
Abstract
Objective
To investigate the conventional ultrasound (US), contrast-enhanced ultrasound (CEUS) manifestations and the corresponding histopathological characteristics of patients diagnosed with breast encapsulated papillary carcinoma (EPC) and to explore the value of CEUS in diagnosis of EPC.
Methods
The clinical, pathological, US, and CEUS features of 16 patients (17 lesions) with EPC confirmed by postoperative histopathology were retrospectively analyzed.
Results
EPC was prevalent in the postmenopausal women. The majority of conventional US images of EPC showed complex cystic and solid masses with circumscribed margins (70.6%), enhanced posterior echo (94.1%), no sonographic calcification (88.2%), rich blood flow in the solid components within lesions (70.6%) on Color Doppler flow imaging, and high resistance index of blood flow (94.1%). Moreover, CEUS showed mainly centripetal hyperenhancement of the solid components within the lesions with irregular outline, and the enhancement area of the whole masses was essentially the same as the B-mode US area.
Conclusions
EPC typically presents as a complex cystic and solid mass. CEUS is helpful to clarify the extent of the solid component and facilitate preoperative core-needle biopsy. A comprehensive evaluation by CEUS is valuable for diagnosing EPC and combining it with clinical features are helpful to further improve the diagnosis of this rare kind of breast cancer.
Keywords
Introduction
Breast encapsulated papillary carcinoma (EPC) is a rare and specific type of breast cancer, accounting for approximately 0.5%–1% of malignant breast tumors. 1 EPC lacks specificity in its clinical presentation and is notoriously difficult to make an accurate pathological diagnosis with preoperative core-needle biopsy due to its cystic-solid nature.2,3 Ultrasound (US) is an important tool in detection of breast disease.4–8 Contrast-enhanced ultrasound (CEUS) can sensitively separate areas of proliferation from necrosis or fibrosis within the tumor, thus effectively improving the success rate of sampling and accuracy of pathological diagnosis in suspected breast cancer cases by preoperative core-needle biopsy. Therefore, preoperative multimodal US assessment is critical for clinical diagnosis and treatment of EPC. The Breast Imaging Reporting and Data System (BI-RADS) is an imaging report and data that classifies lesions based on information from imaging examinations. It effectively distinguishes between benign and malignant breast lesions and provides a reliable reference range for the risk of malignancy to guide clinical decision-making. Owing to the rarity of EPC, the number of research papers available is limited, with most of them being case reports.9,10 No systematic studies on US and CEUS features have been reported. In the present study, we focused on the features of conventional US and CEUS of 16 patients with EPC in combination with pathological characteristics, aiming to deepen the understanding of the ultrasonic features, better diagnostic accuracy, and minimize missed diagnosis. These efforts will yield more valuable information for precise clinical diagnosis and treatment of this rare kind of breast cancer.
Materials and methods
Study sample
The clinical data of 16 patients (17 lesions) who underwent both US and CEUS exams before surgery and were diagnosed with EPC based on postoperative pathology at the Affiliated Hospital of Guangdong Medical University from January 2020 to September 2023, were retrospectively reviewed, collected, and analyzed. The collection included preoperative US images, CEUS images, surgical approaches, and postoperative pathological diagnostic information. The study was reviewed and approved by the Affiliated Hospital Ethics Committee of Guangdong Medical University [IRB: PJKT2023-123]. All participants gave informed consent and signed an informed consent form.
Instruments and methods
Ultrasonography was performed using the following high-resolution US systems with a 2–10 MHz, 7–10 MHz, or 4–10 MHz linear-array transducer: Acuson sequoia (Siemens, Germany); Aplio 500 (Canon, formerly Toshiba, Japan); Aplio 400 (Canon, formerly Toshiba, Japan). US exams were performed following the examination specifications of breast. The patients were placed in a supine or reclined position with both hands raised above the head, thereby exposing the axilla. The frequency, focus, gain, and depth of the instrument were adjusted based on the patient's condition to achieve optimal image quality. During the process of CEUS, the probe remained fixed while injecting a 4.8 mL SonoVue solution sourced from Bracco in Italy through the anterior elbow vein, followed by a quick injection of 5 mL of 0.9% NaCl solution. The arterial perfusion status of the lesions were monitored by real-time imaging, and the 2-min contrast enhancement images were observed and recorded.
The US features of the masses were evaluated, and the relevant data were documented in accordance with the fifth edition of the BI-RADS for US lexicon released in 2013. 11 Color Doppler flow imaging (CDFI) was used to detect both peripheral and internal blood flow signals of the lesions. According to Adler's semi-quantitative method, 12 the class of blood flow signals were graded: grade 0, no blood flow; grade 1, little blood flow; grade 2, moderate blood flow; grade 3, abundant blood flow.
Detection of pathological and histological characteristics
The specimens after surgical excision of breast masses were stained with routine hematoxylin-eosin staining (HE) and immunohistochemistry. Estrogen receptor (ER), progesterone receptor (PR), human epidermal growth factor receptor-2 (HER-2), and Ki-67 proliferation index were detected. Referring to the 2020 version of the Guidelines of Chinese Society of Clinical Oncology (CSCO) on Diagnosis and Treatment for Breast Cancer, 13 ER and PR ≥ 1% were defined as positive; HER-2 was determined to be positive if the immunohistochemistry result was 3+ or in situ hybridization (ISH) testing showed gene amplification. Additionally, low expression was classified as Ki-67 < 15%, while high expression was defined as Ki-67 > 30%.
