
Abstract
Background
Distinguishing between mild cognitive impairment (MCI) and early dementia requires both neuropsychological and functional assessment that often relies on caregivers’ insights. Contacting a patient's caregiver can be time-consuming in a physician's already-filled workday.
Objective
To assess the utility of a brief, machine learning (ML)-enabled digital cognitive assessment, the Digital Clock and Recall (DCR), for detecting functional dependence.
Methods
We evaluated whether the DCR can help identify individuals at risk of functional deficits as measured by the informant-rated Functional Activities Questionnaire (FAQ) in older individuals including cognitively unimpaired, MCI, and dementia likely due to Alzheimer's disease.
Results
The DCR scaled well with FAQ scores, and ML classifiers trained on multimodal DCR features demonstrated strong performance in predicting functional impairment on a held-out test set. Differences in FAQ scores between DCR-predicted classes were comparable across key demographic groups.
Conclusions
The DCR can streamline the clinical decision-making, triage, and intervention planning associated with functional impairment in primary care.
Keywords
Introduction
By the year 2050, the number of individuals with dementia is projected to grow to 13.8 million in the U.S. and 152 million people globally.1,2 Presently, identifying cognitive deficits related to dementia typically occurs when cognitive complaints are shared with healthcare providers. Diagnosis of dementia requires a demonstration of a decline in ability to perform daily activities. By the time a cognitive concern is raised by the individual or their family member or care partner, however, cognitive decline has often progressed beyond the effective window for therapeutic interventions.1,3 Achieving optimal efficacy for disease-modifying treatments (DMT) thus requires a shift from current reactive dementia care to a paradigm of early detection particularly at the stage of mild cognitive impairment (MCI).
MCI is characterized by cognitive performance below one's same-aged peers with minimal or no interference with daily life.4,5 Approximately 10–15% of individuals with MCI progress to dementia each year. 1 Unfortunately, over 90% of MCI cases remain undiagnosed. 6 Changes in functional abilities in instrumental activities of daily living (iADLs) requiring greater executive control, such as managing finances, driving, and keeping track of appointments, are the first to be affected by cognitive impairment and correlate with conversion to dementia.7–10 Subtle impairments in memory and executive function are the most predictive of this conversion.11,12 Distinguishing between MCI and dementia should thus include assessing the impact of cognitive deficits on the patient's functional dependence in iADLs, which is commonly reported by an informant (often a family member or care partner). Given the complexities of involving a care partner in routine care, it would be valuable to know if the patient is unlikely to have a functional impairment that would indicate progression to dementia. Thus, appropriate evaluation of patients with cognitive impairment requires assessing both cognitive and functional status and given the time-pressured workflows of primary-care providers (PCPs), novel solutions are needed.
The Digital Clock and Recall (DCR™) consists of the DCTclock™, a digital, machine learning (ML) enabled version of the traditional clock drawing task and a 3-word delayed recall task, and employs algorithms to evaluate memory, executive function, visuospatial abilities, and motor functions. The DCR has been shown to detect MCI and dementia likely due to Alzheimer's disease (DLAD) in populations relevant to primary care settings with greater sensitivity than traditional pencil and paper cognitive assessments.13–16 Among 706 participants from the multisite Bio-Hemes-001 study with >20% of participants from racial or ethnic minority groups, the DCR was superior to the Mini-Mental State Examination (MMSE) for identifying individuals with mild cognitive impairment and mild dementia. 17 In fact, the DCR identified 80.7% of 104 individuals who were labeled by the MMSE as cognitively unimpaired (score ≥28) but showed verbal-memory impairment on the Rey Auditory Verbal Learning Test (RAVLT). Further, unlike the MMSE, the DCR showed no bias due to participant's ethnicity (Hispanic versus Non-Hispanic). 13 In another study that analyzed data from 922 participants in the Bio-Hermes-001 study, a multimodal ML-enabled model based on the DCR that incorporated process-based drawing, acoustic, and speech metrics of task performance during the DCTclock and Delayed Recall, showed improvement over the DCTclock and the DCR score alone in identifying verbal memory impairment. 14 That DCR-based model achieved an area under the receiver operating characteristic curve (AUC) of 0.83, 0.81 sensitivity, and 0.80 specificity in identifying verbal memory impairment as confirmed by the RAVLT. In a third study on 828 participants in the Bio-Hemes-001 study, the DCR showed greater accuracy in identifying individuals with cognitive impairment than the Mini-Cog. 15 Based on these results, we hypothesized that the DCR can help streamline the PCPs’ workflow to address functional impairment among individuals with MCI and early dementia. Specifically, we evaluated whether the DCR can classify functional impairment, as assessed by the informant-rated Functional Activities Questionnaire (FAQ), in older individuals ranging from cognitively unimpaired to those with MCI and DLAD.18,19 In particular, we focused on the DCR's ability to rule out functional impairment, thus reassuring PCPs when no direct functional evaluation is needed.
Materials and methods
Sample and assessments
We studied data from 941 participants from the multi-site Bio-Hermes-001 study (age median ± SD = 72 ± 6.7; 57% female; years of education = 16 ± 2.71; primary language English), organized by the Global Alzheimer's Platform (GAP).20,21 The study collected blood, positron emission tomography (PET), and digital biomarkers from a large, racially diverse sample of healthy participants and individuals with MCI or DLAD. Data from the Bio-Hermes-001 study will be made publicly available by GAP on the Alzheimer's Disease Data Initiative website in the future. Ethical approval was granted by the Institutional Review Board at each institution participating in the GAP consortium (please see the Bio-Hermes study website 17 for a list of study sites). All participants signed informed consent either directly or via a legally authorized representative prior to participation in the study.
