
Abstract
Internalized racism (IR) is a form of racism that leads people to internalize stereotypes about their racial/ethnic group (i.e., group-focused IR) and/or about themselves because of their racial/ethnic group membership (i.e., self-focused IR). However, although IR is associated with poor mental health, little is known about the underlying mechanisms of these associations. To address this limitation, this research investigates the core self-evaluation (CSE; a person’s fundamental evaluations about themselves, their own abilities, and their own control) mediated pathway as one potential pathway. CSE consists of four traits: self-esteem (SE), locus of control (LoC), emotional stability (ES), and generalized self-efficacy (GSE). With a sample of 780 Black/African American adults (Mage = 37.68 years, % Female = 57.6), this study investigated the independent direct and indirect effects of group- and self-focused IR on depression and anxiety symptoms via CSE using structural equation modeling. Confirming predictions, self- and group-focused IR predicted greater anxiety and depression symptoms and lower SE and ES. However, against predictions, both forms of IR were associated with increased internal LoC and were not associated with GSE. Last, results show partial support for the CSE mediated pathway, such that SE and ES (but not LoC or GSE) mediated the relationship between both self- and group-focused IR and anxiety and depression symptoms. Results suggest that IR is indirectly related to mental health via the more affective (SE, ES) relative to motivational (LoC, GSE) components of CSE, which has implications for understanding underlying mechanisms associating IR with poor mental health among racial/ethnic minorities.
Keywords
Internalized racism (IR) is a form of racism that leads people to internalize beliefs and stereotypes about their racial/ethnic group (i.e., group-focused IR) and/or about themselves because of their racial/ethnic group membership (i.e., self-focused IR; James, 2020). Among racial/ethnic minorities, IR is associated with poor psychological health (for meta-analysis see Gale et al., 2020). For example, previous research shows that IR predicts increased self-reported anxiety and depression symptoms (Campón & Carter, 2015; Hughes et al., 2015). However, while these IR–poor mental health associations have been well documented, little research has examined the underlying mechanisms of these associations (Williams et al., 2019).
Past scholars have theorized that IR leads to poor mental health among racial/ethnic minorities through IR’s negative effects on self-esteem, feelings of self-worth, and self-evaluations (Ahluwalia & Zegeye, 2001); however, empirical support for these claims is lacking. A more recent review suggested that IR is associated with poor mental health via its negative effects on one’s core self-evaluations (detailed below). Specifically, James (2020) suggests that IR leads racial/ethnic minorities to internalize (oftentimes negative) racial/ethnic cultural stereotypes, which leads to negative internal capacities in defining their beliefs, identities, and social relations. These negative internal capacities then lead to poor (mental) health outcomes. This research empirically investigates this core self-evaluation mediated pathway of IR on mental health (see James, 2020). This research is critical given that racial/ethnic minorities report poorer mental health than their US non-Hispanic White counterparts (Substance Abuse and Mental Health Services Administration, 2015).
What is Core Self-evaluation? And What is its Relationship with Mental Health?
Core self-evaluation is defined as a person’s fundamental evaluations about themselves, their own abilities, and their own control (Judge et al., 1997). Core self-evaluation concerns someone’s appraisal of their worthiness, effectiveness, and capability as a person, which is assumed to be central for self-regulation and motivation (Judge et al., 2003). Core self-evaluation consists of four traits: self-esteem, locus of control, emotional stability, and generalized self-efficacy (for review see Chen, 2012). In some instances, core self-evaluation is conceptualized as a higher order (latent) construct of these aforementioned traits (Johnson et al., 2008).
Self-esteem
Self-esteem is defined as a person’s global positive (or negative) feelings about themselves and overall feelings of their own worth (Rosenberg, 1965). As a result of these increased feeling of worth and value, high levels of self-esteem are associated with better mental health outcomes. For example, a longitudinal study by Orth et al. (2009) found that high levels of self-esteem predicted decreased risks for depression over a three-year, six-year and six-week period among adolescents and young adults. Indeed, a meta-analysis of longitudinal data shows that high self-esteem predicts lower anxiety and depression symptoms across time (Sowislo & Orth, 2013).
Locus of Control
Locus of control is described as the degree to which people see themselves as having control over their behavior and life outcomes (Rotter, 1966). Those with an internal locus of control believe that they control their life outcomes, whereas those with an external locus of control believe that their life outcomes are controlled by external forces (e.g., fate or powerful others; Rotter, 1966). A high internal locus of control (relative to a low internal and/or an external locus of control) is associated with positive mental health outcomes. For example, in a meta-analysis, Cheng and colleagues (2013), using 152 independent samples of 33,224 adults, found that a higher internal locus of control is negatively associated with depression and anxiety symptoms.
Emotional Stability
Emotional stability (or low neuroticism) refers to one’s ability to remain or feel calm and secure (Eysenck, 1990) or the ease with which people become upset or distressed (Bolger & Schilling, 1991). Meta-analytic and longitudinal data show that increasing emotional stability negatively predicts lower anxiety and depression symptoms/diagnosis and better overall mental health (Grevenstein et al., 2016; Jeronimus et al., 2016).
Generalized Self-efficacy
Generalized self-efficacy is the degree to which individuals believe that they have the ability or capacity to a achieve their goal or a desired outcome (Bandura, 1977). Higher generalized self-efficacy predicts better overall mental health (Schönfeld et al., 2016) and lower depression and anxiety symptoms (Muris, 2002; Soysa & Wilcomb, 2015).
Why are Core Self-evaluation Traits Associated With Mental Health Outcomes?
Self-esteem, locus of control, emotional stability, and generalized self-efficacy are considered to be core to one’s self-evaluations because they are evaluative, broad, and are fundamental to the self-concept (Smedema, 2014). Core self-evaluation traits are evaluative in that they involve appraisals, rather than descriptions, of the self (e.g., self-esteem involves the appraisals of self-worth; Rosenberg, 1965); they are broad in that they refer to self-based evaluations versus domain-specific evaluations (e.g., generalized self-efficacy versus academic self-efficacy); and are central to the self-concept given their involvement in perceptions and attitudes about the self (Smedema, 2014). As a result, core self-evaluation is often conceptualized as being “comprised of chronic beliefs about basic self-regulatory capacities” (Johnson et al., 2008, p. 396), which involve people’s beliefs about their ability to successfully interact with their environment.
Core self-evaluation traits are believed to affect (mental) health outcomes by influencing people’s appraisals of “situationally appropriate behavioral, emotional, and social strategies to reduce strain levels” (Kammeyer-Mueller et al., 2009, p. 179). Specifically, according to Kammeyer-Mueller and colleagues (2009), after appraising a situation as a stressor, people’s core self-evaluation influences their beliefs about the best ways to handle said stressor. This leads to a response that manifests in two ways: (1) core self-evaluation influences perceptions and judgments of experiences – situational appraisals; and/or (2) core self-evaluation influences the actions people take as a result of their perceptions and judgments – actions (Judge et al., 1997).
These situational appraisals and beliefs about appropriate actions to alleviate the stressor can increase (or decrease) risks to poor mental health via a process of emotional generalization (Johnson et al., 2008; Judge et al., 1997). That is, the positive self-views that result from high, more positive core self-evaluation, can lead individuals to approach positive information and avoid negative information. These approach and/or avoid tendencies influences evaluation of stimuli (e.g., “is this a stressor”), goal-directed behavior (i.e., behaviors that lead to approaching or avoiding stressors), and approach-based (e.g., elation) and avoid-based (e.g., fear) emotions (Kammeyer-Mueller et al., 2009). Ultimately, these situational appraisals and approach/avoid emotions and behaviors influences one’s risk for poor mental health. Indeed, meta-analytic data show that more positive or high core self-evaluation is associated with fewer perceived stressors, lower strain, less avoidance coping, and more problem-solving coping (Kammeyer-Mueller et al., 2009).
IR, Core Self-evaluation, and Mental Health
According to Hipolito-Delgado (2010), prolonged and continued exposure to racism (e.g., through media, racist experiences) and cultural pressures present during socialization processes lead racial/ethnic minorities to internalize beliefs and stereotypes about their racial/ethnic group. The internalization of these stereotypes and beliefs leads racial/ethnic minorities to “take in” and transform “real or imagined regulatory interactions with his[their] environment, and real or imagined characteristics of his[their] environment into inner regulations and characteristics” (Schafer, 1968, p. 9). That is, the “taking in” of cultural-based racial/ethnic stereotypes and beliefs becomes part of the individual’s identity, thus influencing their self-concept (Hipolito-Delgado, 2010).
