
Abstract
Background
Handgrip strength correlates with cognitive function, but how gender and dietary protein interact with it is unclear.
Objective
To investigate the relationship between handgrip strength and cognitive function among non-stroke elders, and potential interaction effects of gender and dietary protein.
Methods
Non-stroke older adults with handgrip strength and cognitive tests available were included from National Health and Nutrition Examination Survey (NHANES) database. Multivariable linear regression analyses were used to explore the association between grip strength and cognitive performance. Multivariable logistic regression analyses were to investigate the effect of weak handgrip strength on cognitive impairment. Subgroup analyses were conducted to explore differences among sub-populations. Interaction effects of gender and protein intake were investigated by interaction analyses.
Results
Larger handgrip strength was associated with preferable memory function in men (CERAD Word Learning sub-test: p = 0.005; CERAD Delayed Recall: p = 0.009), better verbal fluency (Animal Fluency test: p = 0.005) and executive function in women (Digit Symbol Substitution Test: p = 0.017). Weak handgrip strength was associated with cognitive impairment, especially in older, female, obese participants or elders with low protein consumption. Participants with weak grip strength, compared to normal strength, were twice as likely to perform poorly in complex cognition evaluations (odds ratio = 2.01, p = 0.028). Interaction effect of protein intake was observed (p-interaction = 0.022). Compared to conditions of low protein intake, high protein intake significantly offset the impact of weak handgrip on cognitive impairment.
Conclusions
The association between grip strength and cognitive performance varies by gender. Non-stroke elders with weak handgrip strength are vulnerable to cognitive impairment. Improving muscle strength and increasing protein intake may be effective to mitigate decline in executive function.
Keywords
Introduction
Millions individuals are living with dementia worldwide, 1 imposing critical burdens on both patients themselves, families and societies.2,3 It has been reported that parts of dementia would be prevented and reversible if we could identify early cases and optimize modifiable risk factors. 4 Handgrip strength (HGS) is a convenient and cost-friendly assessment of upper limb muscle function, which also parallels with whole muscle strength. Low HGS predicts a wide range of adverse health outcomes.5–7 The latest revised diagnostic standard of sarcopenia has brought muscle strength to the forefront, highlighting its importance. 8
Emerging evidence from cross-sectional studies have shown an association between HGS and cognitive performance.9–11 Longitudinal correlation between HGS and cognitive decline has also been investigated.12–15 For instance, a research suggested nearly one third of dementia cases and dementia deaths could be attributable to low grip strength. 12 Another study found that a 5-kg decrement in HGS strongly predicted lower intelligence scores, worse memory function and incident dementia. 13
Multiple factors contribute to both weak muscle strength and cognitive impairment,8,16 such as advancing age, physical inactivity, malnutrition and multi-morbidity. Adequate intakes of protein and amino acids metabolites assist in alleviating sarcopenia. 17 Meanwhile, branched-chain amino acids content contributes to the homeostasis of brain glutamate, which might provide an explanation for the positive correlation between protein consumption and memory function. 18 Sex differences are noted in cognitive abilities and aging-related muscular degeneration. 19 Some researchers claimed that women were more vulnerable to Alzheimer's disease than men. 20 Thus, we assumed that weak HGS was related to cognitive decline, and this relationship may be differed by disparities of gender and dietary protein intake.
However, most existing studies did not exclude patients with stroke whose HGS and cognitive function could be easily jeopardized by post-stroke sequela. 21 Additionally, few studies have considered comprehensive sociodemographic variables. Hence, to overcome above-mentioned knowledge gaps in the literature, this study aims to (1) examine the association between HGS and cognitive performance in non-stroke older adults, and (2) explore possible interactions of gender difference, dietary protein consumption, and weak HGS on cognitive impairment utilizing data from the National Health and Nutrition Examination Survey (NHANES).
Methods
Study population
This study was conducted based on data from the NHANES database, which is a freely accessible database with information from a continuously collected, nationally representative cross-sectional survey of non-institutionalized civilian residents of the United States using a complex, stratified, multistage probability cluster sampling design. Interview, physical examination, and laboratory data are included in the dataset.
The NHANES study protocols were approved by the National Center for Health Statistics (NCHS) Research Ethics Review Board, and all NHANES participants included in current study had signed a written informed consent form in person.
Participants who were more than 60 years old (n = 3632) were screened from a total of 19,931 NHANES participants in 2011 and 2014 cycle, during which handgrip strength and cognitive function were both available. We excluded those with missing information on cognitive functioning tests (n = 444). Participants without muscle strength tests data were also excluded (n = 382). Moreover, those who had a self-reported history of stroke or incomplete data on other important variables were further excluded (n = 820). Finally, 1986 older adults (1011 male and 975 female) were eligible for inclusion in the present study (Supplemental Figure 1).
Assessment of cognitive function
A battery of cognitive tests was administered to measure the performance of participants in different domains, including the Consortium to Establish a Registry for Alzheimer's Disease (CERAD) Word Learning sub-test, the Animal Fluency test and the Digit Symbol Substitution Test in NHANES 2011–2014 cycles. All assessments were performed by trained interviewers at the Mobile Examination Center (MEC).
