
Abstract
Background
Although COVID-19 has been linked to worse acute outcomes in patients with some neurodegenerative disorders, its long-term impact on dementia remains unclear.
Objective
To investigate the outcomes of COVID-19 survivors with dementia.
Methods
This retrospective study evaluated 9806 patients with dementia in the Montefiore Health System (January 2016 to July 2023). Comparisons were made between dementia patients with and without a positive SARS-CoV-2 polymerase-chain-reaction test who had a follow-up at least two weeks post-infection. Outcomes included all-cause mortality, major adverse cardiovascular events (MACE), new-onset dysphagia, dyspnea, fatigue, new-onset sleep disturbances, altered mental status, first-time fall, headache, new-onset depression, and new-onset anxiety. Adjusted hazard ratios (aHR) were computed adjusting for age, sex, race, ethnicity, and pre-existing comorbidities.
Results
Dementia patients with COVID-19 were younger, more likely to be male, and had a higher prevalence of major pre-existing comorbidities compared to those without COVID-19. Patients who survived acute COVID-19 were more likely to die than non-COVID controls after adjusting for covariates (aHR = 1.65 [1.43, 1.91]). COVID-19 was significantly associated with higher risk of MACE (aHR = 1.58 [1.41, 1.78]), new-onset dysphagia (aHR = 1.64 [1.42, 1.91]), dyspnea (aHR = 1.27 [1.12, 1.44]), fatigue (aHR = 1.42 [1.22, 1.65]), new-onset sleep disturbances (aHR = 1.36 [1.15, 1.60]), altered mental status (aHR = 1.36 [1.16, 1.59]), and first-time fall (aHR = 1.34 [1.09, 1.65]).
Conclusions
COVID-19 increases the risk of mortality and other adverse health outcomes in dementia patients. These findings highlight the need for closer follow-up and management strategies for dementia patients post-COVID-19.
Keywords
Introduction
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) responsible for the COVID-19 pandemic has been linked with a broad spectrum of chronic sequelae. 1 In patients with neurodegenerative diseases, COVID-19 could accelerate disease progression and result in worse long-term outcomes compared to individuals with neurodegenerative diseases but without a history of SARS-CoV-2 infection. There is evidence that SARS-CoV-2 particles can enter brain cells via the angiotensin converting enzyme 2 (ACE2) receptor, invade endothelial cells, trigger neuroinflammation and dysregulated host-immune response, 2 and disrupt the blood-brain barrier (BBB). 3 At the systemic level, cardiovascular and pulmonary distress during acute COVID-19 could result in hypotension, hypoxia and cerebral ischemia.4–7 Hypercoagulability in severe COVID-19 could result in cerebral embolism and microinfarcts. 8 Together, these COVID-19 related insults could exacerbate neurodegenerative symptoms such as dysphagia, dyspnea, fatigue, sleep disturbances, altered mental status, first-time falls, headaches, depression, and anxiety,9–16 as well as increase incidence of major cardiovascular events (MACE) and mortality 17 long after acute COVID-19 symptoms have resolved.
A few studies have reported the associations of SARS-CoV-2 infection and pre-existing neurodegenerative18,19 and cerebrovascular disorders. 20 Multiple sclerosis (MS) patients with COVID-19 were at higher risk of adverse clinical outcomes compared to MS patients without COVID-19,21–31 and Parkinson's disease patients with COVID-19 were at higher risk of adverse clinical outcomes compared to Parkinson's disease patients without COVID-19.32–36 MACE was also associated with a history of SARS-CoV-2 infection, 17 severity of infection, 37 and post-infection mortality risk. 38
The goal of this study was to evaluate the long-term outcomes of patients with pre-existing dementia up to three and a half years post-infection. Outcomes included post-infection mortality, MACE, and as well as new-onset dysphagia, dyspnea, fatigue, sleep disturbances, altered mental status, first-time falls, headaches, depression, and anxiety. Our data came from the Montefiore Health System, which serves a large, low-income, diverse population in the Bronx and its environs, an epicenter of the early COVID-19 pandemic and subsequent surges of infection. Understanding the interplay between SARS-CoV-2 infection and pre-existing dementia may be helpful for providing proactive care to at-risk patients.
Methods
Data sources
This retrospective cross-sectional single-center study was approved by the Einstein-Montefiore Institutional Review Board with an exemption for informed consent (#2021-13658). Data extraction queried records from Jan 1, 2016 to Jul 1, 2023 from the Montefiore Health System, which consisted of multiple hospitals in the Bronx, the lower Hudson Valley, and Westchester County. Data were extracted as described previously.39–48
Study cohort
At the index date, 21,183 individuals had pre-existing dementia. For COVID-19 patients, the index date was defined as the date of the first positive COVID-19 polymerase chain reaction (PCR) test. For non-COVID patients, the index date was defined as the first date patients came across our health system after March 1, 2020 (contemporary controls). Both groups had to return to our health system 14 days after the index date to be included. The follow-up time was up to three and a half years post-infection, with an average follow-up time of 2.8 years post-index date.
Variables
Demographic data included age at index date, sex, race, and ethnicity. Pre-existing comorbidities included hypertension (HTN), type-2 diabetes (T2D), chronic obstructive pulmonary disease (COPD), asthma, congestive heart failure (CHF), chronic kidney disease (CKD), and coronary artery disease (CAD) that were diagnosed at or prior to the index date. Obesity was defined as a body mass index of 30+ or a diagnosis of obesity from any cause. Tobacco use status was defined as the patient self-reporting tobacco use prior to or at index date. A list of diagnostic codes used to define comorbidities is available in Supplemental Table 1.