Critically, however, James (2020) suggested that the relationship between IR and the self-concept depends on the valence (positive, negative) of racial/ethnic group stereotypes. For example, relative to Black/African American stereotypes, stereotypes about Asian Americans stereotypes are generally more positive (less negative; hardworking, intelligent vs. lazy, unintelligent; Ho & Jackson, 2001). Still, while both groups internalize racism, some evidence suggests that IR affects the self-concept of Black/African American and Asian Americans differently. For example, IR predicted increased academic self-efficacy among Asian American college students (Kantamneni et al., 2018) but lower education value among Black/African American college students (Brown et al., 2016). As such, among Black/African Americans, internalizing racism is commonly associated with negative self- and group-appraisals (Kohli et al., 2006).
For example, among Black/African Americans, IR is associated with lower self-esteem (Hughes et al., 2015) and lower generalized self-efficacy (Collins & Lightsey, 2001). In addition, Brown and colleagues (2016) found, among Black/African American college students, that IR predicted greater academic external (lower internal) locus of control in women, but not men – core self-evaluation captures broad self-evaluations, academic locus of control is domain specific. No research – to the author’s knowledge – has investigated the relationship between IR and emotional stability among Black/African Americans or other racial/ethnic minority groups.
Core Self-evaluation Mediated Pathway
Notwithstanding, James (2020) suggests that the internalization of negative cultural stereotypes leads to negative internal capacities, which then leads to poor mental health. Some, although limited, empirical data support claims of this core self-evaluation mediated pathway of IR on mental health. For example, James (2017) found, using a nationally representative sample of Black/African Americans, that self-esteem mediated the relationship between IR and DSM-IV criteria major depressive disorder (MDD). This indirect effect was such that IR was associated with lower self-esteem, which then predicted greater odds of MDD. Also showing evidence of this mediated pathway – although with a physical health outcome – Rivera and Paredez (2014) found that internalized racism predicted lower self-esteem, which then predicted increased body mass index among Hispanic American college students.
Although limited, these two studies provide some evidence of a core self-evaluation mediated pathway of IR on (mental) health. Notwithstanding, given theoretical and empirical evidence demonstrating relationships among IR, core self-evaluations and mental health, it is conceivable to assume that IR increases risks of poor mental health via decrements in core self-evaluation. In particular, drawing from the Challenge Model of the Risk and Resilience Framework (risk factors lead to negative outcomes through their relationship with one, or more, other risk factors: RiskA → RiskB → Outcome) it is likely that IR (a risk factor) leads to decreases in positive core self-evaluation (a second risk factor), which then results in poor mental health (Zimmerman & Arunkumar, 1994). This research examines this relationship.
Self-focused Versus Group-focused IR and Core Self-evaluation
On the one hand, while the effect (positive, negative) of IR on the self-concept might depend on the valence of racial/ethnic stereotypes (Brown et al., 2016; Kantamneni et al., 2018), the extent to which IR affects the self-concept (i.e., the strength of the relationship) is likely to be influenced by the conceptualization and measurement of IR. Particularly, in their review of 81 empirical studies, James (2020) identified two broad conceptualizations of IR: (1) self-focused IR, which captures people’s feelings, opinions, attitudes, views of themselves because of their racial/ethnic group membership (e.g., “I go through periods when I am down on myself for being Black”); and (2) group-focused IR, which captures people’s feelings, opinions, attitudes, and views of their racial/ethnic group (e.g., “Whites are superior to African Americans”).
Across these 81 studies, James (2020) found that approximately 76% and 27% of studies conceptualized IR as “group-focused” and “self-focused”, respectively. Moreover, James (2020) found that studies conceptualizing IR as “group-focused” were more likely to use measures of own-group racial/ethnic stereotype endorsement (e.g., Black/African American participants rating their agreement with Black/African American stereotypes), while studies conceptualizing IR as “self-focused” were more likely to use measures that captured participants’ feelings about themselves as members of their racial/ethnic group (e.g., “I go through periods when I am down on myself for being Black”). Indeed, studies measuring both self- and group-focused IR found different effects of the type of IR on the self-concept, such that self-focused IR had a stronger effect than group-focused IR.
For example, Jones and colleagues (2007) found that self-focused, but not group-focused, IR was associated with lower self-esteem among Black/African American women. Following similar result patterns, Vandiver and colleagues (2002) found a negative correlation between self-focused IR and self-esteem, but no correlation between group-focused IR and self-esteem. Relatedly, Gupta and colleagues (2011) found that self-focused and group-focused IR independently, but not interactively, predicted psychological distress among Asian American adults. Importantly, they found that the effect of self-focused IR on psychological distress was greater than the effect of group-focused IR. It is likely that self-focused IR has a stronger demonstrated effect than group-focused IR on self-concept-related outcomes given that self-referent attitudes are more likely to affect self-appraisals than group-referent attitudes (Krueger & Stanke, 2001; Sim et al., 2014). That is, race-influenced self-evaluations (i.e., self-focused IR) more strongly affect one’s core self-evaluations than race-influenced group-evaluations because they center around the self.
Current Study
This study examines the direct and indirect effects of IR on mental health outcomes via core self-evaluation (see Figure 1). The theoretical model draws from the Challenge Model of the Risk and Resilience Framework (Zimmerman & Arunkumar, 1994), along with meta-analytic evidence presenting IR as a risk to poor mental health (Gale et al., 2020). In addition, the model situates core self-evaluation traits as mediators of the IR–mental health relationship as meta-analytic and longitudinal data provide stronger evidence that core self-evaluations predict mental health than evidence that mental health predicts core self-evaluations (Cheng et al., 2013; Grevenstein et al., 2016; Sowislo & Orth, 2013). As such, this research investigates the independent direct and indirect effects of group- and self-focused IR on depression and anxiety symptoms via core self-evaluation traits.
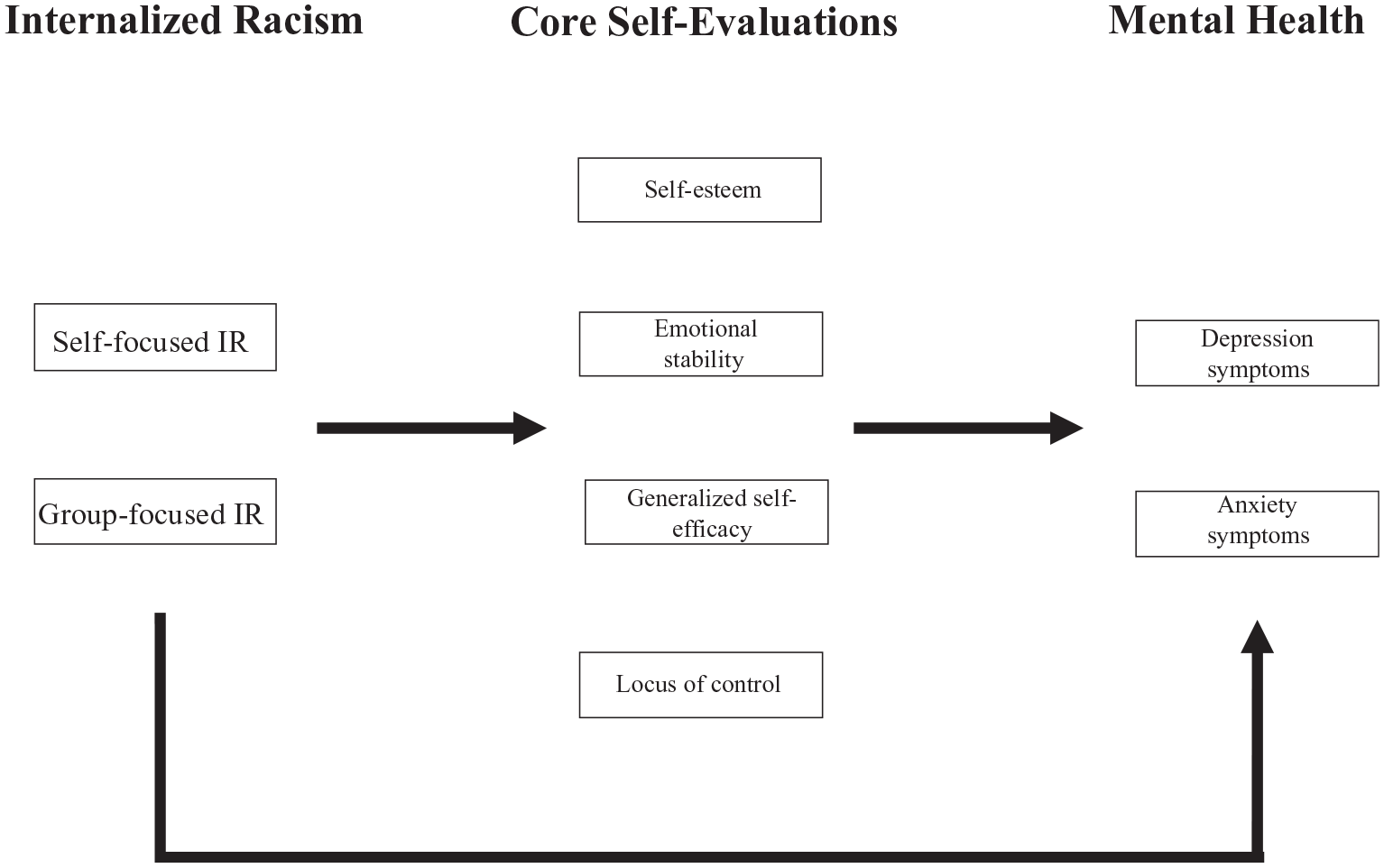
Hypothesized structural model presenting the direct and indirect effects of internalized racism on anxiety and depression symptoms via core self-evaluations (self-esteem, generalized self-efficacy, locus of control, emotional stability).
