
Abstract
Physical activity combined with low temperatures can improve physical fitness, the efficiency of many organ systems, and mental well-being. The study investigated the effects of single sessions of various forms of physical activity (running, walking, lying down) conducted in a thermal climate chamber at a temperature of −5°C on blood rheological properties in young men. The participants (21 men aged 22 years), when performing the activities, were fasting and hydrated with 500 ml of water. Erythrocyte deformability increased at a shear stress of 4.24 Pa in the walking group and in the jogging group between the measurements before and after the activity. An increase in erythrocyte deformability was also recorded at a shear stress of 8.23 Pa, 15.95 Pa, 30.94 Pa, and 60.00 Pa after running, walking, and lying down compared with the blood indicators measured before these activities. Statistically significant changes were reported for aggregation index in the jogging group after the activity. The increase in erythrocyte deformability at higher shear stress levels may constitute a mechanism to facilitate blood flow in men exposed to a temperature of −5°C. The study revealed specific differences that can be used to combine cold therapy with physical exercise.
Keywords
Introduction
Physical activity combined with low temperatures (cold water immersion, cryotherapy) improves physical fitness, the efficiency of many organ systems, as well as mental well-being. 1 One of the key factors in maintaining good physical and mental health is an appropriate level of physical activity. Moderate exertion is defined by a heart rate of 45–70% of the maximum value during physical activity, while vigorous exertion corresponds to a heart rate of 70–85% of the maximum value. The blood of endurance-trained athletes is characterized by lower density compared with non-athletes, 2 but it is not known to what extent, from both a health-related and athletic performance perspective, reduced blood viscosity may be beneficial for the body. 3 The favourable effect of physical exercise on cardiovascular health can be attributed to its ability to inhibit cell death pathways. 4 According to Kordi et al., 5 regular physical activity of suitable intensity can influence the metabolism and reduce the risk of such conditions as metabolic syndrome and cardiovascular diseases. Physical activity can reduce the process of ferroptosis by its effect on the endocrine system, the antioxidant system, inflammatory mechanisms, and a change in cellular reserves. Aerobic training at an appropriate intensity is recommended for the elderly to decrease cell death and ferroptosis. 5 In turn, in patients with coronary artery bypass grafting and with cardiovascular diseases, exercise, together with other clinical therapies, is considered an effective non-pharmacological preventive method. 6 Physical training was reported to increase the mRNA expression level of P2Y receptors in Wistar Kyoto rats and in spontaneously hypertensive rats that were randomly assigned to sedentary and training groups. This finding implies that physical training can reduce hypertension in spontaneously hypertensive rats by enhancing the purinergic relaxation response. 7
Running for the mere of 5–10 min a day at a speed not exceeding 10 km/h is associated with a significant reduction in the risk of death and cardiovascular diseases. 8 Physical activity lasting for less than 1 h per week brings about significant benefits to healthy individuals with sedentary lifestyle. 9 Regular exposure to low temperatures and physical exercise positively affects the proper flow of blood through arteries, veins, and capillaries. 1 Combining cold therapy with physical exercise is recommended as it creates favourable conditions for the circulatory system, can reduce skeletal muscle tension, decreases oedema, increases muscle strength, promotes metabolism, improves well-being, accelerates recovery processes, and enhances mobility in treated joints. 10 According to Ivanov, 11 blood rheology is influenced by sports and physical exertion in various ways and degrees. Rheological indicators of blood in individuals of different ages who engage in sports can well characterize the actual extent and direction of changes induced by exercise combined with low temperatures. 12 It is worth emphasizing that regular moderate physical exercise stimulates immune mechanisms when combined with low temperatures. Regular exposure to cold increases tolerance to cold through numerous adaptive mechanisms. 13 Low temperatures exert analgesic and anti-oedematous effects, improve circulation, have antioxidant properties, reduce inflammation, and positively affect the functioning of the neuromuscular system.14–17
The aim of the research was to examine the effect of the physical effort factor (running and walking) or the lack of it (lying down) at an air temperature of −5°C. With the temperature factor kept under control, a focus on the exertion factor was possible. Including additional measurements in the analysis under thermoneutral conditions would raise doubts as to which factor actually caused the effect: temperature or physical effort. In addition, comparing so many variances involving the obtained means would have made it difficult to identify statistically significant differences. The measurements were limited to three groups at the same low air temperature because the authors believed that it was precisely this type of research that was lacking. The impact of different types of physical activity is well known; what remains less clear, however, is the effects of varying the exertion level at low air temperatures.
