
Abstract
Emotional eating is associated with negative outcomes in children, including elevated weight status and disordered eating. The current study assessed the preliminary psychometric properties of a 10-item parent-report version of the Emotional Eating Scale Adapted for Children (EES-C) Short-Form. Participants were 324 mothers of children ages 5–12 years. The parent-report version of the EES-C Short-Form and the Child Feeding Questionnaire were administered to mothers in the United States online. Cronbach’s alpha for the parent-report version of the EES-C-Short-Form was in the excellent range (α = .94). Mothers reported significantly higher levels of emotional eating in overweight/obese children than healthy weight children eating (effect size = 0.45, p < .001). Maternal reports of their child’s emotional eating on the EES-C-Short-Form were associated with maternal concern about their child’s weight (r = .285; 95% confidence interval = .18–.39), restricted eating (r = .238; 95% confidence interval = .13–.35), and monitoring of their child’s food intake (r = .136; 95% confidence interval = .02–.25) on the Child Feeding Questionnaire, supporting convergent validity. A unidimensional model produced a good fit (χ 2 (35) = 70.31, p = 0.00, CFI = .999, SRMR = .036). Taken as a whole, this study provides preliminary support for the reliability and validity of the parent version of the EES-C Short-Form.
Introduction
Emotional eating occurs when an individual eats in response to experiencing negative emotions (Geliebter and Aversa, 2003; Faith et al., 1997). In children in the United States, prevalence rates of emotional eating are as high as 20.4% (Nguyen-Rodriguez et al., 2009). These rates generally increase during adolescence nationally and internationally (Jääskeläinen et al., 2014; Nguyen-Rodriguez et al., 2009). Emotional eating has been linked to disordered eating behaviors and elevated weight status for children and adolescents (Banna et al., 2018; Jalo et al., 2019; Stice et al., 2002b; Stojek et al., 2017). There is some evidence that emotional eating is also correlated with higher rates of mental disorders among pre-adolescent girls (Munkholm et al., 2016). Taken as a whole, existing research underscores the importance of having psychometrically sound measures to evaluate emotional eating for children and adolescents.
The 25-item Emotional Eating Scale Adapted for Children (EES-C) was validated in 2007 for use with children and adolescents ages 8–17 years (Tanofsky-Kraff et al., 2007). This measure asks children and adolescents to self-report urges to eat in response to distinct emotions, like sadness, anger, or guilt. Limbers et al. (2020) validated a 10-item EES-C Short-Form with children ages 12–17 years (Limbers, Larson, et al., 2020). In this original validation study and a subsequent study, the EES-C Short-Form demonstrated a high degree of overlapping variance with the original EES-C Total Score (rs ranged from. 71 to .96), good internal consistency reliability (Cronbach’s alphas ranged from .84 to .87), and convergent and discriminant validity (r = −0.255 between EES-C Short-Form and a subjective measure of loss of control eating; r = 0.086 between EES-C Short-Form and the Gratitude Questionnaire) (Limbers, Greenwood, et al., 2020b; Limbers, Larson, et al., 2020).
Despite the EES-C Short-Form evidencing sound measurement properties (Limbers, Greenwood, et al., 2020b; Limbers, Larson, et al., 2020), to date there has been limited research investigating psychometric properties of a parent-report measure of the EES-C Short-Form. There is one other parent measure of child emotional eating that has undergone very limited validation work—the Emotional Eating Subscale of the Dutch Eating Behavior Questionnaire - Parent Version (Braet and Van Strien, 1997). There is a need for a psychometrically sound measure to evaluate emotional eating from parental perspectives of younger children (Braet et al., 2007) given research that indicates children younger than 12 years may be less capable of self-reporting on abstract concepts like emotions (Achenbach and Edelbrock, 1983; Edelbrock et al., 1985). Consistent with this research, psychometric properties of self-reported emotional eating measures generally are poorer for younger children (Farrow et al., 2015; Forrester-Knauss et al., 2012; Hirsch et al., 2014; Houldcroft et al., 2014; Ledoux et al., 2011; Steff et al., 2019; Van Strien and Oosterveld, 2008), highlighting the need for validated parent report measures of emotional eating for this population.