It is hypothesized that IR will positively predict anxiety and depression symptoms. In addition, it is expected that the direct effect of both types of IR on anxiety and depression symptoms will be mediated by core self-evaluation traits, such that self- and group-focused IR will predict lower core self-evaluation (i.e., lower self-esteem, internal locus of control, generalized self-efficacy, and emotional stability), which in turn will predict greater anxiety and depression symptoms. Last, it is expected that the effects IR on core self-evaluation traits will be stronger for self- (vs. group-)focused IR.
Method
Participants and Recruitment
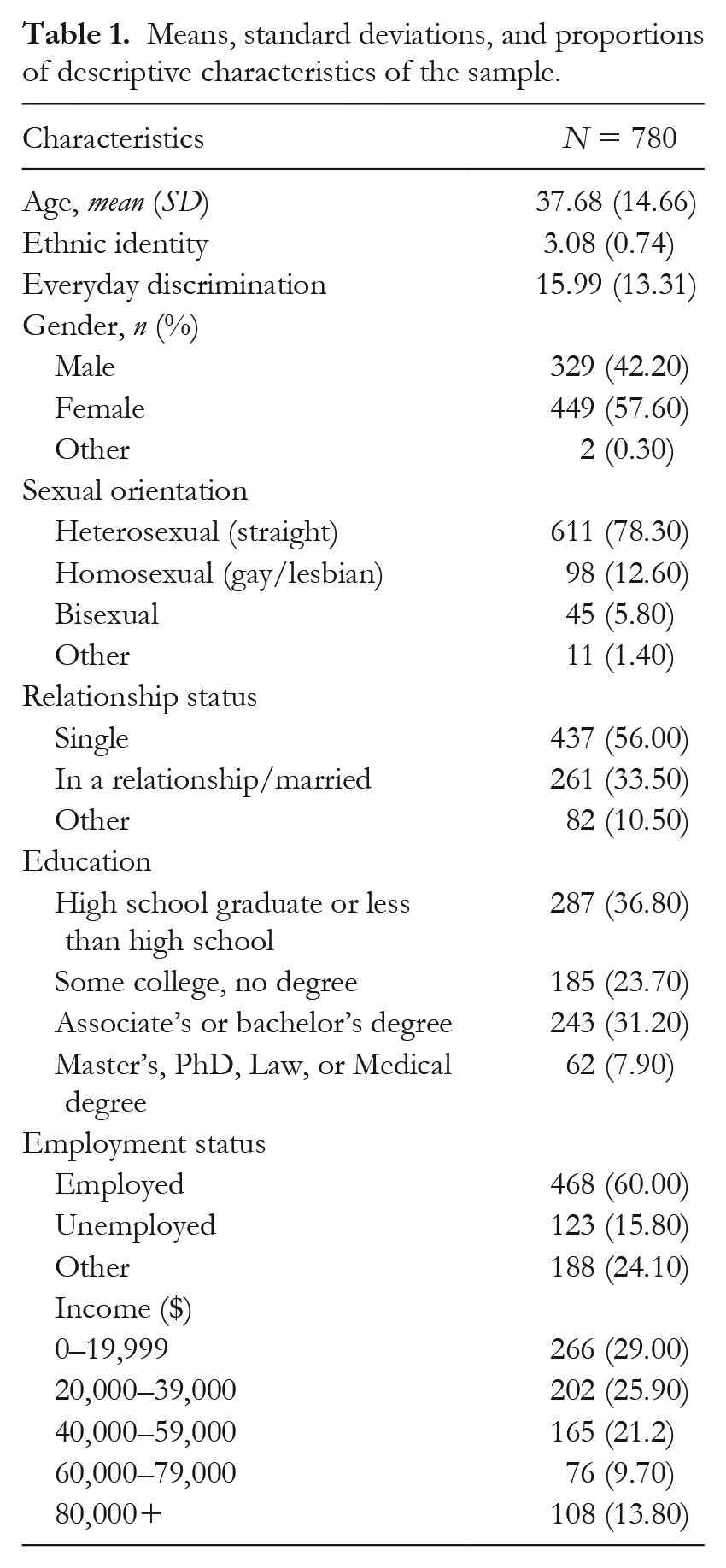
Seven hundred eighty Black/African American adults participated in this web-based survey study (Age: M = 37.68 years, SD = 14.66, range: 18–87; % Female = 57.6). Participants were recruited to complete an anonymous online survey using Qualtrics Panel (for more on the Qualtrics panel visit: https://www.qualtrics.com/research-services/online-sample/). Participants were targeted to participate if they self-identified as Black/African American and were 18 years of age or older. Participants were told that study investigated the social and psychological determinants of health among Black/African American adults. In addition to the measures included in this study, participants completed measures of health behaviors (e.g., sexually risky behaviors), adverse childhood experiences, and health beliefs. (For a complete list of questions included in the survey, please email the corresponding author.) The full study took approximately 60 minutes to complete. Participants were compensated for participating in the study. Compensation was based on participants’ agreement with their panel service provider, which included money, credit card points, and air travel miles. All participants provided informed consent. Data were collected in January 2020. The author’s Institutional Review Board approved this study.
Measures
Self-focused IR
Participants completed the pre-encounter self-hatred subscale of the Cross Racial Identity Scale (CRIS-SH; Worrell et al., 2004). The CRIS-SH is a six-item measure that assesses thoughts, feelings, and opinions about being Black on a seven-point Likert scale (1 = strongly disagree to 7 = strongly agree). Sample item includes: “I sometimes struggle with negative feelings about being Black”. All items were averaged. Higher scores represent greater self-focused IR (α = .94).
Group-focused IR
Participants reported their endorsement of four negative Black/African American stereotypes (Jackson et al., 2004) on a seven-point Likert scale (1 = not true at all to 7 = extremely true). Items include: “lazy”, “unintelligent”, “violent”, “criminal”. All items were averaged. Higher scores represent greater group-focused IR (α = .91).
Self-esteem
Self-esteem was measured using the 10-item Rosenberg Self-esteem Scale (Rosenberg, 1965) on a seven-point Likert scale (1 = strongly disagree to 7 = strongly agree). Sample item includes: “I feel that I have a number of good qualities”. The appropriate items were reverse-coded, and all items were then averaged. Greater values reflect higher self-esteem (α = .83).
