
Abstract
This qualitative study was conducted to determine feelings of nurses caring for children affected by earthquake, and their efforts to manage the disaster using a phenomenological approach. Data were collected through one-on-one in-depth interviews and audio recordings. The data obtained from audio recordings were evaluated using qualitative content analysis method. As a result of the analysis, two main and seven sub-themes were created as Emotional Responses (Anxiety, Fear, and Helplessness), Inadequacy in Disaster Management (Inability to reach children and families, Inability to meet the needs of children and families, Inability to create safe areas, Inadequacy of knowledge and skills). These research findings have demonstrated the importance and necessity of providing psychosocial support to nurses caring for children affected by disasters, given the psychological problems they experience. At the same time, it is necessary to develop preventive strategies regarding negative situations related to the management of children in disaster.
Introduction
Earthquake is a natural disaster that has historically caused the highest number of deaths and devastating consequences (Aydınbaş, 2023; Erdoğan, 2015). Due to its geological structure and climatic characteristics, Türkiye is one of the countries where natural disasters such as earthquakes, floods, landslides, rock falls, and avalanches frequently occur (Emirza et al., 2024; Erdoğan, 2015). Many devastating earthquakes have occurred and caused loss of life and property in Türkiye (Aydınbaş, 2023; Kalanlar and Kubilay, 2015). Two earthquakes that occurred 9 hours apart on February 6, 2023 were called the Disaster of the Century and caused death and injury of many people and destruction of many buildings (AFAD, 2023; Disaster Child Civil Coordination Team Turkey, 2023; Republic of Türkiye, 2023).
Children are among the most vulnerable and fragile groups in the face of extraordinary events such as earthquakes, floods, and epidemics (Bialy et al., 2024; Fong et al., 2025; Montreuil et al., 2025; Oostrom et al., 2023). The fact that children do not have the power to meet their basic needs (shelter, food and drink, security, transportation) during disasters increases risk factors of disaster on children’s general health and safety (Dziuban et al., 2017; Özarslan et al., 2025). According to the American Academy of Pediatrics report, among groups affected by disasters, infants, children, and adolescents are the priority groups in disaster preparation, intervention, and recovery (Krug et al., 2015).
Research shows that disasters have adverse physical, psychological, emotional and social effects on children that can persist for a long time (Dutta et al., 2022; Mudiyanselage et al., 2022; Rezayat et al., 2020; Siwal et al., 2018; Tang et al., 2017). It has been determined that children experience problems in meeting basic needs such as shelter, nutrition, hygienic environment, clean water and food sources, and safety (Rezayat et al., 2020; Tang et al., 2017; Özarslan et al., 2025). It is emphasized that psychological problems such as sleep disorders, anxiety, depression, and post-traumatic stress disorder may also develop and persist over the long term. It has been emphasized that failure to adequately meet basic needs of children after a disaster may increase the risk of emotional and psychological problems developing, which could negatively affect their growth and development during childhood. This situation necessitates comprehensive assessment of children exposed to disasters at an early stage, prioritization of all their needs, and development of a systematic disaster management plan to address potential risks (Dağ et al., 2024; Krug et al., 2015).
Earthquake disaster in Türkiye
A 7.7 magnitude earthquake centered in Pazarcık, Kahramanmaraş hit Türkiye on February 6, 2023, at 04:17. Approximately 9 hours after this earthquake, at 13:24, another earthquake occurred with a magnitude of 7.6 centered in Kahramanmaraş-Elbistan struck, also affecting same provinces. These earthquakes, referred to as Disaster of the Century, devastated 108,812 km2, covering 11 provinces around (Kahramanmaraş, Hatay, Gaziantep, Gaziantep, Malatya, Malatya, Elazığ, Adana, Adıyaman, Diyarbakır, Şanlıurfa, Osmaniye, Kilis) and affected approximately 16.43% of people living in Türkiye (AFAD, 2023; TÜİK, 2022; Aydınbaş, 2023; Bardakçı and Demirtaş, 2023). Thousands of buildings collapsed, and thousands of people lost their lives or were injured (Aydınbaş 2023; Bardakçı and Demirtaş, 2023). As of March 2023, death toll was reported to be 50,873, with number of wounded reported as 108,368 (AFAD, 2023; Support to Life Association 2023). People faced problems meeting their basic needs, especially shelter, due to building damages (Support to Life Association, 2023).
The earthquakes that occurred in Türkiye on February 6 affected 4,805,662 children aged between 0 and 17. This rate constitutes 21.3% of Türkiye’s child population (Presidency of the Republic of Turkey, 2023). Due to the earthquake, many children were trapped under rubble and were referred to different hospitals for emergency intervention and treatment, while some children could not be pulled out alive from under rubble or lost their families in the rubble (Disaster Child Civil Coordination Team, 2023; Turkish Medical Association 2023). After the first earthquake, children had to stay on streets, in hospitals or in cars. The second earthquake caused a much greater destruction and number of injured and missing children increased (Ministry of Family and Social Services, 2023).
Early identification of the effects of disasters on children, planning appropriate intervention measures, and prevention of risks can be achieved through the implementation of disaster management programs developed specifically for children (NAPNAP, 2011; National Advisory Committee on Children and Disasters, 2015). Health institutions play an active and important role in the creation, implementation, and development of disaster management programs (Altman et al., 2019; Koeffler et al., 2019). Qualified health professionals equipped with knowledge and skills are needed to ensure systematic management and organization of disaster processes in health institutions (Abdi et al., 2021; Nakayama et al., 2019). Nurses are among the most active health professionals during disasters (Purta and Petpichetchian 2011; Taşkıran and Baykal 2017). Nurses provide services in many areas during disasters, especially first response, evaluation, and triage (Chan, 2010). Primary responsibility of nurses in disasters is to assess affected individuals in a timely manner, determine their care needs, plan appropriate intervention approaches, identify and manage specific groups, provide basic life support to individuals through necessary interventions in emergencies, and reduce potential risks (ICN, 2019). In addition to these, nurses caring for children in disasters undertake important tasks in determining and meeting needs of children and their family, providing a safe environment, quickly identifying children and parents in risk group and meeting their appropriate care needs (Gladston and Nayak, 2017; Goodhue et al., 2012).
