
Abstract
Oxygen-gradient ektacytometry (oxygenscan) has been recently used in the context of sickle cell disease (SCD) to determine the ability of red blood cells (RBCs) to deform in normoxia and during deoxygenation. While several studies focused on the determinants of oxygenscan parameters in the homozygous form of SCD (i.e., HbSS), very few studies focused on hemoglobin SC disease (HbSC). Oxygenscan parameters were compared between HbSS (N = 304) and HbSC (N = 58) patients, with or without hydroxyurea (HU). RBC deformability measured in normoxia or at low oxygen level was lower in HbSS patients without HU compared to HbSS patients with HU and HbSC patients with or without HU. The propensity of RBCs to sickle during deoxygenation was greater in HbSS than in HbSC patients. Although no significant impact of HU was observed on RBC deformability/sickling in HbSC patients, those with HU had lower blood viscosity. The ability of RBC to recover their maximum deformability after a deoxygenation/reoxygenation cycle was lower in HbSC compared to HbSS patients. Finally, oxygenscan parameters and routine hematological parameters correlated differently in HbSS and HbSC patients. Our study showed difference in oxygenscan parameters between HbSS and HbSC individuals that could partly explain the difference in the clinical expression of SCD.
Introduction
Oxygen-gradient ektacytometry (oxygenscan) has been recently used in the context of sickle cell disease (SCD) to determine the ability of red blood cells (RBCs) to deform in normoxia and during deoxygenation. It allows the determination of maximal RBC deformability in normoxia (EImax), minimum RBC deformability (EImin) reached at low oxygen partial pressure (pO2) and the propensity of RBCs to sickle during deoxygenation (i.e., the pO2 at which RBCs start to sickle, called the Point of Sickling (PoS)). Although the clinical interest of these biomarkers is still under debate,1,2 several studies reported associations with clinical severity in patients with the homozygous form of SCD (i.e., sickle cell anemia or HbSS).3–6
Oxygenscan parameters have also been measured to investigate the effects of various treatments. Since exchange transfusion decreases the relative amount of RBCs containing abnormal hemoglobin and increases the relative amount of normal RBCs into the blood circulation, this treatment results in a decrease of PoS and an increase of both EImin and EImax in HbSS patients.4,6 Hydroxyurea (HU), a drug that promotes the production of fetal hemoglobin (HbF), has also been reported to affect oxygenscan parameters with PoS decreasing and EImin and EImax increasing 3 months after the beginning of treatment in HbSS patients.6,7 Chonat et al. 8 investigated the effects of voxelotor on RBC rheology in HbSS patients and observed a decrease of PoS and an increase of EImin and EImax after 48 weeks of treatment, which led to a reduction of hemolysis and a rise in hemoglobin concentration. The effects of pyruvate kinase activators on RBCs have also been investigated both in-vivo and in-vitro. It was shown that these molecules, by increasing adenosine triphosphate (ATP) and decreasing 2,3-diphosphoglycerate levels, decreased PoS and increased EImin and EImax in HbSS individuals.9–12
Very few studies investigated oxygenscan parameters in patients with sickle cell-hemoglobin C disorder (HbSC), another frequent form of SCD. Patients with HbSC have milder anemia than HbSS individuals and are characterized by higher blood viscosity, which contributes to the occurrence of several clinical complications.13,14 The presence of both HbS and HbC into RBCs affect their rheological properties, with deformability being reduced compared to normal RBCs. 15 Boisson et al. 4 compared small groups of HbSS and HbSC individuals and found higher PoS and lower EImin and EImax in the former group. Joly et al. 16 recently reported that HbS percentage and mean corpuscular hemoglobin concentration (MCHC) are key regulators of the PoS in HbSS individuals but no study focused on the determinants of PoS, as well as of the other oxygenscan parameters, in HbSC patients. The aim of the present study was to compare oxygenscan parameters between HbSS and HbSC patients and to test the associations with several routine hematological parameters. Since HU may impact on HbF, mean cell volume (MCV) and MCHC, patients treated with HU were separated from those without HU in the statistical comparisons.