Materials and methods
Characteristics of the research group
The study group (n = 21) consisted of young men (aged 22 years), third-year physiotherapy students at the University of Physical Culture in Krakow (Poland), who did not practise sport professionally.
The average body mass of the participants was 79.00 ± 3.87 kg in the jogging group, 75.29 ± 10.67 kg in the walking group, and 81.29 ± 9.41 kg in the group lying down. The average height of the individuals equalled 184.00 ± 3.06 cm in the jogging group, 176.57 ± 7.09 cm in the walking group, and 180.86 ± 5.08 cm in the group lying down.
Inclusion criteria: The respondents were students of the University of Physical Culture in Krakow, Poland, performing mental work and physical activity typical of students majoring in physiotherapy. The subjects were included in the research program after obtaining a physician's consent and after a physiotherapist consultation.
Exclusion criteria: Cardiac arrhythmia, cancer, diabetes. Additionally, the participants were excluded if they used beta-blockers or anti-depressants, smoked or chewed tobacco products, or drank more than two alcoholic beverages a day.
Grouping
The individuals involved in the study were randomly divided into three in groups with parallel design:
group No. 1: running at an air temperature of −5°C (n = 7); group No. 2: walking at an air temperature of −5°C (n = 7); group No. 3: lying down at an air temperature of −5°C (n = 7).
Intervention
The study was conducted with the participants fasting, after hydration with 500 ml of water. They performed single instances of different forms of physical activity at an air temperature of −5°C obtained in the thermal climate chamber of the Laboratory for Climate Technology Research and Heavy Duty Machines, Faculty of Mechanical Engineering of Cracow University of Technology.
Group No. 1 performed a 5-min stationary warm-up before entering the chamber, followed by 10 min of running inside the chamber in thermal clothing (gradually increasing the intensity from jogging to running, with an effort level allowing continuous conversation). The Borg scale at the level of 2–3 was applied as a tool to subjectively assess the effort intensity. Group No. 2 performed a 5-min stationary warm-up before entering the chamber in thermal clothing, followed by 10 min of walking inside the chamber. The Borg scale at the level of 2–3 was applied as a tool to subjectively assess the effort intensity. Group No. 3 performed a 5-min stationary warm-up in place before entering the chamber, followed by 10 min of lying on a sleeping mat in a sleeping bag inside the chamber (in thermal clothing).
Research method
Blood samples were collected from the subjects before entering the thermal climate chamber and after leaving it (fasting, from the antecubital vein, in the amount of 10 ml, into Vacuette EDTA K2 tubes) by a qualified nurse. Morphological and rheological indicators were determined in the tested blood at the Blood Physiology Laboratory of the Central Research and Development Laboratory, University of Physical Culture in Krakow. The study was approved by the Ethics Committee of the Regional Medical Chamber in Krakow, Poland (approval No.: 171/KBL/OIL/2023) and followed the tenets of the Declaration of Helsinki.
Morphological and rheological assessments
Morphological analyses
The blood count indicators included: red blood cell count (RBC) [106/mm3], haemoglobin (HGB) [g/dl], haematocrit (HCT) [%], mean corpuscular haemoglobin (MCH) [pg], mean corpuscular haemoglobin concentration (MCHC) [g/dl], mean corpuscular volume (MCV) [μm3], red blood cell distribution width (RDW) [%], white blood cell count (WBC) [103/mm3], lymphocyte count (%LYM), monocyte count (%MON), granulocyte count (%GRA), platelet count (PLT) [103/mm3], mean platelet volume (MPV) [μm3], platelet distribution width (PDW) [%], plateletcrit (PCT) [%]. The indicator markings were performed with an ABX Micros 60 device (HORIBA ABX SAS, Montpellier, France).