Nurses have essential duties in protecting and evaluating children’s health in acute process of disaster. The National Association of Pediatric Nurse Practitioners (NAPNAP) reports that pediatric nurses have important roles in providing guidance and care for children and their families before, during, and after national and global disasters (NAPNAP, 2011). It has also been determined that disasters can negatively affect nurses’ ability to fulfill their roles and professional management skills. Many research reports indicate that disasters have negative effects on nurses and that problems are encountered in management and organization of disasters in healthcare institutions (Emirza et al., 2024; Salik et al., 2024). Literature has shown that nurses caring for disaster victims may cause managerial problems in disaster management due to insufficient areas of appropriate intervention, insufficient equipment and personnel, lack of adequate knowledge and skills, and insufficient organization and coordination (Abdi et al., 2021; Labrague et al., 2018; Nofal et al., 2018; Salmani et al., 2019). It has been reported that this process can cause anxiety, stress, feelings of inadequacy, and helplessness in nurses and can significantly affect their professional competence (Doğan et al., 2024; Nakayama et al., 2019).
Determining experiences of nurses who care for and observe pediatric groups after disasters and addressing problems encountered in disaster management process are important for development of a disaster management plan for children (Şermet Kaya and Erdoğan, 2025; Gladston and Nayak, 2017). There is evidence in literature regarding experiences and problems of nurses working in disasters (Nakayama et al., 2019; Abdi et al., 2021; Akbari et al., 2024). There is a gap in literature on emotions experienced by nurses caring for children, one of the most at-risk and vulnerable groups in disasters, during disasters and their experiences in disaster management process.
Aim
To determine emotions of nurses caring for children affected by earthquake and their efforts to manage the disaster.
Methods
Theoretical framework
This study was conducted using a qualitative phenomenological design. Qualitative phenomenological research method focuses on describing and explaining the subjective life experiences of individuals or groups in a comprehensive and unbiased way (Streubert and Carpenter, 2011; Williams, 2021). For this study, the descriptive phenomenological design proposed by Husserl et al. was employed. Descriptive phenomenological research design enables the identification and interpretation of the impact of an event or situation from the perspective of individuals. This method aims to gain an in-depth understanding of individuals’ experiences of a specific situation by examining how they experience it, what meaning they ascribe to it, and how they are affected by it (Husserl and Moran, 2012). In this regard, it is an important research method for identifying and thematizing the experiences, impressions, and perceptions shared by individuals (Heotis, 2020; Stolz, 2020). This method was used in the present study to gain an in-depth understanding of the emotions and disaster management efforts of nurses caring for children during earthquakes, as seen through their own perspectives.
Sample and sampling method
This study was conducted with nurses working in a public hospital in Elbistan, epicenter of the second earthquake that occurred on February 6, 2023. All nurses worked actively in hospital during the earthquake and subsequent periods. There are 550 nurses working in the hospital where the study was conducted. Seventy-five nurses worked in pediatric units (pediatric services, neonatal intensive care unit, pediatric emergency, gynecology service) during and after the disaster. Purposive and snowball sampling were used to reach nurses working in different clinics. Before starting the research, nurses working in pediatric clinics during and after the earthquake disaster were identified from hospital records. Inclusion and exclusion criteria were determined, and nurses who met inclusion criteria formed the sample. These nurses were then contacted via phone to explain purpose, scope, and voluntary nature of the study. An appropriate appointment day was determined for one-on-one, in-depth interviews with nurses. Since data saturation was achieved, sample size was not increased further. Ensuring data saturation indicates sufficient sample size (Morse, 2015).
Data collection
Data were collected between May 1 and 31, 2023. In this study, face-to-face individual in-depth interview technique was used. The reason for using this interview technique is to reveal intense meanings that individuals attribute to events, to provide an environment for them to express themselves comfortably within sufficient time and without being affected by other individuals (Dömbekçi and Erişen, 2022; Usku and Demir, 2023). Before interviews, permission was obtained from participants for audio recording. All participants gave permission for audio recording. Interviews were held in a meeting room during their off hours in the hospital where nurses worked. Researcher S. O. conducted the interviews. This researcher both experienced the earthquake and worked as a pediatric nurse during the earthquake. The interviewer avoided supportive and judgmental expressions and gestures during one-on-one interviews. No other observer was present during meetings. Each nurse was interviewed once, and each interview lasted approximately 35–45 minutes. Interviews were conducted in Turkish, translated into English by an experienced translator, and then checked by translators fluent in both languages.
In one-on-one in-depth interviews, the researcher asked five open-ended questions to participants: Could you describe the environment you were working in during the initial moments of the earthquake? Could you describe the problems you encountered? How did you generally observe the effects of earthquakes on children? How did you feel during interventions and care of children affected by the earthquake? What issues did you experience anxiety about while providing interventions and care for children? Could you tell us about problems you experienced during disaster management process? During interviews, questions such as 'Can you explain your reasons for not being able to manage the disaster with examples’, 'How did intense fear and anxiety affect you in your disaster management process’, 'Can you elaborate on reasons for anxiety you experienced’ were directed to participants according to flow of the interview. During the interview, the interviewer avoided judgmental expressions, gestures and mimics.
Data analysis
Data from audio recordings of one-on-one interviews were evaluated using inductive content analysis method (Graneheim and Lundman, 2004). Analyzed materials were nurses’ comments regarding their efforts in maintaining care of earthquake-affected children. After interviews were completed, researchers listened to audio recordings repeatedly and independently and transcribed them into written text using a computer. After all data were compiled into a report, they were read to participants, and data security was ensured. Statements written in the text were read repeatedly by both researchers independently of each other, and same/similar and different statements were grouped and coded. Researchers met and codes were compared, showing that the coding of both researchers was consistent with that of the other. Then, main and sub-themes of the study were determined. COREQ checklist was used as a guide for analysis.