Inclusion criteria were adults 60–85 years of age, fluent in the language of the tests used and the test site, and with a Mini-Mental Status Exam (MMSE) score of 20–30 at screening. Exclusion Criteria were extensive and based on underlying conditions (NCT04733989). 20 All participants were classified a priori by the Bio-Hermes team into cognitively unimpaired (n = 402), MCI (n = 297), or DLAD (n = 239) based on combinations of clinical history, clinical examination that included the Rey Auditory Verbal Learning Test (RAVLT), FAQ/partner report, and the MMSE.22–25 Participants completed the DCR on their baseline visit which was not used as part of the cohort definition criteria.
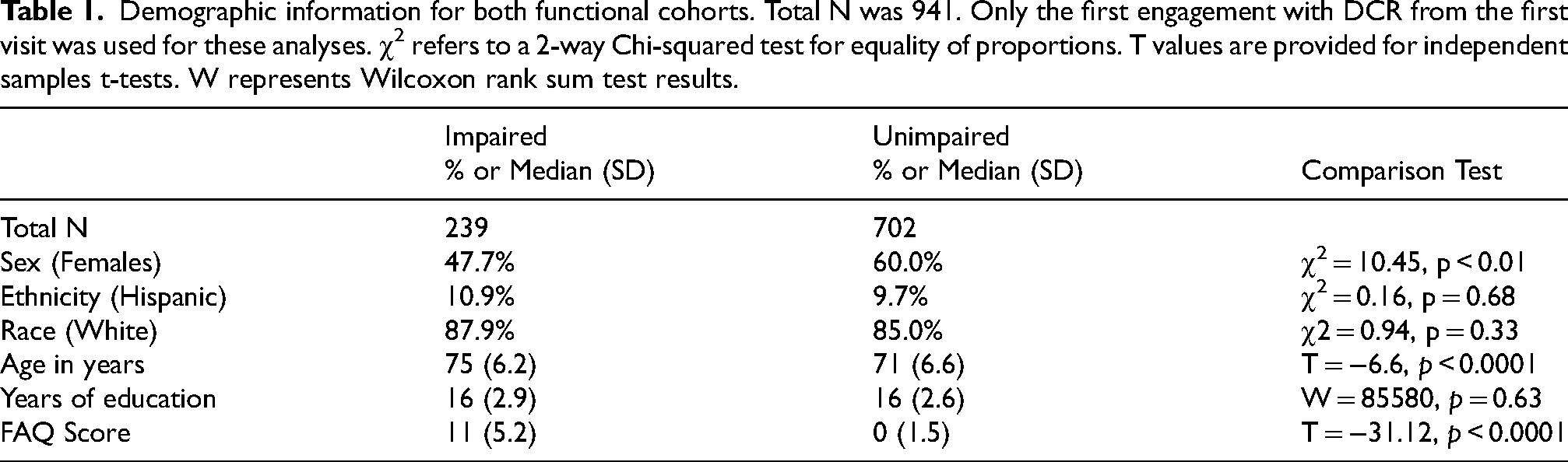
We used the FAQ score to categorize participants into functionally impaired (FAQ score ≥6) and functionally unimpaired (FAQ score <6) cohorts.18,19,26–28 An FAQ score of 6 or greater is equivalent to dependence in two or more activities of daily living, which is interpreted as at least mildly affected functional capacity. 26 Even though an FAQ score cutoff of 9 is also clinically used to indicate functional impairment, we chose not to use this threshold due to the low rate (17%) of participants that would have met this criterion for impairment. 29 Table 1 shows the demographic information for each cohort, including statistical comparisons between them.
Demographic information for both functional cohorts. Total N was 941. Only the first engagement with DCR from the first visit was used for these analyses. χ 2 refers to a 2-way Chi-squared test for equality of proportions. T values are provided for independent samples t-tests. W represents Wilcoxon rank sum test results.
DCR and its multimodal features
The DCR is a semi-supervised and automatically scored 3-min digital cognitive assessment that is automatically scored. The DCR score considers performance on 3-word immediate and delayed recall and the DCTclock, a digital version of the traditional clock drawing test that analyzes the entire drawing process during command (i.e., drawing from memory) and copy (i.e., with an example clock shown right above the drawing canvas) conditions rather than only the final drawing output. Immediate recall is performed before the DCTclock, whereas delayed recall is captured immediately afterward. The DCR produces a score (0–5) that captures key features of cognitive function calculated from clock drawing performance (0–2 points based on DCTclock performance) and delayed recall performance (0–3 points available based on number of words recalled). DCR scores are grouped into three impairment categories: (1) Green, or no indication of cognitive impairment, for scores of 4 and 5; (2) Yellow, or some indication of cognitive impairment, for scores of 2 and 3, and (3) Red, or likely indication of cognitive impairment, for scores of 0 or 1. Further details on the DCR and its subscores can be found in previous studies.14,30,31 In addition to these baseline DCR features, we computed a new set of multimodal features based on drawing time series and speech behavior. This produced 2000 multimodal features that were used as predictors in our ML models. More details on the scoring of these multimodal features can be found in. 15
Analyses
This work was divided into two general steps: (1) examining the association between the summary DCR score and functional impairment, and (2) classifying functional impairment using multimodal features from the DCR. The first goal was examined via adjusted risk ratios (ARR) derived from logistic regressions. The first logistic regression explored differences in functional impairment between individuals with DCR score = 0–1 (Red) versus 4–5 (Green). A second logistic regression explored these differences between individuals with a DCR score of 0 versus 5. Both logistic regressions included regressors for sex, age, and years of education. We also computed the Spearman correlation between DCR and FAQ scores.