To assess the severity of COVID-19, data about corticosteroid (hydrocortisone, methylprednisolone, dexamethasone, and prednisone) and antiviral drug (ritonavir and remdesivir) prescriptions for the treatment of COVID-19, COVID-19 hospitalization status, and critical illness (treated with intensive care unit or invasive mechanical ventilation) were collected.
Outcomes
The primary outcomes included all-cause mortality 14 days or later after index date and MACE, defined as the composite of stroke, myocardial infarction, new-onset heart failure, and cardiogenic shock) 30 days post-index date. The secondary outcomes included developing the following conditions or symptoms 30 days or more post-index date: (i) new-onset dysphagia, ii) dyspnea, iii) fatigue (patient-reported symptom), iv) new-onset sleep disturbances (idiopathic insomnia, irregular sleep-wake pattern, or central sleep apnea), (v) altered mental status, vi) first-time fall, vii) headache (idiopathic migraine or headache), viii) new-onset depression (major depressive disorder diagnosis; or PHQ-9 score of 10 or higher), and ix) new-onset anxiety (organic or generalized anxiety disorder diagnosis; or GAD-7 score of 10 or higher; or GAD-2 score of 3 or higher). Those with a history of dysphagia, sleep disturbances, falls, migraines, depression, and anxiety at index date were excluded from the analysis of the respective outcome.
Analysis and statistics
Python version 3.10.12 and the lifelines package, the survival, survminer, and cmprsk packages in RStudio version 4.3.2 (RStudio, PBC, Boston, MA, USA), and GraphPad Prism 9 version 10.1.1 (GraphPad Software, Boston, MA, USA) were used for data processing and statistical analyses. Group comparison of categorical variables used, the chi-square test, and group comparison of continuous variables used the independent t-test. Kaplan-Meier curves and log-rank analysis were performed for all-cause mortality. Cumulative incidence function and Fine-Gray sub-distribution hazards model analysis were performed for post-index date for all other secondary outcomes associated with SARS-CoV-2 infection. In the univariate analysis, hazard ratios (HR) were computed using the Fine-Gray model to account for mortality as a competing risk for developing non-fatal outcomes. 49 To adjust for other covariates, the multivariate Cox proportional hazards model was used to calculate adjusted hazard ratios (aHR) and 95% confidence interval (CI) for outcomes. The covariates included SARS-CoV-2 infection status, sex, race, ethnicity, and HTN, T2D, COPD, asthma, CHF, CKD, CAD, obesity, and tobacco use. The Cox proportional hazards model captures the relative risk of the event occurring at a given moment, assuming other risks are censored. The Fine-Gray model shows the cumulative probability of the event happening over time, considering that competing risks (such as death) may preclude the event of interest. 50
Results
Figure 1 shows the patient selection flowchart. Among the 21,183 patients with pre-existing dementia from Jan 1, 2016 to Jul 1, 2023, 3119 were infected with COVID-19 and 18,064 were non-COVID. 1988 COVID-19 survivors returned to our health system along with 7818 non-COVID controls.
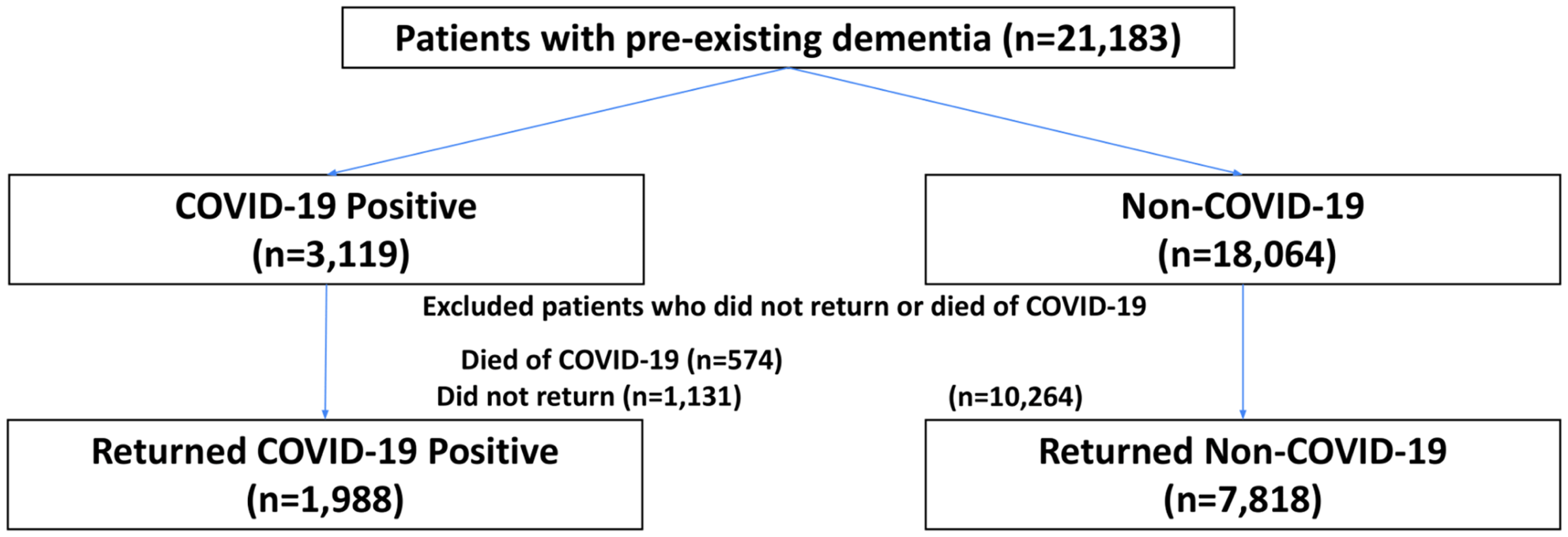
Patient selection flowchart.