Reliability
Research findings’ verifiability, reliability, transferability, and credibility criteria were met (Polit and Beck, 2010). To ensure reliability, interviews were audio recorded and transcribed verbatim. All authors contributed to data analysis to ensure internal validity. To ensure verifiability, two researchers conducted data analyses separately, and findings were discussed in regular meetings. Additionally, excerpts from participants’ speeches are presented in findings. To ensure transferability, socio-demographic characteristics of participants were defined, and diligent efforts were made to provide detailed methods and findings sections. After quotations, transferability of data was enhanced by indicating descriptive characteristics of participants in parentheses. In order to enhance transferability of interview content, it was translated into English by a linguist specializing in the field of interviews. The linguist determined and compared the meanings of interview content in Turkish and English. In a meeting with researchers, it was decided that necessary adjustments would be made to ensure that meanings given by participants to questions did not lose their integrity in English. The linguist made the necessary corrections, and interview responses were presented in the article. At the end of the quotations, pseudonyms have been used for the participants and indicated in brackets.
Ethical guidelines
Ethical approval was obtained from University Health Sciences Non-Interventional Clinical Research Ethics Committee. Purpose and content of study were explained to nurses who agreed to participate. Participants were informed that data obtained from voice recordings would be used for scientific purposes and that their personal information would be kept confidential. Verbal and written consent was then obtained from participants. The study was conducted following principles of the Declaration of Helsinki.
Research team reflexivity
This research need arose from our observations regarding management and organizational problems during major earthquakes in Turkey. The first author worked continuously for 7 days as a nurse in the pediatric emergency department during and after the earthquakes. During this period, while providing necessary interventions to children and their families, she also made observations. These observations revealed that parents whose children died, went missing, or could not be found, as well as children without relatives, were brought to the hospital in large numbers. Furthermore, many came to hospitals seeking refuge, believing them to be safe. This created significant chaos in the emergency department. The inadequacy of hospital resources, the shortage of healthcare professionals, the high intensity of the earthquake, and a lack of preparedness meant that this process was not well managed. The needs of children and families affected by the earthquakes were not adequately met. This intensity prevented nurses from systematically managing the process and organizing themselves, making care and treatment difficult. As a clinician and academic nurse, we observed that the strategies for solving these problems were insufficient. There are gaps in the literature regarding the problems experienced by nurses in the management of children during earthquakes or other major disasters. This study provides evidence regarding the emotions and challenges experienced by nurses in managing earthquakes. It is believed that this will contribute to the development of strategies for nurses to work in a more planned and systematic manner during potential earthquakes and other disasters.
Findings
Nurses’ descriptive Characteristics(N: 30).
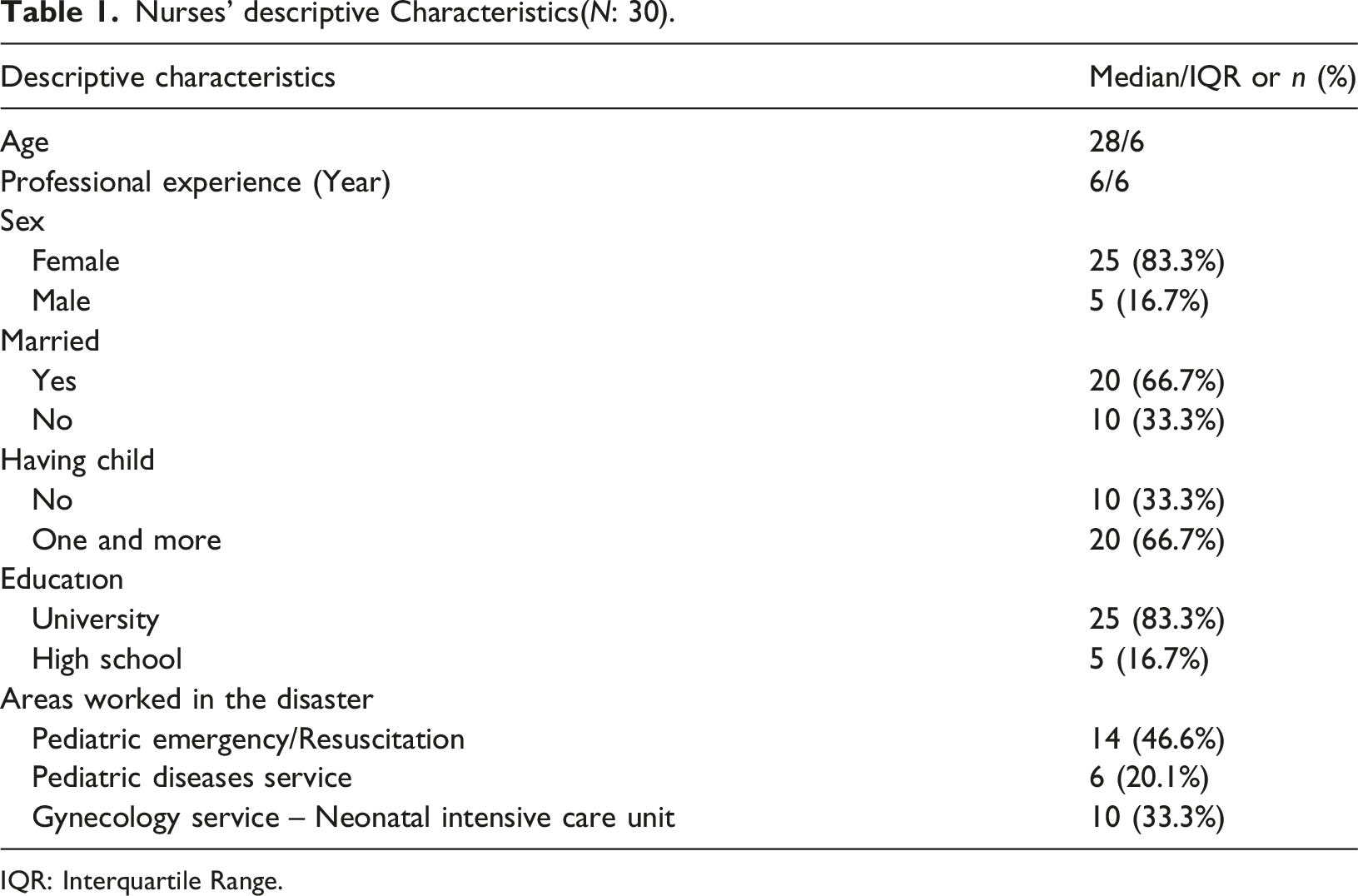
IQR: Interquartile Range.