Results
Clinical findings
The 16 patients diagnosed with EPC were all females, ranging in age from 45 to 83 years, with a median age of 60 years. Each patient presented to the clinic due to a breast lump unaccompanied by nipple discharge or retraction (Table 1).
The clinical features of patients.
Conventional US characteristics
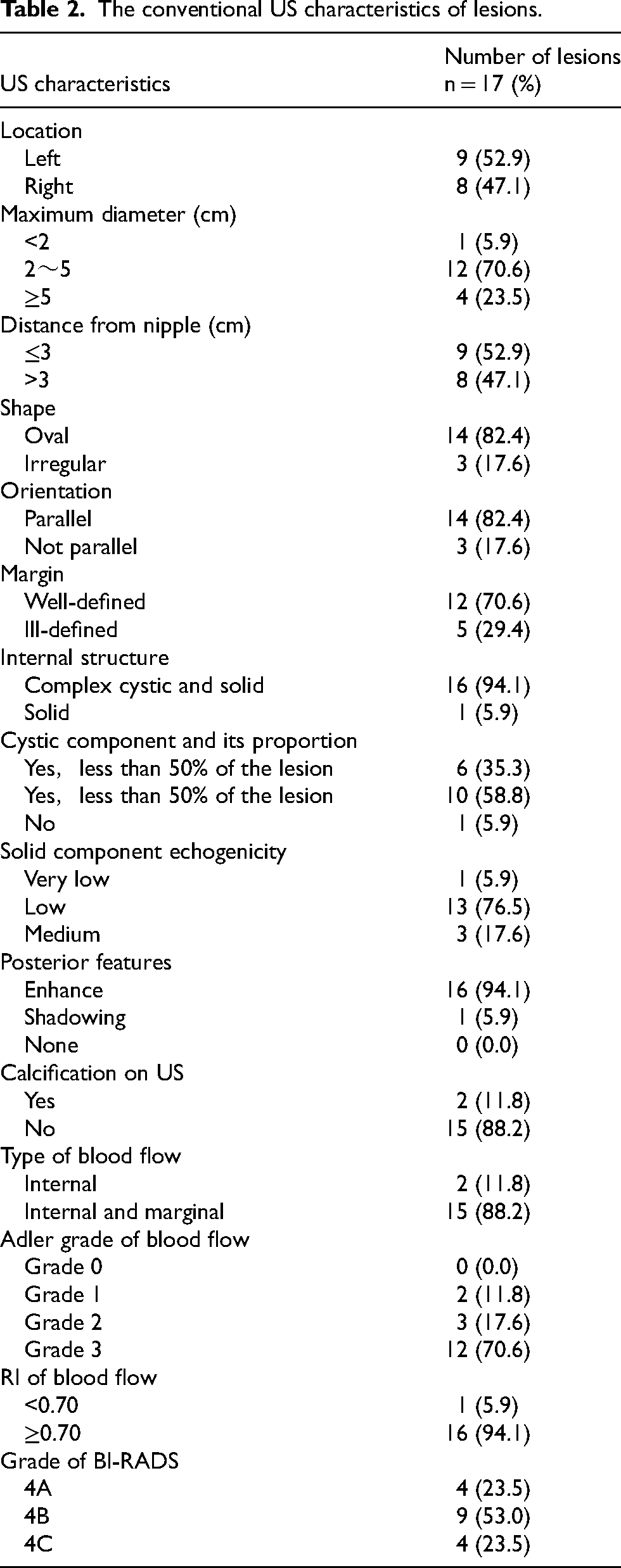
Of the 16 patients with EPC included, 1 patient had lesions in both breasts, resulting in a total of 17 lesions, of which 9 were located in the left breast while 8 were in the right breast (Table 2). The conventional US of the 17 lesions in this study showed mostly oval (82.4%), parallel orientation (82.4%), well-defined (70.6%), enhanced posterior echo (94.1%), no sonographic calcification (88.2%) and complex cystic and solid (94.1%) lesions, with the cystic region in the lesion less than 50% of the lesion (58.8%) and the solid components being predominantly low echogenicity (76.5%). The lesions mainly had internal and marginal blood flow (88.2%) on CDFI. They also showed Adler grade 3 (70.6%) on CDFI and high resistance index (RI) of blood flow (94.1%) on Doppler spectrum (Figure 1). All lesions were classified by BI-RADS assessment based on conventional US characteristics, resulting in 4 lesions rated as BI-RADS 4A, 9 rated as BI-RADS 4B, and 4 rated as BI-RADS 4C.