For the second goal, we employed a ML approach to classify functional impairment. First, we split participants into training (80%) and test (20%) sets, ensuring similar rates of functional impairment across sets (n impaired: train set = 25%, test set = 27%). Predictors included the extended multimodal drawing and speech features with less than 15% of missing data, as well as age (a feature that is collected on every administration of the DCR). Missing predictor data on both training and test sets were imputed using the medians from the training set. For the classifier, we performed recursive feature elimination on 10-fold cross-validated random forests (5 repetitions) on the training set to identify the best model and feature set. Random forests were fitted using 22 features per split until the algorithm reached either 500 trees or an out-of-bag error estimate below 0.001. We evaluated model performance using traditional classification metrics (i.e., sensitivity, specificity, negative predictive value, positive predictive value, area under the receiver operating characteristic curve [AUC], and accuracy) on the held-out test set. These metrics were computed on two classification outputs: a binary classification and a three-class classification format. The binary classification was simply the predicted level of impairment by the ML algorithm (impaired versus unimpaired), with metrics based on optimized decision thresholds provided by the Youden statistic (i.e., the highest balance between sensitivity and specificity). 32 For the three-class format, we searched for a pair of thresholded predicted probabilities that would contain a new “Indeterminate” class. For each combination, we removed the resulting indeterminates and calculated performance on the impaired and unimpaired cohorts. We selected the threshold pair that maximized the AUC first and Youden statistic second, as long as the percentage of lost test data was below 25%. This procedure follows recent work detailing the performance of blood-based biomarkers for identifying AD pathology.33,34 Finally, we fitted a demographics model to compare as a baseline reference. This model included age, sex, years of education, race, and ethnicity as predictors, and followed the same random forest procedures outlined above.
Note that due to the class imbalance for the binary functional impairment outcome, we also fitted models that upsampled the number of functionally impaired individuals in the train set using bootstrap procedures. This approach did not provide an advantage to performance and, therefore, is not reported here.
As a final step, we examined potential demographic disparities in the ML predictions. Using the held-out test data, we first analyzed the FAQ scores of the predicted classes separately for Hispanics versus non-Hispanics, Whites versus non-Whites, Males versus Females, and those with low (<15 years) versus high (≥15 years) education levels. We employed a Poisson regression model on FAQ scores, with predictors for each demographic factor, the predicted cohort (impaired versus unimpaired), and their interactions. We also report the classification performance metrics described above for each of these demographic categories, except for AUC due to the observed low count of participants in certain demographic groups.
Results
Association between DCR and FAQ scores
We first assessed the relationship between DCR and informant-rated FAQ scores (Figure 1). An empirical cumulative distribution function (ECDF) of FAQ scores by DCR category (Green, Yellow, and Red) shows that, generally, individuals with lower DCR scores accounted for the highest percentage of FAQ scores indicative of functional impairment (Figure 1(A)).
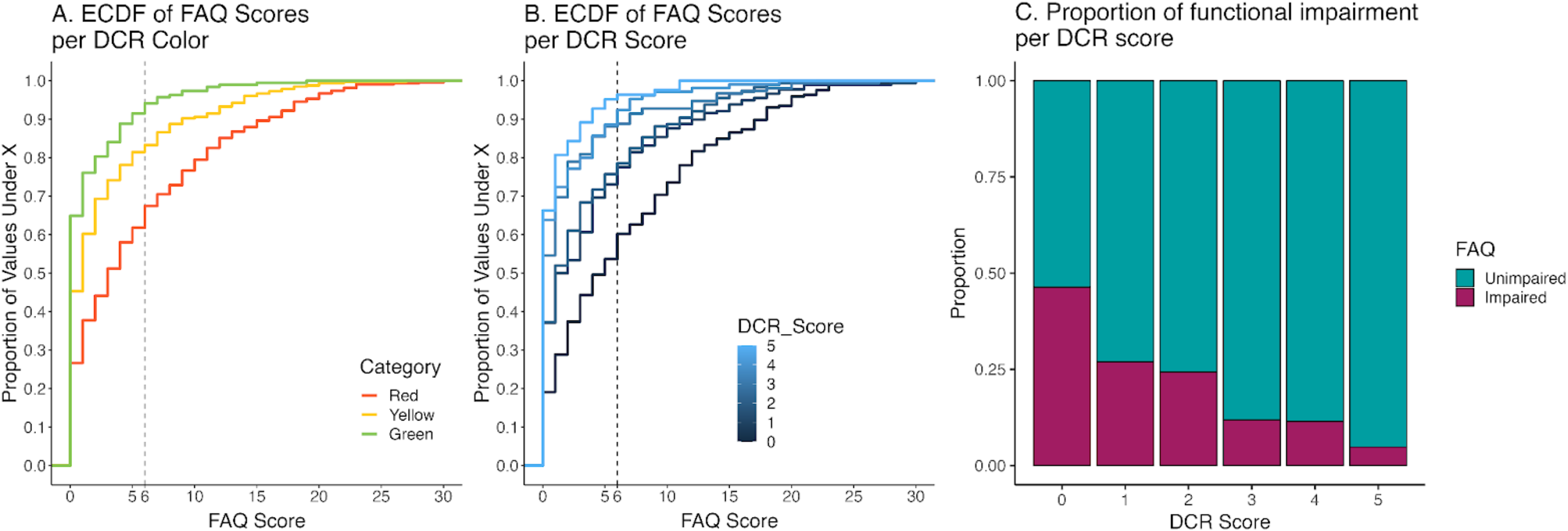
(A) Empirical Cumulative Distribution Function (ECDF) of FAQ scores by DCR category (Green, Yellow, and Red) demonstrating an increasingly higher proportion of individuals with FAQ scores indicative of mild or greater functional impairment (denoted by the dashed line, FAQ score ≥6) in individuals with DCR scores indicative of impairment (i.e., Red) compared to those with higher (Yellow or Green) DCR scores. (B) ECDF of FAQ scores by DCR scores. (C) Proportion of functionally unimpaired and impaired individuals (defined as FAQ score ≥6) per DCR score. Overall, these plots show that DCR scores are associated with functional impairment.