Briefly, the CERAD Word Learning sub-test, consisting of three consecutive learning trials (CFDCST) and an additional delayed recall trial (CFDCSR), is to assess immediate and delayed recall of new verbal information (memory domain) 22 ; the Animal Fluency test (CFDAST) is used to measure the categorical verbal fluency (component of executive function), regardless of cultural context; 23 and the Digit Symbol Substitution Test (CFDDS) is a well-established and validated measure to evaluate processing speed, sustained attention and working memory, representing a sensitive measure of frontal lobe executive functions.24,25 For all tests, higher scores represent better cognitive performance. As there is no well-defined cutoff point of each test score for identifying cognitive impairment, the lowest weighted quartile of each dimension is applied to define cognitive impairment, that is, a threshold of <17 for CFDCST, <5 for CFDCSR, <15 for CFDAST, and <43 for CFDDS, similar to the methods adopted in previous research. 26
Assessment of handgrip strength
HGS was evaluated using a handgrip dynamometer (Takei Digital 5401) and the process was supervised by a trained examiner. A practice trial was utilized to determine whether participants understood the procedure and the grip size was properly adjusted. Participants completed the test by a repeated dynamometer squeeze from each hand in a standing position for three times with a 60-s rest between measurements. HGS was documented in kilograms (kg) and expressed as the maximum value out of the three handgrip attempts in each hand. The largest reading out of six HGS values was adopted to represent individual's strength capacity. The NHANES website provides detailed descriptions of the protocol. 27 Weak HGS was defined as a grip strength of less than 27 kg for men and less than 16 kg for women, according to the standards made by EWGSOP2. 8
Assessment of dietary intake
Participants were eligible for two 24-h dietary recall interviews, of which the first interview was collected in-person in the MEC and the second one was collected by telephone. If an individual completed two 24-h dietary recalls, we calculated the average nutrition intake. Otherwise, we used the data from the first 24-h recall. Information of various foods and beverages intake was obtained to estimate the energy, nutrients and other food components. Relevant calculations were performed using the Food and Nutrient Database for Dietary Studies of the United States Department of Agriculture. 28 We extracted dietary intake data including total calorie, protein, alcohol. Non-protein calories was derived from the formula [Non-protein Calories (kcal) = Total Calories (kcal) - (Protein Intake (gram) * 4)]. Participants were further divided into three groups based on protein intake amount, that is, low (<0.8 g/kg body weight), moderate (0.8–1.0 g/kg body weight), and high group (≥1.0 g/kg body weight). 29
Covariates ascertainment
Other variables including sociodemographic characteristics (age, gender, race, education level, marital status, ratio of family income to poverty), anthropometric parameters (arm circumference, body mass index (BMI), body weight), behavioral factors (smoking, alcohol consumption, physical activity, sedentary lifestyle), medical history, and laboratory results to diagnose chronic comorbidity (diabetes, hypertension, dyslipidemia) were extracted. Age groups were classified as <70 and ≥70 years old. Ethnicity groups were comprised of Mexican American, other Hispanic, non-Hispanic White, non-Hispanic Black, and Other Race. BMI was divided into three categories (BMI < 25 kg/m2, 25–30 kg/m2, BMI ≥ 30 kg/m2). Self-reported education attainment, marital status, and economic status were further categorized, as shown in Supplemental Table 1. Smoking status was derived from Short-Memory Questionnaire. Excessive or limited alcohol consumption was defined by daily alcohol drinking amount based on two 24-h dietary recalls. 30 Time on physical activity and sedentary activity were derived from the Physical Activity Questionnaire. The diagnosis of hypertension, diabetes mellitus, and dyslipidemia was confirmed through medical history and laboratory test results. Detailed definitions and illustrations were presented in Supplemental Table 1.
Statistical analysis
The NHANES sampling weights were considered in the complex sample analysis to achieve nationally representative estimates. Baseline characteristics were presented as mean ± standard error for continuous variables or number (proportions) for categorical variables by HGS status, and by cognitive function status respectively. Differences in characteristics were compared using Student's t-test or Chi-squared tests accordingly. Excluded and included participants were also compared in order to avoid skewed results. Associations between maximal grip strength and cognitive tests scores, both as continuous variables, were investigated using complex sample multivariable linear regression tests, stratified by gender. Similarly, complex sample multivariable logistic regression analyses were performed to explore the link between weak HGS status and the risk of cognitive impairment. Age group, sex, ethnicity, education attainment, marital status, economic status, protein intake categories, non-protein calories, BMI categories, physical inactive or not, sedentary time and comorbidity status were adjusted in the models. Subgroup analysis was further conducted to examine whether this association differed in sub-populations. Considering the effect of dietary protein intake on the relationship between HGS and cognitive decline, interaction analysis was performed using a logistic regression model with low protein intake participants selected as reference.
All hypothesis tests were two sided. Significance was defined at the α = 0.05 level. Weighted analyses were conducted within the R package “survey” to provide reliable national estimates in accordance with National Center for Health Statistics recommendations. Analyses were performed using R, version 4.2.2 (R Foundation for Statistical Computing) with R Studio, version 2022.07.1 Build 554 (R Studio Inc).
Results
Characteristics of participants stratified by HGS status
The characteristics of the study population were shown in Table 1. Compared to normal muscle strength group, participants with weak HGS tended to be older (76 ± 0.74 versus 68.71 ± 0.25), living alone (54.0% versus 33.1%), of lower degree in education (51.0% versus 35.6%) and family income (2.53 ± 0.16 versus 3.27 ± 0.08), and have lower arm circumference (30.03 ± 0.68 versus 32.55 ± 0.16). Besides, lower scores in all domains of cognitive test, that is, CFDCST total (17.45 ± 0.48 versus 19.92 ± 0.26), CFDCSR (4.89 ± 0.29 versus 6.36 ± 0.11), CFDAST (15.37 ± 0.69 versus 18.56 ± 0.20), and CFDDS (41.14 ± 1.87 versus 54.27 ± 0.59) were also noticed in weak HGS group. They were also prone to spend less time in physical activities (75.04 ± 15.67 versus 132.46 ± 8.97) and have higher prevalence of hypertension (78.1% versus 64.8%) and diabetes mellitus (38.3% versus 27.4%) but less likely to be diagnosed with dyslipidemia (66.2% versus 83.9%). No statistically significant differences in gender, ethnicity, daily protein and energy intake, BMI, smoking or alcohol consumption status were found between two groups.
Basic characteristics of the study participants stratified by handgrip strength status.
