
Abstract
Health Play Specialists (HPSs) play an important role in supporting children and young people’s emotional wellbeing in healthcare, yet their contribution remains poorly understood and is inconsistently recognised within paediatric multidisciplinary teams (MDTs). This study examined how HPSs and MDT members understand a HPS’s role and work. An online qualitative survey, distributed via professional networks and social media across the UK, was completed by 101 professionals (56 HPSs and 45 MDT members). Data were analysed using inductive qualitative content analysis. Participants shared recognition of the HPS’s impact, particularly through play, emotional support, and distraction but differed in their appreciation of the role’s scope and complexity. Four key themes were identified: role understanding, impacts, enabling factors and barriers to the HPS role. Participants identified a need for greater MDT integration and standardised education on the HPS’s role across health professional training. Whilst the findings demonstrate an understanding of a HPS’s role and work, there is a need for increased recognition of wider aspects of their role beyond play and distraction to procedural preparation, therapeutic and normalising play, post-procedural support, advocating for children and families, and delivering education to other members of the MDT.
Introduction
All healthcare professionals are encouraged to consider a playful approach to their work with children (Walker, 2006; National Institute of Care Excellence (NICE), 2021). However, it is a key responsibility of Health Play Specialists (HPSs) to deliver play as an organised service within the National Health Service (NHS) in the United Kingdom (UK) (Walker, 2006).
Health Play Specialists (HPSs) are qualified, registered healthcare professionals, occupying a unique role within multidisciplinary teams (MDTs) (NHS England, 2025). HPSs are trained to recognise and respond to children’s play needs in healthcare settings and to safeguard their emotional, psychological, social and physical wellbeing (Children’s Foundation, 2025). Using play as a therapeutic tool, HPSs help children understand illness and treatment, and work with other healthcare professionals to prepare children and support them during procedures (NHS Health Careers, 2025). After more than 60 years of developments in this role, work and training, HPSs have become recognised as important members of paediatric multidisciplinary teams (MDT) in national guidance (Department of Health, 2003; National Institute for Health and Care Excellence, 2021; NHS England, 2025; RCPCH, 2018; Royal College of Anaesthetists, 2023; Royal College of Nursing, 2022).
The Health Play Specialist role within UK NHS paediatric services has equivalent roles internationally with Certified Child Life Specialists (CCLSs) being the most widespread in the US and Canada (Pillai, 2020). Similar roles, such as Child Life Therapists, can also be found in healthcare settings in Australia and New Zealand. Emerging equivalent roles exist also in parts of Europe, South America and Japan (Committee on Hospital Care and Child Life Council et al., 2014). Whilst all these roles share similarities, there is wide variation across settings in terms of training and professional registration (Perasso et al., 2021). Uncertainty regarding training, qualifications, registration requirements, and job titles affects how the role and work of health play staff are perceived, understood and utilised to benefit children receiving healthcare across a variety of settings (Gjærde et al., 2021; Thestrup et al., 2024).
Work undertaken by HPSs has been shown to include roles such as distraction and diversionary play (Drayton et al., 2019; Lane, 2023; Ullán et al., 2014), preparation for procedures and hospitalisation (Grissom et al., 2015), procedural support (Burns-Nader et al., 2016; Diener et al., 2018), normalising play (Lerwick 2019), post-procedural play (Gordan and Paisley, 2018; Jun-Tai, 2008) and aspects of these various therapeutic play approaches, often delivered by HPSs, are commonly included within studies examining the impact of preparation and distraction within paediatric procedures (Brown et al., 2022; Burns-Nader et al., 2016; Zhao et al., 2022). However, literature specifically exploring and presenting evidence of HPS’s work in practice has been scarce, broadly consisting of anecdotal or descriptive narrative accounts, with limited empirical research studies (Graber et al., 2025; Tonkin, 2014; Tonkin et al., 2023).
Since the Coronavirus disease (COVID-19) pandemic, there has been an increase in research and attention given to play and its role in healthcare settings, but only a limited number of studies have involved HPSs who are trained explicitly in health play facilitation (Graber et al., 2025). Recent work has mainly focussed on the impact of play provision and interventions on children’s health, wellbeing and healthcare outcomes, rather than considering the role, work and approach of those trained and employed to oversee and deliver play as a distinct service within healthcare. Research continues to highlight misunderstandings about the role and work of HPS’s (Gjærde et al., 2021; Perasso et al., 2021) and there is a notable gap in research examining factors that can act as barriers or facilitators to HPS practice within children’s healthcare (Perez-Duarte Mendiola, 2021; Stenman et al., 2019).
This paper will report this study according to the Standards for Reporting Qualitative Research (SRQR) (O’Brien et al., 2014) (Supplementary file 1).