Approximately 38% of individuals with a Red score had FAQ scores equal to or above 6, compared with 18% of individuals with a Yellow score and 8% with a Green score. The pattern of increasingly higher functional impairment by DCR score was also noted in the ECDF of FAQ scores by DCR scores (ranging from 0–5; Figure 1(B)). Approximately 46% of individuals with a DCR score of 0 had FAQ scores equal to or above 6, compared with 24–27% of individuals with DCR scores of 1–2 and 5–11% of individuals with DCR scores of 3–5. Figure 1(C) shows that rates of functional impairment declined as DCR scores increased.
A logistic regression model classifying a binary functional impairment (impaired: FAQ score ≥6; unimpaired: FAQ score <6) based on the DCR-score categories showed that individuals in the Red category were five times more likely to be classified as impaired than those in the Green (ARR = 5.10, p < 0.0001). Participants in the Yellow category were twice as likely to be classified as impaired than those in Green (ARR = 2.12, p < 0.05). Age and sex were the only significant demographic predictors (ARR = 1.05 and ARR = 1.42 for Age and Males, respectively; both ps < 0.05), suggesting that older individuals and males were more likely to be classified as functionally impaired. A similar logistic regression comparing individuals with DCR scores of 0 and 5 (n = 329) showed that those with a DCR score of 0 were 17 times more likely to demonstrate functional impairment (ARR = 17.59, p < 0.0001; no significant demographic predictors). These results are in line with a significantly negative Spearman correlation between DCR and FAQ scores (Rho = −0.38, z = −11.95, p < 0.0001).
Classification of functional impairment
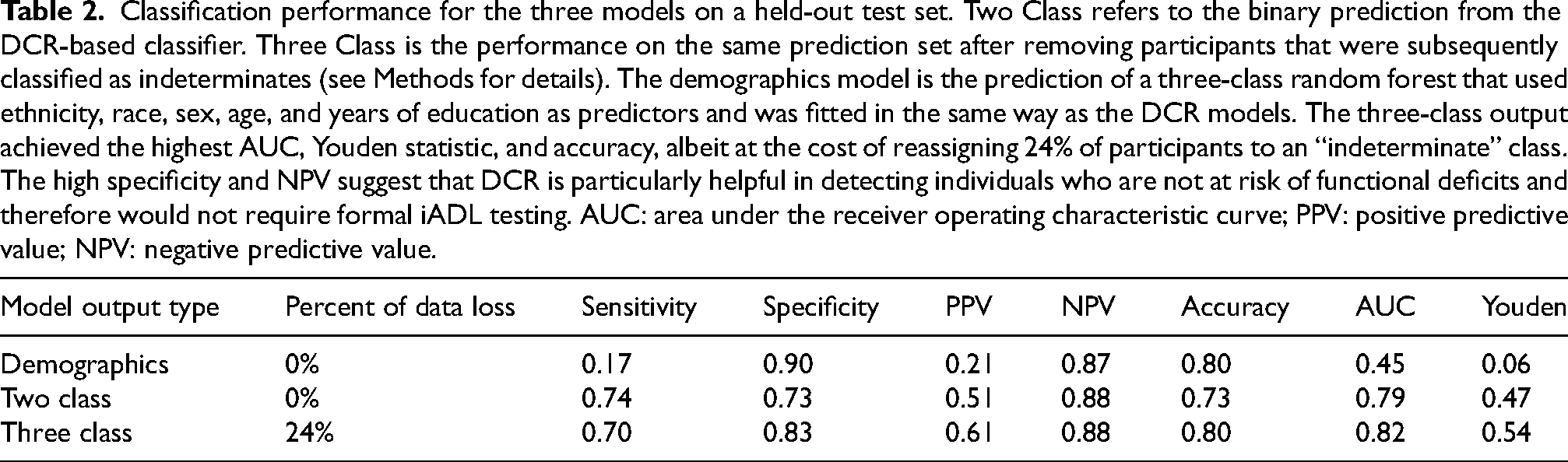
Classification model results were evaluated in two output formats: a binary output (impaired versus unimpaired) and a three-class output (impaired, indeterminates, and unimpaired; see Methods for details). Recursive feature elimination among 2000 multimodal features resulted in a subset of 500 predictors comprising drawing, speech, and memory performance. Among these, the most important predictors were the DCTclock summary score, those related to speech and drawing latency, and recall performance itself. Figure 2 displays the ROCs for all model outputs on the held-out test set, indicating that both two- and three-class classification outputs performed better than demographic information alone in classifying functional impairment. Table 2 shows their respective performance metrics for the DCR model outputs. A total of 53 participants (24.6%) were classified as indeterminates. Even though the two-class output already showed a strong ability to classify functional impairment, the three-class model improved upon most performance metrics, giving a higher Youden statistic (0.54), accuracy (0.80), and AUC (0.82). Specificity (0.83) and NPV (0.88) were especially high, suggesting that DCR is particularly helpful in ruling out functional impairment and thereby identifying individuals who would not require formal iADL testing.