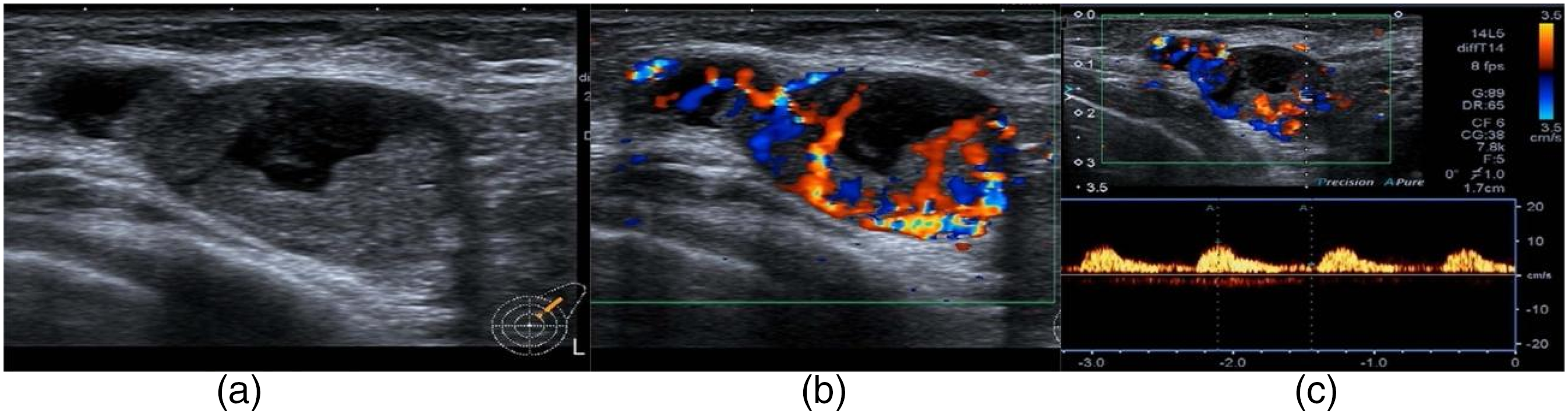
(a) B-mode US showed a complex cystic and solid lesion with clear board and posterior echo enhancement. (b) Abundant blood flow (Adler grade 3) within and around the lesion was observed on CDFI. (c) Doppler spectrum showed that arterial spectra with high RI (RI = 0.71) could be detected.
The conventional US characteristics of lesions.
CEUS characteristics
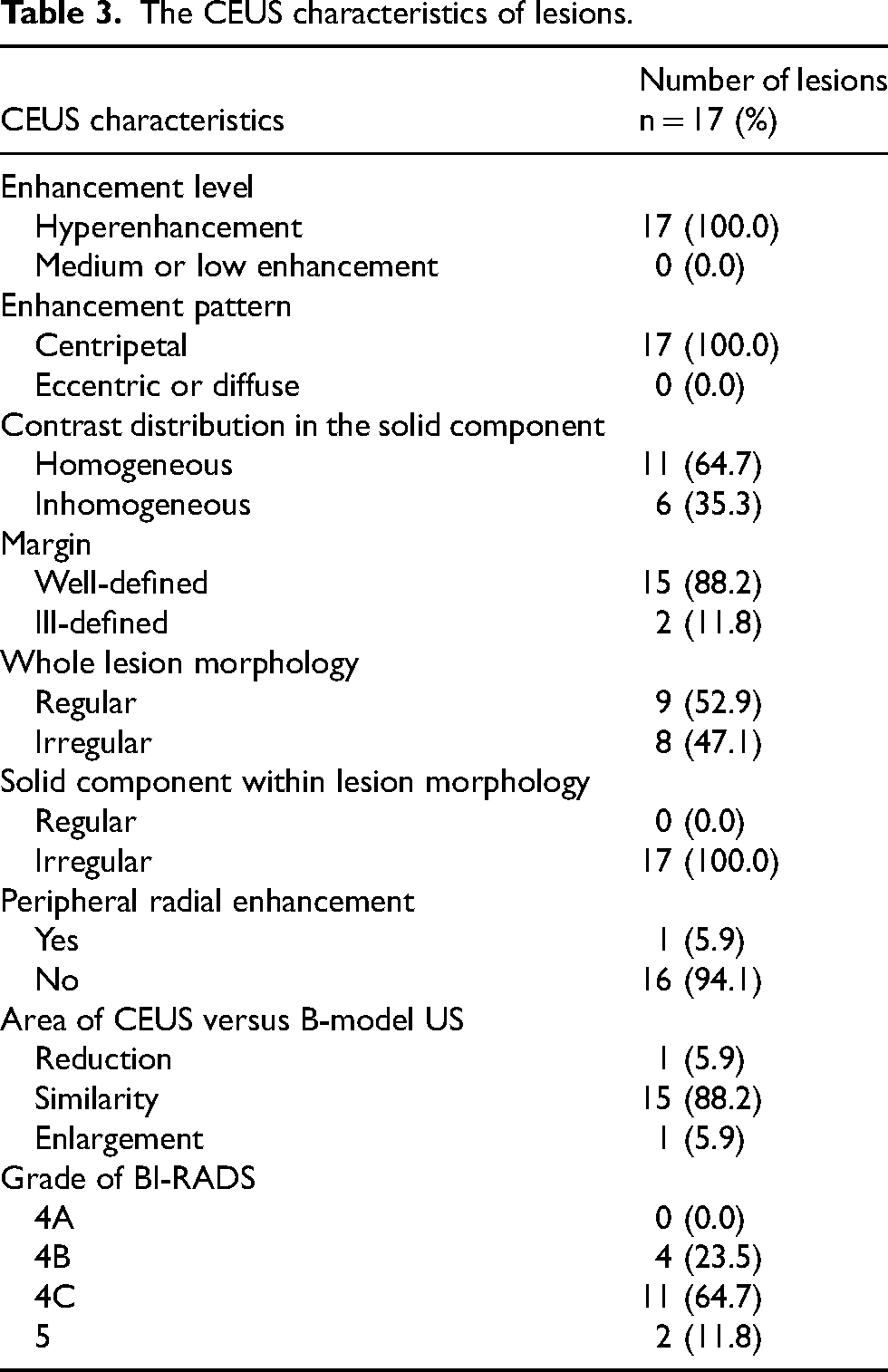
Compared to the surrounding breast tissue, the enhancement of solid components within lesions were irregular (100%), predominantly homogeneous (64.7%), and centripetal (100%) hyperenhancement (100%) (Table 3). The whole lesions enhancement generally exhibited regular morphology (52.9%), well-defined borders (88.2%), absence of radiolucent vessels in the periphery of the lesion (94.1%), as well as a similar area of B-mode US and CEUS (88.2%) (Figure 2). All lesions included in the study were classified by BI-RADS assessment according to CEUS characteristics. Then 4 lesions were classified as BI-RADS 4B, 11 were classified as BI-RADS 4C and 2 were classified as BI-RADS 5.