Main and sub-themes identified as a result of qualitative content analysis of data obtained from interviews.
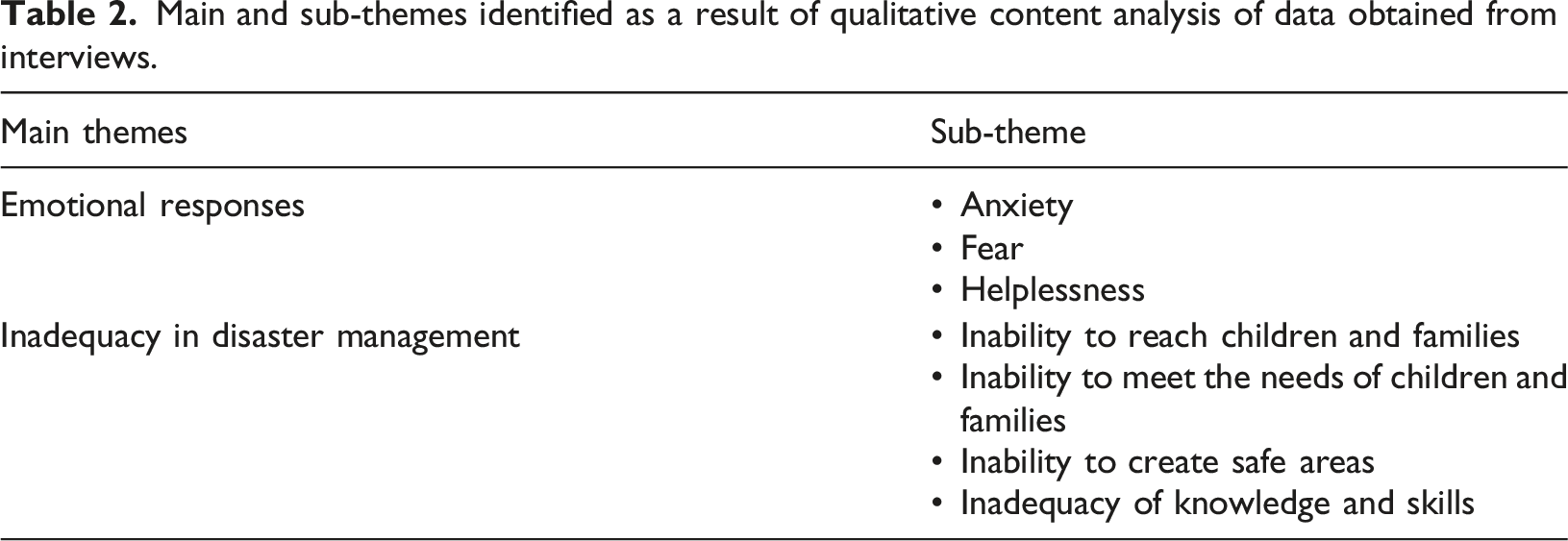
Figure 1 shows distribution of main and sub-themes based on responses given by nurses participating in the study (Figure 1). Distribution of themes formed according to Nurse’s answers.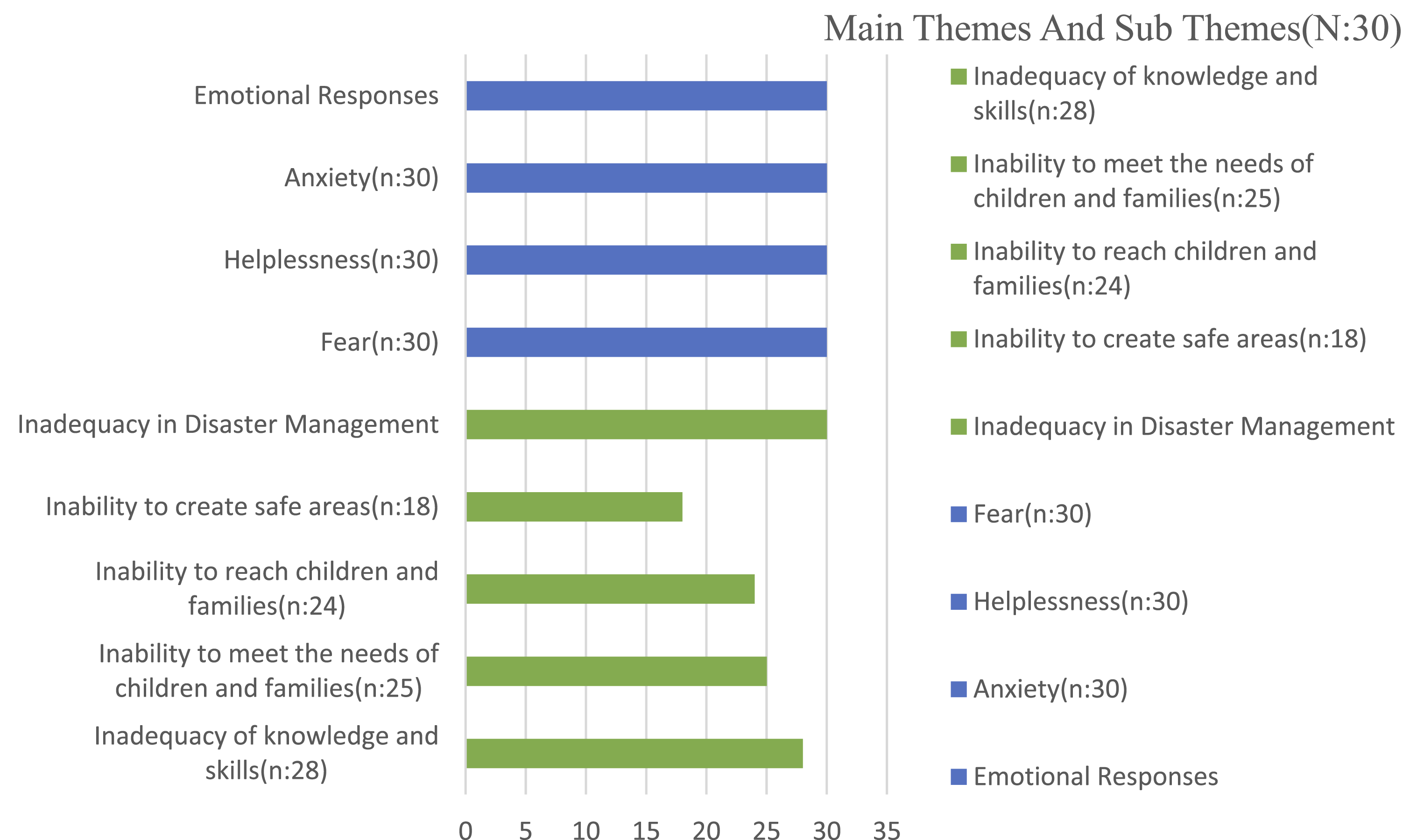
Emotions
Anxiety
The nurses reported being very worried due to the intensity of the earthquake, the ongoing aftershocks, and the uncertainty surrounding their own survival and that of their family members. They stated that the severe tremors following the second major earthquake and the high number of dead and injured increased these concerns. They expressed their anxiety due to the unmanageable number of injured and dead children, the presence of missing and orphaned children, the hospital’s inadequate equipment and staff, and the lack of sufficient knowledge and skills to manage the disaster. “With the second earthquake, number of injured children increased even more. Our hospital is small; we do not have enough staff and equipment. There were children with severe life-threatening conditions. Hospital facilities were limited, and we could not transfer them to another hospital at that time. Everything was destroyed, and roads were closed. At that moment, I was very worried for the lives of those children…” (Fatma) “Number of preterm deliveries increased in neonatal unit, and referral to an advanced center took 10-15 hours longer. Meanwhile, our anxiety and stress increased because we had used all devices we had. If there were another preterm birth, we would have to try to keep the baby alive under much more difficult conditions because of our device shortage….” (Ayşe) “Both major earthquakes were followed by severe aftershocks. With each tremor, our fear increased. Would the earthquakes continue and intensify? In every aftershock, children were crying, and their mothers were scared. It was very difficult for us to bring them to their senses. We had problems calming children, which made us anxious and helpless…” (Hatice).
Fear
Nurses who were in hospital during both earthquakes reported that both they and children and families receiving treatment in the ward experienced fear. Nurses who were providing care during the earthquake described reactions of children and parents. They said they couldn’t control their stress and fears during the earthquake and had difficulty calming their children and families. They particularly emphasized that they observed more intense fear in unaccompanied children who had lost family members in the initial earthquake or whose family members were trapped under the rubble. “As we looked at children, we