Aim
To explore the perceptions of a Health Play Specialist’s role within paediatric multidisciplinary teams and the factors influencing their practice with children and young people.
Method
An online qualitative survey was used to gather data from both HPSs and their MDT colleagues working within paediatric MDTs across the UK. This method was selected to gather detailed accounts directly from participants of their perceptions and experiences of HPSs working in MDTs. Online qualitative surveys are increasingly being recognised as a credible method to collect qualitative data, providing participants with opportunities to freely and anonymously share information about their experiences on their own terms (Braun and Clarke 2022).
A qualitative survey was designed specifically for this study, informed by a review of the literature and the research team’s experience. The survey was pre-tested with four HPSs and two MDT members to ensure clarity in the questions and response options and check accessibility of online features.
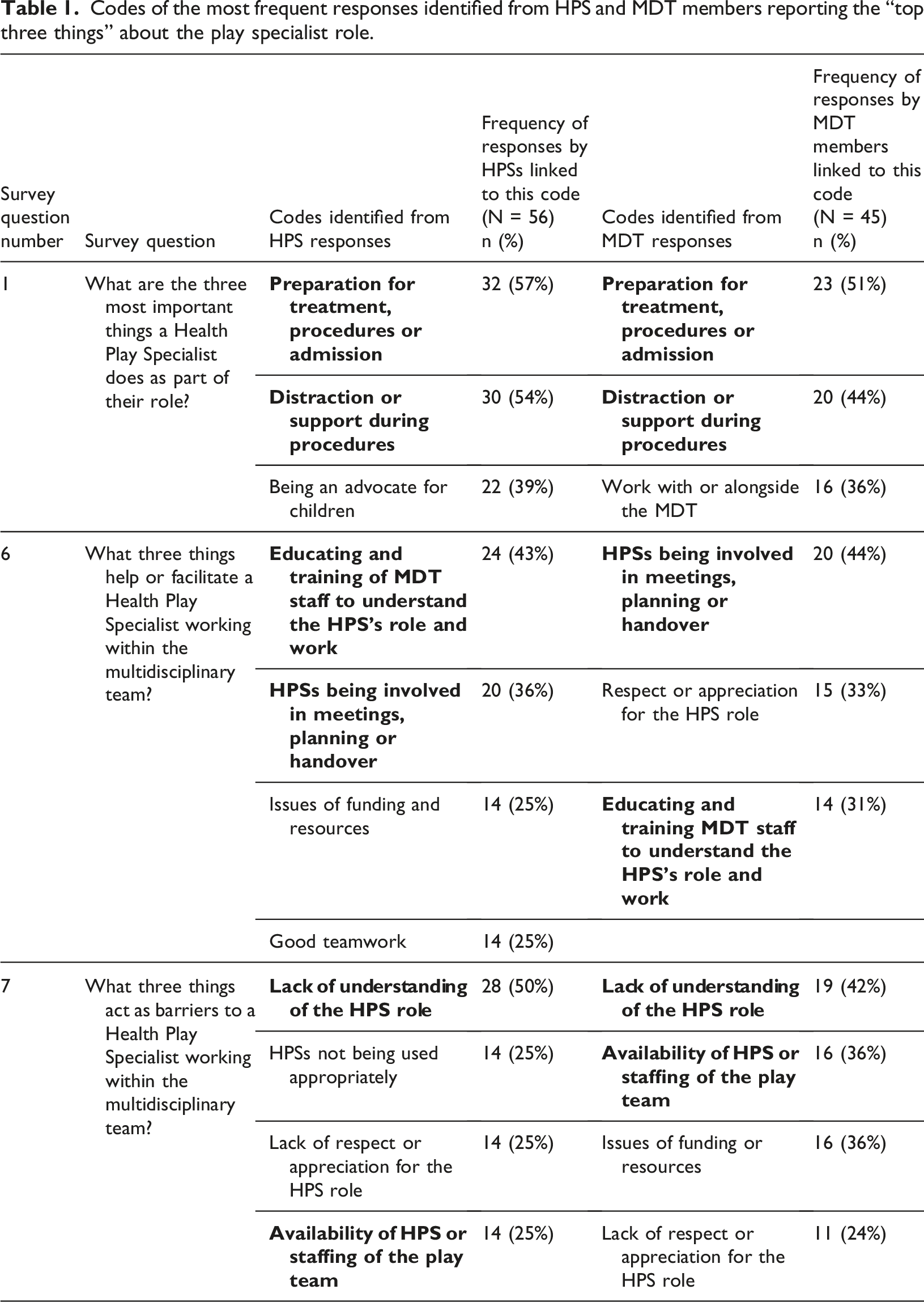
Codes of the most frequent responses identified from HPS and MDT members reporting the “top three things” about the play specialist role.
