures for support (Clinical Excellence Queensland, 2021; Davies et al., 2025; Foster and Blamires, 2023).
A child’s right to know
A simplified version of the convention on the rights of the child by UNICEF Articles 12 states, ‘Children have the right to say what they think should happen when adults are making decisions that affect them and to have their opinions taken into account’ and Article 13 states, ‘Children have the right to get and to share information, as long as the information is not damaging to them or to others’ (United Nations, 1989).
Figure 2 visually presents information transfer that includes children in health conversations with or without parents aligning with the convention. This would be a more radical step and may go against parents’ wishes and preferences of them being filters to how and what information children receive (Coyne et al., 2014; Limb, 2019). Participants indicated there was no pathway or protocol that directed truth-telling to children, rather, there was an expectation that health information would eventually filter down from parents to children after health information disclosure.
Traditional information transfer pathways do not consider contemporary digital clinical environments and internet access (National Digital Health, 2024). The Australian National Digital Health Strategy vision states ‘By enhancing the use of digital technologies and data, it enables informed decision-making, providing people better access to their health information when and where they need it, improved quality of care, and personalised health outcomes’ (National Digital Health, 2024). Access to information can have pros and cons, and can be considered empowering (Hägglund et al., 2022). Participants did not present positive attitudes toward patients and families having access to their own information, nor did such access influence their decision to initiate a truth-telling conversation.
Arguably, parents and children may be more empowered through their access to online information. Literature regarding the use of online sources for self-diagnosis is sparce. In 2019, industry website – Medical Director published a report titled ‘Dr Google: How self-diagnosis impacts clinical care’. This report identified that over half of Australia’s population regularly turned to Dr Google to search for signs and symptoms, with the highest demographic of users being between 18 and 24 years old. The report resulting from a survey of over 1500 Australians discussed how health care practitioners have modified consultancy conversations to correct misinformation that originated through self-symptom checking on ‘Dr Google’ (Bardsley and Middleton, 2019).
Searches for information related to children’s health may be more frequently undertaken by parents motivated by feelings of inadequate health information transfer or lack of compassion with regard to their information needs (Bardsley and Middleton, 2019; Stukus, 2019). Proliferation of Artificial Intelligence (AI) in recent years could exacerbate this situation.
Participants alluded to being aware that children, particularly adolescents, were searching online for health information. They theorised this was resultant from a withholding scenario, when children and specifically adolescents were excluded from the health information conversation, consequently prompting children to seek information online and noting that lack of confirmation from parents and the medical team may have psychological impacts on the children who are not told the truth.
A discussion piece by Scott et al. (2018) explored whether adolescent use of Dr Google was helpful. Scott et al. (2018) supported participants views that information seeking behaviours via google or AI in adolescents were motivated by challenges in ‘accessing health services due to location, inexperience, lack of knowledge and concern over stigma’ (Scott et al., 2018: 1282). This work did not consider children facing serious illness or circumstances where children were searching for information that had been intentionally withheld ultimately supporting the work undertaken in this study. Gaps in the literature around impacts of access to health information for children hospitalised with a serious illness and experiencing a non-disclosure directive should be further explored.
Health information sourced from public sites has a potential to misrepresent facts, compelling health care professionals to have awareness of what is available online, including initial results of a symptom search when adolescents are seeking health information. Parents in particular should be supported through active discussions when decisions regarding their children’s medical care is made based on what they have read online (Stukus, 2019).
Access to one’s own medical records is a separate paradigm for families getting information without direct interaction with a doctor. In 2022 Hagström et al., published a scoping review on children, parents and adolescents’ access to their own medical records. One focus point was the transfer of health information access from parents to children. In Australia, where this study was conducted, access to a child’s health records (including their immunisation record) remains with parents until children reach their 14th year, after which ownership is transferred to the child (MyGov, 2024). Metaphorically, the information baton no longer passes to parents before being given to the child. This then shifts how a non-disclosure directive can occur, when children of a certain age are given decision-making powers around health information ownership and access (MyGov, 2024). The objective of this transition is to enable the protection of privacy and confidentiality of adolescents as they transition to adulthood. Transition ages may vary in other countries (Hagström et al., 2022). This study focused on children below the age at which they are able to make decisions regarding their own health care; however, further study into what limits can be applied to non-disclosure directives in an adolescent population may be warranted in light of the additional complexity presented by digital health and access to on demand health information as this was outside the scope of this study.
Limitations
This was an Australian study; hence, an international perspective on nurses’ practice within a non-disclosure directive would be valuable in identifying similarities or differences in the way information access has altered how children receive health information. Cultural backgrounds of the nurses were not considered as a variable. The discussion on immediate information availability within the practice setting was an unexpected finding, also worth further exploration. This study had a limited sample size appropriate to the qualitative methodology. Further studies could use mixed methods to capture a larger sample size presenting a greater insight into how access to health information can impact truth-telling practices in a paediatric clinical setting.
Practice implications
Findings of this study demonstrated a link between initial assessment of the child and family’s access to information, communication capability and practices; and nurses’ practice of responding to a non-disclosure directive. Health communication practices by nurses were further impacted by theirs and children’s absence from the health information conversation between physicians and parents. The fact that nurses will only communicate health information after it has already been disclosed by physicians, despite some families already having gained access to diagnostics was another interesting finding.
Nurses perceived unrestricted access to online health related content presented challenges in misinformation and misinterpretation of diagnostic results which could potentially cause psychological harm and decreased dependence on medical professionals. The evolving health care landscape and access to health information by the general population may drive a change in how it is shared in practice. There may be a need to establish truth-telling practices that are adaptive to digital information and technologies access. Considering health care professionals are no longer able to restrict information flowing to children and families in their care, research into how a digital environment affects and influences the nursing practice of truth-telling is warranted.
Conclusions
Nurses are well positioned to be conduits for health information transfer from parents to children particularly when parents are reluctant or don’t have the confidence or ability to do so. Nurses enact a supportive role in the practice of truth-telling, which places them in an opportune position to implement structures that support health information transfer to the child. Further research is warranted into nurses’ experiences and understandings of how children and parents access health information outside direct communication with their healthcare provider. The digital health environment has impacted information ownership and implementing non-disclosure directives, emphasising a requirement to develop processes that support physicians and nurses aid truth-telling practices that are catered to the child’s age, stage, and cognitive ability.
Footnotes
Acknowledgements
The author would like to acknowledge the dedicated nurses who participated in this study. She is sincerely grateful to her supervisors, Professor Lynn Gillam and Dr Jenny O’Neill, for their unwavering support throughout the research. Special thanks are also extended to Ms Alycia Jacob for her generous time and insightful feedback on an earlier draft of this article, which enhanced the clarity and impact of the work.
Ethical considerations
This study was approved by The University of Melbourne Human Research Ethics Committee (37283A). All participants provided written informed consent prior to participation in the study.
Funding statement
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The participants of this study did not give written consent for their data to be shared publicly, so due to the sensitive nature of the research, supporting data is not available.
Reporting method
Findings are reported per consolidated criteria for reporting qualitative research.
No patient or public contribution
No patients, service users, caregivers or members of the public were involved in this study. Rather, this study was focused on the experiences and attitudes of nurses working in a paediatric setting.