Generalized Self-efficacy
Generalized self-efficacy was measured using the 10-item Generalized Self-efficacy Scale (Schwarzer & Jerusalem, 1995) on a four-point Likert scale (0 = not at all true to 4 = exactly true). Sample item includes: “When I am confronted with a problem, I can usually find several solutions”. All items were summed. Greater values reflect higher generalized self-efficacy (α = .84).
Locus of Control
Locus of control was measured using the eight-item locus of control subscale of the Levenson Multidimensional Locus of Control Scales (Levenson, 1973) on a five-point Likert scale (1 = strongly disagree to 5 = strongly agree). Sample item includes: “When I make plans, I am almost certain to make them work”. All items were averaged. Greater values reflect greater internal locus of control (α = .84).
Emotional Stability
Emotional stability was measured using the eight-item neuroticism subscale of the Big Five Inventory (John & Srivastava, 1999) on a seven-point Likert scale (1 = strongly disagree to 7 = strongly agree). Participants rated the extent to which a number of characteristics are typical of themselves. Sample item includes: “Is relaxed, handles stress well”. The appropriate items were reverse-coded. Greater values reflect greater emotional stability (α = .76).
Anxiety Symptoms
Anxiety symptoms were measured using the six-item anxiety subscale of the 53-item Brief Symptom Inventory (53-BSI; Derogatis & Melisaratos, 1983) on a five-point Likert scale (0 = never to 4 = very often). Participants rated the extent to which they had experienced select “problems” in the past month. Sample item includes: “Nervousness or shakiness inside”. All items were averaged. Greater values reflect higher levels of past-month anxiety symptoms (α = .93).
Depression Symptoms
Depression symptoms were measured using the six-item depression subscale of 53-BSI (Derogatis & Melisaratos, 1983) on a five-point Likert scale (0 = never to 4 = very often). Participants rated the extent to which they had experienced select “problems” in the past month. Sample item includes: “Feeling hopeless about the future”. All items were averaged. Greater values reflect higher levels of past-month depression symptoms (α = .93).
Covariates
The following socio-demographic variables were included as covariates: age, sex/gender, education, sexual orientation, relationship status, employment status, and income. In addition, participants’ everyday experiences with discrimination and their reported ethnic identity were included as covariates given that they are negatively and positively associated with better mental health among Black/African Americans, respectively (Pieterse et al., 2012; Smith & Silva, 2011). Experiences with discrimination were measured using the 10-item Everyday Discrimination Scale (Williams et al., 1997; α = .95). Ethnic identity was measured using the affirmation and belonging subscale of the Multigroup Ethnic Identity Measure (Phinney, 1992; α = .89).
Data Analytic Strategy
Structural Equation Models
Two structural equation modeling (SEM) analyses were used to test the independent direct and indirect effects of group- and self-focused IR on depression and anxiety symptoms via core self-evaluation. The first SEM model examined the direct and indirect effects of self-focused IR on anxiety and depression via core self-evaluation (Model 1). The second SEM model examined the direct and indirect effects of group-focused IR on anxiety and depression via core self-evaluation (Model 2).
Each SEM model used a two-step approach. Step 1: all covariates were allowed to predict all dependent outcomes. Step 2: all non-significant covariate associations (p > .05) were deleted and significant associations were retained in the final model (Hilbert et al., 2014). Both SEM models were estimated with the maximum likelihood method approach with specified covariances between anxiety and depression symptoms. An additional SEM analysis – using a similar two-step approach – included both self- and group-focused IR in the model to assess their independent direct and indirect effects while controlling for the other form of IR (a conservative test of hypotheses; Model 3). Last, given concerns about the inclusion of covariates in analyses, all models were also examined without any covariates (Ledgerwood, 2019; Wang et al., 2017).
The fit of each model was assessed using the following indices: the root mean square error of approximation (RMSEA); the comparative fit index (CFI); the Tucker–Lewis index (TLI); the standardized root mean square residual (SRMR); and the ratio of chi-square divided by degrees of freedom (χ2/df), which, relative to chi-square (χ2), is less likely to be affected by sample size (Schermelleh-Engel et al., 2003). By conventional standards, a model is considered a “good fit” if χ2/df ⩽ 3, CFI and TLI ⩾ .95, SRMR ⩽ .08, and RMSEA < .06 (Schreiber et al., 2006).
Post hoc power analyses
Given the complex nature of this study’s analyses, Monte Carlo simulations were carried out to assess post hoc statistical power – the probability of correctly rejecting H0 (Hoffman & McDowd, 2010; Schoemann et al., 2017). Indeed, according to Schoemann and collogues (2017) “for complex models such as mediation models, Monte Carlo power analysis may be the only method available to estimate statistical power” (p. 382). Briefly, Monte Carlo simulations are computer-driven studies in which parameters, such as population means and standard deviations and covariances – which are known a priori (from model results in this study) – are fitted to hypothesized models on random samples of generated data (Sigal & Chalmers, 2016). Monte Carlo simulations provide power estimates for multiple parameters in a single model (Schoemann et al., 2017).
Using Mplus, Monte Carlo simulations were conducted for all models. In Monte Carlo simulations, statistical power is estimated as the number of times H0 is correctly rejected in each generated sample divided by the total number of generated samples, specifically when “the proportion of replications for which the null hypothesis that a parameter is equal to zero is rejected at the .05 level” is greater than 80% (Muthén & Muthén, 2017, p. 472). See the online supplementary material for an example of Monte Carlo simulation codes using Mplus.
Results
Table 1 shows the means, standard deviations, and proportions of descriptive characteristics of the sample. Table 2 shows the means, standard deviations, and correlations of main study variables. Table 3 presents post hoc power analysis results for all models, with and without covariates. Table 4 shows fit indices and coefficient of determination (R2) for all models, with and without covariates. Fit indices show that models with covariates (“adequate-to-good”) fit relatively better than those without covariates (“bad fit”). As such, results of Models 1–3 with covariates are presented in text. Results for Models 1–3 without covariates are presented in the online supplementary materials.
Means, standard deviations, and proportions of descriptive characteristics of the sample.
Means, standard deviations, and correlations of main study variables.
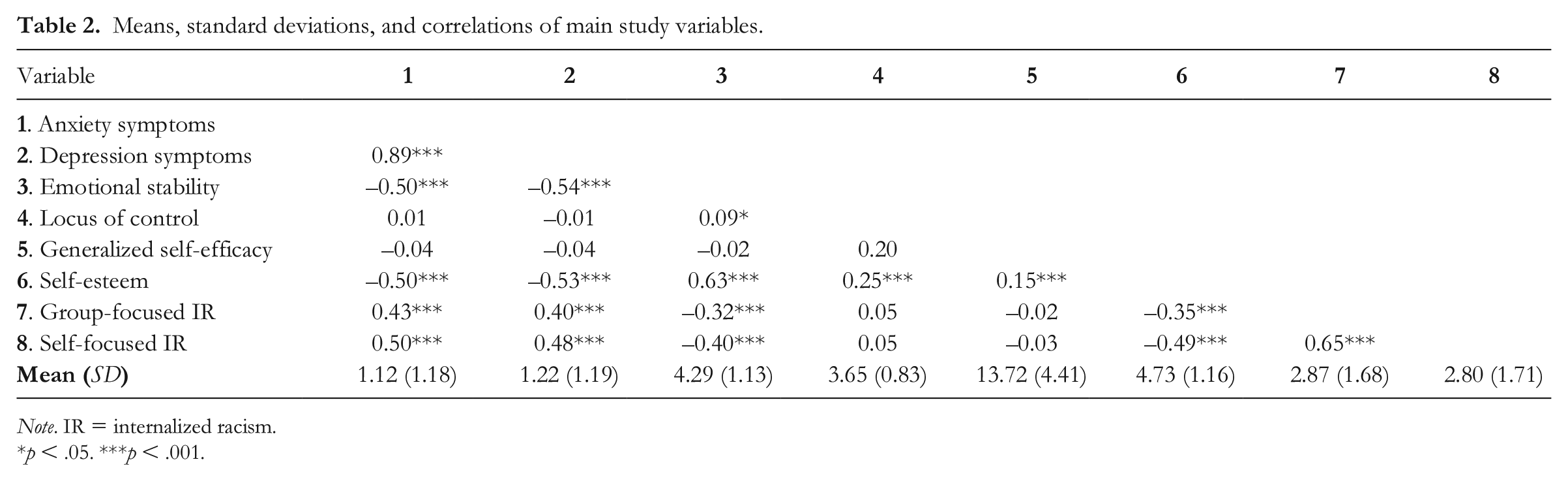
Note. IR = internalized racism.
p < .05. ***p < .001.