An absence of psychometrically sound parent report measures of emotional eating is also problematic because emotional eating behaviors often begin at a young age (Farrow et al., 2015). A reliable and valid parent-report measure of child emotional eating is necessary to identify younger children in need of early intervention who are at-risk for developing obesity or binge eating disorder or in instances in which older children and adolescents are not able to provide reliable and valid self-report of their emotional eating due to illness or disability (Frayn and Knäuper, 2018; Stice et al., 2002a).
Aim
The aim was to evaluate the psychometric properties of the parent-report version of the EES-C Short-Form in a sample of mothers from the United States.
Methods
Population
To meet inclusion criteria for the study, an individual had to be a woman 18 years or older with at least one child between the ages of 5 and 12 years who lived with them at least 50% of the time. Mothers who were not literate in English and were not from the United States were excluded from the study. Mothers who had multiple children in the 5- to 12-year-old age range were asked to report on their oldest child.
Measures
EES-C short-form
The EES-C Short-Form is a 10-item self-report measure that assesses the urge to cope with negative affect by eating in children and adolescents ages 8–19 years (Limbers, Greenwood, et al., 2020a; Limbers, Larson, et al., 2020). It has demonstrated strong psychometric properties (Limbers et al., 2020). The parent-report adaption of the EES-C Short-Form used in the present study included language modifications to make the items relevant to the respondent’s child. For example, “When I feel sad/disobedient/jealous/lonely/confused/nervous/angry/guilty/helpless/they’re not doing enough, I have a strong desire to eat” was modified to, “When your child feels sad/disobedient/jealous/lonely/confused/nervous/angry/guilty/helpless/they’re not doing enough, they have a strong desire to eat.” Mothers were asked to report on their child who is between the ages of 5 and 12 years, and the eldest child within that range should a mother have more than one child. Responses to the items were summed together to yield a total score, in which higher scores were indicative of a greater desire to eat in response to negative emotions.
Child Feeding Questionnaire
The Child Feeding Questionnaire (CFQ) was developed by Costanzo and Woody (Costanzo and Woody, 1985). The CFQ was intended to assess parental perceptions of childhood obesity and weight status, as well as child-feeding attitudes and practices (Birch et al., 2001). The version of the CFQ used in the present study contained 18 items and 4 dimensions related to child feeding and weight status: parental concerns about child’s weight (3 items), restriction (8 items), pressure to eat (4 items), and monitoring (3 items) (Anderson et al., 2005). Restriction, pressure to eat, and monitoring refer to parental control of their child’s feeding behaviors, whereas concerns about child’s weight status refer to parental concerns about child obesity. Birch et al. reported coefficient alphas of .75 (concern about child weight), .70 (pressure to eat), .73 (restriction), and .92 (monitoring) for the CFQ subscales (2001). Scores on each of these four dimensions were summated so that higher scores reflected more concerns about child’s weight, more restriction of intake, pressure to eat, and monitoring.
Demographics
A demographic questionnaire was administered to collect both mother and child characteristics. Participants answered questions regarding maternal age, race/ethnicity, height, weight, marital status, education level, occupational status, and household income. Child characteristics including age, gender, height, and weight were also assessed. Height and weight (kg/m2) were used to calculate maternal and child body mass index (BMI). Maternal BMI was computed following Centers for Disease Control and Prevention (CDC) classifications for those considered underweight (below 18.5), healthy weight (18.6 to 24.9), overweight (25.0 to 29.9), and obese (30.0 and above) (CDC, 2015). Child BMI percentiles were determined based on the CDC’s age and gender norms. These percentiles were used to classify children into healthy (BMI percentile 5 to 84.99), overweight (BMI percentile 85 to 94.99), and obese (BMI percentile 95 and greater) categories (CDC, 2015).