Rheological assessments
The blood rheology parameters, such as erythrocyte aggregation index (AI) [%], amplitude and total extent of aggregation (AMP) [arbitrary units], half-time of total erythrocyte aggregation (T1/2) [s], and deformability (elongation index, EI) were evaluated with the Laser-Assisted Optical Rotational Red Cell Analyzer (Lorrca) (MaxSis Lorrca®, RR Mechatronics, the Netherlands) by using the method described by Hardeman et al. 18 Mean EI values were determined at the shear stress values of 0.30 Pa, 0.58 Pa, 1.13 Pa, 2.19 Pa, 4.24 Pa, 8.23 Pa, 15.95 Pa, 30.94 Pa, and 60.00 Pa, with the automatic analysis function of the Lorrca system, which allows assessing erythrocyte deformability as a function of shear stress and erythrocyte aggregation. Fibrinogen determinations [g/l] were performed with the use of a CHROM-7 coagulometer.
Research location
The thermal climate chamber possesses accreditation certificate No. AB 1678 issued by the Polish Centre for Accreditation and meets the requirements of the PN-EN ISO/IEC 17025:2005 standard. The Laboratory for Climate Technology Research and Heavy Duty Machines is a research centre accredited in the field of defence and security by the Minister of National Defence (accreditation No.: 55/MON/2018).
Statistical analysis