Estimate of power for each parameter in Models 1–3 with and without covariates.
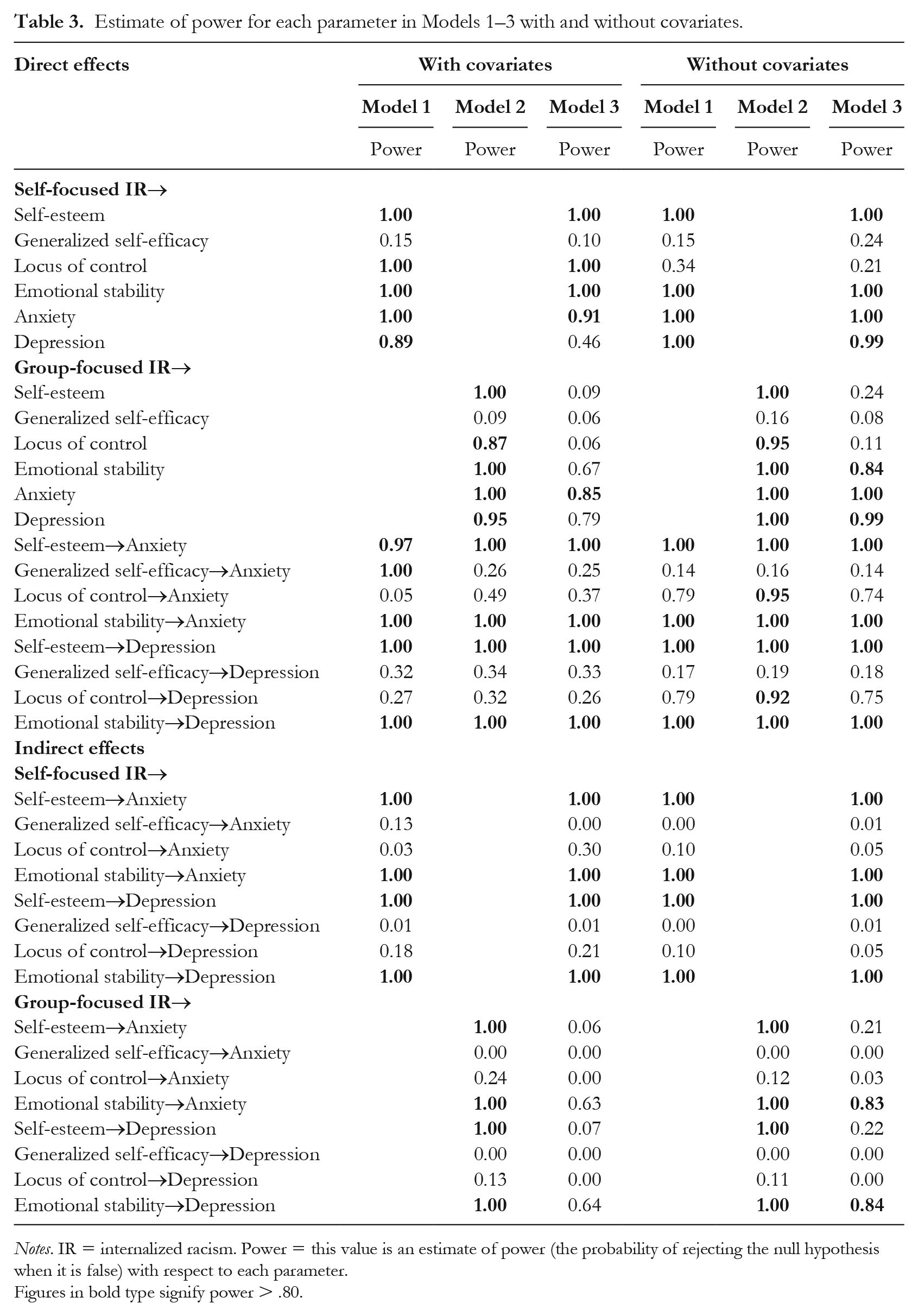
Notes. IR = internalized racism. Power = this value is an estimate of power (the probability of rejecting the null hypothesis when it is false) with respect to each parameter.
Figures in bold type signify power > .80.
Fit indices and R2 of the structural equation Models 1–3 with and without covariates.
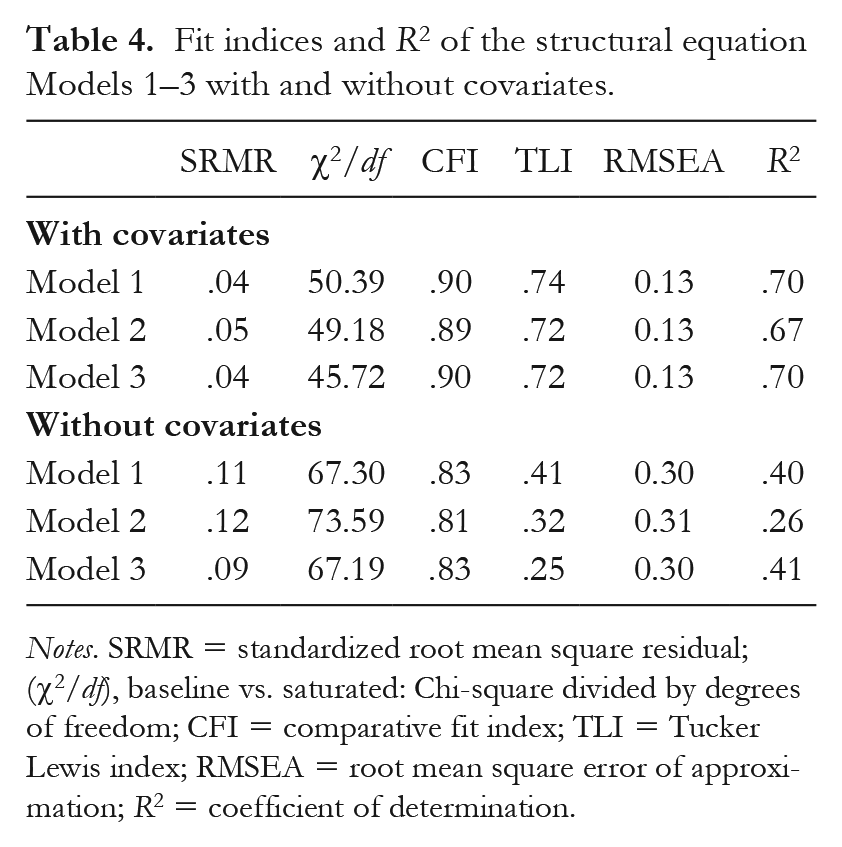
Notes. SRMR = standardized root mean square residual; (χ2/df), baseline vs. saturated: Chi-square divided by degrees of freedom; CFI = comparative fit index; TLI = Tucker Lewis index; RMSEA = root mean square error of approximation; R2 = coefficient of determination.
Structural Equation Models with Covariates
Figure 2 and Figure 3 present standardized coefficients for Models 1–2 and Model 3, respectively (see online supplementary materials for standardized covariate coefficients). Table 5 presents the indirect effect coefficients for Models 1–3 with covariates (see online supplementary materials for models without covariates).
