
Abstract
Background
Alzheimer's disease (AD) is a multifactorial and progressive neurodegenerative disorder influenced by a variety of genetic and environmental factors. The apolipoprotein E (APOE) gene is known to have a pivotal impact on disease onset, yet clinical studies on its impact on AD remain scarce in Lebanon.
Objective
This study investigates the interplay between environmental risk factors, the APOE gene, and AD in North Lebanon.
Methods
A case-control study was conducted with 136 individuals, including 57 AD patients and 79 normal individuals, among which 55 individuals were verified to be cognitively normal via the Mini-Mental State Examination (MMSE). A comprehensive survey was used to collect data on lifestyle factors, medical history, and other possible diseases and deficiencies. Blood samples were collected from all participants, then their DNA was isolated and stored. Real-time PCR was adopted for genotyping.
Results
The total APOE ε4 allele prevalence was reduced from 19.1% to 16.1% after MMSE adjustment. Based on the univariate analysis, factors like age, illiteracy, vitamin and iron deficiencies, blood pressure, and chronic diseases were identified as prominent risk factors, while the allele showed no significant correlation with AD. However, in the multivariable analysis, this allele emerged as a key risk factor (p = 0.04). Factors like age ≥ 65, vitamin deficiency, iron deficiency, blood pressure, and other chronic diseases were consistently significant.
Conclusions
Our results provide significant evidence that the influence of APOE ε4 on AD is governed by several environmental factors such as age, vitamin and iron deficiencies, high blood pressure, and chronic diseases.
Introduction
Sixty–80% of dementia scenarios are caused by Alzheimer's disease (AD). 1 AD is a neurodegenerative disorder characterized by the presence of amyloid-β peptide (Aβ) in the brain, along with the accumulation of hyperphosphorylated tau protein. These aggregations affect synaptic function and lead to neuronal death.2,3 There are two types of this disease: late-onset AD and early-onset AD. The more prevalent type is late-onset AD, which typically affects people after the age of 65. 4 This illness progressively destroys memory and eventually impairs the body's ability to perform some serious functions. Thus, it leads to the loss of ability to carry out daily life tasks, decreases the quality of life for the patient and their caregivers, and can be fatal to the patients 3 to 9 years after the recognition of the disease.5–7 AD is a progressive disease, developing gradually from the preclinical stage to mild cognitive impairment and finally AD. Therefore, early diagnosis is crucial, as it is one of the key factors in possibly slowing the progression to severe stages of AD.8,9
This illness has numerous risk factors, both preventable and non-preventable. Preventable factors include smoking, alcohol intake, illiteracy, cardiovascular disease, overweight, diabetes, atherosclerosis, lack of exercise, vitamin B12 deficiency, lack of brain activity, and unhappiness. whereas, the non-preventable factors include age, genetic predisposition (such as Triggering Receptor Expressed on Myeloid cells 2 (TREM-2) and apolipoprotein E (APOE)), sex, race, and family history. 10
Regarding age, it's important to note that the number of elderly people is increasing, which will lead to a significant increase in the number of AD patients. 11 According to the World Health Organization (WHO), the number of elderly individuals was 1 billion in 2019 and is expected to increase to 2.1 billion by 2050. Thus, according to the World Alzheimer Report (2023), the number of dementia cases worldwide is estimated to increase from 55 million in 2019 to 139 million by 2050 and this burden will also impact the economic sector, with costs estimated to reach 2.8 trillion dollars by 2030. In Lebanon, the number of aged people has been progressively increasing since 2012 (≈6%) according to the World Data Bank, and is projected to reach ≈27.1% by 2050 for people more than 60 years old. 12 Additionally, it is well established that females are more susceptible to developing AD compared to males, at least partly attributable to their longer average lifespans. 13
However, the APOE gene is also the most common factor, responsible for more than 50% of AD cases, 14 knowing that the impact of this gene can also vary according to race. 15 APOE is a lipoprotein lipid transporter that maintains cell homeostasis. 16 This gene has different alleles, including ε2, ε3, and ε4 with the ε4 being the variant most associated with AD and linked to the accumulation of brain amyloid.14,17 Thus, individuals carrying the APOE ε4 allele are more susceptible to risk factors than others, 18 and those with two copies of the APOE ε4 allele are more likely to develop tau aggregates in their brains than those having one APOE ε4 allele or the other variants. 19 In other words, many risk factors can influence the impact of this gene and contribute to the disease. 20
This study aims to identify the correlation between environmental risk factors (lifestyle and comorbidities), the APOE gene, and AD in North Lebanon. Though it is crucial to understand how genetics and lifestyle factors affect health outcomes globally, particularly with the growing older population, the research in this field remains sparse. To achieve this, we conducted a comprehensive analysis of various risk factors. This will allow us to determine the impact of the risk factors on the APOE gene expression in patients from North Lebanon.