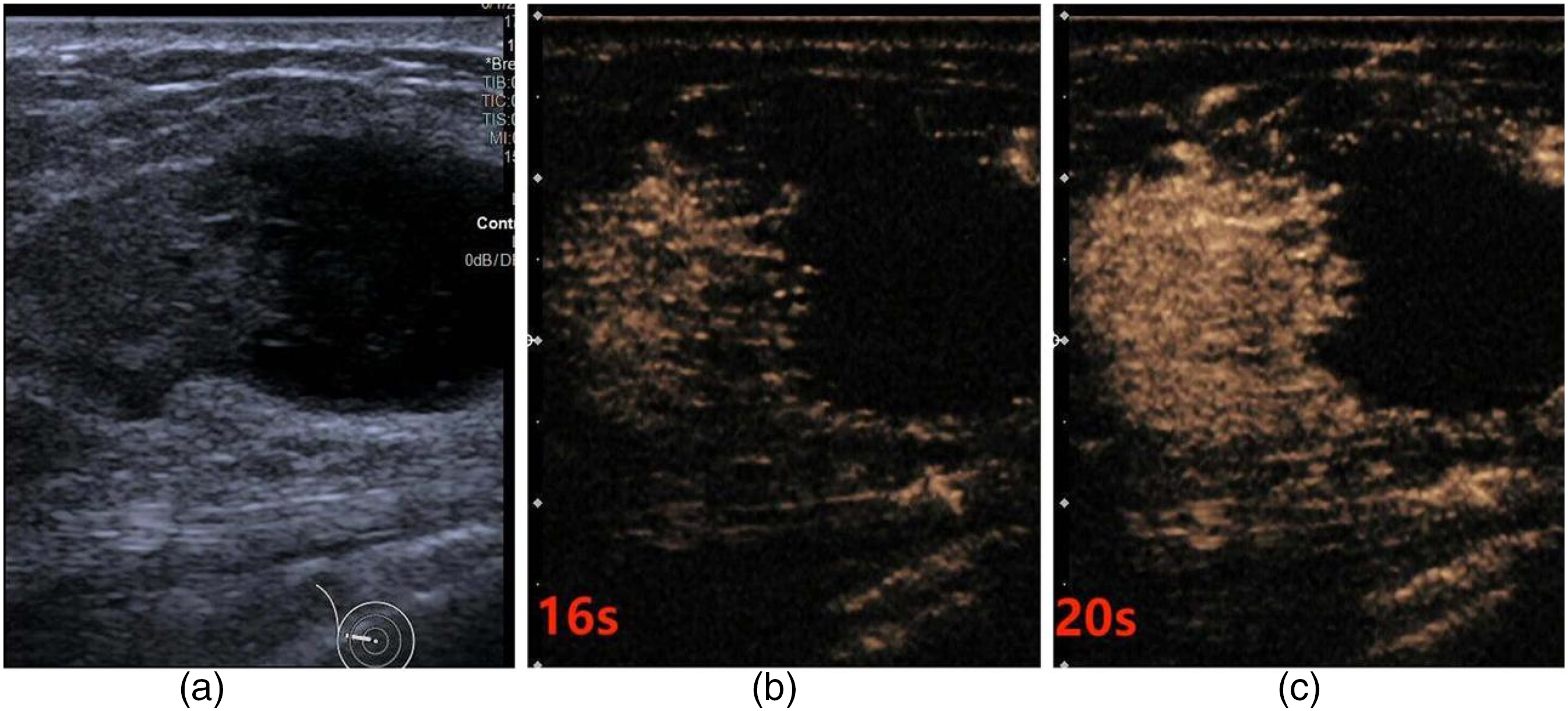
(a) A cystic-solid complex echogenic mass was observed on B-mode US. (b) CEUS showed a hyperenhancement mass, which rapidly enhanced at 16 s. (c) At 20 s, CEUS showed homogeneous enhancement and there was no radial enhancement sign in the periphery of the lesion. The area of the whole lesion enhancement was essentially the same as the B-mode US area.
The CEUS characteristics of lesions.