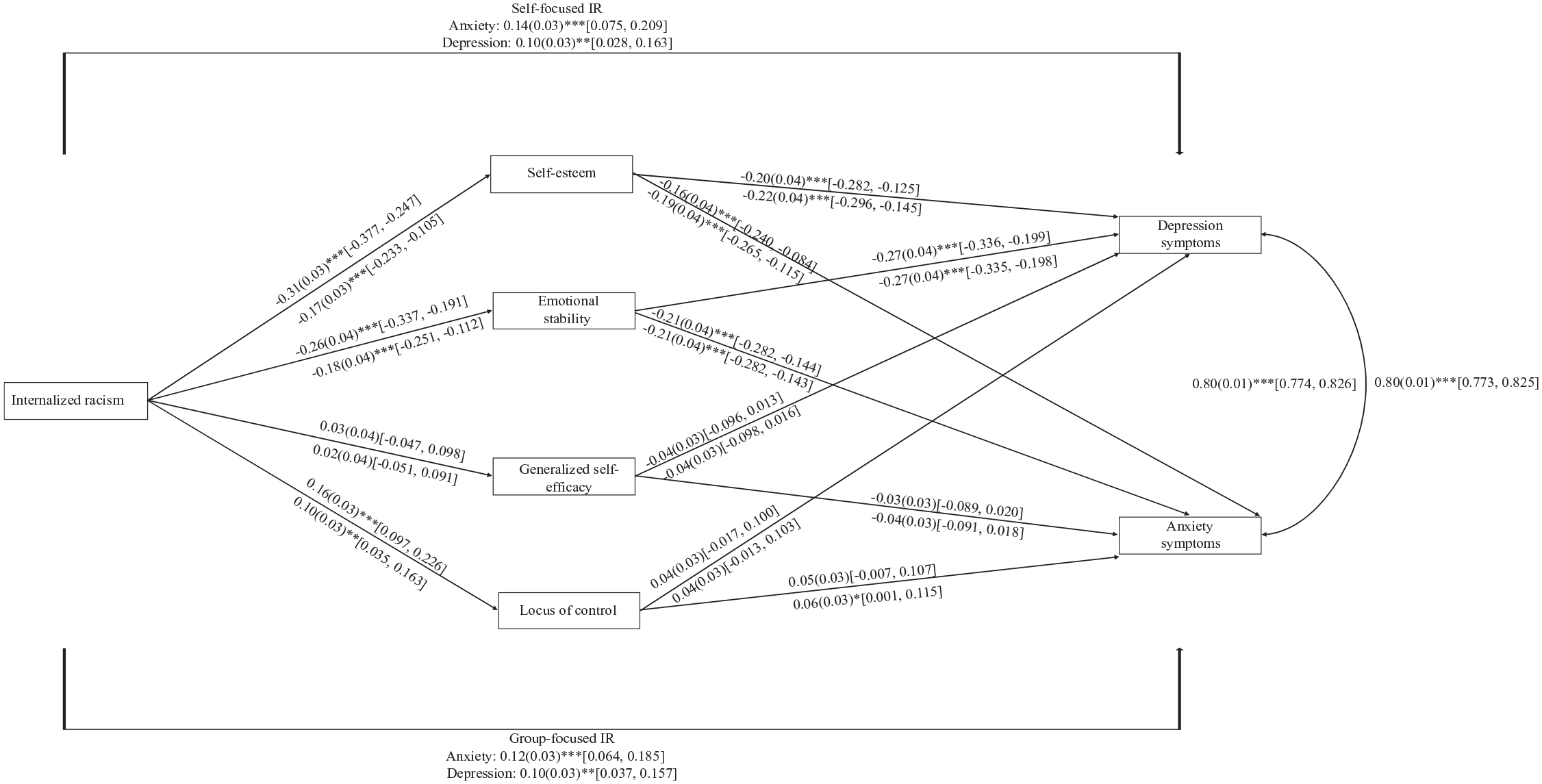
Structural model presenting (1) the independent direct and indirect effects of self-focused IR on anxiety and depression symptoms via core self-evaluations (Model 1), and (2) the independent direct and indirect effects of group-focused IR on anxiety and depression symptoms via core self-evaluations (Model 2). Path coefficients (to be interpreted as regression coefficients) are standardized. Standard errors are in parentheses. 95% confidence intervals are in brackets. Coefficients above the line represent relationships from Model 1. Coefficients below the line represent relationships from Model 2. Covariates are not included for clarity (see online supplementary materials for covariate effects).
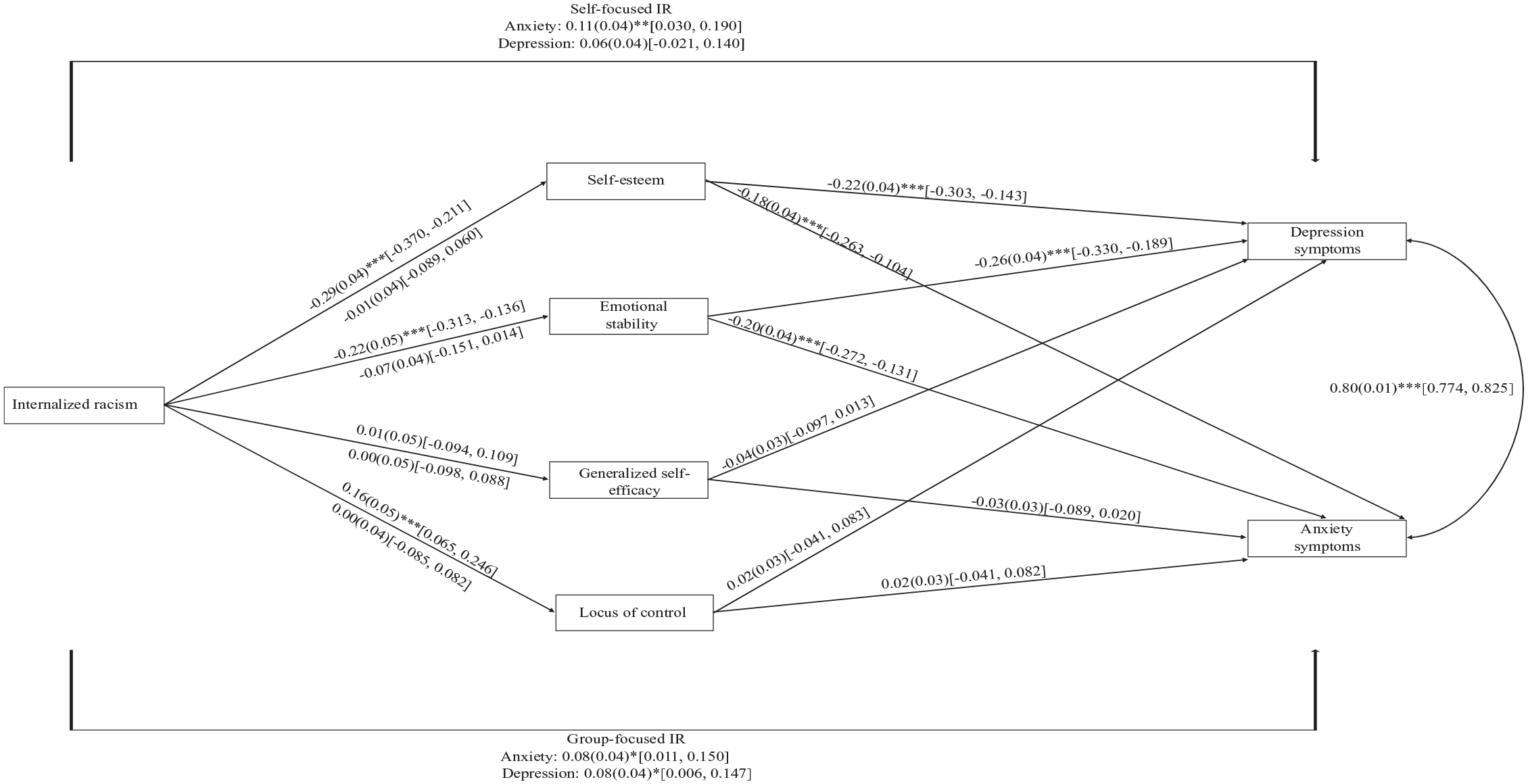
Structural model presenting the independent direct and indirect of self- and group-focused IR on anxiety and depression symptoms via core self-evaluations with simultaneous inclusion of both self- and group-focused IR (Model 3). Path coefficients (to be interpreted as regression coefficients) are standardized. Standard errors are in parentheses. 95% confidence intervals are in brackets. Coefficients above the line represent relationships for self-focused internalized racism. Coefficients below the line represent relationships for group-focused internalized racism. Covariates are not included for clarity (see online supplementary materials for covariate effects).
Indirect effect coefficients for Models 1–3.