One-way analysis of variance (ANOVA) with repeated measures served to assess differences between the study groups. Multiple comparisons were performed with the Bonferroni test. Cohen's d coefficient was applied to provide a standardized difference in the measurements before and after the intervention. The normality of the distribution was assessed with the Shapiro-Wilk test. Homogeneity of variance was checked by using Levene's test. Differences between means were considered significant at p ≤ 0.05. The analyses were performed with the Statistica 13 software package (StatSoft Polska).
Results
The results of the study are presented in Tables 1 to 3.
Blood morphological parameters in the investigated groups presented as mean and standard deviation in measurements before and after the intervention with the consideration of the significance test probability p-values.
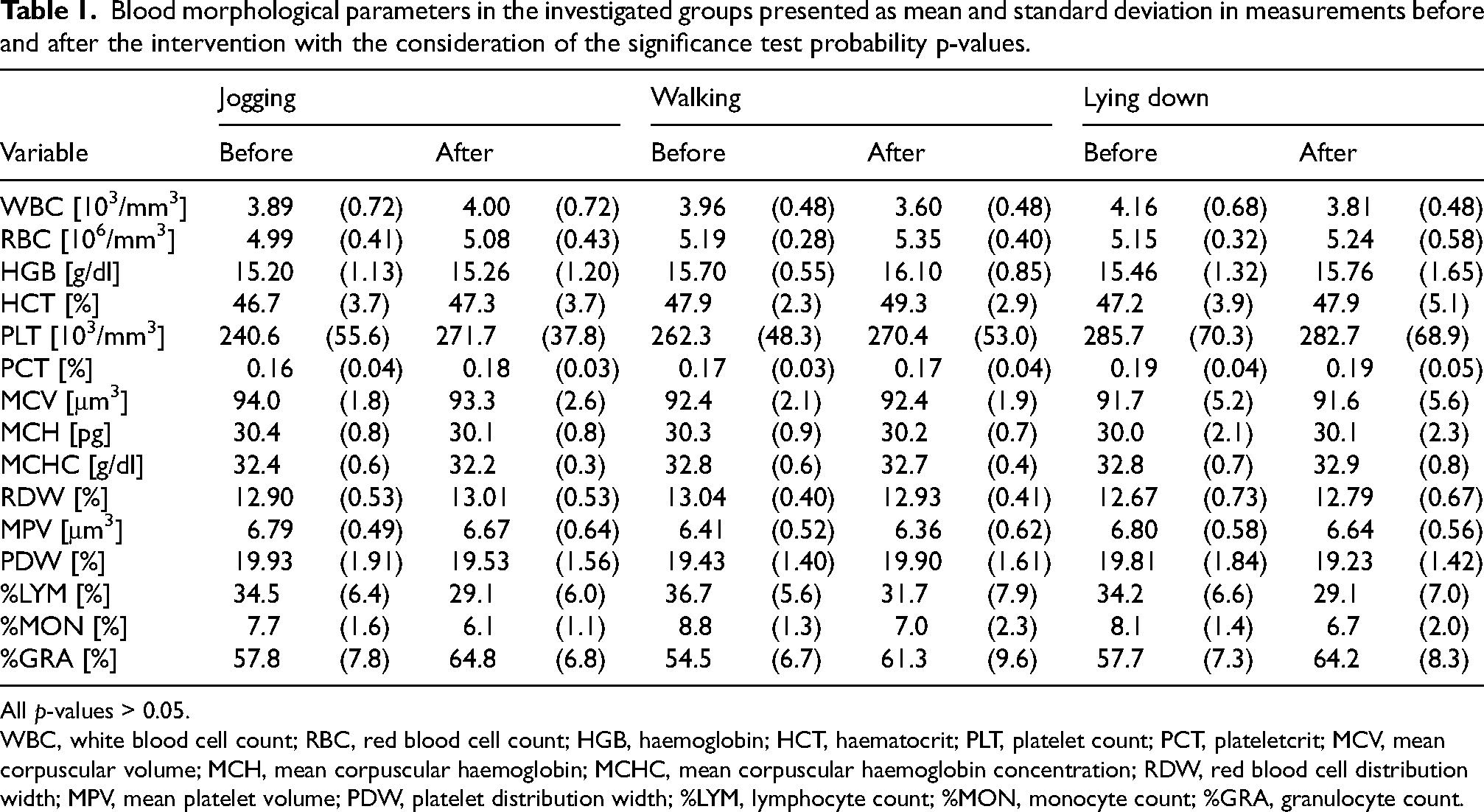
All p-values > 0.05.
WBC, white blood cell count; RBC, red blood cell count; HGB, haemoglobin; HCT, haematocrit; PLT, platelet count; PCT, plateletcrit; MCV, mean corpuscular volume; MCH, mean corpuscular haemoglobin; MCHC, mean corpuscular haemoglobin concentration; RDW, red blood cell distribution width; MPV, mean platelet volume; PDW, platelet distribution width; %LYM, lymphocyte count; %MON, monocyte count; %GRA, granulocyte count.
Blood rheological parameters in the investigated groups presented as mean and standard deviation in measurements before and after the intervention with the consideration of the significance test probability p-values.
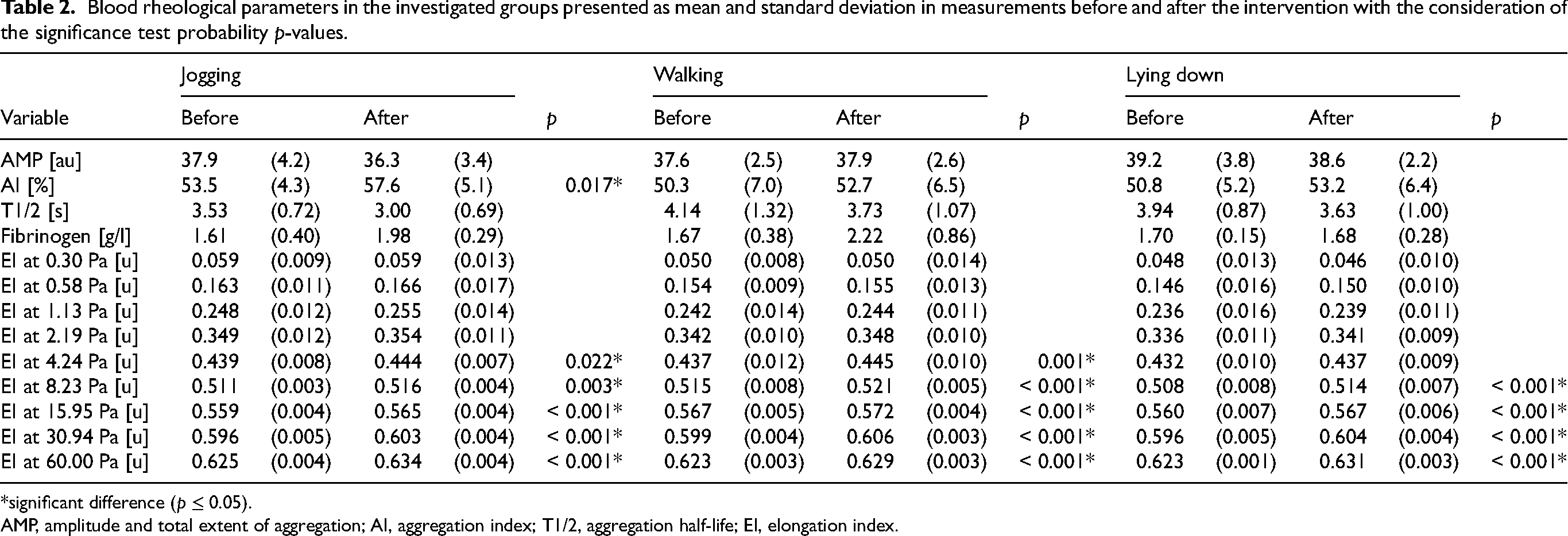
*significant difference (p ≤ 0.05).