Material and methods
Participants
A group of 362 patients with SCD (304 HbSS: 27.4 ± 13.6 yrs, 152 males, 152 females, 222 treated by HU; 58 HbSC: 34.2 ± 17.3 yrs, 26 males, 32 females, 15 treated by HU) followed by the Sickle Cell Centre of Lyon were included in the present study. All patients were at steady-state: no transfusion and no acute complication in the last 3 months. Patients under HU treatment received their medication since at least 3 months. Blood was sampled in EDTA tubes to perform hematological and hemorheological measurements. The study was conducted in accordance with the guidelines set by the Declaration of Helsinki and was approved by the Regional Ethics Committees (L14-127).
Hematological and oxygenscan parameters
Hemoglobin concentration (Hb), hematocrit (Hct), MCV and MCHC were determined with a hematology analyzer (Advia, Siemens, Rungis, France). HbS, HbC and HbF levels were measured by capillary electrophoresis (Capillarys 2 FP, Sebia, Lisses, France). Blood viscosity was measured at 225 s−1 with a Brookfield DVT cone-plate viscometer and a CPE-40 cone, as previously described. 17 Ektacytometry was carried out with the laser-assisted optical rotational red cell analyzer (Lorrca, RR Mechatronics, The Netherlands) with the oxygenscan module to measure RBC deformability over an oxygen gradient. A volume of 50 µL of blood, standardized to a fixed RBC count of 200 × 106, was mixed with 5 mL of high viscous (30 cP) Oxy-Iso polyvinylpyrrolidone (PVP) suspension. 18 The suspension was sheared at 30 Pa and 37°C into the Couette system made of glass of the ektacytometer. The oxygen partial pressure (pO2) was gradually decreased from 160 mmHg to 20 mmHg (deoxygenation) and then re-increased to normoxic values.7,18,19 The diffraction pattern was analyzed by the computer, and an elongation index (EI) that reflects RBC deformability was calculated. Several parameters were derived: (1) EImax, the RBC deformability at normoxia; (2) EImin, the lowest RBC deformability reached upon deoxygenation; (3) point of sickling (PoS), the pO2 at which RBC deformability decreases below 5% of EImax during deoxygenation; (4) Delta-EI, the difference between EImin and EImax and 5) the percentage of recovery, which corresponds to the difference between EImax and the EI value reached after the end of the reoxygenation process. All measurements were standardized as recommended. 18 Since blood storage (24 h or longer) may affect oxygenscan parameters,18,19 all measurements were carried out within 4 h after sampling.
Statistics
Comparisons between the four groups (HbSS patients with HU, HbSS patients without HU, HbSC patients with HU, HbSC patients without HU) were performed using a one-way ANOVA followed by Tukey post-hoc tests when appropriate. A Pearson test was used to test the associations between oxygenscan parameters and the other parameters for HbSS and HbSC patients separately. A p value less than 0.05 was considered as statistically significant. GraphPad Prism (version 8.3) was used for the statistical analyses.
Results
Comparisons of the four groups
Figure 1 shows the results of hematological, blood viscosity and oxygenscan parameters in the four groups. HbF level was higher in HbSS compared to HbSC individuals. HU-treated patients had higher HbF than untreated patients in the HbSS genotype but not in the HbSC genotype (p ranging from < 0.01 to < 0.0001). Hb was lower in HbSS without HU compared to the 3 other groups (p < 0.0001). HbSS with HU had lower Hb than HbSC with (p < 0.001) and without HU (p < 0.0001). No significant difference in Hb was observed between HbSC with or without HU. Blood viscosity was not different between HbSS patients with HU and those without. HbSC individuals with and without HU had greater blood viscosity than HbSS patients without HU (p < 0.05 and p < 0.0001, respectively). HbSC patients with HU had lower blood viscosity than HbSC patients without (p < 0.05). EImin of HbSS patients without HU was lower compared to HbSC individuals with and without HU (p < 0.05). HbSC patients with HU had higher EI min than HbSS patients with HU (p < 0.05). No difference was observed between the two HbSC groups for EImin. EImax of HbSS patients without HU was lower compared to HbSS patients with HU (p < 0.0001), HbSC with HU (p < 0.01) and HbSC patients without HU (p < 0.05). No other difference was observed for EImax. PoS was lower in the two HbSC groups (p < 0.05 and p < 0.001) compared to HbSS patients without HU. HbSC patients without HU had lower PoS than HbSS patients with HU (p < 0.05). No PoS difference was observed between HbSS with and without HU, or between HbSC patients with and without HU. Delta-EI of HbSS patients with HU was higher compared to HbSS patients without HU (p < 0.01) and HbSC patients without HU (p < 0.001). No other difference was observed for Delta-EI. The percentage of recovery of EI was systematically lower in HbSC compared to HbSS patients (p ranging from < 0.01 to < 0.0001). No difference in the percentage of recovery was observed between the two HbSC groups while we observed slightly lower values in HbSS patients with HU compared to those without (p < 0.01). MCV of HbSS individuals with HU was higher compared to those without (p < 0.0001) and to the two HbSC groups (p < 0.0001). MCV was not different between the two HbSC groups. MCHC of HbSS patients without HU was lower compared to the three other groups (p ranging between < 0.05 and < 0.0001). HbSS patients with HU had lower MCHC than HbSC patients without HU (p < 0.01). No difference in MCHC was observed between HbSC patients with and without HU.