Table 1 shows the profiles of patients with pre-existing dementia who experienced SARS-CoV-2 infection and those who did not. Compared to non-COVID patients, COVID-19 patients were younger (78.75 versus 80.57 years, p < 0.005), more likely to be Black and other races (p < 0.0005 for all), and more likely to have all major comorbidities (p < 0.05 for all). Most of pre-existing dementia were non-specific (59.91%), 26.41% were Alzheimer's disease, 20.0% were vascular dementia. Most (86.97%) were hospitalized for COVID-19, only 3.57% had critical illness, 28.77% were treated with steroid for COVID-19, 33.55% were treated with antiviral medications.
Profiles of patients with pre-existing dementia with and without COVID-19.
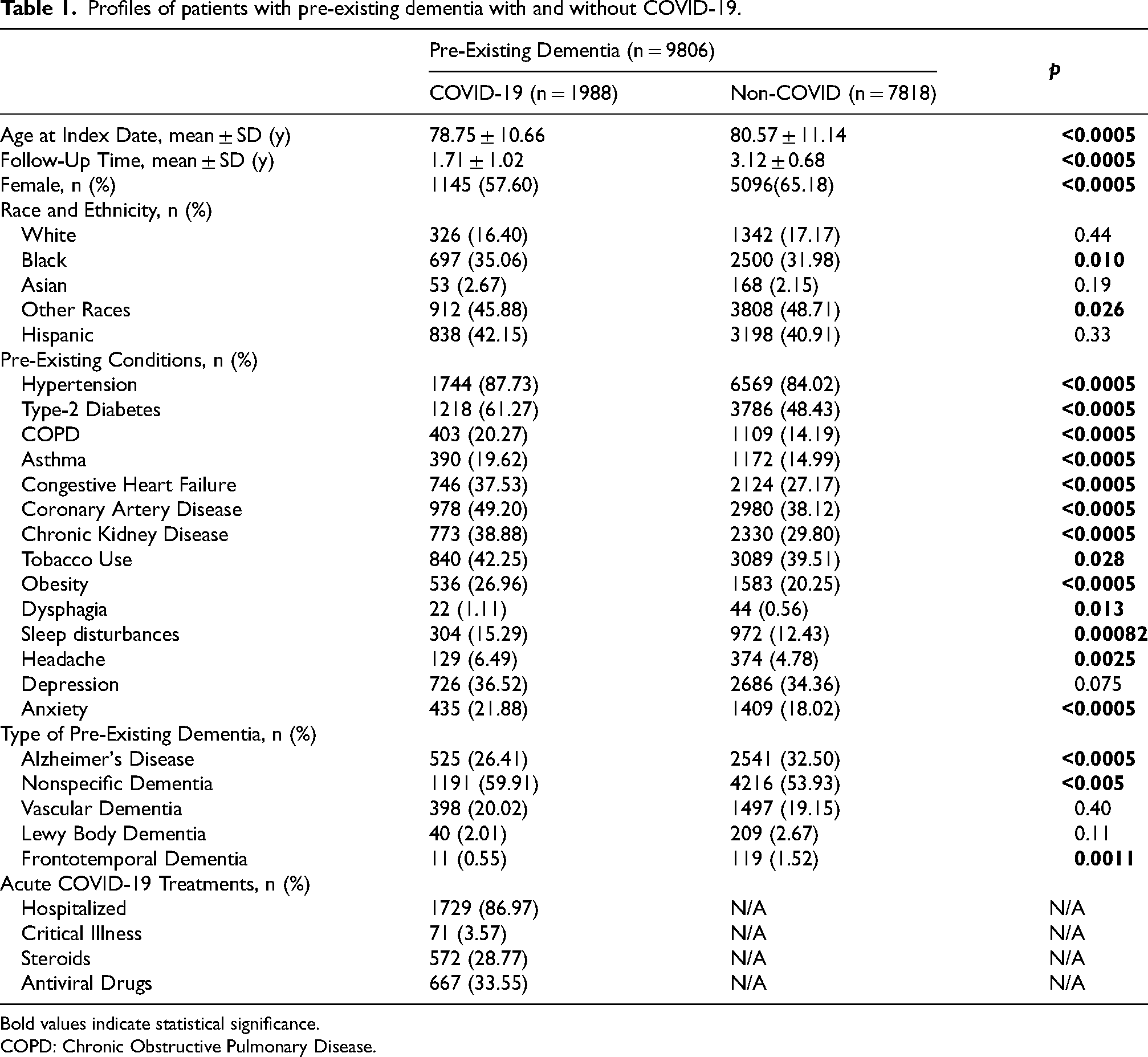
Bold values indicate statistical significance.