Codes of the most frequent responses identified from HPS and MDT members open text responses.
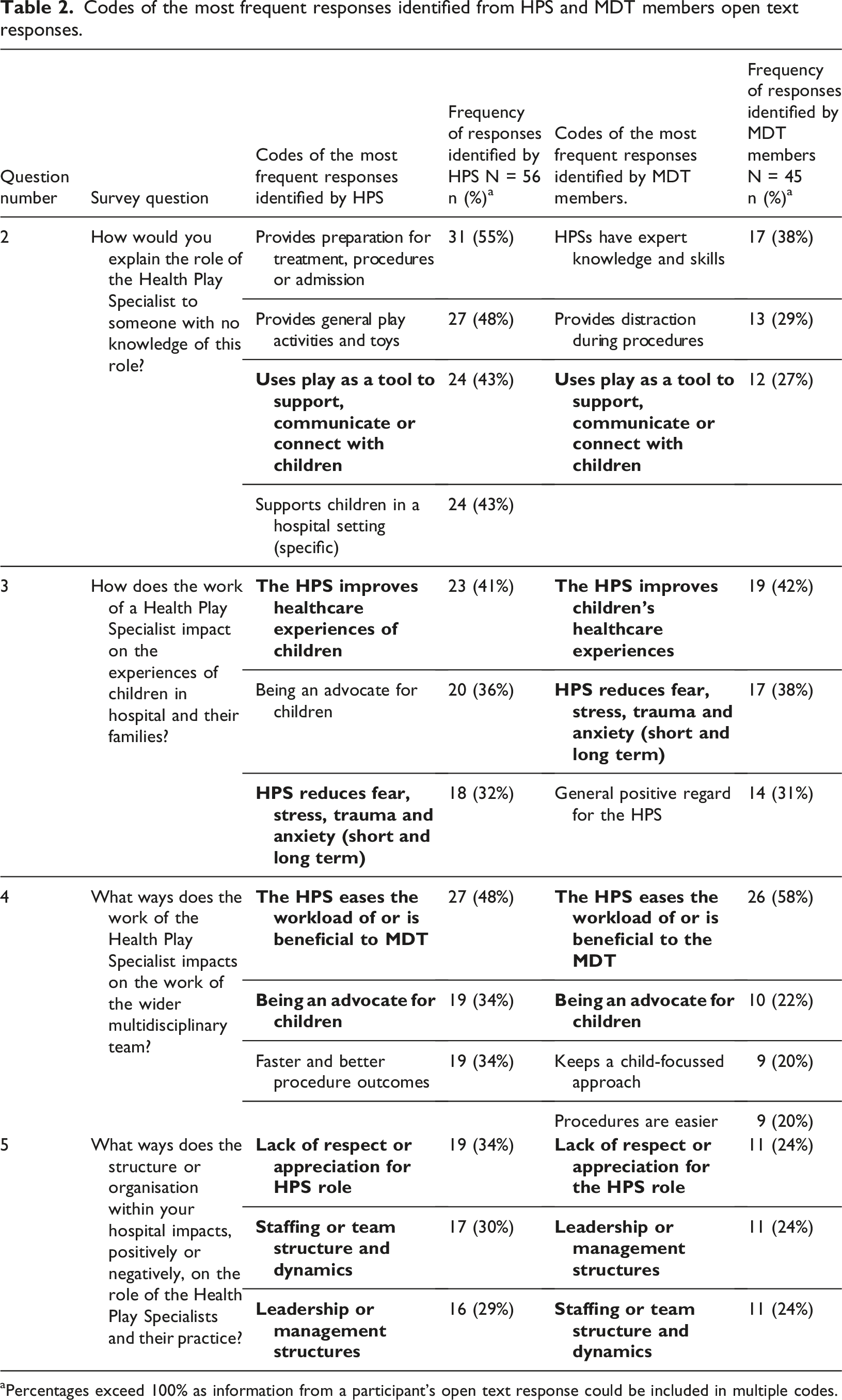
aPercentages exceed 100% as information from a participant’s open text response could be included in multiple codes.
Sample and recruitment
Survey distribution occurred through key professional networks established on various social media platforms, including X (formally Twitter) and Facebook and therefore used a convenience sampling strategy where participants self-selected if they wished to participate (Stratton, 2021). Participants eligible for inclusion in this study were employed as HPSs within MDTs and healthcare settings in the UK and individuals who were part of UK paediatric MDTs and who worked regularly with HPSs in clinical, patient-facing roles were also eligible. These included professionals such as nurses, paediatricians, psychologists and Allied Health Professionals (AHPs).