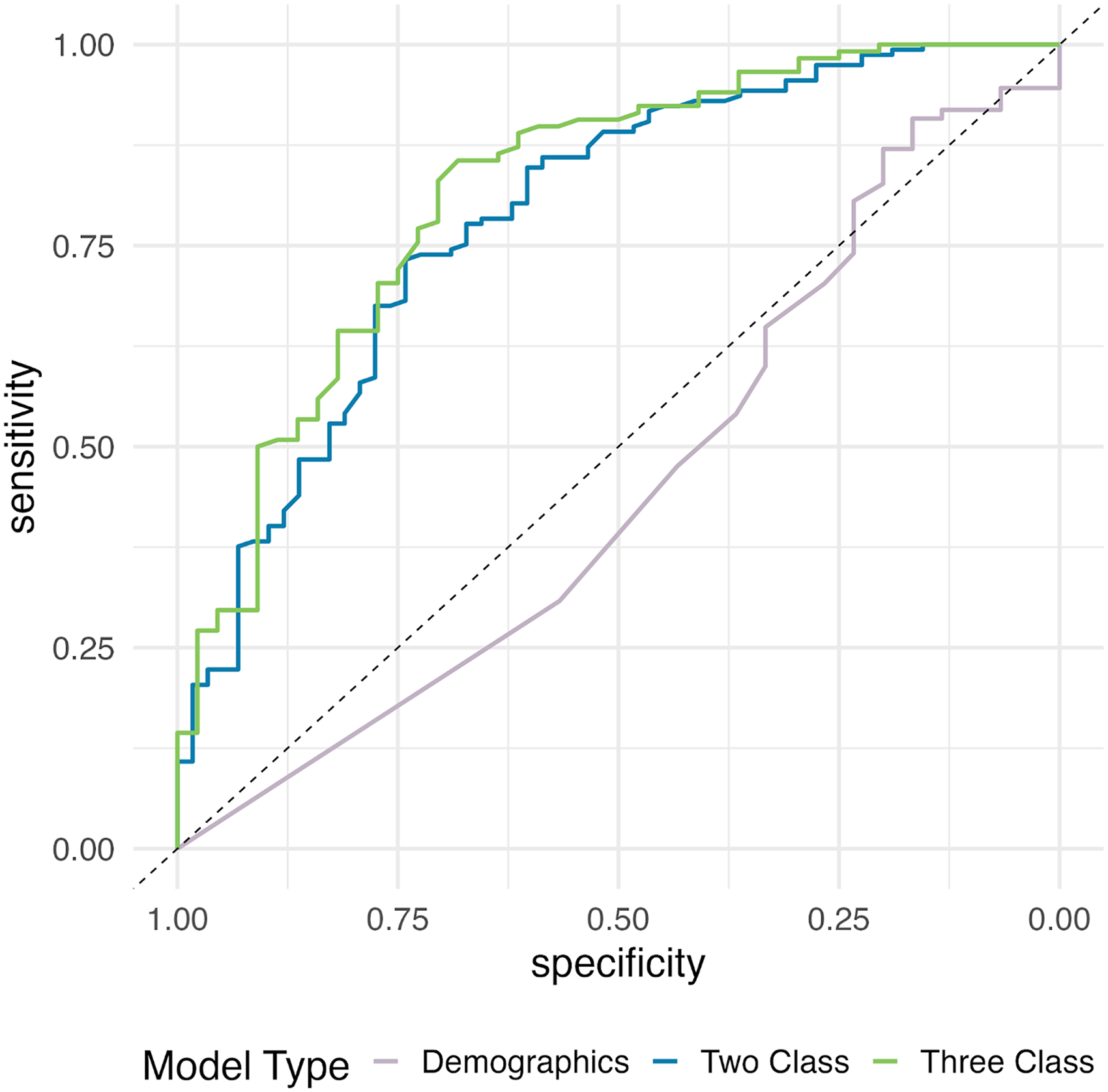
Receiver operating characteristic curves for classification on a held-out test set. Two Class refers to the binary prediction from the DCR-based classifier. Three Class is the performance on the same prediction set after removing participants that were subsequently classified as indeterminates (see Methods for details). The demographics model is the prediction of a three-class random forest that used ethnicity, race, sex, age, and years of education as predictors and was fitted in the same way as the DCR models. Both DCR classifications outperformed demographics, with the three-class model producing a higher AUC (0.82) than the two-class one (0.79). See Table 2 for other metrics.
Classification performance for the three models on a held-out test set. Two Class refers to the binary prediction from the DCR-based classifier. Three Class is the performance on the same prediction set after removing participants that were subsequently classified as indeterminates (see Methods for details). The demographics model is the prediction of a three-class random forest that used ethnicity, race, sex, age, and years of education as predictors and was fitted in the same way as the DCR models. The three-class output achieved the highest AUC, Youden statistic, and accuracy, albeit at the cost of reassigning 24% of participants to an “indeterminate” class. The high specificity and NPV suggest that DCR is particularly helpful in detecting individuals who are not at risk of functional deficits and therefore would not require formal iADL testing. AUC: area under the receiver operating characteristic curve; PPV: positive predictive value; NPV: negative predictive value.