COPD: Chronic Obstructive Pulmonary Disease.
All-cause mortality by Kaplan-Meier analysis up to three and a half years post-infection was significantly different between COVID-19 and non-COVID groups (unadjusted log-rank HR = 1.86 [CI:1.61, 2.15] p < 0.0005) (Figure 2). Table 2 shows the multivariate Cox proportional hazard ratios for all-cause mortality up to three and a half years post-index date. Dementia patients with COVID-19 had a higher risk of mortality compared to non-COVID patients (adjusted HR = 1.65 95%CI [1.43, 1.91], p < 0.005) compared to dementia patients without COVID-19. Age was a significant risk factor with a 2% increased risk for every year of age (adjusted HR = 1.02 95%CI [1.01, 1.02], p < 0.005). Those with CHF (aHR = 1.52), COPD (aHR = 1.27), CKD (aHR = 1.30), and CAD (aHR = 1.16) were at higher risk of death (p < 0.05 for all).
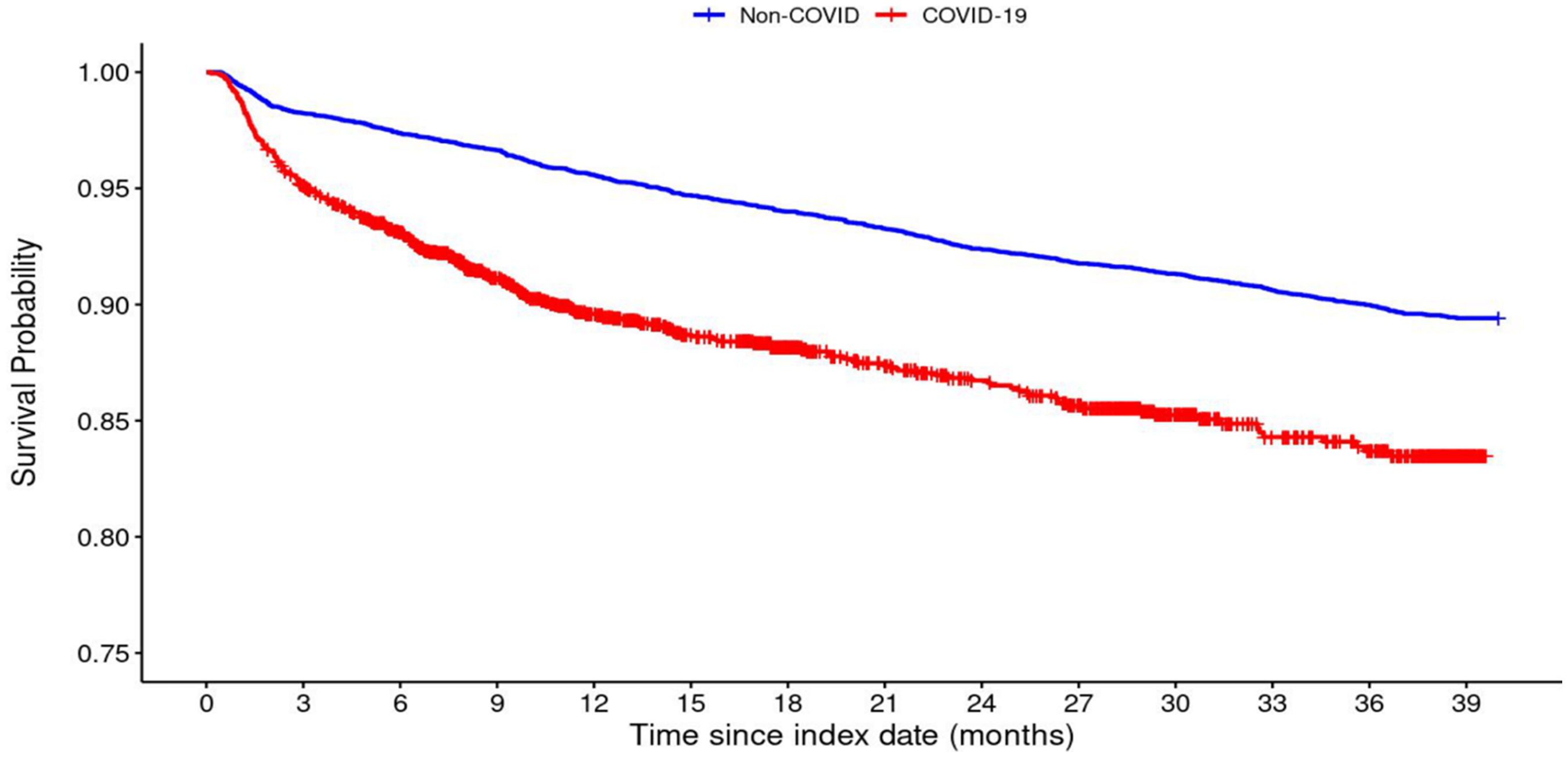
Kaplan-Meier curve of all-cause mortality fourteen days or more post-index date between COVID-19 and non-COVID patients. (unadjusted log-rank HR = 1.86 [CI:1.61, 2.15] p < 0.0005).
Multivariate Cox proportional hazards model hazard ratios for mortality.