AMP, amplitude and total extent of aggregation; AI, aggregation index; T1/2, aggregation half-life; EI, elongation index.
Cohen's coefficient.
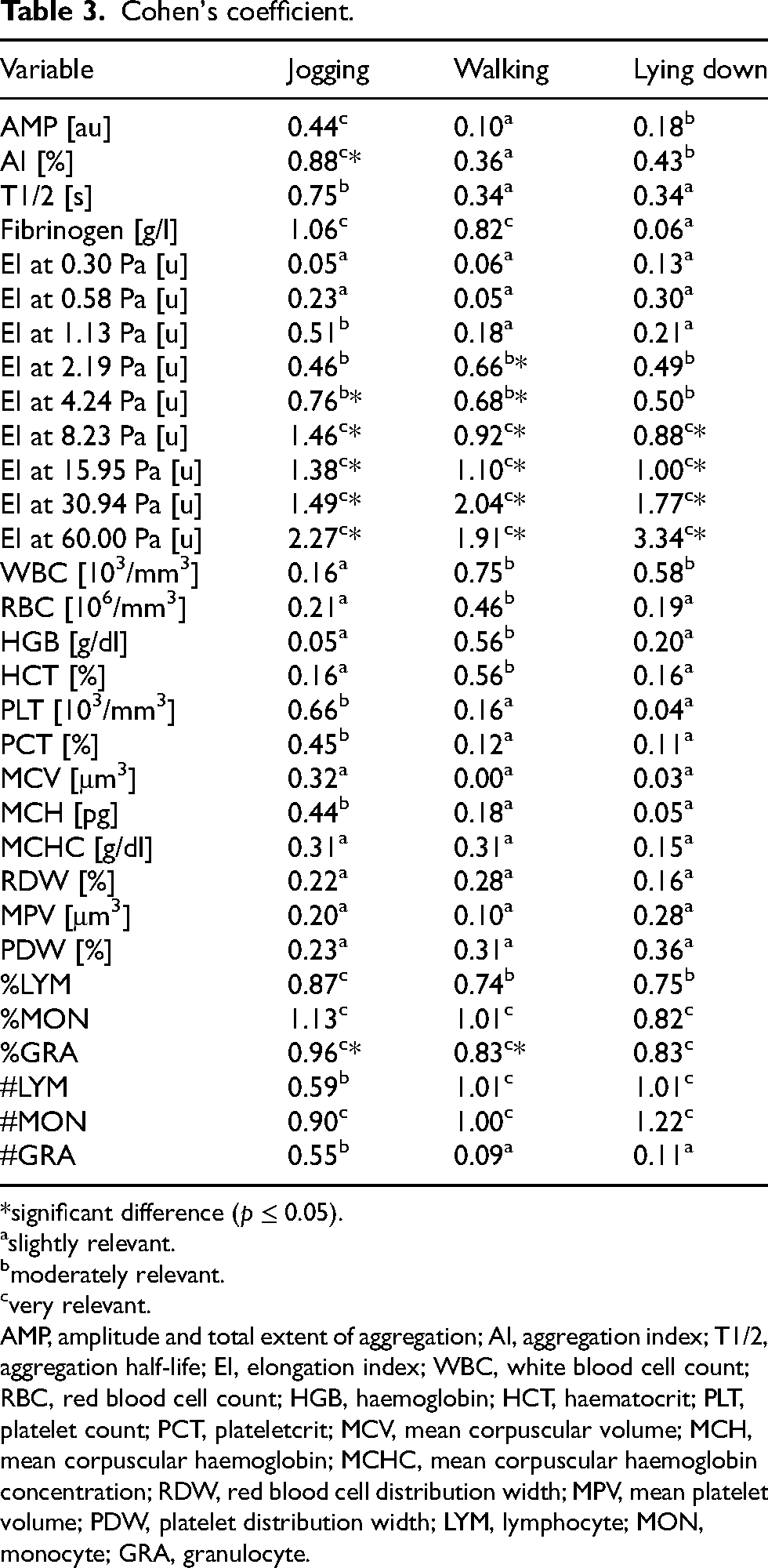
significant difference (p ≤ 0.05).