suddenly started to feel a tremor bigger than the first earthquake. All children started screaming and crying. Some children did not have their families with them. They hugged us…” (Rabia) “Pediatric clinic is on the second floor, and it shook so much that everything fell on floor. At that moment, I was taking vital signs of an injured child. The child suddenly threw himself off stretcher and fell on floor. He hit his head and hugged me…. His parents were not with him. We waited in fear…” (Elif). “On the first day, aftershocks were very frequent. After every aftershock in emergency room, children and families ran outside. But they had to return to hospital because the weather was freezing…” (Zeynep).
Helplessness
Nurses reported that they were struggling to provide care to children and systematically implement care interventions due to a lack of equipment. They reported communication problems in determining needs of children and their families, insufficient communication with some unaccompanied children, and inability to reach children’s families. They said that some children and their families felt helpless because they couldn’t adopt a solution-oriented approach to problems due to a lack of equipment to meet even their basic needs. Some unaccompanied children reported increased anxiety and feelings of helplessness due to the death of their family members or being unable to contact them for days. “…We didn't have boots or coats for children who were cold. They were waiting in emergency room without anyone with them. I felt very helpless…” (Hasret) “…Our hospital had limited facilities… We were not ready for a disaster…There were many families and children who needed us. However, we were both few in number and our equipment was inadequate. Therefore, we were helpless at times.” (Kübra) “There were many unaccompanied children in emergency room, and we were unable to reach some of their families for a long time. The second earthquake was even bigger, and number of children increased rapidly. We felt very helpless because we couldn't manage the situation…” (Zeynep)
Inadequacy in Disaster Management
Inability to reach children and families
Due to destructive impact of disasters, collapsed roads, and difficult weather conditions, nurses reported that families and children living in rural areas arrived at hospital too late. They stated that disruptions in telephone networks caused problems in establishing adequate communication between family members and healthcare personnel working in ambulances. They specifically mentioned difficulties in establishing and maintaining communication between family members and ambulance personnel for children who were scheduled to be transferred to a different center.