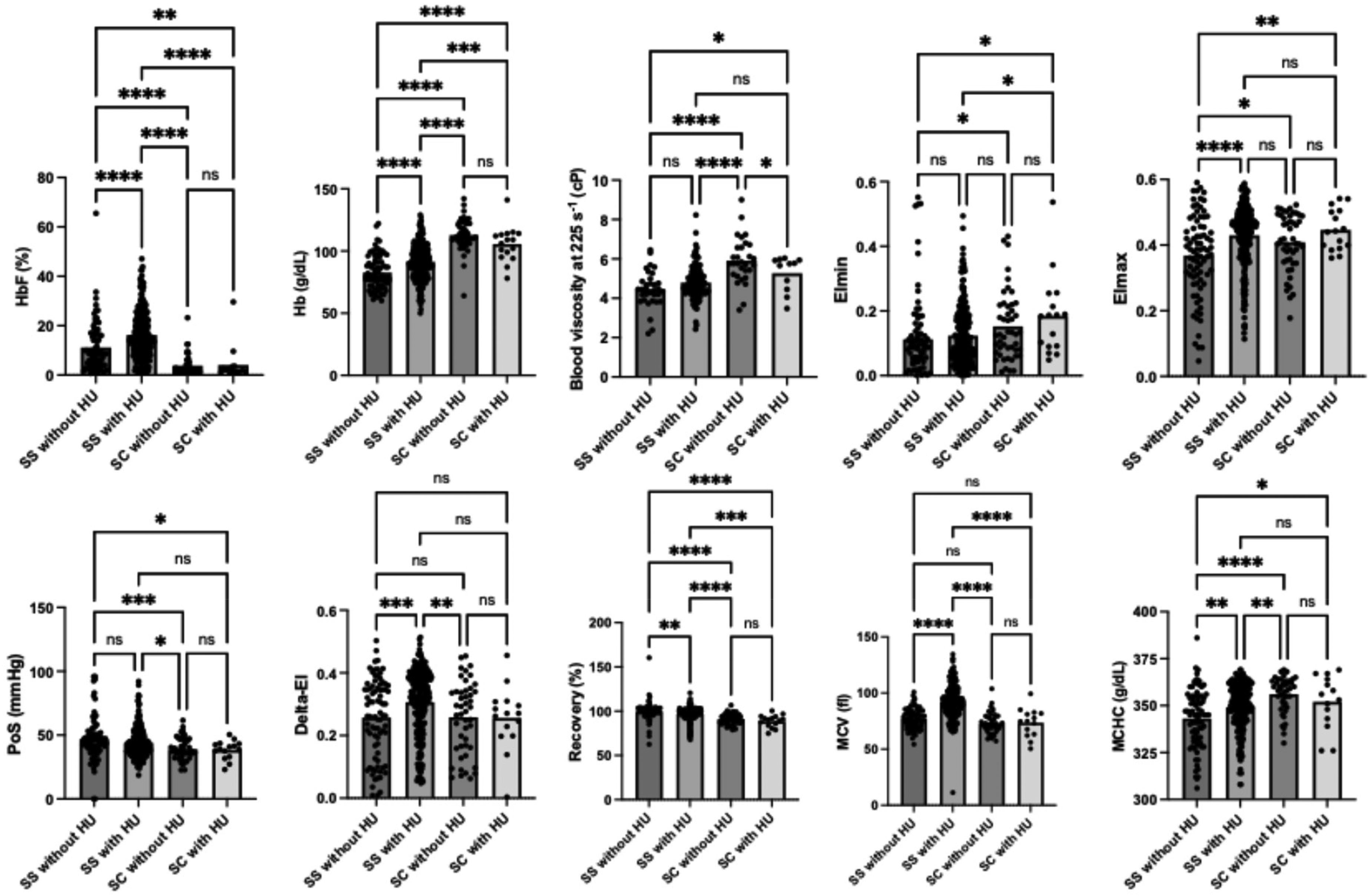
Comparisons of blood viscosity and of the oxygenscan and hematological parameters between HbSS patients with HU, HbSS patients without HU, HbSC patients with HU and HbSC patients without HU. HbF = Fetal hemoglobin, Hb = hemoglobin, EImin = minimum RBC deformability reached at low oxygen partial pressure (pO2), EImax = maximal RBC deformability in normoxia, PoS = point of sickling (i.e., the pO2 at which RBCs start to sickle), Delta-EI = difference between EImin and EImax, recovery = difference between EImax and the EI value reached after the end of the reoxygenation process, MCV = mean cell volume, MCHC = mean corpuscular hemoglobin concentration. Significant difference: *p < 0.05; **p < 0.01; ***p < 0.001; ****p < 0.0001.