slightly relevant.
moderately relevant.
very relevant.
AMP, amplitude and total extent of aggregation; AI, aggregation index; T1/2, aggregation half-life; EI, elongation index; WBC, white blood cell count; RBC, red blood cell count; HGB, haemoglobin; HCT, haematocrit; PLT, platelet count; PCT, plateletcrit; MCV, mean corpuscular volume; MCH, mean corpuscular haemoglobin; MCHC, mean corpuscular haemoglobin concentration; RDW, red blood cell distribution width; MPV, mean platelet volume; PDW, platelet distribution width; LYM, lymphocyte; MON, monocyte; GRA, granulocyte.
Discussion
The interaction of exercise and cold has been scarcely investigated in the literature, particularly in the context of the rheological properties of blood. Low temperature is not an obstacle to physical activity. 1 In the present study, the intervention applied in the walking group in the form of physical effort at a temperature of −5°C best demonstrates the adaptation in young men in terms of blood rheological properties, as evidenced by a significant increase in red blood cell deformability.
An increase in red blood cell deformability was observed in the thermal climate chamber only at a shear stress of 4.24 Pa in group No. 2 (walking) between the measurements before and after the intervention and at a shear stress of 4.24 Pa in group No. 1 (jogging) between the measurements before and after the intervention. For each exercise, an increase in red blood cell deformability was also recorded in the chamber at −5°C at a shear stress of 8.23 Pa, 15.95 Pa, 30.94 Pa, and 60.00 Pa after running, walking, and lying down, compared with the blood indicators obtained before these forms of exercise. Statistically significant changes were reported for AI in group No. 1 (jogging) between before and after the exercise but the difference was not huge, with AI values remaining normal.
The most usual haemorheological change is an increase in the overall blood viscosity, determined by the haematocrit, plasma viscosity, and the rheological behaviour of the erythrocytes. 19 The haematocrit reflects both the number of red blood cells and their volume (MCV). When the volume of blood cells decreases, the haematocrit also decreases; with increasing blood cell volume, the haematocrit increases. The haematocrit value rises with an increase in the number of red blood cells or a decrease in plasma volume, which occurs in dehydration. Red blood cells, which lack nuclei, have a characteristic biconcave disc shape with an average diameter of 7.7 ± 0.7 μm and a thickness of about 2.8 ± 0.5 μm at the thickest point and about 1.4 ± 0.5 μm in the centre. 20 It is likely that increasing red blood cell deformability at higher shear stress values serves as a protective mechanism facilitating blood flow in individuals exposed to an air temperature of −5°C. According to Harrison, 21 body position during physical exercise can also alter the rheological properties of blood. Haemoconcentration, and thus a decrease in plasma volume, occurs during exercise performed in a standing or seated position, as well as when changing from a seated to a standing position. 21 Short-term exercise most likely contributes to the development of haemoconcentration, which results from the movement of fluids from the intravascular space to the tissues of working muscles. According to Tikhomirova, 22 proper hydration is important, as a lack of water leads to a progressive decrease in the fluidity of blood and plasma. A single exercise most often results in a decrease in EI,23–25 but there are studies that support the present research finding of increased deformability after a single effort.26–28 The intensity and duration of exercise may determine changes in erythrocyte deformability. The reason for the increase in deformability after exercise may lie in early rehydration, as well as in increased blood cell volume and decreased mean cell haemoglobin concentration.27,29 Haemorheological effects of exercise can be short-term effects, indicating excessive viscosity, mainly caused by fluid shifts and changes in red blood cell deformability and aggregation. 19 Moreover, a physiological increase in leukocyte count is typically observed after physical exercise and stress. 19 Granulocyte activation may play a role in the haemorheological effects of strenuous exercise as an inflammatory response. 19
In turn, group No. 1 (jogging), despite the increase in red blood cell deformability, exhibited an increase in erythrocyte aggregation, but the difference was not huge, with AI values remaining normal.