Nurses stated that vast majority of children rescued from rubble were transported to different hospitals by air and road. They reported problems with keeping records of children. They reported that they did not have access to information about the transferred children. They emphasized that this situation led to families not receiving sufficient information about their children and caused conflicts among family members. “While I was in emergency room, a child was brought in at the 48th hour of earthquake. Their house collapsed in the earthquake, and stove fell on the child. The mother claimed that they could not reach the hospital and ambulance teams. The child’s burns were so severe, I don’t know how he/she made it…” (Eda) “After the earthquake, we sent so many children to different provinces. Later, some families came to look for their children, but we could not help them. Rescued from the rubble, a mother came to us and said, ‘They brought my child here and then transferred to another hospital, but we cannot find out which hospital they took him/her…’” (Münevver)
Nurses stated that number of preterm births increased, they could not communicate adequately with family members after birth. They also mentioned that there were newborns pulled out from under rubble, they also had problems communicating with their families. “Transfer of many preterm babies to advanced intensive care took longer, and they stayed with us until late hours. We had problems reaching family during transfer process. Phones did not work. But we had to transfer preterm babies. We had no other choice. We transferred them to other hospitals before their families arrived.” (Münevver)
Inability to meet the needs of children and families
Nurses reported that every place where shelter and food were provided had been destroyed by the earthquake, and that children and their families had taken refuge in hospital because their homes had been destroyed or severely damaged. They emphasized that the facilities at the hospital were insufficient to meet some basic needs of the children and their families (clothing, special care needs, etc.). Nurses stated that this situation significantly disrupted care process and that they felt helpless because they were not qualified to meet these needs. They also stated that shelter and medical treatment and care needs were partially met, while nutritional needs were not adequately met. They emphasized that the large number of people affected by the earthquake and the extent of the destruction negatively impacted the ability to adequately and systematically meet the needs of children and families. “We could not meet the needs of children under our care. Many children stayed in hospital because it was the only safe place. They needed us in every aspect… yet we struggled to find solutions to their material and spiritual needs. With each passing minute, the number of dead and severely injured children increased…” (Büşra) “After the second big earthquake, most of the resources we relied upon were destroyed. For a long time, we could not meet needs of the children and parents in our care, as well as our own…” (Hacer).
Inability to create safe areas
Nurses said that they were unable to keep children away from the chaotic environment and that children witnessed many interventions. They also stated that weather conditions were very bad, that some children had been exposed to the cold and trapped under rubble for a long time, and that they observed that children were cold. It was found that number of unaccompanied children increased over time, the hospital did not have suitable areas for permanent accommodation of unaccompanied children. It was determined that all areas of hospital were providing care to earthquake victims and that most individuals were meeting their accommodation needs. This situation was found to make it particularly difficult to create safe spaces for orphaned children. Nurses also mentioned lack of security personnel in creating safe spaces for orphaned children. Some nurses stated that they mostly focused on treating injured children and could not think about children’s need for shelter in safe spaces during treatment. “Children in emergency department witnessed every intervention. They saw lifeless bodies in corridors. They observed people’s reactions. I don’t even want to speculate what was going through their minds. We didn’t have a safe space for the children…” (Büşra). “We couldn’t ensure safety of children because we didn’t have such a team. We solely focused on attending to injured children and couldn’t see other children…” (Kübra).
Inadequacy of knowledge and skills
Nurses stated they realized during this process that they did not have sufficient information about disaster management. They stated that there were deficiencies in knowledge and awareness regarding the rapid and comprehensive assessment of children, the identification of care needs, the analysis of child groups at-risk, the management of unaccompanied children, and meeting the needs of specific child groups. Nurses stated that they were familiar with first aid and basic life support measures for children, but were unable to apply them during the earthquake. They also that anxiety and fear they experienced had a negative effect on their critical thinking and decision-making. It was also emphasized that despite the large number of injured and dead children, the lack of intervention equipment was a significant factor in managing the process. “…We weren’t expecting a devastating earthquake and didn’t know what to do. What we knew of disaster management was insufficient…” (Ayşe) “More severely injured patients were coming in and were hurriedly brought to emergency room. We accepted every patient without question and didn’t follow a specific triage. We provided care in same area for those who were deceased, severely injured, and those with minor injuries…” (Hacer) “…Chaos ensued in emergency room, and we lacked sufficient experience and skills regarding the disaster process. We tried to educate each other and intervene at the same time…” (Zeliha).
Discussion
This study was conducted using in-depth qualitative interviews to determine feelings of nurses caring for children affected by the earthquake and their efforts to manage the disaster. Results of this study show that nurses providing care for children in disasters experience emotions such as anxiety, fear, and helplessness, and are unable to manage disasters systematically. Some results of this study are similar to results of other studies examining experiences of nurses who care for individuals in disasters ( Abdi et al., 2021; Doğan et al., 2024). To the best of our knowledge, no research has been found that examines emotions experienced by nurses caring for children during disasters and their efforts to manage disasters. This study has produced results that could fill an important gap in literature and serve as a guide for nurses working in this field.
Major disasters are significant events that cause fear and anxiety among individuals living in affected areas. Wide-ranging impact, potential loss of life and property, possibility of recurrence, and post-disaster uncertainty are among main causes of fear and anxiety. Some studies in literature have shown that healthcare professionals experience emotions such as anxiety, fear, inadequacy and helplessness during disasters (Abdi et al., 2021; Johal et al., 2016; Li et al., 2015; Salik et al., 2024). Johal et al. found that devastating effects of the earthquake on nurses’ workplaces caused these emotional reactions (Johal et al., 2016). It has been reported that violent tremors during earthquakes in Turkey have caused nurses to experience psychological difficulties such as inadequacy, fear and helplessness (Doğan et al., 2024; Emirza et al., 2024; Salik et al., 2024; Topal et al., 2024).