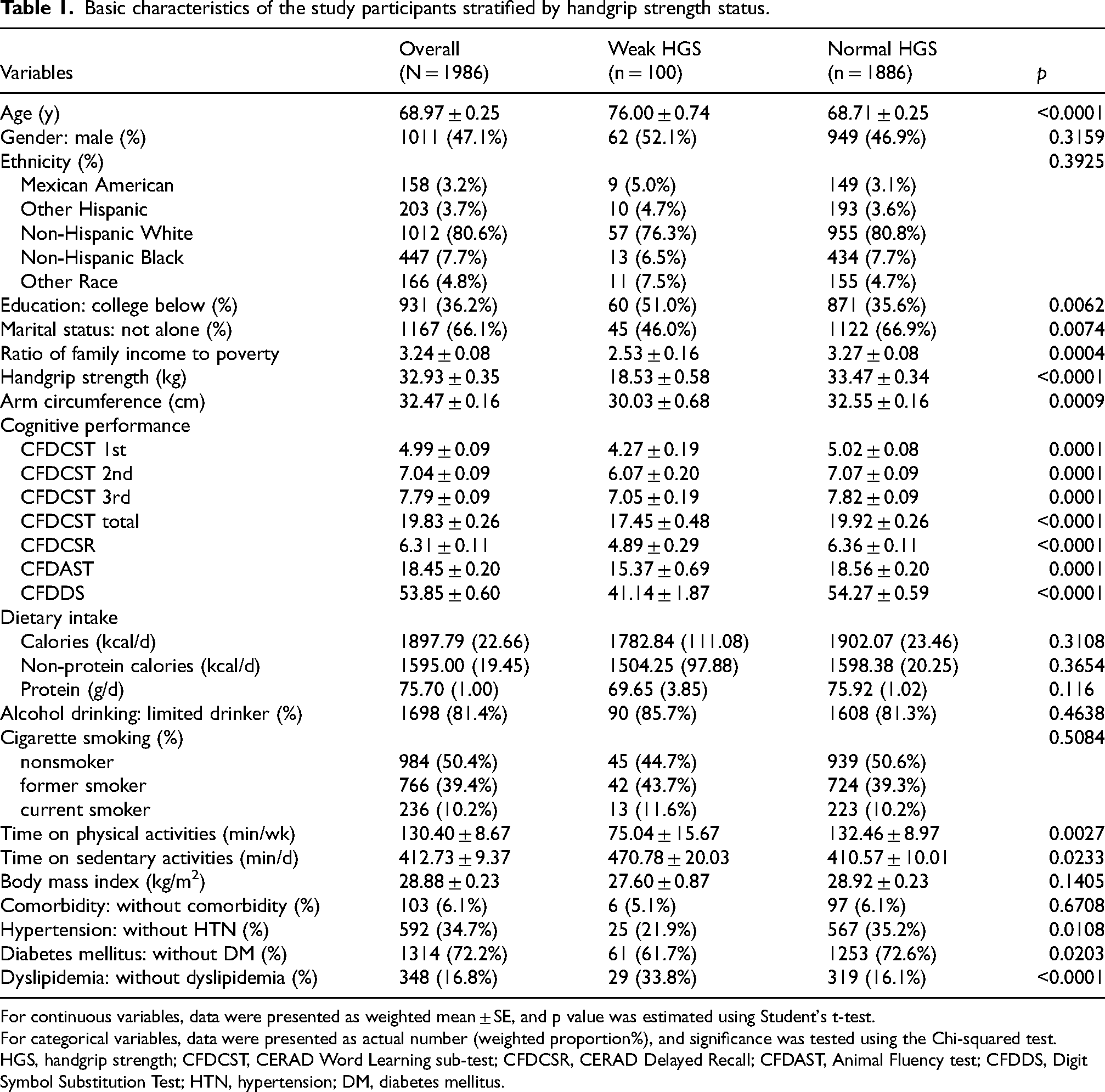
For continuous variables, data were presented as weighted mean ± SE, and p value was estimated using Student's t-test.
For categorical variables, data were presented as actual number (weighted proportion%), and significance was tested using the Chi-squared test.
HGS, handgrip strength; CFDCST, CERAD Word Learning sub-test; CFDCSR, CERAD Delayed Recall; CFDAST, Animal Fluency test; CFDDS, Digit Symbol Substitution Test; HTN, hypertension; DM, diabetes mellitus.
To be mentioned with, maximal handgrip strength, cognitive scores were quite different between the excluded and included participants (shown in Supplemental Table 2). Included participants were younger, had higher HGS, lower prevalence of weak HGS and performed better in cognitive tests. Differences in demographic background, lifestyle modifications, glucolipid metabolic profiles, and comorbidity status were also statistically significant.
Association between handgrip strength and cognitive performance
Survey multivariable linear regression model was used to explore the association between handgrip strength and cognitive tests scores in different domains including CFDCST, CFDCSR, CFDAST, and CFDDS. As indicated in Table 2, for male participants, HGS was positively associated with better performance in CFDCST (exp(β) = 1.06, 95%CI: 1.01–1.11, p = 0.005) and CFDCSR (exp(β) = 1.04, 95%CI: 1.01–1.07, p = 0.009), but not in CFDAST or CFDDS. Similar pattern was also noticed in female participants, HGS was associated with higher scores in CFDAST (exp(β) = 1.11, 95%CI: 1.02–1.20, p = 0.005) and CFDDS (exp(β) = 1.33, 95%CI: 1.02–1.74, p = 0.017) in fully adjusted models, while not in CFDCST or CFDCSR domain.
Association between cognitive test scores and per kilogram increase in handgrip strength, stratified by gender.
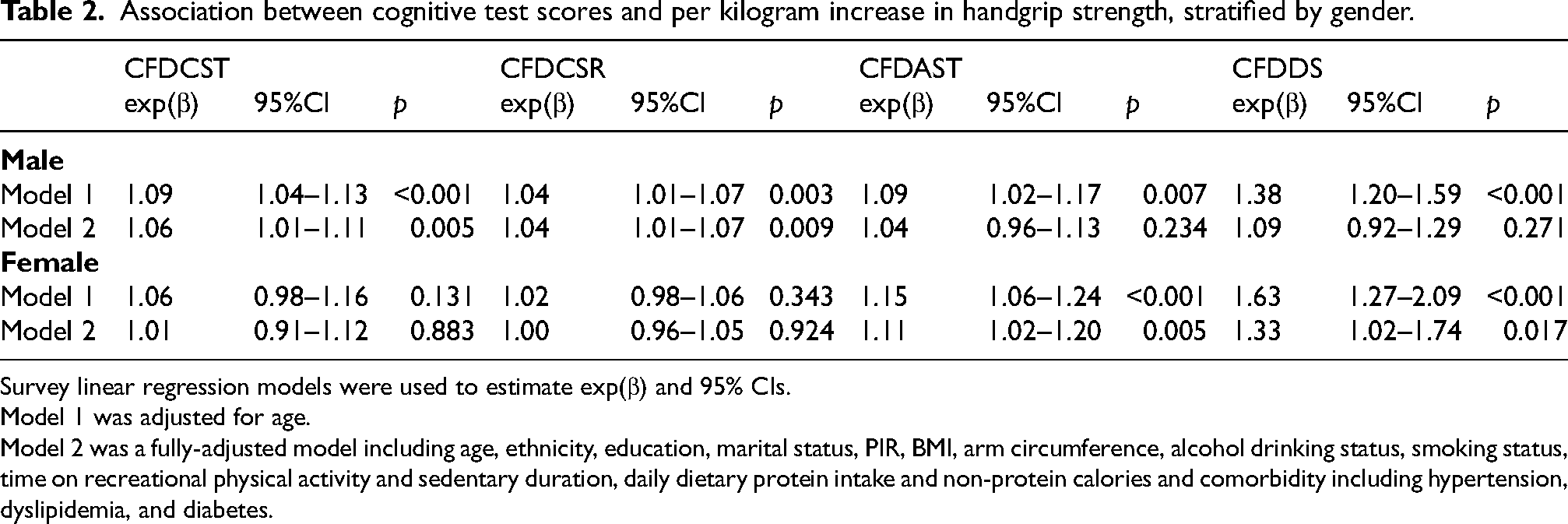
Survey linear regression models were used to estimate exp(β) and 95% CIs.