Understanding indeterminates and demographic fairness
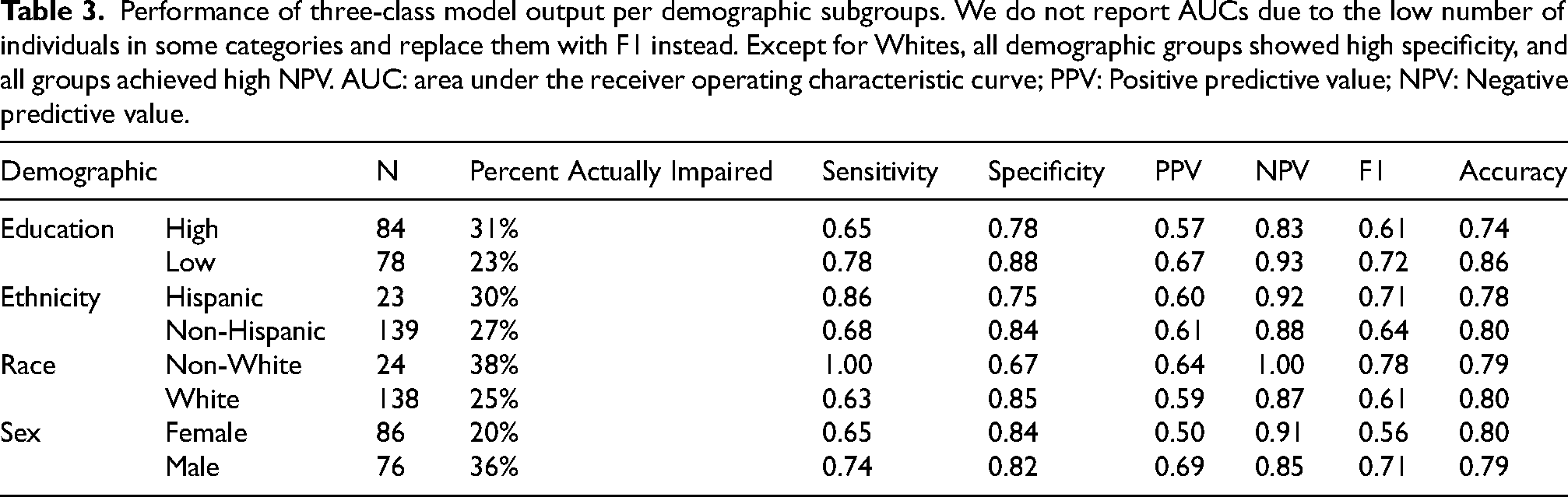
Indeterminates from the three-class model included 24% of the true positives and 25% of the true negatives from the held-out set. Figure 3 shows that differences in FAQ scores among the three classes predicted by the DCR met expectations regardless of demographic group (Supplemental Figure 1 shows the same information for the ground truth classes). A Poisson regression assessing the interaction in FAQ score differences between each demographic group and the DCR predictions (unimpaired and impaired only, n = 162) resulted in significant results only for Whites, whereby White individuals had smaller differences between the predicted impairment classes (z-value = −2.66, p < 0.01). This regression also resulted in the main effects of predicted class (z-value = 2.77, p < 0.001), Race (z-value = 2.89, p < 0.01), and Sex (z-value = 3.78, p < 0.001), indicating observed differences in FAQ scores between these demographic groups. Finally, Table 3 shows the three-class classification performance metrics per demographic group on the held-out test set (without AUC, given the low number of participants in some of these sub-groups). Except for Whites, all demographic groups showed high specificity, and all groups achieved high NPV. These numbers match the overall classification performance trends reported above. While the interactions in the Poisson regression should be interpreted with care due to the low number of observations, these results support the conclusion that predictions of functional impairment by the DCR are similar across demographic groups.