Procedures
Recruitment was performed through Prolific (a platform that connects researchers with human subjects and provides a small monetary compensation for human subjects completing online questionnaires), social media sites including Facebook and Reddit, and flyers posted at local coffeehouses and libraries located in Central Texas. Digital recruitment methods have demonstrated a greater reach at lower costs and are not considered significantly different than traditional paper and pencil methods (Weigold et al., 2013). An online consent form included a screener to identify eligible participants who fit the study’s criteria (i.e., consenting to participate in the following questionnaire assumes that you are a mother of a child ages 5 to 12 years who lives with you at least 50% of the time), after which potential participants were either exited from the survey or began a demographic questionnaire. Potential participants who wanted to continue with the study were asked to read the consent form and provide their consent to participate in the study by checking a box on the screen. Study questionnaires were then completed by participants online through Qualtrics. This study received approval from the Institutional Review Board at the authors’ institution (IRB Net ID 1729764-3).
Statistical analysis
All statistical analyses were conducted using IBM Statistical Package for the Social Sciences, Version 26 and The R Foundation R Version 1.4.1106.
Internal consistency reliability
Reliability of the EES-C Parent-Report Short-Form was assessed with Cronbach’s alpha, following conventions recommended by Urbina (2014). Cronbach’s alpha coefficients were interpreted in the following manner: >0.9, excellent; >0.8, good; >0.7, acceptable; >0.6, questionable; >0.5, poor; <0.5, unacceptable (George and Mallery, 2019).
Construct validity
Construct validity was assessed by examining known groups, convergent, and structural validity. A known groups comparison was used to evaluate differences between healthy weight and overweight/obese children’s levels of emotional eating as rated by their mothers. This analysis was chosen considering previous research that indicates children are more likely to have overweight and obesity if they engage in emotional eating (Belcher et al., 2011; Rhee et al., 2015). Independent samples t-tests were used to investigate whether there was a statistically significant difference (p < 0.05) between healthy weight and overweight/obese children on the adapted EES-C. A Cohen’s d effect size was calculated in order to determine the magnitude of the difference between healthy weight and overweight/obese children. Effect sizes were calculated by taking the difference between the healthy weight sample mean and the overweight/obese sample mean, divided by the pooled standard deviation. Effect sizes for differences in means were classified as small (0.20), medium (0.50), and large (0.80) in magnitude (Cohen, 1988).
As an indicator of convergent validity, a correlation between the EES-C total score and a measure of a theoretically related construct was examined. Given that emotional eating and parental perceptions of child feeding behaviors and weight status are theoretically related constructs (Gouveia et al., 2019), it was predicted that the EES-C total score would be significantly correlated with the CFQ. p values less than 0.05 were considered statistically significant (Sakoda et al., 1954).
Considering an existing theoretical model of the factor structure of the EES-C Short Form, a confirmatory factor analysis (CFA) was conducted to examine structural validity of parent-report of the EES-C Short-Form. The CFA model was created based on the theoretical structure of the EES-C Short-Form, which was found to be unidimensional (Limbers, Larson, et al., 2020). To assess model fit, the Comparative Fit Index (CFI) and Standardized Root Mean Residual (SRMR) were estimated. Based on the recommendations of Hu and Bentler, a model with adequate fit should meet the requirements of a two-index strategy of CFI ≥.95 and SRMR ≤.09, which together tend to have lower error rates than examining stand-alone values (Hu and Bentler, 1999).