Pathological findings
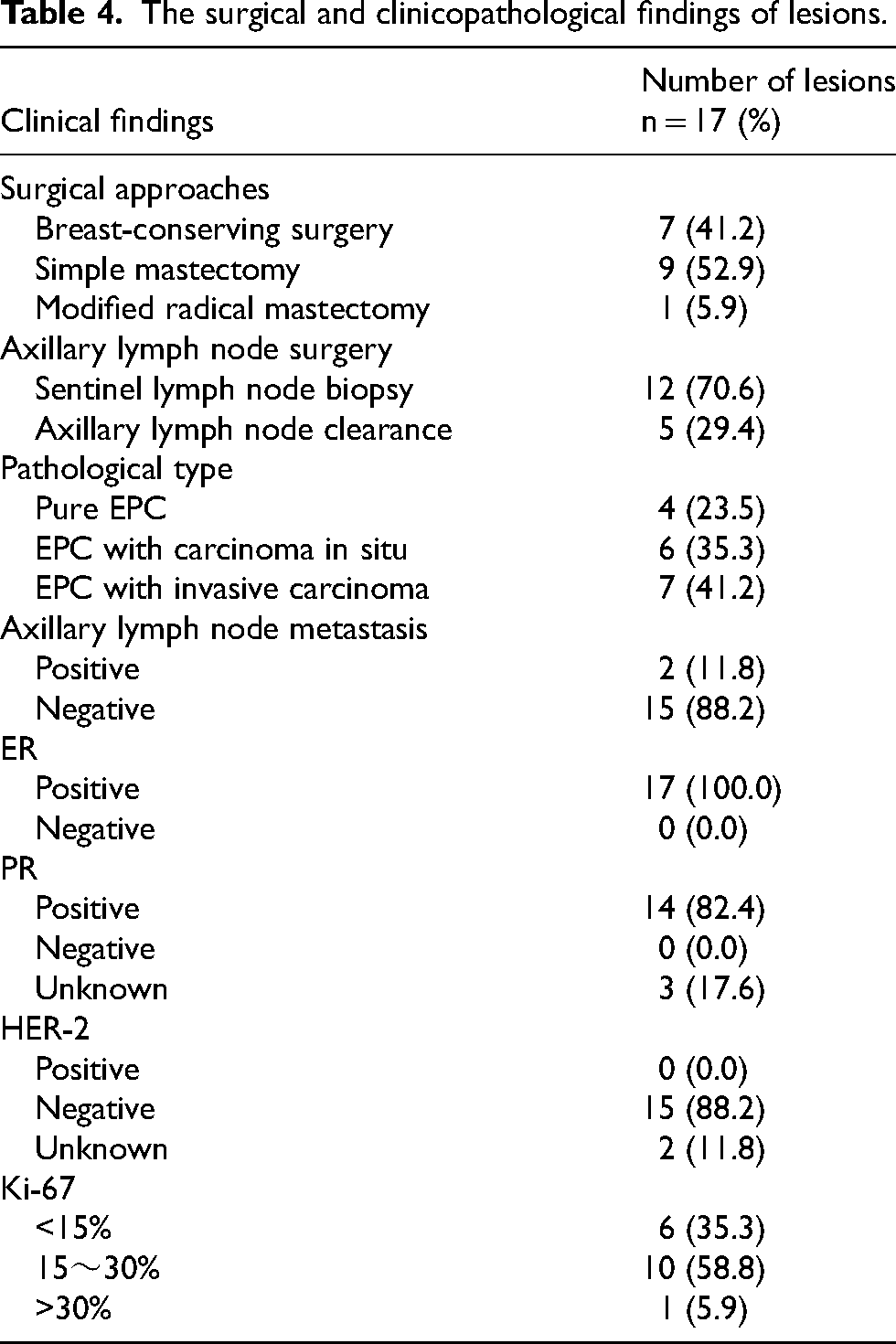
Surgery was performed on all lesions. 7 lesions (41.2%) underwent breast-conserving surgery, of which 5 patients received postoperative radiotherapy. 9 of the lesions (52.9%) underwent simple mastectomy (Table 4). 1 lesion (5.9%) underwent a modified radical mastectomy, and the patient was treated with chemotherapy after the surgery. Sentinel lymph node excision biopsy was performed in 12 lesions (70.6%). Axillary lymph node clearance was performed in 5 lesions (29.4%), of which pathologically confirmed axillary lymph node metastasis was found in 2 cases, and both of them were patients with EPC with invasive carcinoma.
The surgical and clinicopathological findings of lesions.
Discussion
EPC, which was previously referred to as intracapsular papillary carcinoma, was once thought to be a variant of ductal carcinoma in situ. 14 It manifests as a papillary carcinoma inside a dilated duct. Subsequent research has concluded that such tumors are rare, expanding-growing, and non-aggressive malignancies. 1 The neoplastic lesions located in the fibrous capsule wall and were lack of myoepithelial cells in the central papilla and surrounding the capsule wall, 15 which led to the term EPC. The 2012 edition of the World Health Organization (WHO) classification of breast tumor categorized it as a distinct subtype of the papillary lesions. 16 EPC is generally viewed as an intermediate pathological type between carcinoma in situ and invasive carcinoma among the majority of scholars.15,17
EPC is more prevalent in postmenopausal women but has also been reported in males and young females.18,19 In this study, the patients were mostly menopausal females, with a median age of 60 years, which gives a hint that older age is a significant predictor of intracapsular papillary malignant tumors. 20 In addition, there is a hypothesis 21 that EPC with a larger size may predictably have a higher likelihood of being associated with invasion. The final pathology of this study showed that the median sizes of pure EPC, EPC with carcinoma in situ, and EPC with invasive carcinoma were 2.6 cm, 2.8 cm, and 3.3 cm, respectively. It suggests that the size of the lesion may be of great value in identifying the pathological type of EPC. Patients with EPC are commonly referred to the clinic with a palpable lump in the breast, sometimes accompanied by nipple discharge. In the present study, they all were presented to the clinic with a palpable breast lump as the primary symptom, with no nipple discharge and hard on palpation, which accorded with previous reports in the literature. 22
With its advantages of low cost, non-invasiveness, sensitivity, and real-time dynamic imaging, US has been demonstrated as an efficient screening technique for dense breasts in China. 23 In the conventional US images of the 17 lesions, a majority of which showed oval shape (82.4%), parallel orientation (82.4%), well-defined margins (70.6%), and no sonographic calcification (88.2%), which were in line with the results of earlier related reports.24,25 The US presentations closely correspond to the pathohistological features. EPC is typically manifested as cystic-solid masses with solid components lying within the thick-walled cyst. The mass features a papillary protrusion, which is often attached to the capsule wall with a broad base. The 16 lesions in this study exhibited composite masses containing cystic and solid components during US. Additionally, one or more focal papillary-like solid structures from the wall of the capsule could be observed, protruding into the lumen of the capsule. Occasionally, solid hypoechoic without cystic components also were observed in EPC and their pathological types were predominantly confirmed to be non-pure ones, 26 aligning with the pathological findings of only one solid hypoechoic lesion in this study.