Correlations with oxygenscan parameters
Figure 2 shows the correlation matrix (r values) between all parameters for HbSC and HbSS individuals.
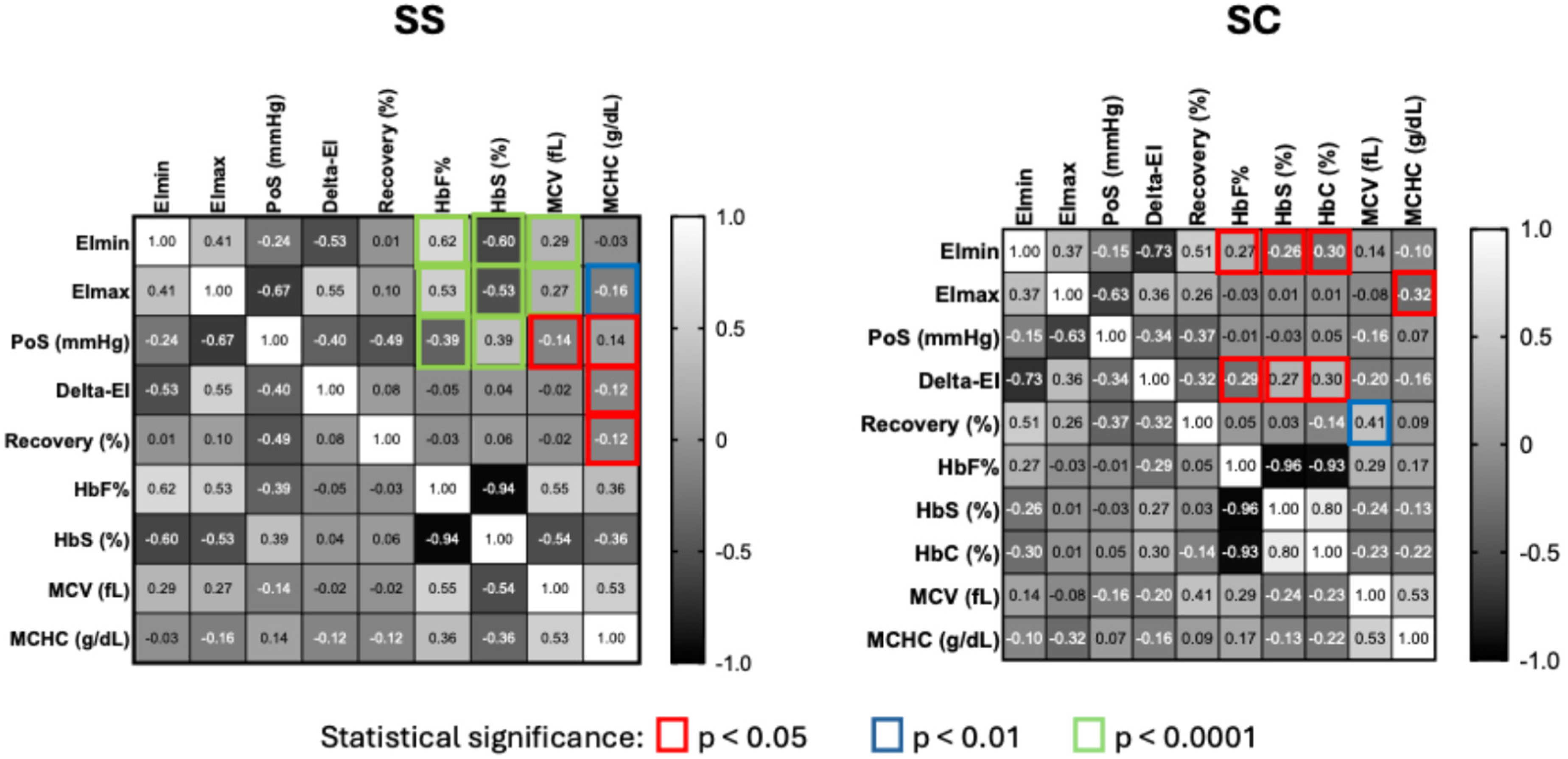
Correlations matrix (r values are indicated) between oxygen gradient ektacytometry and hematological parameters in HbSS (SS) and HbSC (SC) patients. Colored squares indicate the level of statistical significance.