Model 1 was adjusted for age.
Model 2 was a fully-adjusted model including age, ethnicity, education, marital status, PIR, BMI, arm circumference, alcohol drinking status, smoking status, time on recreational physical activity and sedentary duration, daily dietary protein intake and non-protein calories and comorbidity including hypertension, dyslipidemia, and diabetes.
Comparisons of participants from normal cognitive performance and cognitive impairment group
As shown in Supplemental Table 3, people from cognitive impaired group were older, had less education experiences, less income, more likely to have hypertension and diabetes. Participants with worse scores in CST, CSR, and DS tests were likely to be male. When came to maximal HGS evaluation, participants in cognitive impaired group were lower. Elders in cognitive impairment group had a higher prevalence of weak HGS status (CST: 6.9% versus 2.6%, CSR: 7.1% versus 2.5%, AST: 5.9% versus 2.6%, DS: 7.2% versus 2.0%, respectively). Besides, dietary protein intake and non-protein calories intake also differed, which were less consumed in three out of four cognitive impaired groups.
Weak HGS and cognitive impairment in overall and subgroup analysis
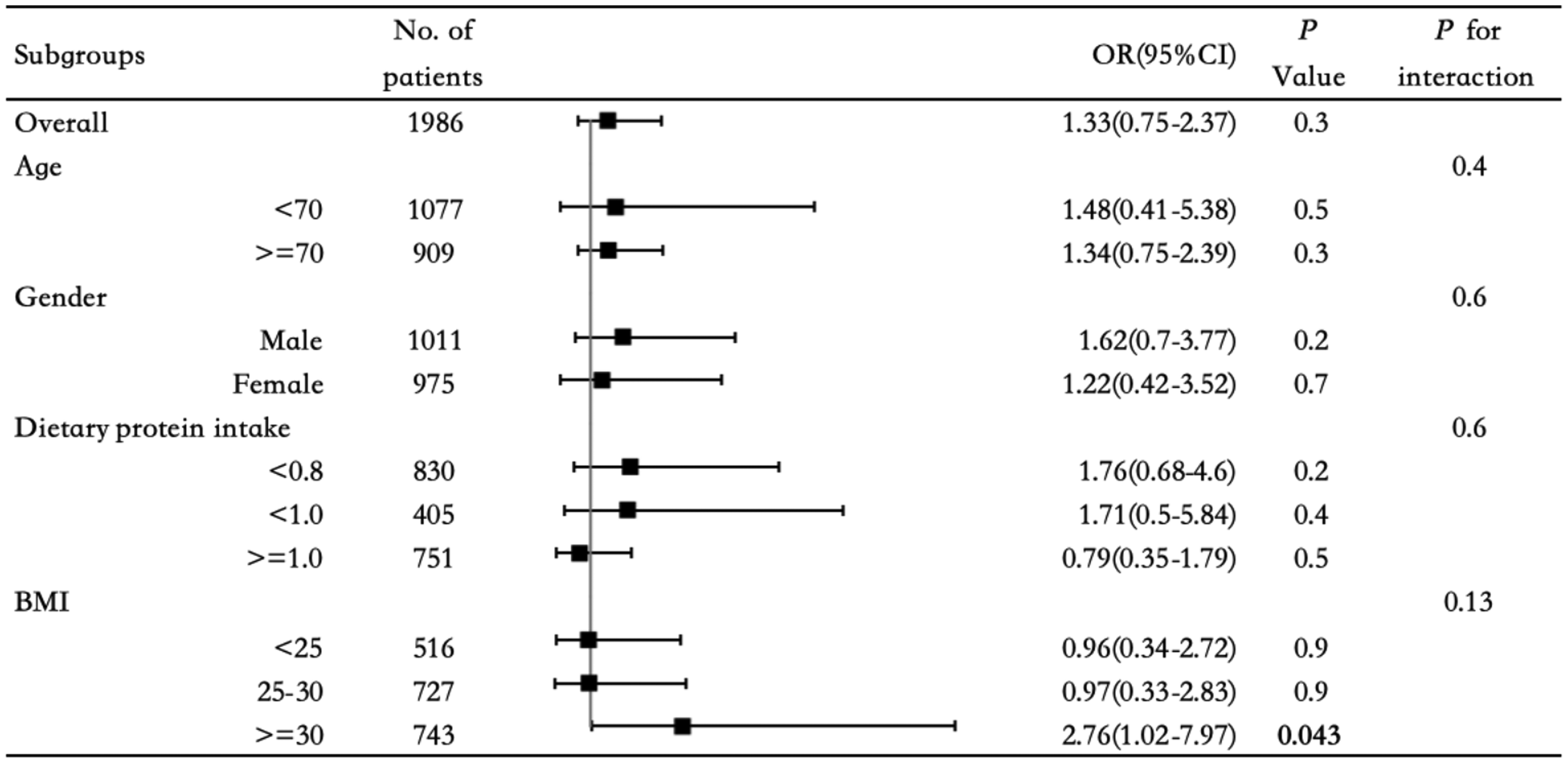
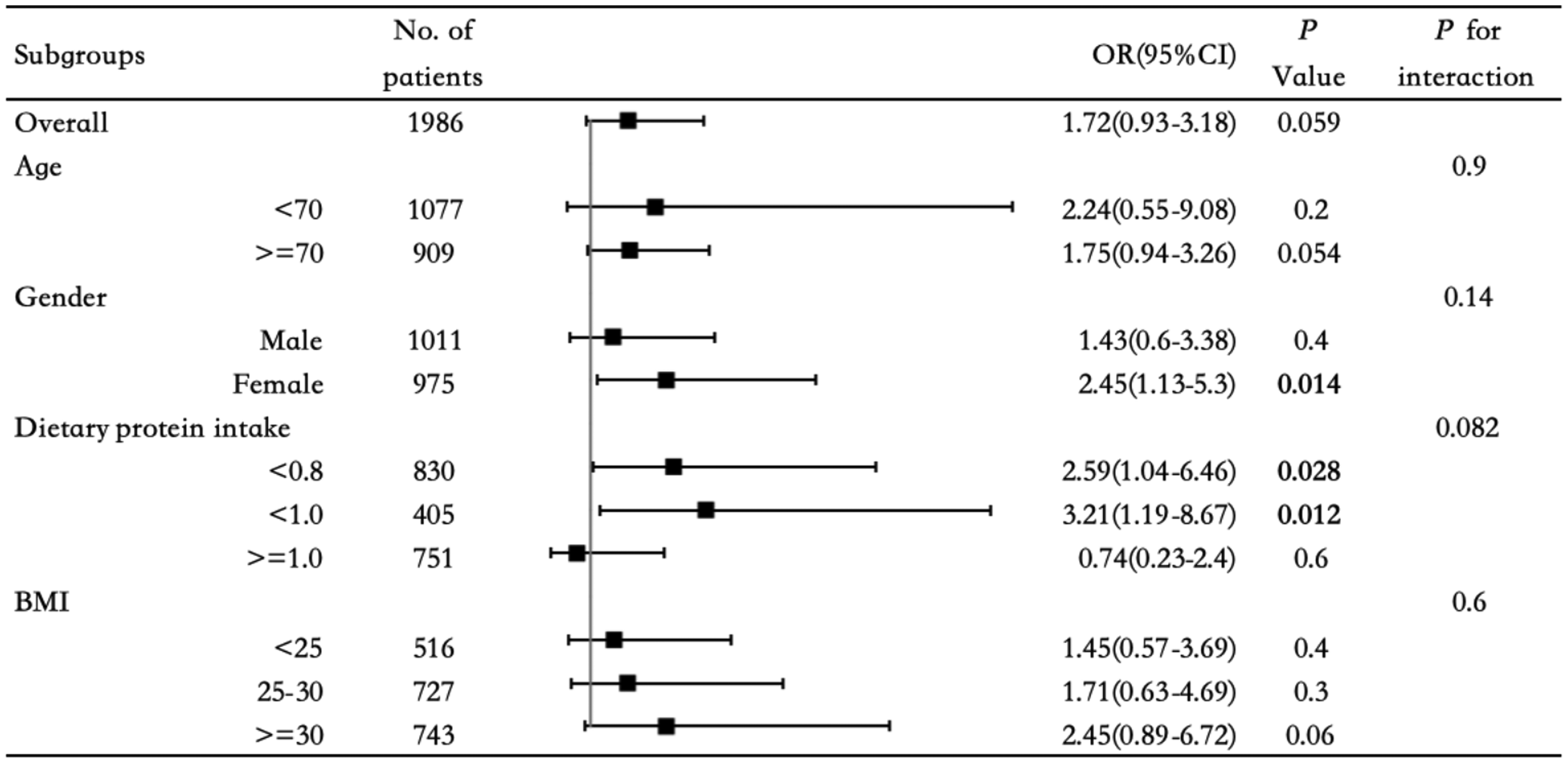