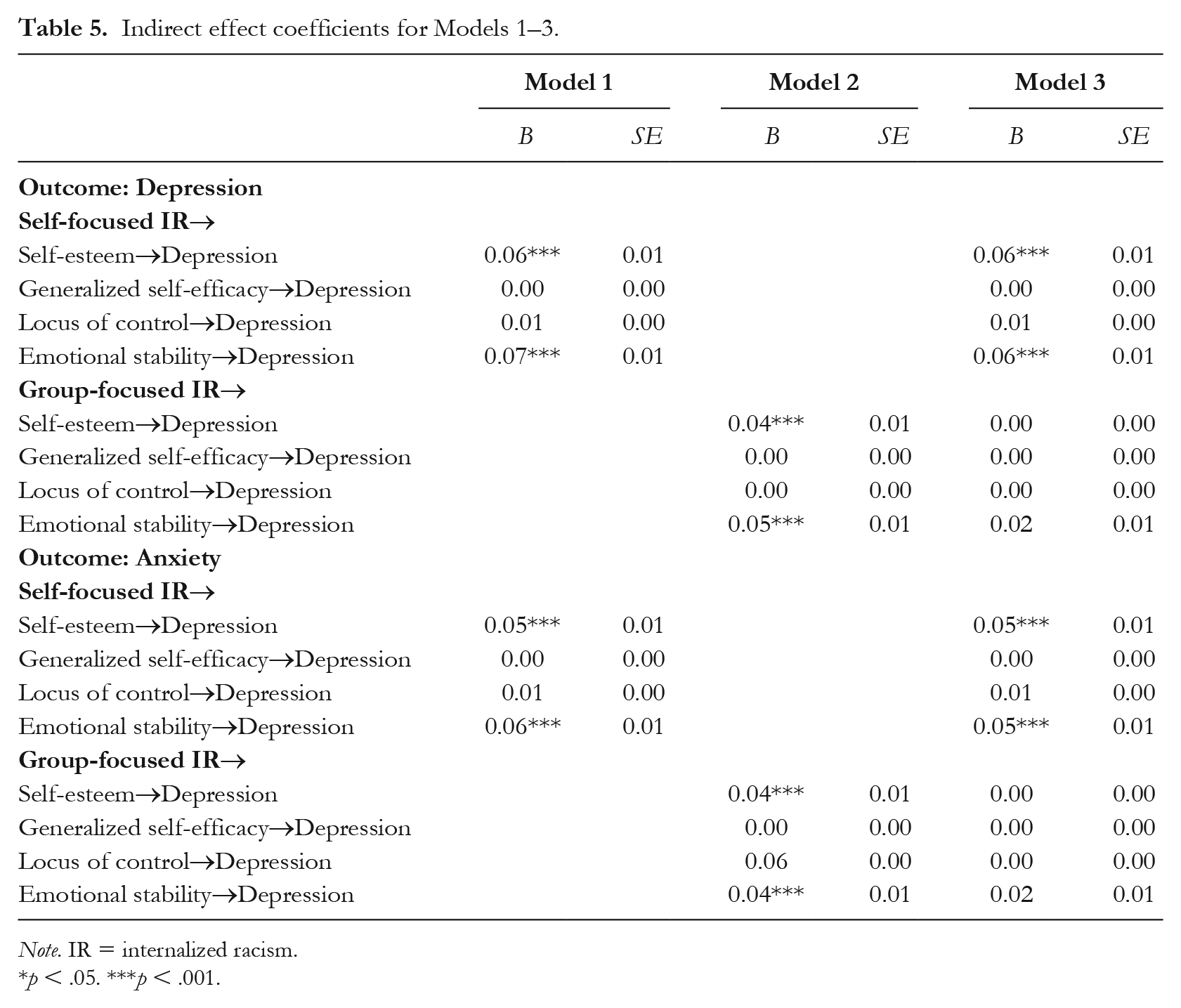
Note. IR = internalized racism.
p < .05. ***p < .001.
Direct Effects of IR
Confirming hypotheses, both self-focused and group-focused IR predicted greater anxiety and depression symptoms (see Figure 2). Also confirming hypotheses, self- and group-focused IR predicted lower reported self-esteem and lower emotional stability. However, against hypotheses, self- and group-focused IR predicted greater internal locus of control. Also against predictions, self- and group-focused IR were not associated with generalized self-efficacy (see Figure 2). When both self- and group-focused IR were included in the model simultaneously, group-focused IR was no longer associated with any core self-evaluation traits and self-focused IR was no longer associated with depression (see Figure 3).
Indirect Effects of IR
Confirming hypotheses, self-esteem and emotional stability mediated the indirect effect of self-focused IR on anxiety and depression symptoms. In particular, self-focused IR predicted (1) lower self-esteem and (2) lower emotional stability, which in turn predicted greater anxiety and depression symptoms. Presenting a similar pattern, self-esteem and emotional stability mediated the indirect effect of group-focused IR on anxiety and depression symptoms. Specifically, group-focused IR predicted lower (1) self-esteem and (2) lower emotional stability, which in turn predicted greater anxiety and depression symptoms. Against hypotheses, locus of control and generalized self-efficacy did not mediate the indirect effect of either self- or group-focused IR on anxiety or depression symptoms. Last, the indirect effects of group-focused IR on anxiety and depression symptoms via either self-esteem or emotional stability were no longer present when self-focused IR was included in the model (See Table 4 for indices).
Discussion
Direct Effects of IR
Confirming hypotheses, group- and self-focused IR predicted greater anxiety and depression symptoms. These results replicate previous work showing that IR increases the risk of poor mental health among racial/ethnic minorities (for meta-analysis see Gale et al., 2020). Also confirming hypotheses, self- and group-focused IR predicted lower self-esteem and emotional stability. These results also replicate previous work demonstrating negative relationships between IR and self-esteem (e.g., Campón & Carter, 2015). This is the first study – to the author’s knowledge – showing that increasing IR is negatively associated with emotional stability; a relationship consistent with previous theorizing (Ahluwalia & Zegeye, 2001).
Against predictions, although both self- and group-focused IR predicted internal locus of control, the relationship was in the opposite expected direction. In particular, self- and group-focused IR were associated with increased internal locus of control. This result, although against expectations, conceptually replicates previous work demonstrating the self-protective nature of IR. For example, Molina and James (2016) found that IR was associated with decreased odds of DSM-IV past-year major depressive disorder among a nationally representative sample of Afro-Caribbeans in the US. In this example, it is conceivable based on previous research that internal locus of control mediates the IR–positive mental health relationship. For example, previous research shows that those who are less aware of structural inequalities are more likely to internalize racism (Tran & Curtin, 2017) and that those who internalize racism are more likely to deny the existence of blatant racism, institutional racism, and white privilege (Campón & Carter, 2015). As such, it is possible that this lack of racial structural (inequality) awareness leads Black/African Americans higher in IR to increasingly believe in their own control of their life outcomes. This increasing internal locus of control resulting from increasing IR then leads to better mental health outcomes (Cheng et al., 2013).
Against predictions, neither self- nor group-focused IR predicted generalized self-efficacy. Although Collins and Lightsey (2001) showed that IR predicted lower generalized self-efficacious beliefs, this relationship was demonstrated in a Black/African American female only sample. As such, it is possible that gender might moderate the effect of IR on generalized self-efficacy (see also Buchanan & Selmon, 2008). In addition to gender, other factors such as socio-economic status (e.g., education and income; Assari, 2017), one’s endorsement of sex roles and mental health status (e.g., prior history with depression; Buchanan & Selmon, 2008) might also moderate the effect of IR on generalized self-efficacy. Future studies should investigate these and other factors as potential moderators of the IR-generalized self-efficacy relationship.
Indirect Effects of IR
Consistent with predictions, self-esteem and emotional stability mediated the indirect effect of both self- and group-focused IR on anxiety and depression symptoms. However, against predictions, locus of control and self-efficacy did not mediate these indirect effects. These results show partial support for the core self-evaluation mediated pathway of IR on mental health. This suggests that perhaps the indirect effect of IR on mental health outcomes operates through the more affective (i.e., self-esteem, emotional stability) relative to the more motivational (i.e., locus of control, self-efficacy; Chen, 2012) core self-evaluation traits.