Although EPC has a variety of manifestations, interestingly, in this study we found that EPC has a unique US characteristic. Based on the proportions and distribution of solid and cystic components within the lesion, we tried to propose EPC to be categorized into four types: solid mass, solid mass with a few cystic components, cyst with multiple peripheral solid components, cyst with a solitary peripheral solid component (Figure 3). This is the first-time image typing of EPC has been proposed. Besides, the manifestation of glossy margin correlates with the microscopic visualization of a thick-wall fibrous membrane and the expansive growth pattern of the tumor. When cancer cells appear outside the fibrous coating and infiltrate into the surrounding tissues, they appear on US as having blurred margins. 2 lesions in this study showed burred and angular margins and were pathologically confirmed to be EPC in conjunction with invasive carcinoma, which was consistent with the literature report. 26
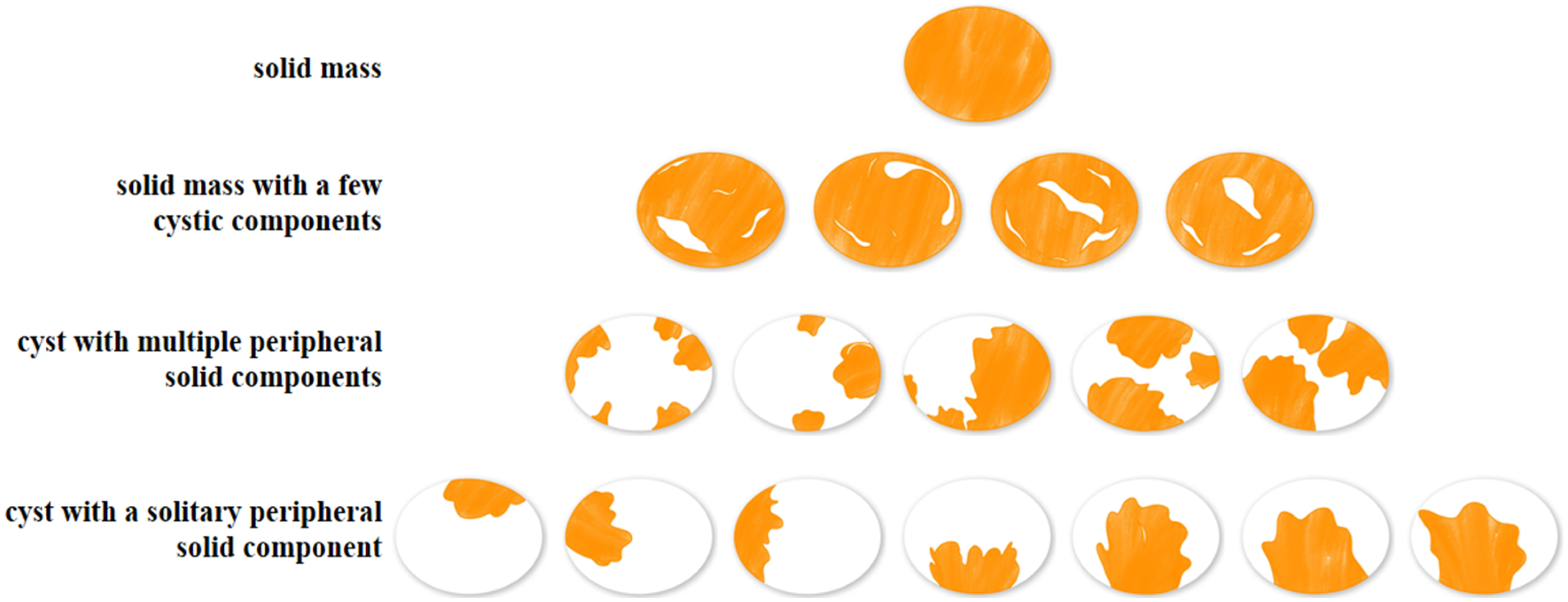
According to the proportion and distribution characteristics of cystic and solid components within the lesion, the images of EPC were divided into four types: solid mass, solid mass with a few cystic components, cyst with multiple peripheral solid components, cyst with a solitary peripheral solid component. Here shows the schematic structure of the four types.