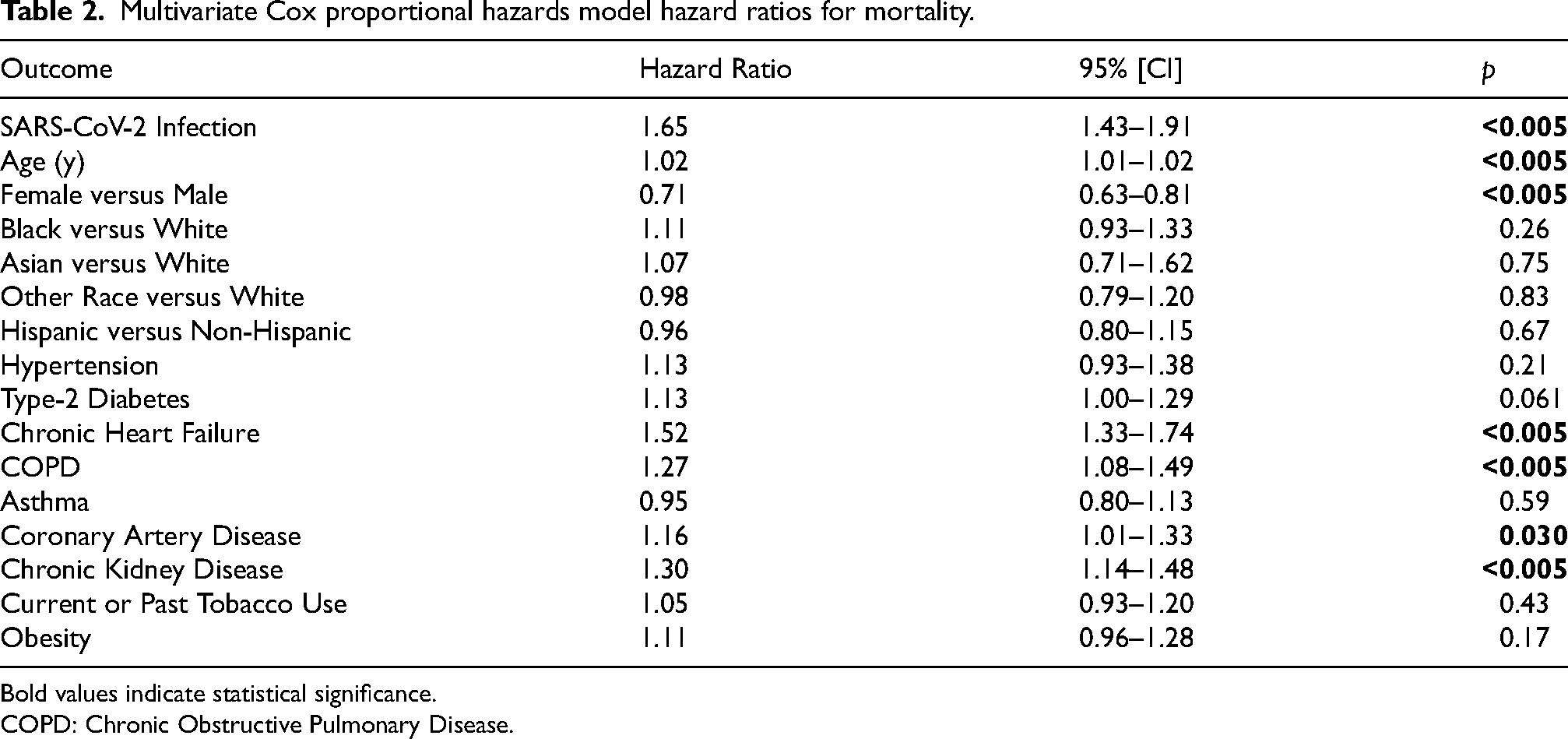
Bold values indicate statistical significance.
COPD: Chronic Obstructive Pulmonary Disease.
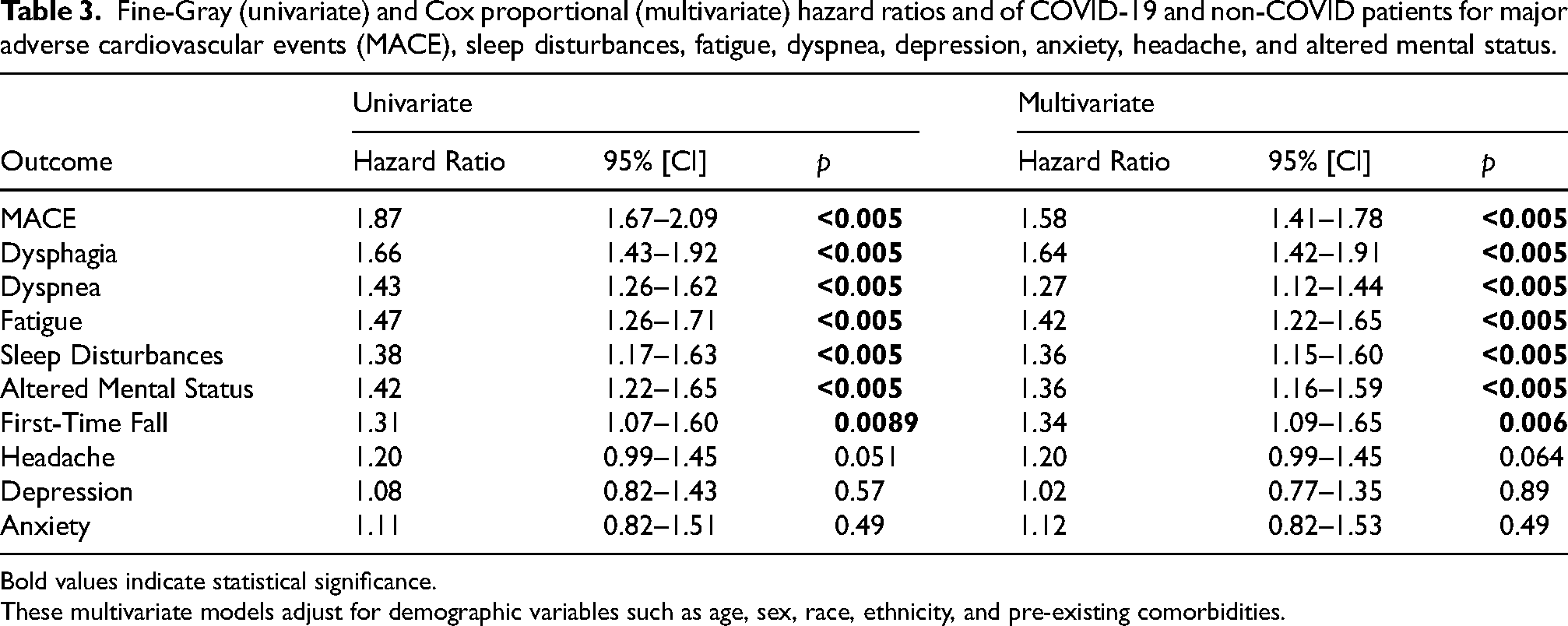
In addition, cumulative incidences for post-index date MACE, sleep disturbances, fatigue, dyspnea, depression, anxiety, headache, and altered mental status and their Fine-Gray hazard ratios were computed (Figure 3). Table 3 shows the univariate and multivariate hazard ratios for these outcomes post-index date. Patients with COVID-19 had a significantly higher risk for MACE (HR = 1.87 [CI:1.67, 2.09], p < 0.005) and developing new dysphagia, dyspnea, fatigue, sleep disturbances, altered