Results
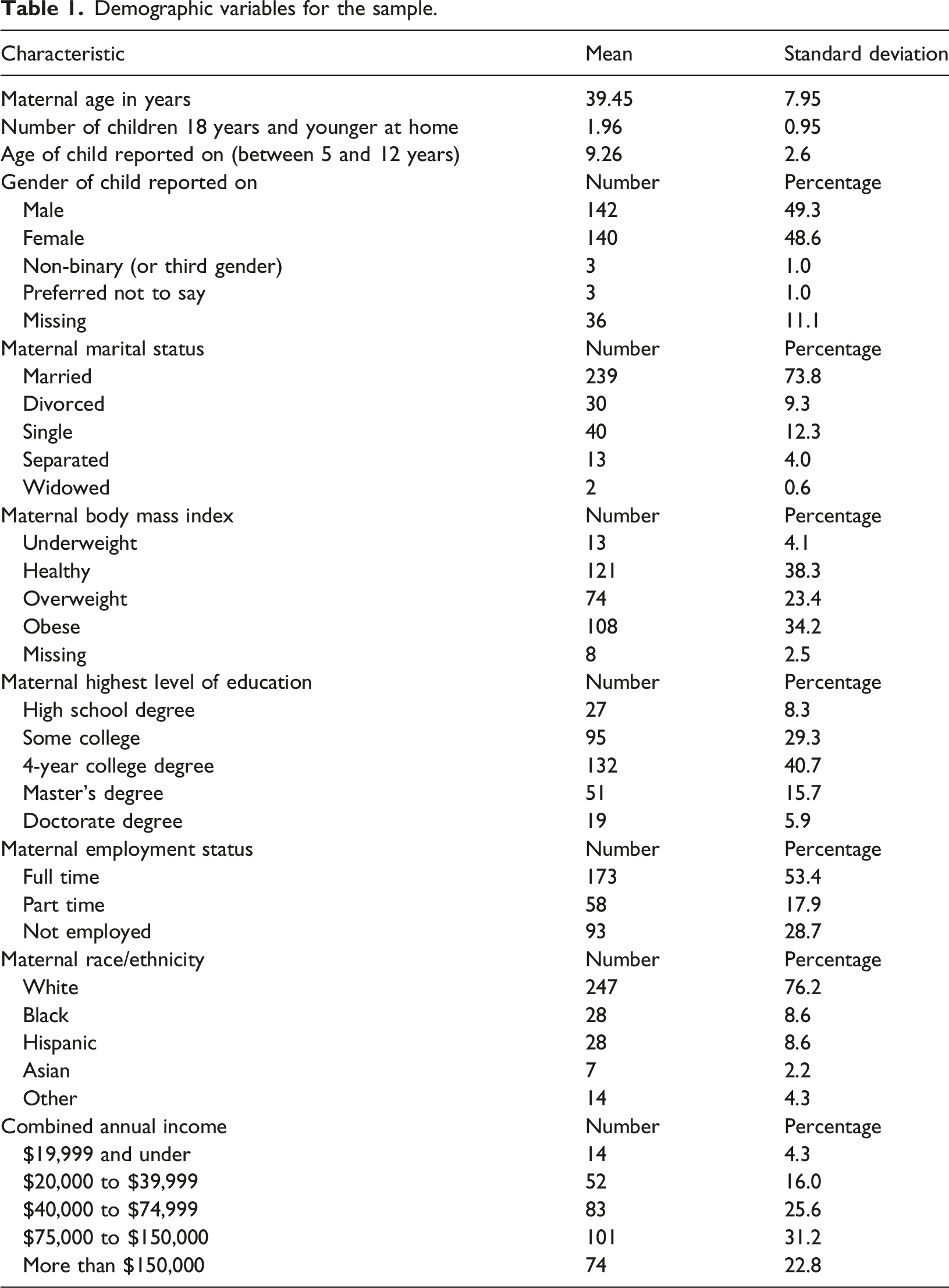
Participant characteristics
Demographic variables for the sample.
Internal consistency
Internal consistency of the EES-C Short-Form for the current study was in the excellent range (Cronbach’s alpha = .94). The CFQ also demonstrated good internal consistency reliability (concern about child’s weight α = .90, restriction α = .84, pressure to Eat α = .72, and monitoring α = .89).
Known groups analysis
Skewness and Kurtosis of the EES-C Short-Form Total Score were .67 and .15, respectively, which support a normal distribution. There was a significant difference between the mothers’ rating of their healthy weight children’s level of emotional eating versus mothers’ ratings of their overweight/obese children’s level of emotional eating (d = 0.45, t (205) = −3.16, p < .001) with mothers of overweight/obese children reporting more emotional eating (mean = 19.41, standard deviation = 6.78) than mothers of healthy weight children (mean = 16.28, standard deviation = 6.98). The effect size was 0.45, which is approaching the medium effect size range.
Convergent validity
Correlations between the parent version of the Emotional Eating Scale for Children and Child Feeding Questionnaire.