US imaging is based on pathology, and echoes within and behind the lesion are closely related to the internal structure of the tumor, in addition to its cystic component. High content of cancerous tissue within the lesion, with fewer acoustic interfaces and good transmittance, shows low internal echo and enhanced posterior echo. 27 During the study, all 16 complex cystic and solid lesions demonstrated posterior echo enhancement. However, the only solid hypoechoic lesion that was identified to be combined with invasive carcinoma displayed posterior echo shadowing. This phenomenon could be linked to various factors, including increased collagen fiber tissue components produced by the invasive carcinoma cells and its disordered arrangement. Additionally, calcification presented on the sonograms of 2 lesions accompanied by invasive carcinoma in this study may be attributed to the fact that high-grade tumors are more metabolically active, which can cause local malnutrition due to their rapid growth. Then calcium and phosphorus within cancer cells can lead to the deposition of calcium salts, resulting in the formation of calcification. 28
Moreover, neovascularization is a crucial feature of breast malignancy and is the pathological foundation for the abnormal proliferation and invasion of cancer cells. 29 The literature reported that color doppler blood flow signals serve as a characteristic indicator to identify benign and malignant breast tumors 30 and arterial spectra can be detected in most malignant lesions. 31 In this investigation, CDFI indicated that the lesions primarily showed Adler grade 3 blood flow (70.6%), internal and marginal blood flow (88.2%) with high RI of arterial blood flow spectrum (94.1%), aligning with previously published findings.31,32 Microscopically, the lesions contain abundant fibrovascular axes, corresponding to the rich trophoblastic vessels seen on US. The reason for the abundant high RI of blood flow in the lesion is that the vascular endothelial growth factor (VEGF) secreted by cancer cells stimulates the generation of new capillaries, which results in an abundant blood supply. 33 Then the invasion of tumor cells into the blood vessels can form cancer thrombi, and the blood vessels are tortuous and irregular, resulting in poor venous return and high resistance.
There are limited studies about US manifestations of EPC and even fewer reports focusing on characteristics of CEUS, the majority of which are in the form of case reports.9,10 The enhancement patterns of all 17 lesions showed irregular internal solid components with centripetal hyperenhancement (Figure 4), in keeping with the findings that malignant breast lesions tend to display high-intensity perfusion. 34 The EPC demonstrates an expansive growth pattern instead of the traditional crab-foot-like infiltrative growth and is encased by fibrous membranes. As a result, the enhancement size of solid components within the lesions was comparable to that observed pre-enhancement. The study identified one solid hypoechoic lesion with a sharply different contrasting pattern, exhibiting centripetal inhomogeneous hyper-enhancement. After enhancement, the solid components within the lesions appeared irregular in shape, with an unclear edge that showed an enlargement in area compared to B-mode US. Furthermore, there was a filling defect presentation, consistent with typical CEUS manifestations of breast malignant tumors. The reason for this is that the rapid growth of tissue, coupled with inadequate nutrient and blood supply may result in varying degrees of necrosis in the internal tissues. According to the features of CEUS, the BI-RADS assessments of 9 lesions were upgraded, of which 2 lesions were upgraded from BI-RADS 4A to BI-RADS 4B and 2 lesions were upgraded from BI-RADS 4A to BI-RADS 4C. Eventually, the postoperative pathological examination validated that the upgrading of these lesions was correct, which indicates that CEUS helps improve diagnostic accuracy and avoid misdiagnosis or omissions.
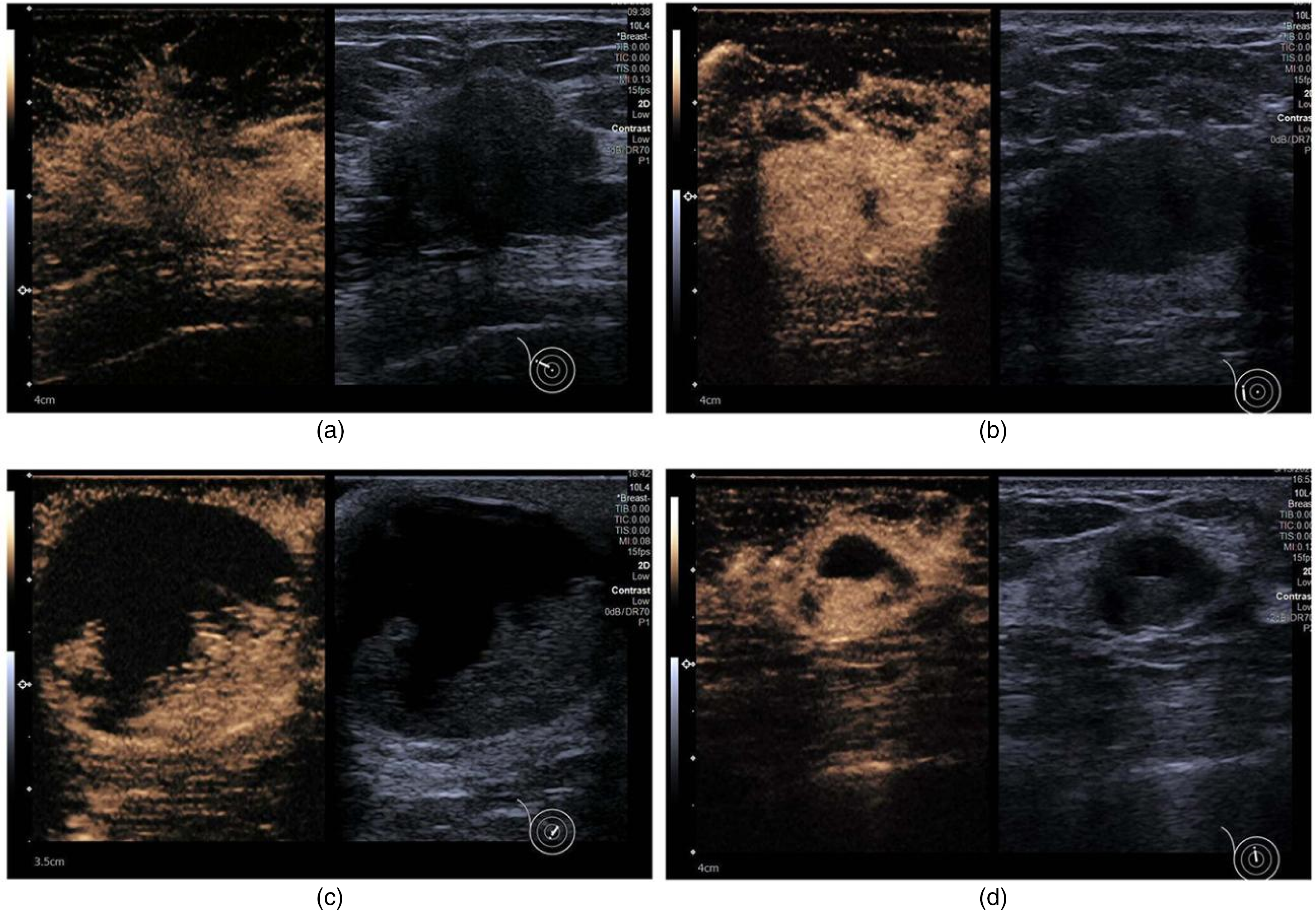
(a) An irregular hypoechoic solid mass was showed on B-mode US. After enhancement, the lesion appeared irregular in shape, with an unclear edge that showed an enlargement in area compared to B-mode US. (b) A solid mass with a few cystic components showed homogeneous enhancement with well-defined margin. (c) CEUS showed the solid components of the lesion were distributed in a scattered pattern. (d) CEUS showed the solid component with eccentric and localized distribution within the lesion.