mental status, and falls (p < 0.05 for all). In addition, the results of analysis adjusting only for demographic variables are available in Supplementary Table 2 for comparison.
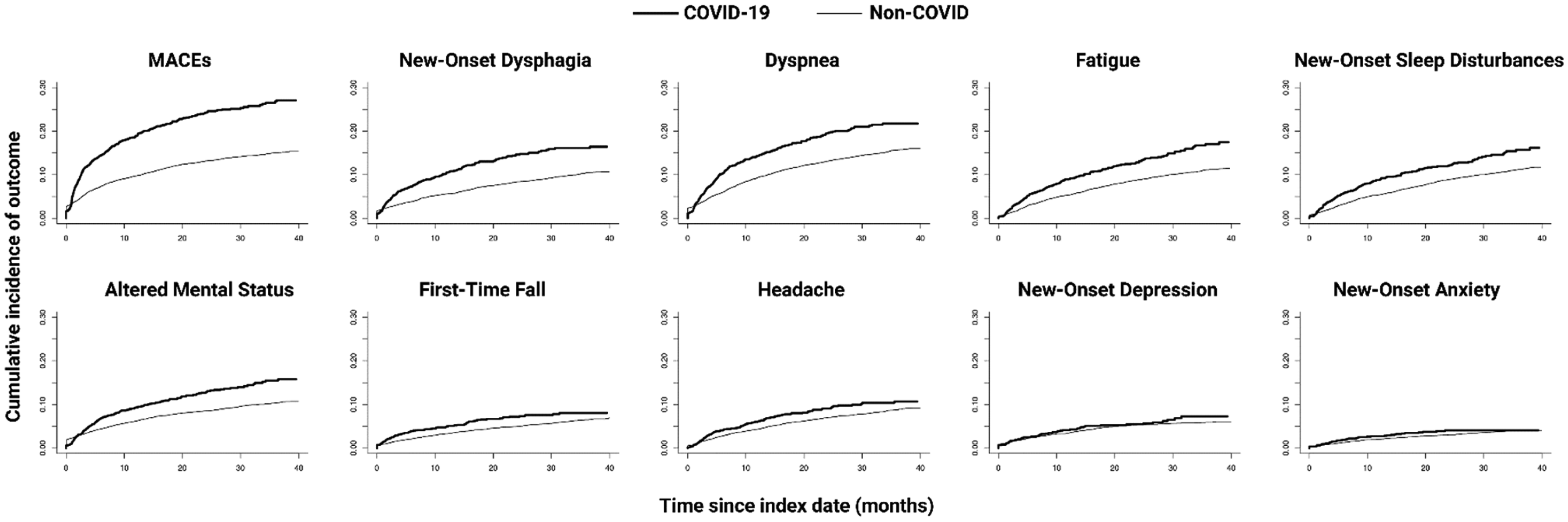
Cumulative incidence curves of post-index date major adverse cardiovascular events (MACE), sleep disturbances, fatigue, dyspnea, depression, anxiety, headache, and altered mental status.
Fine-Gray (univariate) and Cox proportional (multivariate) hazard ratios and of COVID-19 and non-COVID patients for major adverse cardiovascular events (MACE), sleep disturbances, fatigue, dyspnea, depression, anxiety, headache, and altered mental status.