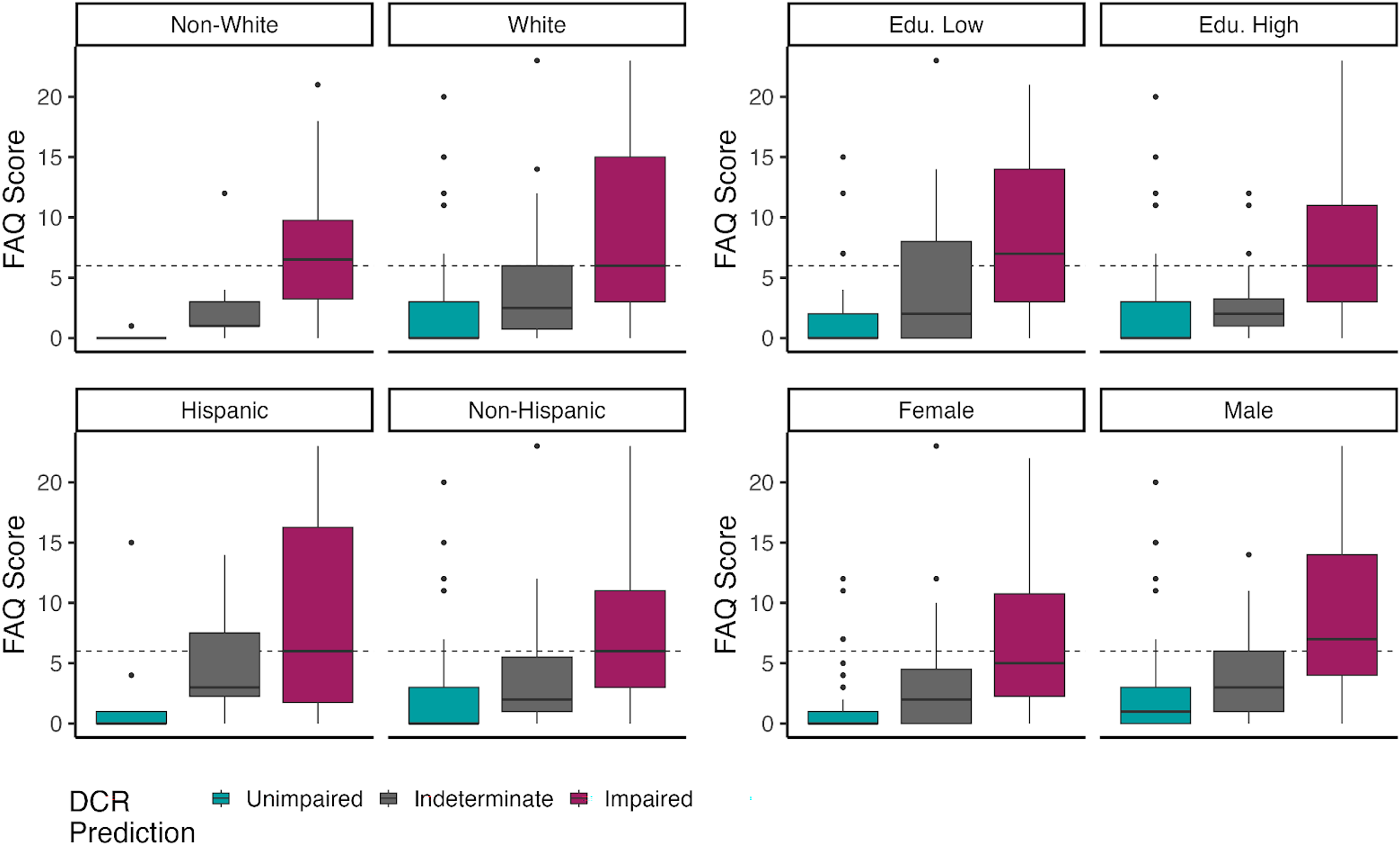
The plots show similar trends across demographics, where median scores among predicted impaired individuals (right-most box) were greater than those for predicted unimpaired (left-most box; middle box is indeterminate).
Performance of three-class model output per demographic subgroups. We do not report AUCs due to the low number of individuals in some categories and replace them with F1 instead. Except for Whites, all demographic groups showed high specificity, and all groups achieved high NPV. AUC: area under the receiver operating characteristic curve; PPV: Positive predictive value; NPV: Negative predictive value.
Discussion
Our results indicate that the DCR and its multimodal features achieve high classification performance of functional independence, as measured by the informant-based FAQ, in individuals with designations ranging from cognitively unimpaired to MCI and to DLAD. The summary DCR score scaled well with FAQ scores. This suggests that objective assessment of various cognitive domains and motor performance through the DCR can classify clinically meaningful levels of functional impairment, particularly helping clinicians triage those who may not need further functional dependence assessment. We found differences in functional impairment between cognitively impaired and unimpaired groups. This finding was expected since functional impairment typically increases with greater cognitive impairment and is needed for a dementia diagnosis. We also found that differences in FAQ scores between DCR-predicted cognitively impaired and unimpaired were similar between demographic groups, aligned well with ground truth, and mostly matched the classification performance of the undivided test set. However, whites had a smaller difference between classification groups than non-whites.
DCR's ability to detect cognitive impairment along with the present findings on the utility of the DCR to rule out functional impairment speaks to the utility of the DCR for differentiating between MCI and dementia.14,15
Further, this indicates that the DCR can be used to aid providers in taking the optimal next steps for the diagnosis and clinical management of a patient. The strong classification performance of the multimodal DCR on a held-out test set and its high specificity and negative predictive value suggests that the DCR can be particularly helpful in determining who does not need further confirmatory functional impairment evaluation. It also indicates that an individual unlikely to have clinically relevant functional impairment can be reassured that, by definition, they are unlikely to meet the criteria for dementia, and they also are likely to be safe returning to a future visit without the need for an informant. Depending upon clinical workflows, those with lower scores indicating functional impairment could be referred for follow-up functional independence assessments, such as the FAQ or Functional Assessment Staging Test (FAST), thus optimizing triage and resource allocation in the primary care setting.35,36
Another implication of our findings relates to scaling emerging therapeutics. Given the reported success of recent anti-amyloid therapy clinical trials, therapeutic agents targeting the removal of amyloid from the brain have shown beneficial effects in slowing down the trajectory of cognitive decline.37,38 Particularly for those in earlier stages of cognitive decline, a measurable overall clinical benefit, as demonstrated by everyday activities, is a useful metric of clinical meaningfulness. 39 Assessing cognitive impairment with a brief digital cognitive assessment while concurrently ruling out functional impairment can streamline access to these novel therapeutic interventions to the individuals most likely to be the best responders. In addition, it can enable individuals to better weigh potential risks and financial implications, as well as considerations on adhering to intensive treatment protocols, and help to quickly establish a lack of suitability for other individuals who can go on to consider other alternatives such as lifestyle interventions. Thus, the ability to concurrently infer insights on cognitive performance and iADLs may be useful in the treatment and monitoring of people receiving or considering taking these drugs.