Core-needle biopsy is presently a reliable approach for diagnosing breast tumors before surgery. 35 Accurately localizing the solid portion of the lesion and ensuring sufficient sampling of the specimen are dependable guarantees for diagnosing EPC via preoperative puncture biopsy. EPC grows expansively within dilated catheters, and it behaves similarly to complex cysts on US. Further, solid structures within the lesion are prone to spontaneous hemorrhage due to their rich vascularity. 36 When the lesion bleeds, it results in intracapsular complex echogenicity, which may obscure the solid part of the capsule. 37 This may easily lead to an erroneous diagnosis of breast cysts in conjunction with haemorrhage or haematoma.32,38 Due to these qualities, preoperative diagnosis of EPC may be challenging because of erroneous sampling locations, insufficient cell counts, or unclear pathological features. At this point, CEUS can provide a real-time, dynamic display of the blood perfusion of the lesion and surrounding glands, which allows for clear and accurate identification of solid structures. Thus, real-time guided puncture under CEUS contributes to precise preoperative biopsy.
Until now, there is no consensus on the treatment of EPC, but surgery-based comprehensive treatment models are common in clinical practice. Among them, breast-conserving and simple mastectomy surgeries are frequently used as surgical methods for EPC.39,40 At our research center, 15 patients with EPC received breast-conserving surgery or simple mastectomy. Most of the cases in the study were diffusely positive for ER and PR, negative for Her-2, and negative for myoepithelial markers. 15 hormone-receptor-positive patients underwent endocrine therapy, while only 1 case received chemotherapy. Most of the EPC do not show a high index of Ki-67. Only 1 patient in the study had a high level of Ki-67 expression, and this was pathologically confirmed as EPC with invasive carcinoma. Nevertheless, it has been reported that the discrepancy in 10-year overall survival between patients with EPC alone and with EPC combined with invasive carcinoma was not significant. 41 Furthermore, there is an excellent prognosis for patients diagnosed with EPC regardless of whether the tumor is diagnosed as in-situ or invasive and few patients have axillary lymph node involvement.40,41 2 of the patients with axillary lymph node metastasis in the study were pathologically confirmed to be EPC with invasive carcinoma, which was consistent with the results of the previous study. 21 None of the follow-up patients in this study experienced local recurrence, distant metastasis, or death, and displayed a sound clinical prognosis, which was basically in line with the literature.40,41
However, there were some limitations in this study as it is a single-center retrospective study. Firstly, the analyzed US images were obtained from three distinct types of instruments, which might have affected the consistency and accuracy of the results. Secondly, the number of cases included in the study was small, particularly with regards to solid mass. Finally, further investigation is necessary to determine the diagnostic value of US elastography for this disease. Consequently, we look forward to conducting a multicenter prospective study in the future to validate our findings.
Conclusion
In summary, we firstly tried to categorize EPC sonograms into four distinct types, offering clinicians a more visualized and impressive understanding of EPC US imaging. Additionally, a comparative analysis of US performance and pathological features can further enhance physicians’ comprehension of the EPC images. The cystic-solid nature of EPC leads to conventional US presentations similar to benign tumors and makes preoperative diagnosis by core-needle biopsy more difficult. However, the application of CEUS to discern cystic and solid components of EPC and to correct BI-RADS assessment classification, provides clinicians with a more reliable range of malignant risks. This approach decreases the frequency of unnecessary missed diagnoses and avoids secondary surgery after minimally invasive procedures. Finally, the combination of age, clinical presentation, US, and CEUS manifestations provides suggestive evidence for diagnosing this disease. Meanwhile, clinicians can also formulate the best treatment plan based on the preoperative assessment of the malignant risk.
Footnotes
Acknowledgments
This work was supported by the Science and Technology Bureau Project of Zhanjiang [Grant No. 2020A01036], the “Three-Aspected Education” Special Project of the First Clinical Medical College of Guangdong Medical University, and the Graduate Teaching Reform Research Project of the Affiliated Hospital of Guangdong Medical University.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.