Bold values indicate statistical significance.
These multivariate models adjust for demographic variables such as age, sex, race, ethnicity, and pre-existing comorbidities.
Discussion
This study characterized the clinical outcomes of dementia patients with and without COVID-19 up to three and a half years post-pandemic in an underserved inner-city population. SARS-CoV-2 infection was associated with increased risks of death, MACE, dysphagia, dyspnea, fatigue, altered mental status, sleep disturbances, and first-time fall.
Mortality
Risk of mortality posted by COVID-19 (aHR = 1.65 [1.43, 1.91]) in dementia patients was higher than that of CHF (aHR = 1.52 [1.33, 1.74]), COPD (aHR = 1.27 [1.08, 1.49]), CKD (aHR = 1.30 [1.14, 1.48]), and CAD (aHR = 1.16 [1.01, 1.33]), which is concerning. Additional studies are needed to confirm these findings.
This cohort had high prevalences of comorbidities, and these patients might have had more frequent hospital visits and were more likely to have adverse outcomes reported in the electronic health records. Moreover, interactions between COVID-19 and pre-existing comorbidities could also contribute to worse outcomes. In addition, COVID-19 could also exacerbate the effects of comorbidities (such as CHF, CAD, and CKD) that are highly prevalent in our cohort, further contributing to adverse outcomes. In our multivariate analysis these contributions were accounted for, and COVID-19 status remained an independent risk factor for worse outcomes, although residual unintentional biases could exist in patient selection in such retrospective studies.
Other outcomes
COVID-19 patients in our cohort were also at increased risks of developing dysphagia, dyspnea, fatigue, sleep disturbances, altered mental status, and first-time fall. Although these outcomes are not specific to dementia disease progression, epidemiological studies have shown that dementia patients are at an elevated risk of experiencing these conditions compared to age-matched controls.51–53 Neurodegeneration can lead to impaired muscle coordination required for swallowing (dysphagia) 12 and damage to circuits necessary for restful sleep (sleep disturbances). 54 Dementia patients are also at an elevated risk of falls, 13 and more frequent acute episodes of delirium (altered mental status).15,16 Dyspnea 55 and fatigue, 56 have been previously associated with long-COVID.11,57–59 The hypoxic 60 and inflammatory61–63 effects of acute COVID-19, in addition to reduced physical activity and isolation, 64 can exacerbate neuronal damage and neuroinflammation in dementia patients. These factors may be leading to accelerated dementia disease progression,6,65–67 which may manifest itself as elevated risk of new-onset of dysphagia, sleep disturbances, and falls, in addition to altered mental status and fatigue.
Sex and age differences
Dementia is more prevalent in females 68 as observed in our cohort. However, there were relatively more males in COVID-19 cohort compared to the non-COVID-19 cohort (42.40 versus 34.82, p < 0.0005). Male sex was associated with an increased risk of long-term mortality (aHR = 1.41 [1.23, 1.59]). While males have been shown to be more likely to exhibit worse acute COVID-19 outcomes,69–72 this is the first report of increased susceptibility to long-term mortality in male dementia patients. Several factors likely contribute to this sex difference. Biologically, women tend to have stronger immune responses to viruses, partially due to higher levels of hormones like estrogen, which may offer some protection against the virus. 73 Conversely, testosterone in men may suppress immune responses, making them more vulnerable. 74 Behavioral and lifestyle factors also play a role.
Dementia patients with COVID-19 were on average slightly younger compared to those without COVID-19 (78.75 versus 80.57 years, p < 0.005). Although this difference was statistically significant due to large sample sizes and the difference was small and unlikely to have clinical significance.
Potential mechanisms of action
Severe SARS-CoV-2 infection exerts a complex array of physiological stressors that can exacerbate dementia by impacting multiple organ systems and increasing the risk of neurological deterioration. The virus could trigger a severe systemic inflammatory response characterized by hyperinflammation, dysregulated immune function,75,76 and the release of pro-inflammatory cytokines, 77 which can disrupt the BBB and promote neuroinflammation. 78 This neuroinflammatory state has been associated with increased amyloid-beta production and tau hyperphosphorylation, both of which are hallmarks of Alzheimer's disease and other dementias.79,80 Moreover, COVID-19-related hypercoagulability can manifest as thrombosis, which could result in cerebral microinfarcts and hemorrhagic strokes, further compromising cognitive function.81–83 These ischemic events could lead to white-matter damage (visible as white-matter hyperintensities) which contribute to cognitive decline.84,85 The hemodynamic instability associated with severe COVID-19—including episodes of hypotension and hypoxia—could further contribute to cerebral hypoperfusion, further exacerbate neurodegeneration in vulnerable brain of patients with dementia.86–90
Additionally, respiratory damage and persistent pulmonary complications can lead to chronic hypoxemia, resulting in reduced oxygen supply to the brain. 91 Chronic hypoxemia has been linked to hippocampal atrophy and memory impairment, thereby worsening the cognitive deficits in dementia patients. 92 The metabolic93,94 and cardiovascular disruptions 17 seen in severe COVID-19 may also contribute to systemic inflammation and oxidative stress, creating a milieu that is particularly harmful for individuals with dementia, who may already have compromised neurovascular integrity and an impaired ability to repair neuronal damage.