Importantly, the relatively small number of individuals classified by our models as indeterminates were evenly divided between true positives and true negatives. The practical implication of this group is that there is a stronger need to apply a provider's clinical judgment to determine whether a follow-up evaluation is needed. Alternatively, these individuals may benefit from closer observation to determine the likelihood and timing of follow-up evaluation and potential treatment. Ultimately, this should be left up to the care provider but, the DCR again provides utility in elucidating the cases that would benefit from potential follow-up evaluation or closer observation.
Limitations of the administration of any self/informant-reported survey include the reliance on subjective ratings. In older adults, these limitations may be compounded by potential cognitive impairment in which an informant-rated survey may be a better option. Although self-reports of function may be confounded due to an individual's cognitive status, studies have shown moderate agreement between self- and informant-reported measures of function in people with cognitive impairment.11,40 The low positive predictive value reported here is expected given the low incidence of functional impairment in the study sample (present in less than 20% of participants). This low incidence of positive cases limited our models’ abilities to identify individuals who are likely to have clinically relevant functional impairment (i.e., those who should bring an informant to perform a validated functional impairment assessment). Instead, the sample from the present study allowed us to concretely answer a separate important question (i.e., could the DCR results be used to reassure individuals, their clinicians, and care partners that they are unlikely to have a functional impairment?). However, studies to answer the separate issue of sensitivity are planned with study samples that have a higher incidence of functional impairment. In addition, our capacity to detect subtle graphomotor processes and speech-related signals suggests that future work based on the DCR will achieve higher predictive power via feature engineering.
Conclusion
The DCR, a self-administered, automatically scored digital test of cognition, can also classify informant-based clinically relevant levels of functional impairment in older adults in around 3–5 min. The high negative predictive value emphasizes the utility of the DCR to dispel concerns of impairment of iADLs/ADLs or dementia. We found strong links between DCR and FAQ, which resulted in the robust ability of the DCR to determine individuals who are unlikely to be functionally impaired. This can help primary-care providers streamline the clinical decision-making, triage, and intervention planning along the spectrum of MCI and early dementia.
Supplemental Material
sj-docx-1-alz-10.1177_13872877241290123 - Supplemental material for Detecting functional impairment with the Digital Clock and Recall
Supplemental material, sj-docx-1-alz-10.1177_13872877241290123 for Detecting functional impairment with the Digital Clock and Recall by Marissa Ciesla, Claudio Toro-Serey, Ali Jannati, Russell E Banks, Joyce Gomes-Osman, John Showalter, David Bates, Sean Tobyne and Alvaro Pascual-Leone in Journal of Alzheimer's Disease
Footnotes
Acknowledgments
The authors thank the participants, organizers, and staff of the GAP Bio-Hermes-001 study.
ORCID iDs
Author contributions
Marissa Ciesla (Methodology; Writing—original draft; Data Interpretation); Claudio Toro-Serey (Formal analysis; Methodology; Visualization; Writing—original draft; Data Interpretation); Ali Jannati (Methodology; Writing—review & editing; Data Interpretation); Russell E. Banks (Writing—review & editing; Data Interpretation); Joyce Gomes-Osman (Writing—review & editing); John Showalter (Writing—review & editing; Data Interpretation); David Bates (Conceptualization; Project administration; Writing—review & editing); Sean Tobyne (Methodology; Writing—review & editing; Data Interpretation); Alvaro Pascual-Leone (Conceptualization; Methodology; Writing—review & editing; Data Interpretation).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Bio-Hermes-001 study was organized by the Global Alzheimer's Platform (GAP) and funded by the Alzheimer's Drug Discovery Foundation (ADDF). Neither GAP nor ADDF had any influence on the analysis, decision to publish, or manuscript preparation.
Declaration of conflicting interests
DB is a co-founder of Linus Health and declares ownership of shares or share options in the company. APL is a co-founder of Linus Health and declares ownership of shares or share options in the company. APL serves as a paid member of the scientific advisory boards for Neuroelectrics, Magstim Inc., TetraNeuron, Skin2Neuron, and MedRhythms. MC, CTS, AJ, RB, JGO, JS, and ST are employees of Linus Health and declare ownership of shares or share options in the company. DB, APL, ST, AJ, and JGO are listed as inventors on a pending patent assessing central nervous system functionality using a digital tablet and stylus. APL is further listed as an inventor on several issued and pending patents on the real-time integration of transcranial magnetic stimulation with electroencephalography and magnetic resonance imaging, and applications of noninvasive brain stimulation in various neurological disorders, as well as digital biomarkers of cognition and digital assessments for early diagnosis of dementia.
Data availability
The data that support the findings of this study were collected as part of the Bio-Hermes-001 study (ClinicalTrials.gov Identifier: NCT04733989) and are governed by the Global Alzheimer's Platform (GAP) consortium agreement. Data will be made available via the Alzheimer's Disease Data Initiative (ADDI) Workbench in the future and at the discretion of GAP. All requests for data access should be made directly to GAP. The code used to calculate the reported results is available from Linus Health, Inc. upon reasonable request and with the permission of Linus Health, Inc. Usage restrictions apply to the availability of this code, which is not immediately publicly available.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.