Analysis
Data were analysed using inductive qualitative content analysis (Elo and Kyngäs, 2008), carried out across three stages. Firstly, the text was read and re-read to gain an overall sense of the content, or “to obtain a sense of the whole” (Vaismoradi et al., 2013: p401). Second, data were open coded per question by highlighting commonly used words, phrases or statements. Finally, codes were grouped and organised into key categories. Frequencies were used to describe the brief open text responses in line with the qualitative content analysis approach and served a descriptive rather than an analytic purpose. The initial coding was conducted by [insert initials after review] and the identification and organisation of codes were then independently checked by other team members [insert initials after review], refined and then redefined through ongoing discussions. A rigorous and reflexive approach was adopted throughout analysis, team members from mixed disciplinary backgrounds, including one registered HPS, a children’s nurse and a human geographer reflected on their professional and personal assumptions that may have influenced the interpretation of data.
Participants provided consent by ticking a box within the online survey confirming they had read the full study information sheet and understood that submitting responses indicated agreement for their data to be used for study purposes. The information sheet outlined study aims, what participation involved, voluntary nature of participation, confidentiality and data handling procedures, potential risks and benefits of taking part and provided information on where further details could be obtained after participation if needed. As responses were anonymous, participants were informed that they would be unable to withdraw their data once it had been submitted.
Findings
Characteristics of participants
A total of 101 professionals participated in the study. Of these, 56 were HPSs working across a range of healthcare settings. 23 (41%) worked in a Specialist Children’s Hospital and 23 (41%) worked in a District General Hospital. 10 participants (18%) worked in “other” settings, including community and hospice settings or in academia.
45 participants were MDT members representing a variety of health professions, including doctors/paediatricians (n = 10, 22%), nurses (n = 19, 42%), and Allied Healthcare Professionals such as physiotherapists (n = 3, 7%), occupational therapists (n = 3, 7%) and psychologists (n = 3, 7%). Less frequent roles included one chaplain, four play workers, one pharmacist and one speech and language therapist.
Key findings
Findings highlight a HPS’s role to be complex, varied and multi-layered in nature. Areas of consensus between HPS and MDT members were highlighted, as well as some divergence in understandings of the role (Table 1 and Table 2). Where survey questions sought a specific number of answers to be given (e.g. “name three things”) (Table 1), data are presented as a proportion and percentage of the total number of participants. Where less structured open text responses were provided, data are presented to show the number (frequency) and percentage of participants who mentioned a particular code (Table 2). These figures are provided for descriptive purposes only. Where consensus between participant groups was identified amongst key codes, this is shown in tables (1 and 2) in bold type.
Study findings are presented under four key categories identified through analysis: understanding of the role of the HPS working within paediatric MDTs; Descriptions of the impact of the HPS’s work; factors that support or facilitate HPS’s work; and issues that disrupt or act as barriers to the fulfilment of the HPS’s work (as seen in Figure 1). Quotations are identified by participant number and job role. Visual representation of the research findings.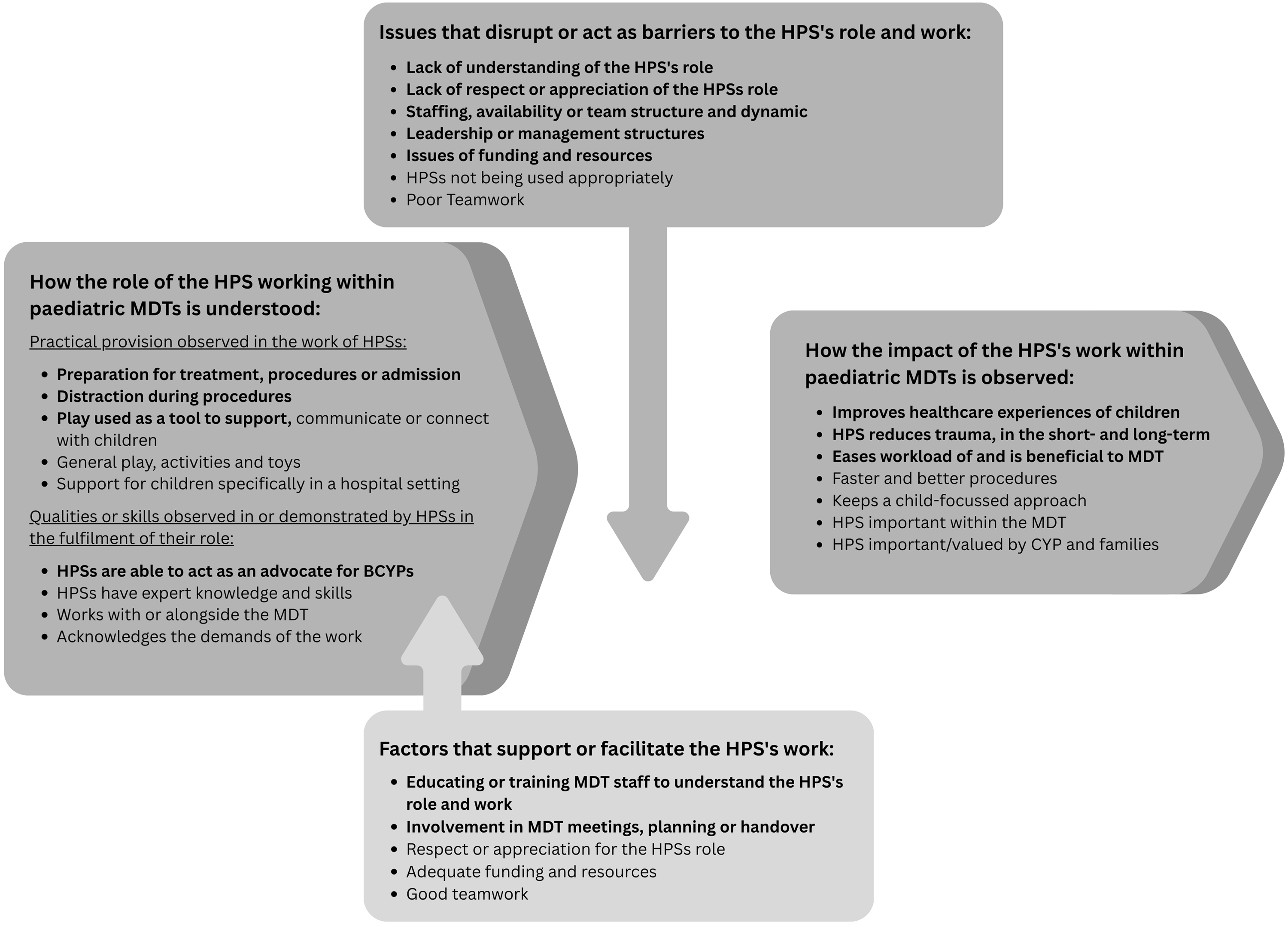