These pathophysiological changes are especially concerning for elderly dementia patients, who often have multiple comorbidities, such as HTN, T2D, or cardiovascular disease, making them more susceptible to severe COVID-19 outcomes. 95 Consequently, these cumulative insults not only increase the risk of mortality and MACE but also potentiate neurodegenerative processes, thereby accelerating dementia progression and cognitive decline.
Comparison with other neurodegenerative diseases
To our knowledge, there are no studies comparing the long-term outcomes of dementia patients with and without COVID-19 to date. Similar studies on MS found COVID-19 to be associated with long-term worsening of MS disability, 29 higher risk of developing new magnetic resonance imaging (MRI) lesions, 28 higher rate of admission for neurological symptoms, 27 worsening of neurologic outcomes, 30 and higher risk of mortality and optic neuritis. 31 Prior studies found MS patients with COVID-19 had worse long-term outcomes than MS patients without COVID.21–31 MS patients are on average younger compared to dementia patients.96,97 MS is an autoimmune disease 98 and COVID-19 could trigger dysregulated host-immune responses and induce hyperinflammation,75,76 resulting in immune cells migration through the BBB. 99 This may exacerbate damage to myelin, resulting in acute MS disease activity and white matter hyperintensities on MRI, which has been observed in MS patients with COVID-19.26,28 In contrast, dementia pathogenesis is more gradual and less likely to involve the same acute episodes of immunological insult. Dementia patients may be more susceptible to respiratory and cardiovascular stress, leading to hypoxia, stroke, or microinfarcts,100–103 resulting in accelerated brain atrophy and cortical thinning 104 and cerebrovascular dysfunction. 105
Strengths and limitations
Strengths of this study included novelty in studying the long-term effects of COVID-19 on dementia patients with a non-COVID control group, large sample size, long follow-up time, and a diverse and underserved population in the Bronx. It is possible some patients with dementia might have not received a diagnostic code in our health system. However, this misclassification occurred in both COVID-19 and non-COVID-19 cohort and is thus unlikely to alter the overall conclusions. Our cohort did not consist of the usual distribution of dementia subtypes. It is possible patients with Alzheimer's disease were classified as non-specific dementia or not formally diagnosed as Alzheimer's disease. Additionally, this cohort from the Montefiore Health System is not necessarily representative of the national average. Data was only available for patients who returned to our health system. It is plausible that patients who returned for follow-up appointments were more likely to have more severe COVID-19. However, patient records included those who returned for any medical reason, including but not limited to routine office visits. SARS-CoV-2 vaccination status was not reliably recorded if patients received vaccines outside of the Montefiore Health System, and thus it was difficult to analyze our outcomes with respect to vaccination status. Because vaccination decreases risk of severe COVID-19,106,107 it is expected that it would reduce the risk of COVID-19 associated long-term sequelae. Another limitation is that we did not analyze outcomes with respect to dementia severity, frailty, and other dementia-associated comorbidities. Most of these variables are not available or consistently documented in the electronic health records. Our cohort's demographics consist of large proportion of underserved minorities, with low proportion of Caucasians. Our findings may not be applicable to populations that are less diverse. We did not analyze outcomes with respect to social determinants of health and it is likely that socioeconomic status could affect outcomes. As with any retrospective study, there could be other unintended patient selection biases and confounds
SARS-CoV-2 infection was significantly associated with a higher adjusted risk of MACE, dysphagia, dyspnea, fatigue, sleep, altered mental status, and falls in patients with pre-existing dementia. Our findings suggest that COVID-19 status is associated with broad accelerated dementia disease progression. This data further supports the notion that SARS-CoV-2 infection leads to a higher risk of adverse outcomes in patients with pre-existing neurological conditions. Understanding the interplay between COVID-19 and dementia is helpful for developing effective long-term management strategies and mitigating the potential exacerbations and progression of dementia in the context of the ongoing COVID-19 pandemic. More specifically, studies are warranted to investigate if COVID-19 survivors with dementia benefit from more intensive monitoring to prevent or promptly address dysphagia, fractures from falls, cognitive impairment worsening from sleep disturbances, and MACE.
Supplemental Material
sj-docx-1-alz-10.1177_13872877241303934 - Supplemental material for Long COVID-19 outcomes of patients with pre-existing dementia
Supplemental material, sj-docx-1-alz-10.1177_13872877241303934 for Long COVID-19 outcomes of patients with pre-existing dementia by Roham Hadidchi, Rachel Pakan, Tharun Alamuri, Noel Cercizi, Yousef Al-Ani, Stephen H Wang, Sonya Henry and Tim Q Duong in Journal of Alzheimer's Disease
Footnotes
Acknowledgments
The authors have no acknowledgments to report.
ORCID iDs
Author contributions
Roham Hadidchi (Conceptualization; Formal analysis; Investigation; Methodology; Visualization; Writing – original draft; Writing – review & editing); Rachel Pakan (Conceptualization; Formal analysis; Investigation; Methodology; Visualization; Writing – original draft; Writing – review & editing); Tharun Alamuri (Writing – original draft; Writing – review & editing); Noel Cercizi (Writing – original draft; Writing – review & editing); Yousef Al-Ani (Conceptualization; Formal analysis; Writing – original draft); Stephen H Wang (Conceptualization; Supervision; Validation); Sonya Henry (Data curation; Resources; Supervision; Validation); Tim Q Duong (Conceptualization; Resources; Supervision; Validation; Writing – original draft; Writing – review & editing).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data availability
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.