Methods
Participants
Study participants were either recruited from different elderly care centers or grouped individually from houses in North Lebanon. Their selection was based on age criterion; only individuals over 55 years old were eligible to participate in the study. Furthermore, AD patients were selected according to their clinical diagnosis by a neurologist.
Questionnaires
The survey comprises two distinct questionnaires that have been developed by our team for 136 individuals. There is a common section between AD patients and healthy individuals where we completed, for all participants, a survey of simple questions concerning mainly the risk factors, including medical, nutritional, and social lifestyle choices. However, it is important to emphasize that the most studied risk factors in literature were selected for the present study, while less influential ones were not included. For AD patients who were diagnosed by a neurologist, an additional questionnaire, including medications taken and symptoms experienced, was filled out by their treating supervisors. For healthy participants, an Arabic version of the Mini-Mental State Examination (MMSE) test was performed to verify cognitive functions of normal individuals recruited in the study. As a result of this test, individuals who got a score of 20 or above were considered healthy, and those who got a score under 20 were assumed to have cognitive decline.
Sampling
5 ml of whole blood was collected in EDTA tubes from all participants and stored at 4°C for at least 1 month. Note that all volunteers, healthy individuals, and patient supervisors signed a research consent form. Therefore, the study was performed in accordance with the Declaration of Helsinki and approved by the Ethics Committees of the associations (CE-EDST-7-2021).
At this point, it is good to mention that we have faced many obstacles, whether from the caregivers or the relatives of the patients such as getting enough blood samples and information about the AD patients’ past nutritional habits and lifestyle choices since the supervisor at the center was responsible for answering and not a relative of the patients.
Genomic DNA extraction from blood samples
DNA was extracted from the buffy coat following the method of “Gen-Elute TM Blood Genomic DNA Kit of Sigma ALDRICH”. The main solutions used in the extraction were proteinase K, lysis C, ethanol, prewash, wash and elution solutions and were obtained from Sigma, USA. After extraction, the eluted DNA was stored at a temperature of −2 to −8°C in the case of short-term storage and at −20°C in the case of long-term storage in Eppendorf tubes of 2 μl each. The total volume of DNA collected was 200 μl. 21
Real time polymerase chain reaction (PCR)
A real-time PCR was used to determine the type of APOE allele in all individuals. The APOE gene is polymorphic with 3 known alleles: ε2, ε3, and ε4. The proteins coded by these alleles differ by the nature of amino acids at positions 112 and 158 22 : APOE ε2 (cys112, cys158), APOE ε3 (cys112, arg158), and APOE ε4 (arg112, arg158). The chosen primers for PCR reactions are mentioned in Table 1. 23
Nucleotide sequences of primers.