Understanding of the role of the HPS working within paediatric MDTs
When participants were asked to describe the “three most important things that HPSs do” as part of their role, HPSs presented 35 distinct examples, and MDT members gave 30. Responses revealed a wide and varied understanding and observations of what HPS’s do, and their role within teams. This indicated an acknowledgement within MDTs that a HPS’s role is complex and that its demands extend far beyond “just” playing. As one HPS explained: “The role of the HPS is beyond any job description – there are many elements to the role and no one day in the role is ever the same’ (P28–HPS).
Within this category, participants identified practical aspects of the work undertaken by HPSs. While there was agreement on the three most important things a HPS does as part of their role across both participant groups, preparation activities for children for treatment, procedures and admission to hospital were discussed slightly more frequently by HPSs (n = 32, 57%) than MDT (n = 23, 51%) and mentioned more by HPSs in response to open text questions (Table 2), with one HPS sharing that HPSs “prepare children for procedures using an array of tools and techniques suitable for their level of understanding” (P24–HPS). Distraction during procedures, while identified by both groups as an important thing a HPS does (HPS n = 30, 54%; MDT n = 20, 44% (question 1) was discussed more frequently by MDT members than by HPSs across the open text responses (Table 2). One nurse participating in the study noted that; HPSs can commit more time before, during and after an intervention to ensure they know the patient and what distraction would work well for them (P7-nurse).
Study findings indicate a shared understanding between both groups that HPSs use play as a key tool in supporting children within healthcare settings (HPS n = 24 (43%), MDT n = 12 (27%), question 2, table 2). However, while the provision of general or “normalising” play, including the creation and maintenance of play spaces and helping children to access play activities was discussed frequently in open text responses by HPSs (n = 27, 48%), there was a lack recognition of this in responses by MDT members, despite this being a fundamental part of the HPS’s role. In emphasising this work as being central to their role, some HPS participants linked it to children’s fulfilment of their right to play. One HPS explained, it is important in order “to meet article 31 of the United Nations Convention on the Rights of the Child (UNCRC)” (P5–HPS) while others included provision of normalising play as a distinct aspect of a HPS’s role with an equal weighting to more specialised and purposefully therapeutic play delivered within their work. This provision was described as a varied spectrum of different techniques and activities by one participating HPS: From the basic of keeping [children] busy with activities and toys to alleviate boredom to the complicated, empowering them through procedures and treatment (P24–HPS).
Participants also identified qualities acknowledged to be central to a HPS’s approach and work. There was recognition in open text responses from MDT participants (n = 17, 38%) (Table 2) that HPSs have expert knowledge and skills that are observable through their practice. These observations considered HPS’s “specialist and unique knowledge of child development and psychology” acquired by their training that “improves the experience of healthcare and hospital for children” (P33–nurse) and the significance on teams of having: Hospital professionals with skills to care for the non-medical…needs of children and young people while they are required to have medical treatment (P68-nurse).