Survey multivariable logistic regression model was used to investigate the association between weak HGS and cognitive impairment. Subgroup analysis stratified by sex, age, daily dietary protein intake and BMI, based on multivariable logistic regression model, was also performed. As indicated in Figure 1, participants with weak HGS were twice as likely to have cognitive impairment in a more complex cognition evaluation (CFDDS). This relationship was more pronounced in participants who were older (OR = 2.18, 95%CI: 1.09–4.34, p = 0.016), obese (OR = 5.35, 95%CI: 1.26–22.8, p = 0.014) and in those who consumed less dietary protein (OR = 4.78, 95%CI: 1.67–13.7, p = 0.002). Meanwhile, obese participants with weak HGS were likely to get lower scores in instant memory assessment (OR = 2.76, 95%CI: 1.02–7.97, p = 0.043), as revealed in Figure 2 (CFDCST). Among female elders (OR = 2.45, 95%CI: 1.13–5.3, p = 0.014), people who had low (OR = 2.59, 95%CI: 1.04–6.46, p = 0.028) or moderate protein intake (OR = 3.21, 95%CI: 1.19–8.67, p = 0.012), weak HGS was independently correlated with delayed memory dysfunction, as depicted in Figure 3 (CFDCSR). However, no such association was detected between weak HGS and verbal frequency subdomain, either in overall participants or in subgroup analysis, as shown in Figure 4 (CFDAST).