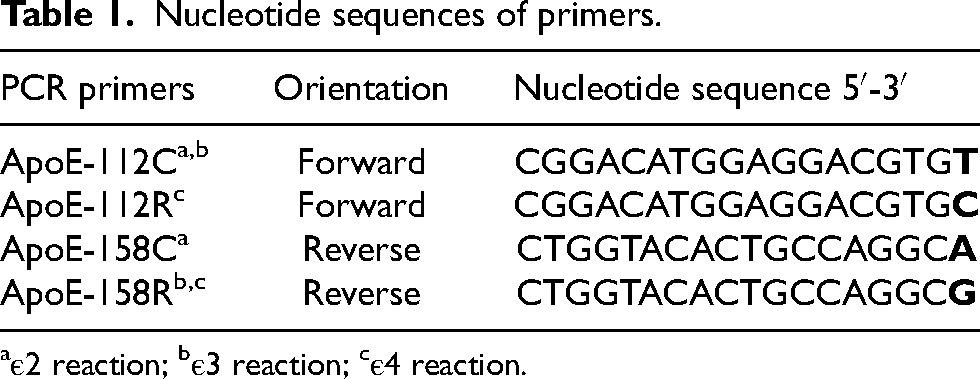
aε2 reaction; bε3 reaction; cε4 reaction.
The reaction mixture was denatured at 95°C for 10 min and after optimization, the PCR reaction was performed for 40 cycles under the following conditions: denaturation at 95°C for 15 s, annealing and elongation at 65°C for 1 min. PCR products were analyzed by agarose gel electrophoresis. DNA fragments were visualized under UV light after staining with the appropriate dye (ethidium bromide).
Statistical evaluation methods
All the data collected from the questionnaire and the blood samples were scrutinized for completeness and consistency before performing any analysis. The statistical analyses were done using the R software (R Core team, version 4.3.2; R Studio, version 2023-10-31). The dataset was imported, cleaned, and prepared for variable coding and data analysis. Plots were represented using the ggplot2 R package. Continuous variables were reported as mean ± standard deviation, while categorical variables were represented as frequency distributions. Fisher's exact test and two-sample t-test were performed for categorical and continuous data respectively. In this univariable analysis, a comparison between AD patients and the control group allowed the assessment of possible risk factors. A multivariable analysis was also conducted using logistic regression models. Potentially significant risk factors were included in the first model, then a backward logistic regression algorithm was adopted in order to remove non-contributing factors and get the best model conferring to the lowest Akaike information criterion (AIC) score. Statistical results were displayed as odds ratios (OR) with 95% confidence intervals (CI). All tests were two-sided, with a type I error rate of α = 0.05.
Results
Data distribution
The distribution of the study sample across different factors included within the study survey is reported in Table 2. This table highlights the prevalence of different factors within the study sample and helps with a more robust interpretation of the results. For each considered factor, the prevalence of missing NA values was displayed in the table.