For HbSS patients: 1) EImin did not correlate with MCHC (p = 0.59), positively correlated with HbF (p < 0.0001) and MCV (p < 0.0001), and negatively with HbS (p < 0.0001); 2) EImax positively correlated with HbF (p < 0.0001) and MCV (p < 0.0001), and negatively with HbS (p < 0.0001) and MCHC (p < 0.01); 3) PoS negatively correlated with HbF (p < 0.0001) and MCV (p < 0.05) and positively with HbS (p < 0.0001) and MCHC (p < 0.05); 4) Delta-EI did not correlate with HbF (p = 0.39), HbS (p = 0.51) or MCV (p = 0.70) but correlated negatively with MCHC (p < 0.05); 5) The percentage of recovery negatively correlated with MCHC (p < 0.05) but did not correlate with HbF (0.56), HbS (p = 0.26) or MCV (p = 0.74).
For HbSC patients: 1) EImin was negatively correlated with HbS (p < 0.05) and HbC (p < 0.05), and positively with HbF (p < 0.05) but no correlation was observed with MCV (p = 0.29) or MCHC (p = 0.44); 2) EImax was negatively correlated with MCHC (p < 0.05) but no correlation was found with the other parameters (HbF: p = 0.85; HbS: p = 0.94; HbC: p = 0.96; MCV: p = 0.58); 3) no correlation between PoS and the other parameters was observed (HbF: p = 0.96; HbS: p = 0.81; HbC: p : 0.69; MCV: p = 0.23; MCHC: p = 0.61); 4) Delta-EI negatively correlated with HbF (p < 0.05) and positively with HbS and HbC (p < 0.05), but no correlation was observed with MCV (p = 0.15) or MCHC (p = 0.24); 5) only MCV positively correlated with the percentage of recovery (p < 0.01; HbF: p = 0.70; HbS: p = 0.83; HbC: p = 0.28; MCHC: p = 0.52).
Discussion
The present study mainly showed that 1) RBC deformability measured in normoxia or at low oxygen level was lower in HbSS patients without HU compared to the three other groups, 2) the propensity of RBC to sickle during deoxygenation was greater in HbSS than in HbSC patients, 3) although no significant impact of HU was observed on Hb and RBC deformability/sickling in HbSC patients, those with HU had lower blood viscosity, 4) the percentage of RBC deformability recovery during reoxygenation was lower in HbSC compared to HbSS patients, 5) oxygenscan parameters correlated differently with HbS, HbC, HbF, MCHC or MCV in HbSS and HbSC patients.
As shown in our study, HbSC patients are usually marked by milder anemia than HbSS patients, leading to chronic blood hyperviscosity, which plays a major role in the occurrence of chronic organ complications such as retinopathy, otologic disorders or osteonecrosis.13,14,20 Although no difference in Hb level was observed between the two HbSC groups, patients with HU exhibited a lower blood viscosity. This difference could be attributed to the slightly higher, although not significant, RBC deformability measured in normoxia and at low oxygen level in HU-treated HbSC patients compared to the untreated ones. Luchtman-Jones et al. 21 reported increased HbF level and MCV in HbSC patients treated with HU. Although no significant difference in HbF level, MCV or MCHC was observed between the two HbSC subgroups, the correlation analyses suggested that HbS and HbF levels, and MCHC may modulate RBC deformability in HbSC individuals. Indeed, drugs targeting HbF, MCV and/or MCHC in HbSC individuals could result in greater RBC deformability, which in turn could lower blood viscosity for a given Hb level, as it is the case in HbSS patients treated by HU. 22 The lowering of blood viscosity in HbSC patients could be expected to decrease the risk for vaso-occlusive like events as it does in HbSS individuals.23–25 Beside, Luchtman-Jones et al. 21 previously observed a reduction of painful events in HbSC patients older than 15 yrs old treated by HU.