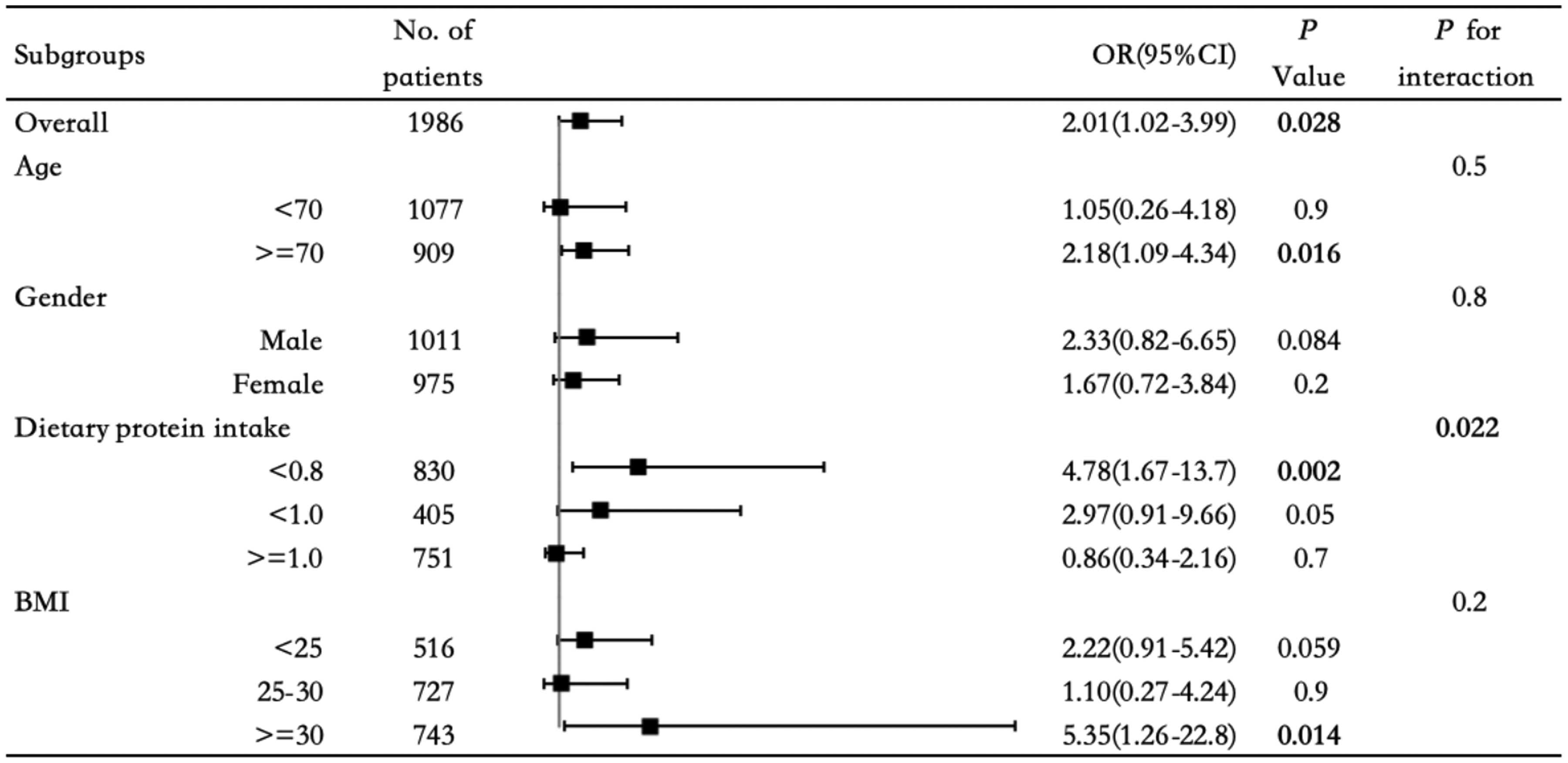
Overall and subgroup analysis of weak handgrip strength and cognitive impairment in CFDDS.
Overall and subgroup analysis of weak handgrip strength and cognitive impairment in CFDCST.
Overall and subgroup analysis of weak handgrip strength and cognitive impairment in CFDCSR.
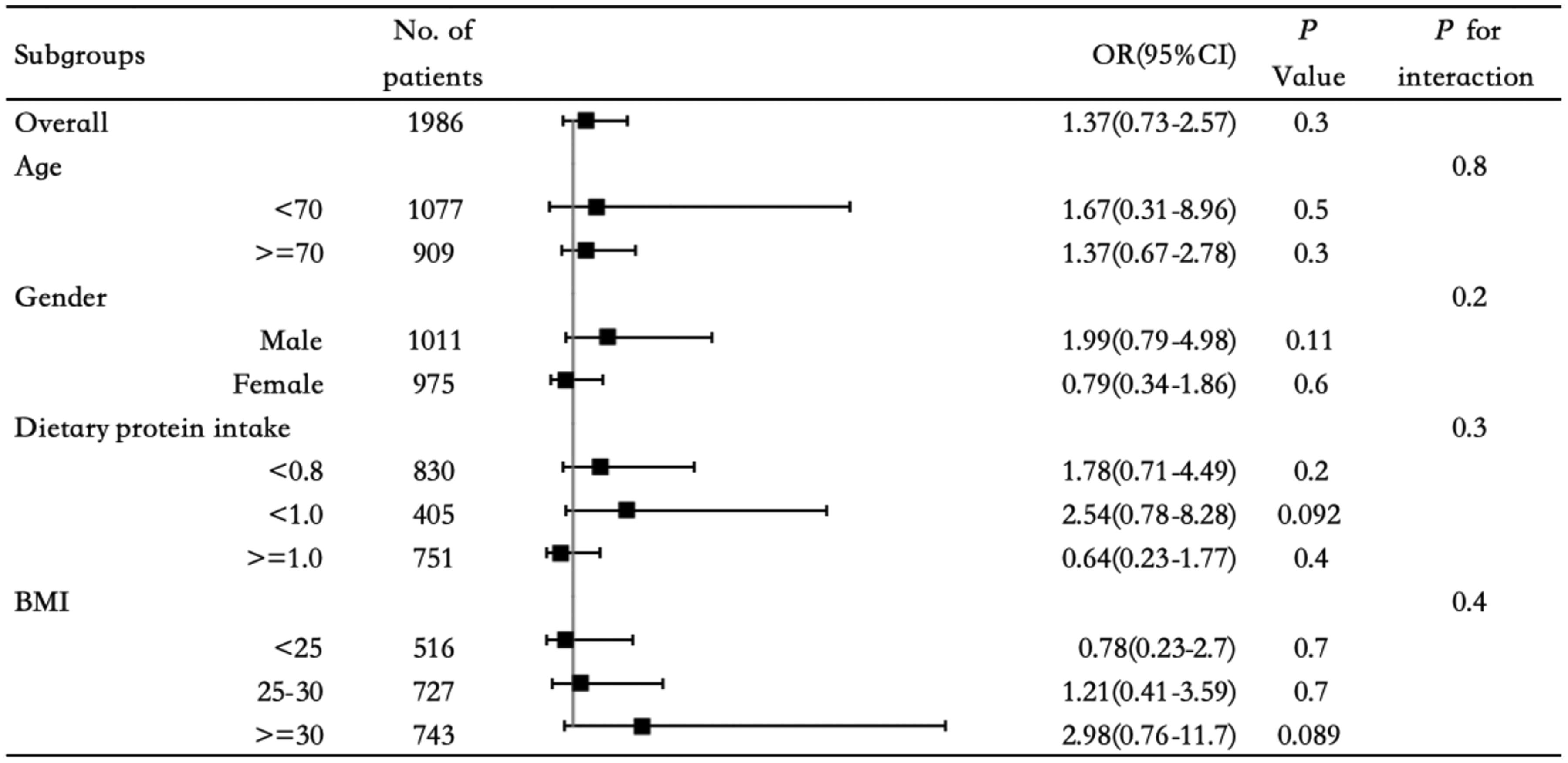
Overall and subgroup analysis of weak handgrip strength and cognitive impairment in CFDAST.