An advocacy role of HPSs on behalf of babies, children, young people, and their families was recognised by both participant groups. However, MDT members mentioned it only in response to a question exploring HPSs’ impact on the wider work of MDTs. In contrast, HPSs referred to advocacy in response to three separate questions, describing it in a variety of ways including “giving children choice and a voice” (P54–HPS) and “advocating children and families’ needs and rights to the multidisciplinary team” (P29–HPS), and supporting them consistently “throughout their hospital journey, both at diagnosis and [during] treatment” (P56–HPS). These responses suggest that HPSs view advocacy as a central and ongoing aspect of their role.
The reported impact of the HPS’s work in paediatric teams
Both groups of participants reported in open text responses that HPSs positively improved children’s healthcare experiences through their work (HPS n = 23, 41%; MDT n = 19, 42%) (question 3 Table 2) and that involving HPSs in their healthcare experiences, contributed to reducing children’s trauma, both short and long term (HPS n = 18, 32%; MDT n = 17, 38% (question 3, Table 2). These observations reflected both an immediate view of children’s experiences where HPSs “makes a big difference in how the visit or procedure goes and how [they] view the hospital environment” (P28–HPS) and a longer-term perspective whereby having HPSs working in teams was understood to be “a long-term investment in a child’s interactions with health services” (P52–Paediatrician).
HPSs (n = 19, 34%) (Table 2, question 4) perceived that their work contributed to “faster procedures” (P9–HPS) or better outcomes with “reduced clinical risks” (P86–HPS) for children. Some HPSs shared their observations that the presence of a HPS could “cut down the need for more invasive procedures such as general anaesthetic (GA) or sedation” (P21–HPS) for some procedures including MRI scans. MDT members shared some similar examples, but these observations split across two distinct codes. MDT participants (n = 9, 20%) (Table 2, question 4) discussed their perception that procedures are easier with the HPS’s involvement, and that “the success of certain treatments/procedures can depend on the input of play specialists” (P72–Nurse). These participants (n = 9, 20%) (Table 2, question 4) equally highlighted that having HPSs present contributed to and encouraged a child-focussed approach within teams, due to a HPS being a practitioner who “connects the team to the essence and functioning of the child” (P84–Paediatrician).
Across both participant groups (HPS n = 27, 48%; MDT n = 26, 58% (Table 2, question 4) there was a shared view that HPSs ease the workload of, and are beneficial to, the wider MDT. Participants expressed considerable positive regard for HPSs and their role within paediatric MDTs, with one noting that having a HPS present could “make or break a stay in hospital” (P58–HPS) or invasive procedure.
The factors reported as supporting or facilitating the HPS’s role and work
Key factors strongly identified by both participant groups as supporting or facilitating a HPS’s role and work within MDTs were the education or training of MDT staff to understand the HPS’s role and approach (HPS n = 24, 43%; MDT n = 14, 31% (question 6) and the inclusion of HPSs in MDT planning or handover meetings (HPS n = 20, 36%; MDT n = 20, 44% (question 6).
Education of healthcare staff was discussed many times by participants (HPS n = 24, 43%; MDT n = 14, 31% (question 6)) but was emphasised more by HPSs as a key facilitator to being able to carry out their work and this, in turn, was acknowledged ultimately to be beneficial to children receiving healthcare. One HPS expressed that “teaching…doctors…about our role helps raise our profile and helps more children” (P21–HPS). Another HPS shared that teaching focused on play benefits and the specific role of HPSs should be delivered to “all Trust staff, not just ward staff” (P24–HPS). MDT participants also emphasised a need for the role to be better understood widely throughout healthcare teams and that “education of the wider MDT as to the scientific basis for [having an] HPS in children’s services” (P75-Pharmacist) was key. Different suggestions were made by both HPS and MDT members about when and where this training could or should be delivered, including “being part of the induction for all new staff” (P38–HPS), something that should happen for nurses and doctors “at university level” (P16–HPS) and that a “bigger national voice” (P5–Nurse) is needed to educate others “as to the scientific basis for the HPS in children’s healthcare services” (P75–Pharmacist).
Ensuring that HPSs are involved in MDT planning was reported as being of benefit to all involved by both HPS and MDT participants. Attendance at meetings should be “consistent” (P49–Occupational Therapist) and a space for two-way sharing, for HPSs “to share their knowledge of a child or family” (P43–Psychologist) and because equally this may “help them plan [their work] better” (P35–Paediatrician). Ultimately, integration of HPSs into whole team planning was important since they “should be seen as part of the team just like any other specialist” (P52–Paediatrician). MDT members also expressed a view that HPSs should; [Have] a seat at the senior management table so that the voice of children and young people, which Health Play Specialists are uniquely placed to give, is heard consistently (P101–Chaplain).