This study also showed that nurses caring for children experienced anxiety, fear and helplessness due to aftershocks they experienced. Furthermore, efforts to care for children and families, who are among the most vulnerable groups, high number of lost and orphaned children, inability to reach groups of children at risk, and failure to provide safe spaces for children were found to be significant factors contributing to increased anxiety. It was also found that psychological reactions experienced by children and their parents negatively affected nurses’ emotional processes.
It has been reported that psychological problems experienced by nurses during critical processes such as disasters can negatively affect continuity of care and management of critical processes. It has been emphasized that strategies aimed at ensuring and strengthening continuity of systematic care are necessary for nurses providing care for children in all circumstances (Kim and Chae, 2025; Ramritu et al., 2002). Ensuring the continuity and manageability of children’s care by strengthening child-parent-nurse interaction may reduce likelihood of nurses experiencing stress and other psychological problems (Kim and Chae, 2025; Lewis et al., 2019). Therefore, it is clear that nurses working in disasters must be psychologically prepared and that it is important to develop their anxiety and stress management skills during disasters (Dağ et al., 2024; Johal et al., 2016; Şermet Kaya and Erdoğan, 2025).
Similar to other studies, this research also found that nurses had insufficient knowledge and skills in disaster management, experienced organizational and coordination problems, and were unable to manage disasters adequately (Abdi et al., 2021; Salik et al., 2024). Severity of the disaster, coupled with nurses’ inadequate level of training in disaster management, lack of team preparedness, and low level of awareness regarding potential disasters, may contribute to these problems. In this study, nurses reported that the disaster was severe and widespread, that children and families were unable to reach hospital, that needs of children and families could not be met, and that their knowledge and skills were insufficient for disaster management. It was found that nurses experienced difficulties in continuing treatment and care of children due to insufficient equipment and personnel, inadequate organization and coordination, and an inability to develop solution strategies. A study revealed that nurses experienced coordination problems due to insufficient equipment, coupled with high number of children admitted to emergency department (Dağ et al., 2024).
It was also found that during the earthquake, while providing care, nurses were unable to keep adequate records of lost and orphaned children and experienced difficulties in establishing safety and secure areas for children. It was observed that inadequacy of equipment (personnel and intervention equipment) and solution strategies increased their anxiety and helplessness. Nurses caring for earthquake victims in Iran struggled to manage the process amid psychological difficulties due to inadequate organization and a lack of human resources (Abdi et al., 2021). It was found that nurses who experienced the Wenchuan earthquake were psychologically unprepared for violent tremors and the process of managing the disaster, and were unable to cope psychologically with the situation (Li et al., 2015). It was reported that nurses who responded to the disaster of the century in Turkey experienced various psychological difficulties such as inadequacy, fear and helplessness in management of the disaster, along with severe shocks (Doğan et al., 2024; Emirza et al., 2024; Salik et al., 2024; Topal et al., 2024). These results show the necessity of increasing nurses’ knowledge and skill levels regarding critical processes such as disasters, increasing their level of preparedness, creating disaster action plans, and resolving managerial issues (Abdi et al., 2021; Li et al., 2015; Salik et al., 2024).
Nurses must possess sufficient knowledge and skills to carry out necessary interventions during disasters and be prepared for such events (ICN, 2019; WHO, 2014). World Health Organization (WHO) emphasizes that healthcare professionals must be sufficiently equipped to respond to all disasters, regardless of their severity (WHO, 2014). However, this study, along with other studies conducted, shows that healthcare professionals lack knowledge and skills regarding disasters and do not feel prepared for them (Abdi et al., 2021; Labrague et al., 2018; Nofal et al., 2018; Salik et al., 2024; Salmani et al., 2019). In a study evaluating level of preparedness for disasters among nurses working in pediatric clinics, it was determined that 51.1% of nurses were moderately prepared for disasters (Gladston and Nayak, 2017). This study also shows that nurses were unable to coordinate disaster response for children and their families and manage crisis process due to their lack of preparedness for disasters. A study conducted after the earthquakes in Turkey indicated that nurses working in pediatric emergency departments struggled to perform triage due to their inadequate level of disaster preparedness (Topal et al., 2024). The American Academy of Paediatrics stated that healthcare providers’ being sufficiently prepared for disasters could reduce the risks to children and families (Altman et al., 2019). Therefore, it is important to support nurses with continuous and regular training programmes on management of children and families in disasters and to update their knowledge.
Literature review indicates increased disaster nursing education and training programs over past 20 years (Loke et al., 2021). In most countries, disaster nursing education is integrated into undergraduate programs, with various courses and certification programs offered to keep knowledge updated. Postgraduate education programs are also made available in this field and implemented as specialized nursing branches (Kalanlar and Kubilay, 2015; Yamamoto, 2013). The education curricula of these programs cover topics such as disaster preparedness, response, rescue, and risk reduction (Hamid et al., 2023). Education programs focusing on assessing children, approaching them, and child-centered disaster management seem inadequate (Goodhue et al., 2012). In addition, it is seen that there is an insufficient number of studies examining experiences of nurses regarding management of children in disasters. It is emphasized that children may have special needs during disasters compared to adults, so they should not be addressed same as adults (Koeffler et al., 2019). Integrating specialized disaster management education programs tailored to children into training of healthcare professionals can help mitigate negative effects of disasters on children (Disaster Preparedness Advisory Council, Committee on Pediatric Emergency Medicine, 2015; National Advisory Committee on Children and Disasters, 2015). It is necessary to develop educational content on initial assessment and triage of children in times of disaster, their comprehensive assessment according to age groups, identification of their basic needs, identification of at-risk groups of children, and management of missing and orphaned children. In addition, educational content should be developed on organization of pediatric services, emergency and intensive care, determination of medical treatment and care needs, and determination of nurses’ duties, authorities, and responsibilities (NAPNAP, 2011). These training materials are expected to be effective in reducing potential risks to children by increasing nurses’ knowledge, skills, and awareness regarding systematic management of children in disasters (Özarslan et al., 2026). Studies have shown that training programs organized for nurses are effective in preparing nurses psychologically for disasters (Lan et al., 2023; Yıldız and Yıldırım, 2022; Said and Chiang, 2020; Özarslan et al., 2026). It has also been emphasized that negative emotions such as anxiety, stress, and helplessness, which may arise due to lack of systematic management and organization during a disaster, can be reduced through training programs (Lan et al., 2023; Said and Chiang, 2020; Yıldız and Yıldırım, 2022).