If one compares these two forms of physical effort in a thermal climate chamber at a temperature of −5°C, it is physical activity No. 2 (walking) that produces more favourable effects, as increased EI was already observed with the initial forces at a shear stress of 4.24 Pa to 60.00 Pa, with no changes in the remaining haemorheological blood indicators. The phenomenon of red blood cell deformability plays an important role in the flow of blood cells through capillaries, with a diameter even twice smaller than that of erythrocytes. 30 For example, Freitas Leal et al. 31 proved that a walk (30–50 km) of moderate intensity practised for four consecutive days, was sufficient to improve the functional activity of erythrocytes (higher deformability and reduced aggregability). Increased deformability of erythrocytes is hypothesized to significantly contribute to athletes’ good ‘sports fitness'. 32
In group No. 3 (lying down), in the measurements before and after the intervention, the smallest EI increase was reported at a shear stress of 8.23 Pa to 60.00 Pa, which implies that in the group with no effort, exposed only to a low air temperature of −5°C, the effect of low temperature alone exerted the least influence on the haemorheological properties of blood.
Further investigation of the rheological properties of blood in response to single forms of physical exercise in low temperatures may reveal additional specific differences that could be utilized by combining cold therapy with physical exercise. In summary, on the basis of the available literature and the presented research findings, it can be concluded that single forms of physical exercise at a temperature of −5°C are safe, with no pathological changes observed.
Practical applications
The results of the experiment demonstrate the effectiveness of walking in cold air at a temperature of −5°C, which can be utilized by coaches and athletes in training, owing to an enhancement of blood haemorheological properties.
Conclusions
The intervention applied among the subjects in the form of physical effort at a temperature of −5°C in the walking group best demonstrates the adaptation in young men in terms of blood rheological properties, as evidenced by a significant increase in red blood cell deformability.
The applied intervention in the form of jogging at an air temperature of −5°C, despite an increase in erythrocyte deformability, evidenced a rise in erythrocyte aggregation, but within normal limits.
The sole influence of cold air at a temperature of −5°C in the group lying down that stayed in a thermal climate chamber did not result in a significant improvement in blood rheological properties among the young men.
Study limitations
This study is not without limitations. One of the limitations is the lack of heart rate, blood pressure, or maximal oxygen uptake measurements. Also, no comparison with thermoneutral conditions was performed. An important aspect that may have influenced the results is the relatively small sample size. The obtained results are significant for determining safety in the thermal climate chamber at an air temperature of −5°C; therefore, the research should be continued with larger and more diverse groups of individuals.
Footnotes
Acknowledgments
A.T. wishes to thank Professor Janusz Pobędza for the opportunity to complete an internship at the Laboratory for Climate Technology Research and Heavy Duty Machines, Faculty of Mechanical Engineering, Cracow University of Technology, which contributed to the creation of this manuscript.
Author contributions
Conceptualization, A.T., K.R., and J.P.; Methodology, A.T., K.R., and J.P.; Formal analysis, K.R.; Data curation, A.T., K.R., J.P., Z.D., A.C., J.L., M.Ś., and A.U.; Writing—original draft, A.T.; Writing—review & editing, A.T.; Supervision, A.T., J.P., and J.M.; Project administration, A.T.; Funding acquisition, A.T. and P.M. All authors have read and agreed to the published version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication was financed within the project number 365/BS/INP/2024.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Institutional review board statement
The study was approved by the Ethics Committee of the Regional Medical Chamber in Krakow, Poland (approval No.: 171/KBL/OIL/2023) and followed the tenets of the Declaration of Helsinki.
Informed consent statement
Informed consent was obtained from all subjects involved in the study.