When blood was deoxygenated, the propensity of RBCs to sickle (i.e., PoS) was higher in HbSS individuals compared to HbSC patients, leading RBC deformability to reach lower values in HbSS patients (i.e., EImin). EImax, EImin and PoS were associated to MCV, MCHC, HbF and HbS in HbSS patients, which may explain why patients treated by HU are usually characterized by higher EImax and EImin, and lower PoS.4,6 The present study only found higher EImax in HbSS patients treated by HU compared to those without, but the cross-sectional nature of the study does not allow to really investigate the impact of HU on EImin and PoS. It was recently proposed that oxygen-gradient ektacytometry could be useful for dose titration of hydroxyurea therapy in children with HbSS. 26 While EImin of HbSC patients was associated with HbS, HbC and HbF, PoS was not associated with any of the parameters investigated. It is thus unknown if HU treatment in HbSC patients would decrease the PoS but one could suspect that it would improve EImin. The ongoing clinical trial focusing on the longitudinal effects of HU in HbSC patients, which incorporated oxygen gradient ektacytometry measurements, should help in providing a clear answer on these points. 27
One of the most surprising findings of the present study is the lowest ability of RBCs from HbSC individuals compared to HbSS patients to recover their normoxic deformability after a full cycle of deoxygenation. The percentage of recovery from HbSC individuals was positively correlated with MCV, suggesting that the hydration status of RBCs could play a key role in the ability of RBCs to recover their normoxic deformability after a deoxygenation cycle. This finding might be particularly important in the context of HbSC since it has been demonstrated that RBC tend to be very dehydrated because of the increased K:Cl cotransporter (KCC) activity in this sickle cell genotype. 28 Whether the percentage of recovery would further decrease after several oxygenation/deoxygenation cycles is unknown and further studies are needed to test the clinical usefulness, if any, of this parameter in the context of SCD.
Although, the clinical usefulness of oxygen-gradient ektacytometry in SCD has been questioned, 1 several studies found some associations between oxygen-gradient ektacytometry parameters and several clinical complications. For instance, Rab et al. 6 reported that the PoS was higher and EImin was lower in both HbSS adults and children with frequent vaso-occlusive crises compared to those who did not experience any vaso-occlusive crises in the 2 yrs preceding the inclusion in the study. This finding has been reinforced by another study 5 where it was demonstrated that for every 10 mmHg increase in PoS, the likelihood of an HbSS individual experiencing >1 type of acute complication increased (adjusted odds ratio = 1.65). In another study, Boisson et al. 4 found that the PoS was increased in HbSS individuals during vaso-occlusive crises compared to steady-state, suggesting a greater propensity of RBCs to sickle upon deoxygenation during this acute complication. However, it must be acknowledged that, at that time, there is no proof of the superiority of the oxygen-gradient ektacytometry parameters, compared to more well-known biomarkers of SCD such as HbF, F-cells, and dense RBCs, 29 or compared to shear-stress gradient ektacytometry parameters, 3 in predicting the onset of a clinical complication. However, oxygen-gradient ektacytometry seems to be very useful for testing the effects of some medications/new molecules targeting HbS polymerization/RBC sickling or to identify new mechanisms that could modulate RBC sickling.8,9,12,30–35
In conclusion, our study showed difference in oxygenscan parameters and blood viscosity between HbSS and HbSC individuals that could partly explain the differences in the clinical and hematological expression of the disease. Future studies focusing on the effects of various drugs in HbSC patients should account for the distinct determinants of RBC rheology and sickling in this genotype, which may influence treatment responses.
Footnotes
Author contribution
PC, MM, CB, ES, CR, PJ, and EN performed the experiments. SP, CHD and AG recruited the patients. PC, CB and EN designed the research study. PC and EN analyzed the data. PC and EN wrote the paper. All authors carefully read the paper and approved the final version.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.