Interaction effect of dietary protein intake
Simultaneously, we noticed an interaction effect of dietary protein intake on the association between weak HGS and cognitive impairment (Figure 1). After incorporating the product-term of two variables into fully-adjusted logistic regression model, we found the multiplicative interaction between low HGS and high protein consumption on cognitive impairment risk was statistically significant (OR = 0.17, 95%CI: 0.04–0.70). As shown in Table 3, compared to low protein intake, under high protein intake conditions, the effect of weak handgrip on cognitive dysfunction is significantly offset; whereas under moderate protein intake conditions, the association between weak HGS and cognitive impairment is not significant.
Multiplicative interaction of dietary protein intake and HGS on cognitive impairment (CFDDS).
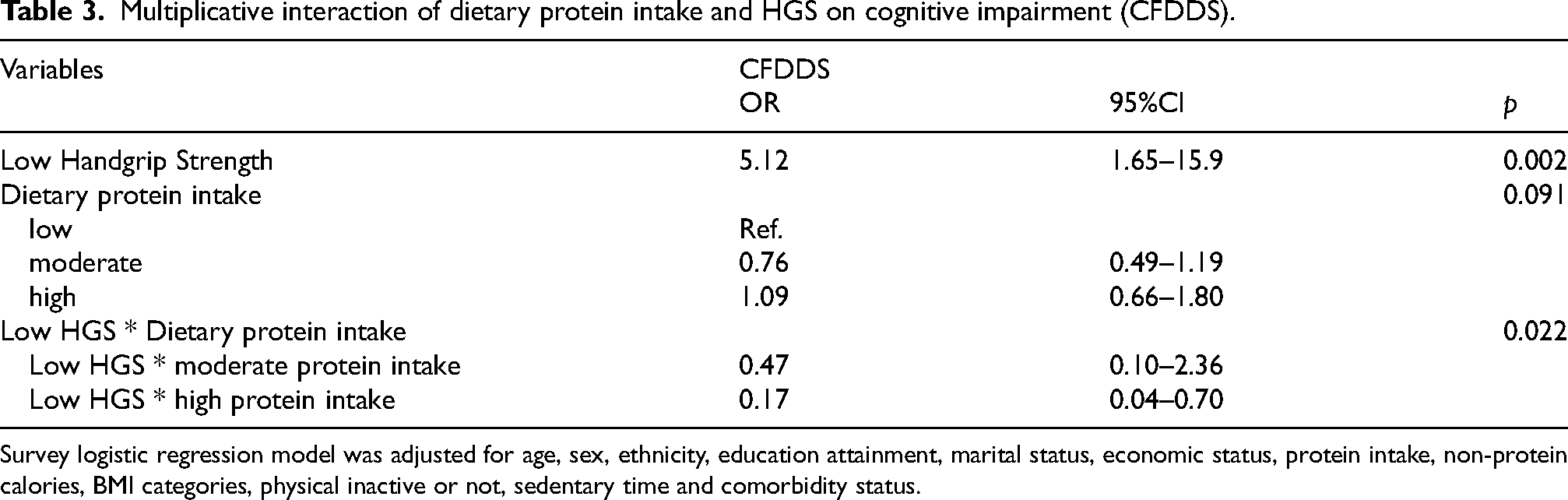
Survey logistic regression model was adjusted for age, sex, ethnicity, education attainment, marital status, economic status, protein intake, non-protein calories, BMI categories, physical inactive or not, sedentary time and comorbidity status.
Discussion
The current study aligns itself with the most recent literature which demonstrate a positive relationship between HGS and cognitive performance. Larger HGS correlates with favorable memory ability in older men, with better performance in executive function and processing speed among female participants. In non-stroke elders, weak handgrip strength can be a predictor of cognitive impairment, especially in those who are females, more than 70 years old, obese, or who consume less protein. Affected individuals are twice as likely to experience cognitive difficulties in CFDDS test, which is a more complex cognitive evaluation. Dietary protein intake poses interaction effects on the association between weak HGS and cognitive decline. High protein intake significantly offsets the association of weak HGS and poor performance in executive functions (CFDDS).
Previous cross-sectional studies have come to a similar conclusion that individuals with larger HGS had better cognitive function.31–34 Prokopidis et al. reported this relationship was more pronounced in learning ability and verbal fluency, 31 while similar pattern was seen in memory recall aspect in Chinese population. 32 Besides, two studies showed the link between HGS and cognitive impairment merely existed in men.31,33 A meta-analysis identified consistently positive longitudinal associations between HGS and cognitive function. 35 Other researchers explored potential predictive value of HGS for prospective cognitive decline and incident dementia, but most studies also included middle-aged population.36,37 Peng et al. found poor HGS predicted cognitive impairment merely in men. 14 Haagsma et al. reported a gender-specific dose response between HGS and cognitive performance, with strongest in verbal fluency in females but memory recall in males. 37 Several intervention studies indicated that enhancing muscle strength also benefited cognitive function.38,39 However, none has investigated the effect of dietary factors.
The completion of the handgrip strength test requires more than muscle contraction, but also a complicated coordination behavior including signals transmitting orderly across neurons and the activation of brain networks. 40 This implies handgrip strength and cognitive function may parallel each other. For instance, one research conducted in 14,775 Americans showed that maintaining a higher HGS may reduce the risk of developing and worsening cognitive impairment, while cognitive impairment also negatively affects HGS during a two-year follow-up. 41 Similar conclusions were also reached from other cohorts,42,43 indicating a bidirectional association might exist between HGS and cognitive function.