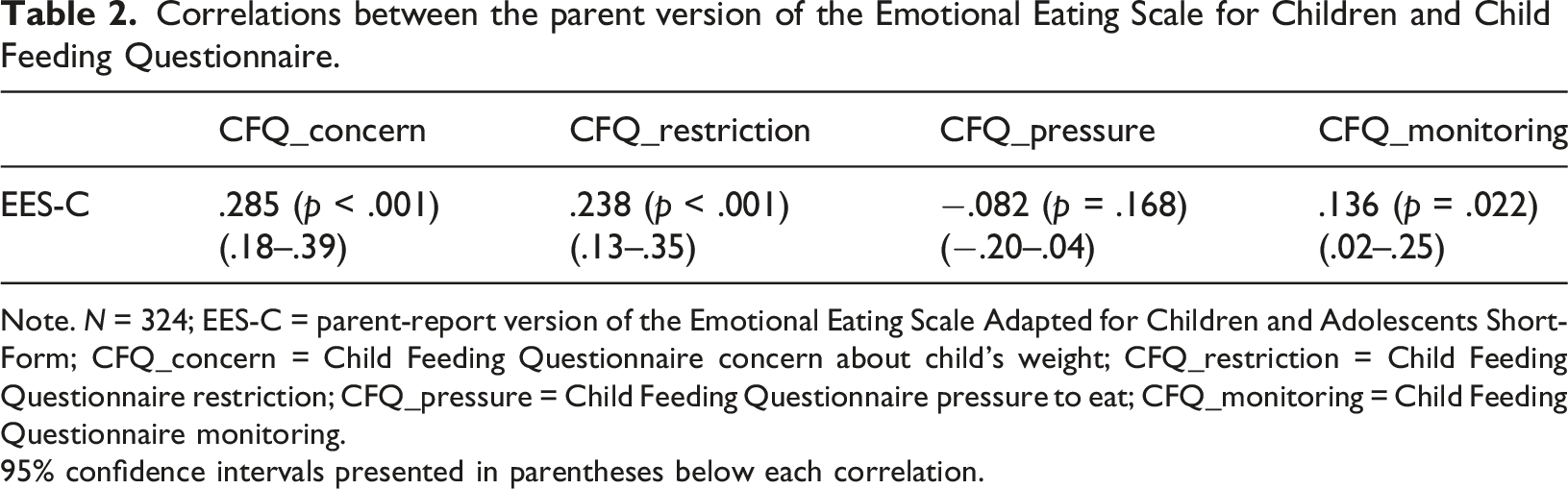
Note. N = 324; EES-C = parent-report version of the Emotional Eating Scale Adapted for Children and Adolescents Short-Form; CFQ_concern = Child Feeding Questionnaire concern about child’s weight; CFQ_restriction = Child Feeding Questionnaire restriction; CFQ_pressure = Child Feeding Questionnaire pressure to eat; CFQ_monitoring = Child Feeding Questionnaire monitoring.
95% confidence intervals presented in parentheses below each correlation.
Structural validity
A confirmatory factor analysis revealed that a unidimensional model met criteria for a good fit, χ 2 (35) = 70.31, p = 0.00, CFI = .999, SRMR = .036, and all of the items had good standardized factor loadings, ranging from .732 to .902. Supplemental Table 1 presents the standardized factor loadings. The chi-square statistic was significant for the unidimensional model; however, it is common for the chi-square statistic to be significant when utilizing large samples (Byrne, 2013; Kenny and McCoach, 2003).
Discussion
The current study examined psychometric properties of a parent-report version of the EES-C Short-Form. In this sample of mothers of children ages 5–12 years recruited online, we found preliminary support for the reliability and validity of the parent version of the EES-C Short-Form. Excellent internal consistency reliability was demonstrated, well exceeding the standard recommendation for making group comparisons. A unidimensional model demonstrated good fit, which is consistent with the theoretical model previously identified for the EES-C Short-Form self-report version and suggests preliminary support for the structural validity of the parent-report version (Limbers, Greenwood, et al., 2020a). The parent version of the EES-C Short-Form was associated with three dimensions of maternal perceptions of child feeding practices and weight status (concerns about child’s weight, restriction, and monitoring), suggesting favorable convergent validity. A known groups analysis indicated that mothers reported significantly higher emotional eating in overweight/obese children than healthy weight children, further supporting construct validity. Taken as a whole, these findings initially support the parent version of the EES-C Short-Form as a psychometrically acceptable measure to assess parental perceptions of their children’s emotional eating. The present findings are largely in line with a recent study published on the measurement properties of the parent version of the EES-C Short-Form (Summers and Limbers, 2024). While the study by Summers and Limbers (2024) had some methodological differences from the current study, including in-person data collection and the inclusion of both mothers and fathers, the two studies in combination provide growing support for the parent version of the EES-C Short-Form as a psychometrically sound tool to evaluate parental perceptions of child emotional eating.