HPSs also reported adequate funding or resources (n = 14, 25%) (question 6) and good teamwork (n = 14, 25% (question 6)) as additional positive factors influencing an ability to deliver their work effectively.
The issues reported as disrupting or acting as barriers to the fulfilment of HPS’s work
Across both participant groups, factors most frequently reported that were identified as disrupting or acting as a barrier to HPS practice were a lack of understanding around a HPS’s role (HPS n = 28, 50%; MDT n = 19, 42% (question 7)) and issues arising from HPS availability within healthcare settings, staffing or team structures (HPS n = 14, 25%; MDT n = 16, 36% (question 7)). Health play teams were reported to be “small teams spread too thinly” (P25–HPS) across clinical services with the hard reality of understaffing in health play provision being expressed by both HPSs and their MDT colleagues who stated that there are “too few of them” (31-paediatrician) and that “we miss them in the evening and at weekends” (P65–Nurse).
Both groups of participants also shared a point of view that the HPS’s role is not respected or appreciated within healthcare teams and settings (HPS n = 19, 34% (question 5), n = 14, 25% (question 7); MDT n = 11, 24% (question 5), n = 11, 25% (question 7)). This issue was commonly discussed in a question that asked specifically about how the structure of organisation with hospital settings impacts a HPS’s role and practice. Reasons for this difficulty were broadly attributed to hierarchical structures within the health service and HPSs not being perceived as skilled practitioners within a paediatric MDT;
People not understanding the value of play specialists and the depth of knowledge they have about each individual child they work with (P57–Paediatrician).
HPSs also reported that not being used appropriately acted as a barrier to practice (n = 14, 25%). Specific examples from practice were shared to illustrate this point with HPSs sharing that other MDT members “always leave calling us to the last minute or after they have distressed the child” (P24–HPS). Such frustration was expressed many times by HPS participants recounting “being called too late and [then] being expected to ‘wave a magic wand’ when it doesn’t work like that – preparation takes time” (P64–HPS).
Discussion
This study explored perceptions of the role of Health Play Specialists within paediatric multidisciplinary teams and factors influencing their practice with children and young people. This study represents the first qualitative exploration of these perspectives within UK paediatric MDTs. Findings demonstrate work undertaken by HPSs to be complex in nature and highlight both shared understandings and important differences between HPSs and their MDT colleagues.
Findings support existing research and evidence which highlights the important role HPSs have in providing play equipment and activities to entertain children, which improves wellbeing whilst they are receiving healthcare (Gulyurtlu et al., 2020) and in reducing the impact of medical and hospital associated trauma (Starlight Children’s Foundation, 2023). In this study, HPSs were described by both MDT participants and HPSs as “joy bringers” and “superheroes”. This aligns with dominant perceptions of their role within available literature as a nice job “which includes lots of laughter and silliness” (Lane, 2023) and where the complex, varied work of HPSs is rather diminished as “just what we do” (Elliot, 2023) or described, somewhat unhelpfully by both HPSs and their MDT colleagues, as “magic” (Hubbuck, 2023). However, participants in this study were keen to present a view of HPSs as being skilful contributors to children’s healthcare, of their work as being much more than “just” playing and of their role as being more complex than just being a nice, friendly member of a child’s healthcare team.
Findings from this study add to current understanding of HPSs (Thestrup et al., 2024; NHS England 2025; Starlight Children’s Foundation, 2023) by highlighting the multi-layered nature of their role. There was wide recognition and agreement across participant groups of a HPS’s role in providing distraction during procedures, and there is a growing body of evidence to support the important contribution HPSs make to distraction and support during a child’s procedural experience (Boles, 2018; Diener et al., 2018; Drayton et al., 2019). HPSs are also increasingly called upon to assess a child’s ability to undergo complex medical procedures without sedation or anaesthesia, and then to support them to do so (O’Donnell, 2023; Pillai, 2020).
The range and complexity of the HPS’s work has previously not been the focus of research but is beginning to be acknowledged more within UK literature (Gulyurtlu, 2025; Pérez-Duarte Mendiola, 2021) and some international studies (Gjærde et al., 2021; Graber et al., 2025; Perasso et al., 2021). Breadth and depth within a HPS’s role has been discussed within the context of such categories as normalising play (Hubbuck, 2009, 2015), therapeutic play (Burns-Nader and Hernandez-Riaf, 2016; Luongo and Vilas, 2018), and medical play, which is often used as a tool to prepare children for hospital admissions, surgical or medical procedures or longer-term treatment (Ortiz et al., 2019; O’Donnell, 2023). These focussed pieces of research highlight how play is used as an important way of reassuring, communicating with and therapeutically attending to children’s needs while they are receiving healthcare.