Indeed, weak HGS and cognitive impairment share similar brain structural and neurochemical changes, as well as common pathways and mechanisms. Recent studies have demonstrated people with stronger HGS had larger hippocampal and lobar brain volumes quantified by MRI.44–46 Meanwhile diminished HGS was in parallel with increased cerebral white matter hyperintensity,47,48 providing a morphological perspective in terms of the bidirectional association between muscle strength and cognitive impairment. Vints et al. also found participants who had larger muscle strength presented with healthier brain neurometabolism, measured by blood biomarkers such as kynurenine and N-acetylaspartate/Creatine levels. 49 Mechanisms involved in the association between weak HGS and cognitive impairment may be explained as follows. Firstly, chronic inflammation and oxidative stress are both involved in the damage of muscle strength and cognitive function. Inflammatory cytokines such as tumor necrosis factor-α and Interleukin-6, negatively correlated with HGS and cognitive function. 50 Low grip strength, to some extent representing a pro-oxidative state, subsequently or simultaneously leads to cognitive deficits. 51 Secondly, skeletal muscle is the main source of myokines, including brain-derived neurotrophic factor and irisin. 52 Such myokines can cross the blood-brain barrier and thus affect neuronal proliferation, differentiation, and plasticity in brain.53–55 Moreover, mitochondrial dysfunction is also involved in neurological and skeletal muscular diseases as both are highly dependent on mitochondrial energy metabolism.56,57
Research regarding the gender disparities on cognitive impairment have been well-documented. Most researchers pointed out that women were more likely to develop dementia than men,20,58 though some disagreed. 59 Aforementioned studies also suggested sex-differences in the relationship of HGS and cognitive function.14,31,33,37 Our analysis demonstrated some gender disparities: 1) HGS correlated with cognitive performance in a sex-dependent way, 2) female participants with weak HGS were more prone to cognitive impairment than men in low HGS status. However, we observed no significant interaction effect of sex difference on the impact of HGS on cognitive impairment.
Malnutrition also plays an essential role in the pathogenesis of poor functioning and loss of muscle mass, given that insufficient protein intake leads to an imbalance in muscle homeostasis. 60 Older adults with high protein intake performed better in physical tests than those not. 61 The protective effect of high dietary protein intake on cognitive impairment has also been investigated.62,63 In agreement with prior work, 64 our subgroup analyses indicated participants with weak HGS and consumed less protein had higher odds ratio for cognitive impairment in delayed recall memory (CSR) and frontal lobe executive functions (DS) test. Further interaction analysis showed that the impact of low HGS on cognitive outcomes, mainly executive functions domain, was significantly mitigated by higher protein intake. Among various dietary patterns, Mediterranean diet (MedDiet) has been extensively investigated and is well known for its benefits in cardiovascular disease prevention. Proteins obtained in a typical MedDiet meal are diverse, from plants-based food including legumes and whole grains, to animal-based food such as seafood, moderate consumption of poultry and dairy, limited red meat. There are a wealth of studies demonstrating its potential efficacy in cognitive decline prevention. 65 Nevertheless, another systematic review including five randomized controlled trials has revealed no benefit of the MedDiet for incident cognitive impairment or dementia. 66 Other researchers also explored MedDiet-related biological and structural changes in brain. Frye et al. have found MedDiet conferred protection against central inflammation by assessing RNAseq-generated transcriptional profiles in lateral temporal cortex. 67 Adherence to MedDiet also leads to cerebrospinal fluid metabolomics changes, 68 modulates plasma concentrations of endocannabinoids and N-acylethanolamines, which are lipid mediators involved in multiple neurological disorders. 69 Hence, long-term adequate protein intake, a proper dietary pattern might be proposed as a strategy to preserve cognitive performance in older adults. Further insight into how and at what level protein supply interacts with the brain and skeletal muscle system is warranted.
The originality of the present study relies on the evaluation of most updated EWGSOP2-defined low HGS in relation with cognitive function across various subdomains in the first place. Besides, we explored this association for the first time in community dwelling non-stroke population, among whom the prevention and primary screening for dementia is particularly important. This study also pioneers in assessing interaction effects of protein intake and weak HGS on the risk of cognitive impairment. Fourthly, we controlled for a comprehensive range of sociodemographic variables and health-related behavioral factors. Moreover, another strength of this study is the utilization of a large representative sample from the NHANES which guarantees the accuracy and validation of the original data.
However, some limitations should be acknowledged. Dietary recall of two single days may not be representative enough of one individual's habitual protein intake. Furthermore, inherent to retrospective observational study, it is impossible to determine whether a causal or bidirectional association exists between low HGS and cognitive impairment. Extrapolating results to all the population of the United States should be cautious as there were differences in important variables between included and excluded participants. Lastly, more details on quality and sources of dietary protein, other putative risk factors as well as underlying mechanisms could not be further investigated.
In conclusion, our study identifies that weak HGS is independently associated with poor cognitive function, especially in participants with characteristics such as older age, female, obese and less protein consumption. It is therefore feasible to monitor HGS decreases among seniors in early recognition of cognitive decline, particularly in targeted sub-populations. Besides, higher protein consumption might counteract the impact of low HGS on executive function in older adults. This relationship underscores that maintaining muscular strength and optimizing dietary protein intake could be served for cognitive health.
Supplemental Material
sj-docx-1-alz-10.1177_13872877241289379 - Supplemental material for Dietary protein intake interacts with weak handgrip strength and cognitive impairment
Supplemental material, sj-docx-1-alz-10.1177_13872877241289379 for Dietary protein intake interacts with weak handgrip strength and cognitive impairment by Lingling Zhou and Cui Zhang in Journal of Alzheimer's Disease
Footnotes
Acknowledgments
We appreciate the efforts given by the NHANES team for collecting and providing data publicly to researchers. We also acknowledge all participants and staffs involved in this research.
Author contributions
Lingling Zhou (Conceptualization; Data curation; Formal analysis; Methodology; Software; Visualization; Writing – original draft); Cui Zhang (Data curation; Formal analysis; Funding acquisition; Software; Writing – review & editing).
Funding
This research was supported by the National Natural Science Foundation of China (Grant Number: 82100545). The funder had no roles in the design of the study; collection, analysis, and interpretation of data; or writing the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.