While the Emotional Eating Subscale of the Dutch Eating Behavior Questionnaire - Parent Version can be used with parents of children as young as 7 years old (Braet and Van Strien, 1997), psychometric properties of this measure have not been extensively evaluated. There is some evidence in a validation study among pre-adolescent Italian youth that the Emotional Eating Subscale of the Dutch Eating Behavior Questionnaire - Parent Version does not differentiate between normal weight, overweight, and obese preadolescents (Caccialanza et al., 2004). This finding contrasts from the current findings in which the parent version of the EES-C Short-Form differentiated between overweight/obese children and healthy weight children. Another limitation of the Dutch Eating Behavior Questionnaire - Parent Version is that it does not specifically assess a child’s emotional eating in response to a range of different emotions (Braet and Van Strien, 1997). These factors should be taken into consideration when researchers and clinicians are selecting a parent measure of child emotional eating.
Study limitations
There were a number of limitations to the present study. Construct validity and internal consistency reliability were the only psychometric properties evaluated. Future studies should examine test-retest reliability, discriminant validity, and incremental convergent validity of the measure. Additionally, the current study utilized a predominantly white and highly educated online sample of mothers. Given evidence that emotional eating may be impacted by acculturative stress and other relevant multicultural considerations (Simmons and Limbers, 2019), future validation work of the measure is recommended in diverse samples, including mothers and fathers from a range of educational and socioeconomic status backgrounds. We excluded underweight children from the known groups analysis given the limited research on emotional eating in this population. Given that the Emotional Eating Subscale of the Dutch Eating Behavior Questionnaire - Parent Version is not in the public domain and the limited funding available for the current study, we were not able to use the Emotional Eating Subscale of the Dutch Eating Behavior Questionnaire - Parent Version for validation purposes in the present study. Finally, the current study only assessed parental perceptions of their child’s emotional eating; future studies should evaluate both parent and child perceptions of the child’s emotional eating behaviors and assess parent-child agreement across the measure forms. These limitations notwithstanding, the present study was one of the first evaluations of the psychometric properties of the parent version of the EES-C Short-Form. It also contributes to growing literature on parents and child emotional eating (Ekim and Ferda Ocakci, 2021).
Implications for practice
The psychometric properties of the parent version of the EES-C Short-Form reported in the current study have implications for clinical practice. Specifically, the findings provide preliminary evidence for the utilization of the parent version of the EES-C Short-Form for screening children between the ages of 5 and 12 years for emotional eating in settings where there is limited time and availability of resources. While further validation work of the measure is needed, these preliminary findings indicate that in situations in which child self-reported emotional eating is not possible (i.e., child is too young or is not able to provide self-report due to illness or disability), the parent version of the EES-C Short-Form may provide a reliable and valid alternative for evaluating child emotional eating. These findings highlight that prior to adolescence, differences in child emotional eating can be observed by parents across children of different weight categories and underscore the importance of early intervention as targeting child emotional eating at a young age has the potential to positively influence child weight status.
Conclusion
This study examined psychometric properties of a parent-report version of the EES-C Short-Form. In a sample of mothers of American children ages 5–12 years, we found preliminary support for the reliability and validity of the parent version of the EES-C Short-Form, including internal consistency reliability, convergent validity, and construct validity.
Supplemental material
Supplemental material - Validation of a parent-report version of the Emotional Eating Scale Adapted for Children and Adolescents Short-Form in American mothers
Supplemental material for Validation of a parent-report version of the Emotional Eating Scale Adapted for Children and Adolescents Short-Form in American mothers by Emma Summers and Christine A. Limbers in Journal of Child Health Care
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding to carry out this research was received from the Department of Psychology and Neuroscience at Baylor University.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.