Previous research finds self-esteem and emotional stability to be important determinants of affect regulation (i.e., the ability for an individual to modulate their emotional state; Heimpel et al., 2002; Tamir, 2005). For example, Wood and colleagues (2003) found that people with low self-esteem are more likely to dampen their mood when they feel good relative to those with high self-esteem. McNiel and Fleeson (2006) found that participants who were instructed to act in a neurotic way (“emotional, subjective, moody, and demanding”) reported more negative affect than those instructed to act in a stable way (“unemotional, objective, steady, and undemanding”). Given that negative affect increases risk of depression and anxiety (Brown et al., 1998), it is likely that the indirect effect of IR on depression and anxiety symptoms through decreased self-esteem and emotional stability reflects an increased propensity to experiencing negative affect.
On the other hand, Johnson and colleagues (2008) purport that generalized self-efficacy and locus of control are fundamental to “self-regulatory functioning” as they concern a person’s beliefs about their competence and their perceived control over their behavior and life outcomes (Bandura, 1977). As such, it is possible that whereas low self-esteem and emotional stability directly increase the likelihood of experiencing negative affect, low generalized self-efficacy and locus of control lead to lower beliefs about self-regulatory functioning capabilities. This reduced belief in one’s ability to engage self-regulatory functioning might lead to decreased self-regulatory behavior, which then increases the likelihood of experiencing negative affect.
Thus, unlike self-esteem and emotional stability, self-regulatory behavior might be an additional factor in the mechanistic path associating IR with mental health via locus of control and generalized self-efficacy. For example, Scoffer and colleagues (2010) found that low internal locus of control predicted lower self-regulation of eating attitudes, which increased disordered eating (e.g., “I avoid eating when I am hungry”). Similarly, Shikai and colleagues (2007) found that low generalized self-efficacy was related to decreased emotion-focused coping (i.e., blaming oneself for being too emotional), which then increased reported depression symptoms. Future studies should investigate self-regulatory behavior as an additional mediator in the IR core self-evaluation mental health predictive model.
Self- and Group-focused IR on Core Self-evaluation Traits
Last, as expected, the effect of self-focused IR on self-esteem, emotional stability, locus of control, and generalized self-efficacy (although non-significant) was stronger than the effect of group-focused IR on these outcomes. These patterns suggest, consistent with predictions, that race-influenced self-evaluations (i.e., self-focused IR) more strongly affect one’s core self-evaluations than race-influenced group-evaluations (Krueger & Stanke, 2001; Sim et al., 2014). This is also evidenced with Model 3 which shows that the direct effects of group-focused IR on core self-evaluation (and the resulting indirect effects IR via self-esteem and emotional stability) fall to non-significance when self- and group-focused IR are simultaneously included in the model.
Covariate, Model Fit, and Statistical Power Considerations
All models were examined with and without covariates given concerns around the inclusion of covariates in analyses (see Ledgerwood, 2019; Wang et al., 2017). Covariates were also included to strengthen claims of the direct and indirect effects of IR on mental health as factors such as ethnic identity and experiences with discrimination also influence Black/African American mental health (Pieterse et al., 2012; Smith & Silva, 2011). Indeed, fit indices show that models with covariates were a relative better fit than models without covariates. Nevertheless, no models were a “good fit” for the data (Schreiber et al., 2006).
Notwithstanding, scholars have cautioned against relying too heavily on fit indices, particularly RMSEA, to infer the theoretical meaningfulness of relationships among variables (Chen et al., 2008; Hayduk et al., 2007). Importantly, the specification of the SEM models (see Figure 1) was informed by theoretical and empirical evidence (Cheng et al., 2013; Gale et al., 2020; Grevenstein et al., 2016; Sowislo & Orth, 2013). In addition, the relationship among IR, core self-evaluation traits and mental health drew heavily on the hypothesized core self-evaluation mediated pathway of IR on mental health presented in James’ (2020) 81-study review of IR and health among racial/ethnic minorities. Nevertheless, although “theoretical meaningfulness” is important, so too is statistical power, especially when considering overall model fit (Chen et al., 2008).
To that end, Monte Carlo simulations were carried out to assess post hoc statistical power – the appropriateness of this study’s sample size – given some unexpected findings (Hoffman & McDowd, 2010). One advantage of a Monte Carlo simulation is that it provides power estimates for each parameter included in a model (Schoemann et al., 2017). As such, post hoc power estimates were calculated for all main predictors in this study. Results from the Monte Carlo simulations show that while the indirect effects of IR (self- and group-focused) on depression and anxiety via either self-esteem or emotional stability across all models (with and without covariates) were appropriately powered (> .80), the indirect effects of IR via either locus of control or generalized self-efficacy were not.
According to Wolf and colleagues (2013), the difference in statistical power across these indirect effects in the same sample occurs because larger effects are likely to achieve statistical power for direct and indirect effects with relatively smaller samples. This is evidenced by results revealing stronger effects of group- and self-focused IR on self-esteem and emotional stability than either locus of control or generalized self-efficacy. Similar patterns emerged such that the effects of self-esteem and generalized self-efficacy on anxiety and depression were greater than the effects of either locus of control or generalized self-efficacy. Altogether, the post hoc power analysis results provide stronger support for the indirect effects of IR (self- and group-focused) on depression and anxiety via either self-esteem or emotional stability than for the indirect effects via either locus of control or generalized self-efficacy. Indeed, assuming similar effects, Monte Carlo simulations suggest a sample of N > 3500 to detect indirect effects of IR via either locus of control or generalized self-efficacy at p < .05.
Last, some effects differed between the models with covariates and those without covariates. For example, the indirect effect of group-focused IR on depression was significant in models without covariates but not those with covariates. These differences in the models with and without covariates are likely due to difference in statistical power that result from the increased number of parameters included in models with covariates (see results of post hoc power analyses; Wolf et al., 2013). Underscoring previous claims, these allow for greater confidence in results showing the indirect effect of IR on mental health via the more affective components of core self-evaluations (i.e., self-esteem, emotional stability) relative to the more motivational components (i.e., locus of control, generalized self-efficacy). Still, future research should replicate this study with a larger sample.
Conclusion
This study addresses a significant gap in current scholarship on IR, namely the mechanism through which IR affects racial/ethnic minority health (James, 2020). In particular, this shows that IR (self- and group-focused) is associated with poor mental health among Black/African American adults via decrements in self-esteem and emotional stability. Post hoc power analyses suggest a need to replicate this research with a larger sample to detect to the indirect effects of IR on depression/anxiety via either locus of control or generalized self-efficacy. This research shows, replicating previous findings, that how IR is measured (and conceptualized) is important to understanding its phenomenology. Importantly, this study shows that how IR is measured (and conceptualized) affects the conclusions made about its determinants and consequences. Future research on IR should pay explicit attention to how IR is measured to more fully address current theoretical and conceptual limitations of contemporary IR scholarship (see James, 2020). Future studies should also investigate the relationships among IR, core self-evaluations, and mental health longitudinally with representative samples to address concerns of causality and between- and within-person variation and generalizability.
Altogether, this study investigated the direct and indirect effects of group- and self-focused IR on depression and anxiety symptoms via core self-evaluation (i.e., self-esteem, generalized self-efficacy, locus of control, emotional stability). Results show that self-esteem and emotional stability mediated the indirect effects of both self- and group-focused IR on anxiety and depression symptoms – with statistical power of these indirect effects > .80. However, the results show no indirect effects of either self- or group-focused IR on anxiety and depression symptoms via either locus of control or generalized self-efficacy, which is attributed to lower statistical power of these parameters. As such, this research should be replicated with a larger sample to detect the indirect effects of IR on depression and anxiety symptoms via either locus of control or generalized self-efficacy. Importantly, this research informs understanding of the mechanisms associating IR with poor (mental) health among Black/African American adults and has implications for addressing racial/ethnic (mental) health disparities broadly.
Supplemental Material
Supplementary_Material – Supplemental material for Self- and group-focused internalized racism, anxiety, and depression symptoms among African American adults: A core self-evaluation mediated pathway
Supplemental material, Supplementary_Material for Self- and group-focused internalized racism, anxiety, and depression symptoms among African American adults: A core self-evaluation mediated pathway by Drexler James in Group Processes & Intergroup Relations
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.