Literature emphasizes need for hospitals to be prepared for disasters from a pediatric perspective (Koeffler et al., 2019; Altman et al., 2019; Loke et al., 2021). In this study, it was determined that nurses had difficulties in maintaining intervention and care of children due to inadequate equipment and personnel, inadequate organization and coordination. In addition, it was found that nurses were unable to keep adequate records of lost and homeless children while providing care during the earthquake, and that they experienced problems in creating safety and secure areas for children. Lack of preparedness of healthcare institutions for disasters and equipment shortages negatively impacts healthcare professionals’ ability to address challenges they face (Nakayama et al., 2019; Abdi et al., 2021; Doğan et al., 2024). In hurricane disaster in the United States, it was discovered that lack of preparedness for disasters and equipment shortages increased morbidity and mortality rates among disabled children (Dolan and Krug, 2006). It has been reported that severe damage to hospital and inoperability of most equipment during the Great Japan Earthquake caused nurses to experience conflicts and difficulties in care process (Nakayama et al., 2019). A study conducted with nurses following the earthquakes in Turkey showed that they experienced problems in continuing care and that care was disrupted due to insufficient number of health professionals capable of managing the disaster (Doğan et al., 2024). These results show that healthcare institutions need to make disaster plans taking into account necessary number of medicines, medical supplies, and healthcare professionals for every level of disaster in emergency situations.
Limitations of the study
Earthquakes affected 11 provinces located close to each other. This study included nurses who experienced the disaster and worked in Kahramanmaraş-Elbistan, one of the provinces most affected by the earthquake and the epicenter of the second earthquake. Conducting such studies in larger and more diverse sample populations is necessary to better emphasize importance of initiatives to be implemented for nurses working in disasters and to take necessary measures. Only nurses who had been working in pediatric clinics for at least 1 year were included in the study. During disasters, nurses’ workplaces may change, and they may be assigned to intervene with groups they are unfamiliar with. Therefore, it is important to plan studies on management of children in disasters for nurses working in pediatric clinics as well as those working in other clinics. Investigating experiences of nurses who have worked in different fields but have been assigned to care for children during disasters can serve as an important guide for possible measures to be taken. This study reports on difficulties and emotional problems experienced by pediatric nurses in managing children during acute phase of a disaster. It is important and necessary to determine the factors that affect professional skills of nurses in the long term.
Implications for practice
The findings of this research show that nurses working to manage children in disasters may encounter emotional and managerial problems, and that problem-solving process may be negatively affected by equipment shortages and unfavorable conditions. Difficulties encountered in managing children with increased protection, care, and treatment needs during disasters may contribute to development of physical and psychosocial health problems in children. At the same time, unmet protection and care needs may increase risk of neglect and abuse. Therefore, it is important and necessary to assess ability of nurses, who are an important professional group involved in disasters, to manage children during disasters in order to plan appropriate intervention efforts. Most research reports show that training programs organized for disaster management and repeated at regular intervals have a significant positive effect on nurses and other health professionals. Tailoring these trainings to management of children and developing training content can raise awareness among health professionals on many issues, such as comprehensive assessment of children in disasters, management and protection of missing children. Additionally, identifying potential risks related to management of children in disasters, enhancing knowledge and skills, and developing problem-solving strategies can help determine measures that can be taken.
This research, and many others, have proven that nurses can also experience psychological problems during disasters. Experiencing a disaster, the loss of loved ones, and continuing to work actively in the field can reduce nurses’ psychological resilience. Therefore, periodic assessments of the psychological and mental health of nurses exposed to disasters and appropriate supportive approaches are important and necessary. In this sense, psychosocial support centers can be established, and platforms can be created where they can share their feelings and experiences. At the same time, increasing the level of psychological preparedness for disasters before they occur will be an important supportive approach. The experiences of pediatric nurses in providing care for children necessitate that pediatric nurses also have a good level of psychological preparedness in order to manage children and families in disasters. Initiatives aimed at increasing nurses’ preparedness for disasters can be integrated into disaster education programs and disseminated.
Conclusion
This study found that nurses experienced emotions of fear, anxiety, and helplessness while caring for children affected by the earthquake. High number of injured and dead children, lack of equipment and personnel, and lack of knowledge and skills in disaster management were found to increase intensity of negative emotions and complicate disaster management. To increase nurses’ preparedness levels in managing children during disasters, it is necessary to establish regular and continuous education programs to raise awareness, develop knowledge and skills, and ensure psychological preparedness. This preparation process can support systematic disaster management by enabling nurses to experience negative emotions with less intensity during disasters and develop their ability to cope with stress and problems.
Footnotes
Acknowledgment
The authors sincerely thank the pediatric nurses working in the earthquake area.
Ethical considerations
Ethical approval was obtained from the Inonu University Health Sciences Non-Interventional Clinical Research Ethics Committee with the number 2023/4515. The purpose and content of the study were explained to the nurses who agreed to participate. The participants were informed that the data obtained from the voice recordings would be used for scientific purposes and that their personal information would be kept confidential. Verbal and written consent was then obtained from the participants. The study was conducted following the principles of the Declaration of Helsinki.
Author’s contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Research data is used solely for this research report and can be shared upon request.
Data collection
Researcher S. O. conducted the interviews. This researcher both experienced the earthquake and worked as a pediatric nurse during the earthquake.