Study findings demonstrate that HPSs also have important roles in advocacy, preparation before and support during healthcare procedures, post-procedural play and contribution to planning for better patient outcomes. HPS participants highlighted the importance of their advocacy role in empowering children and connecting, communicating with children and young people and representing their voices, where needed, in often highly pressurised healthcare environments. It is of interest that some of these broader roles were acknowledged less by MDT members than by HPS themselves. This may be because work linked to these broader roles is often undertaken by HPSs on a one-to-one basis with children and may be less visible, and therefore less likely to be acknowledged, by their MDT colleagues (Weldon and Peck, 2025). An HPS’s role in advocating for children is less well recognised within current literature than the provision of play items and facilitation of play activities that is more often described (Gjærde et al., 2021; Graber et al., 2025).
Study findings revealed some noted paradoxes. Both MDT members and HPSs identified and described a lack of respect and appreciation for the HPS role, along with a need for greater understanding and education about it. Yet, at the same time, participants reported the significant impact HPSs have on patient experience and the high levels of expertise they bring to paediatric care. A lack of health professional education around the role and work of the HPS and play more generally has been previously noted (Lerwick, 2019) and findings from this study support that play and playful approaches should be incorporated into the professional training of all healthcare staff.
The study also demonstrated conditions which facilitate ways that HPSs work within paediatric MDTs, in a skilled way, with good outcomes for children, families and healthcare practitioners. Alongside respect and appreciation, adequate staffing and resources were considered as key facilitators for this work. HPSs being fully integrated within teams by being involved in planning meetings and patient handover was also reported as an important way to support HPSs in their work directly with children and families across diverse healthcare settings.
Findings from this study demonstrated a recognition of normalising play (Gjærde et al., 2021; Hubbuck, 2009; NHS England, 2025; Weldon and Peck, 2025) and the HPS’s role as being important for children amid the more extraordinary, often adverse aspects of being unwell and in hospital or accessing healthcare in other settings. There is a need for clearer national guidance about how HPSs and other health play staff are included within MDTs to ensure good, consistent staffing across diverse healthcare settings according to need. A recent NHS England publication, the “Play Well Toolkit”, produced in collaboration with Starlight Children’s Foundation, sets out standards for play services nationally in England and states that “health play services should be seen as integral to paediatric care, supporting children through their health journeys by normalising their experiences…and mitigating the risks of trauma” (NHS England, 2025).
Embedding education within formative training of healthcare professionals around the importance of play, playful approaches in children’s healthcare and ways to utilise HPSs as a clinical resource is needed to ensure a HPS’s work is facilitated well in practice (NHS England, 2025). Further research is also needed to evidence the nature and impact of the broader, sometimes invisible and unrecognised aspects of how HPSs work.
Limitations
Whilst this study contributes an important understanding of the role of HPS, the data are from a voluntary and self-selecting sample, and therefore, the responses may reflect perspectives of individuals with a particular interest in the topic and not represent the views of all health play specialists. The study focussed on the role of HPS in the UK, and whilst some findings may be transferable to other international settings the role and context is unique to the UK.
Implications for practice
Findings from this study highlight that better and clearer national guidance and an increase in funding that can be sustained is needed to support the inclusion of HPSs and other health play staff within MDTs. Dedicated education sessions developed with and, where possible, delivered by HPSs should be included within undergraduate health professional training programmes, clinical skills training and trust-wide hospital induction sessions. More HPS led research is needed to examine the unique role and approach of HPSs in paediatric MDTs as well as evaluate the observable outcomes from HPSs being integrated into the complex and clinical aspects of children’s healthcare.
Conclusion
This research study explored how HPSs and paediatric MDT members understand a HPS’s role and work within UK healthcare. There was agreement across groups on the benefits of key aspects of the HPS’s work such as distraction, emotional support, and improved patient experiences but there were differences in awareness around their broader responsibilities, including advocacy, procedural preparation, and post-procedural play. Key facilitators of this role were reported as education for MDT staff and HPSs being included in planning meetings, while barriers involved limited staffing, lack of respect, and late referrals for increased procedural support. Findings emphasise a need for clearer national standards, sustainable funding, and integration of play-focused education into professional training across paediatric healthcare MDTs.
Footnotes
Acknowledgements
Thank you to all the professionals for sharing their views and opinions.
Ethical considerations
The Edge Hill University Health-Related Ethics Committee approved our study and use of anonymous online surveys (approval: ETH2122-0251) on 9th September 2022.
Consent to participate
Respondents confirmed by checking a box on the online survey to confirm they had read the information and provided consent for taking part.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, [LB] upon reasonable request.