Descriptive distribution of the study sample across different risk factors comprising Age, BMI, Sex, Family history, Disease knowledge, APOE status, Lifestyle choices, and Comorbidities.
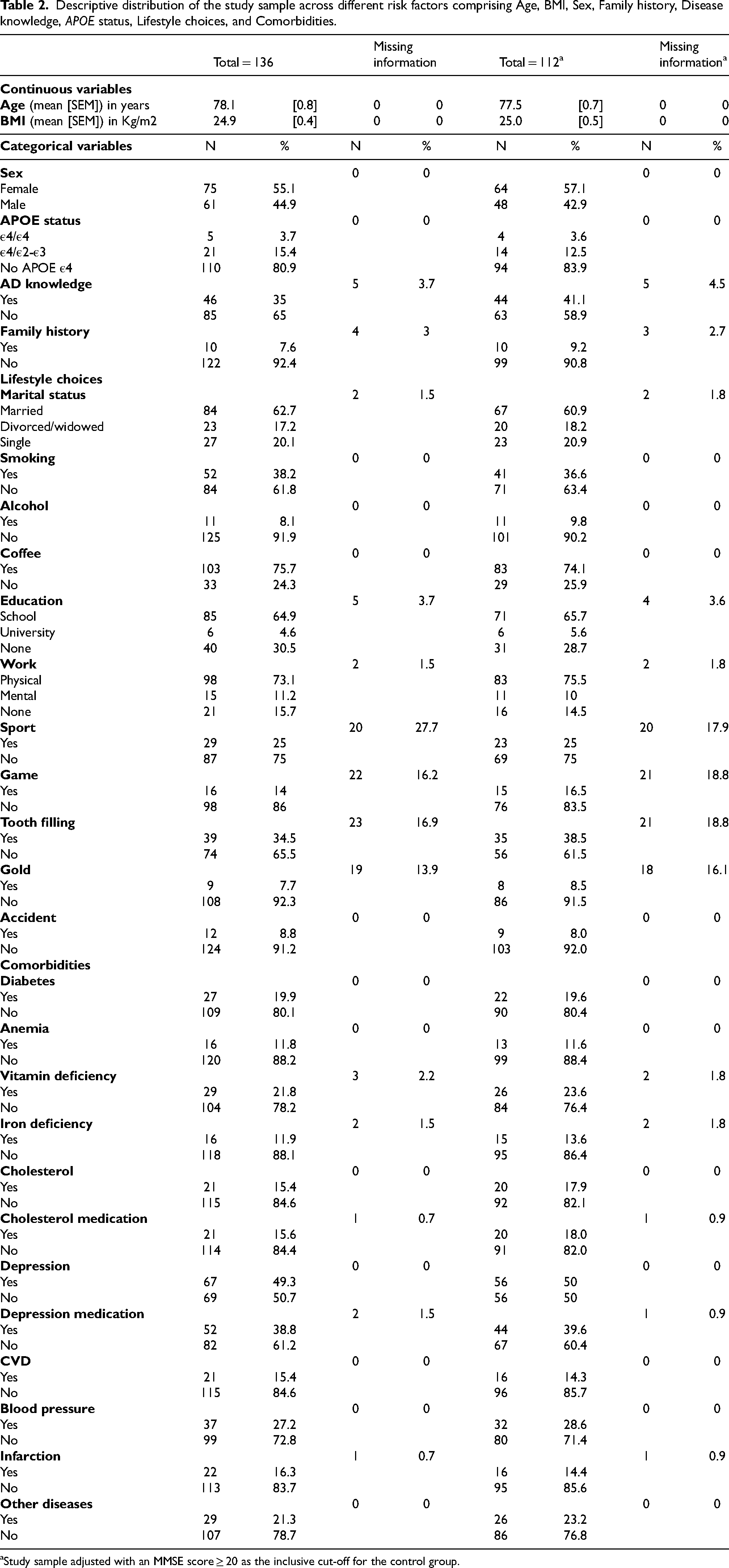
aStudy sample adjusted with an MMSE score ≥ 20 as the inclusive cut-off for the control group.
APOE ε4 predisposition
Interestingly, the prevalence of APOE ε 4 allele at its homozygous and heterozygous state constitutes 19.1% of the study sample, and 16.1% after MMSE score adjustment for controls at values ≥20. Furthermore, APOE ε4 genetic predisposition among the control population was 19.0%, which was remarkably reduced to 12.7% post-MMSE score correction Figure 1. Note that the homozygous state is rare in our data, constituting around 3.6%– 3.8%, thus the difference in E4 predisposition refers to a difference in the prevalence of patients heterozygous for the allele. To solve this issue, each analysis was performed before and after MMSE adjustment to avoid bias.

Prevalence of APOE ε4 in the control population. (A) Before MMSE correction; (B) Adjusted for MMSE score ≥ 20.
Univariate analysis
A univariate analysis was performed in order to compare each individual factor between Alzheimer's disease patients and controls. The analysis was done for all the sample first, as shown
in Table 2, and then the controls were selected based on their MMSE score to avoid any misclassification bias.
Based on Fisher's exact test, the presence of APOE ε4 did not show significant associations, at least not alone, either before or after MMSE score cut-off correction. Although the prevalence of APOE ε4 in our study sample was relatively high, this lack of significance may be attributed to the limited data availability. Factually, based on Tables 2 and 3, the insufficient frequencies of patients and controls with APOE ε4 allele at either its homozygous or heterozygote state could explain the insignificance of this genetic factor.
Univariate analysis of different risk factors potentially associated with Alzheimer's disease compared to controls in northern Lebanon.
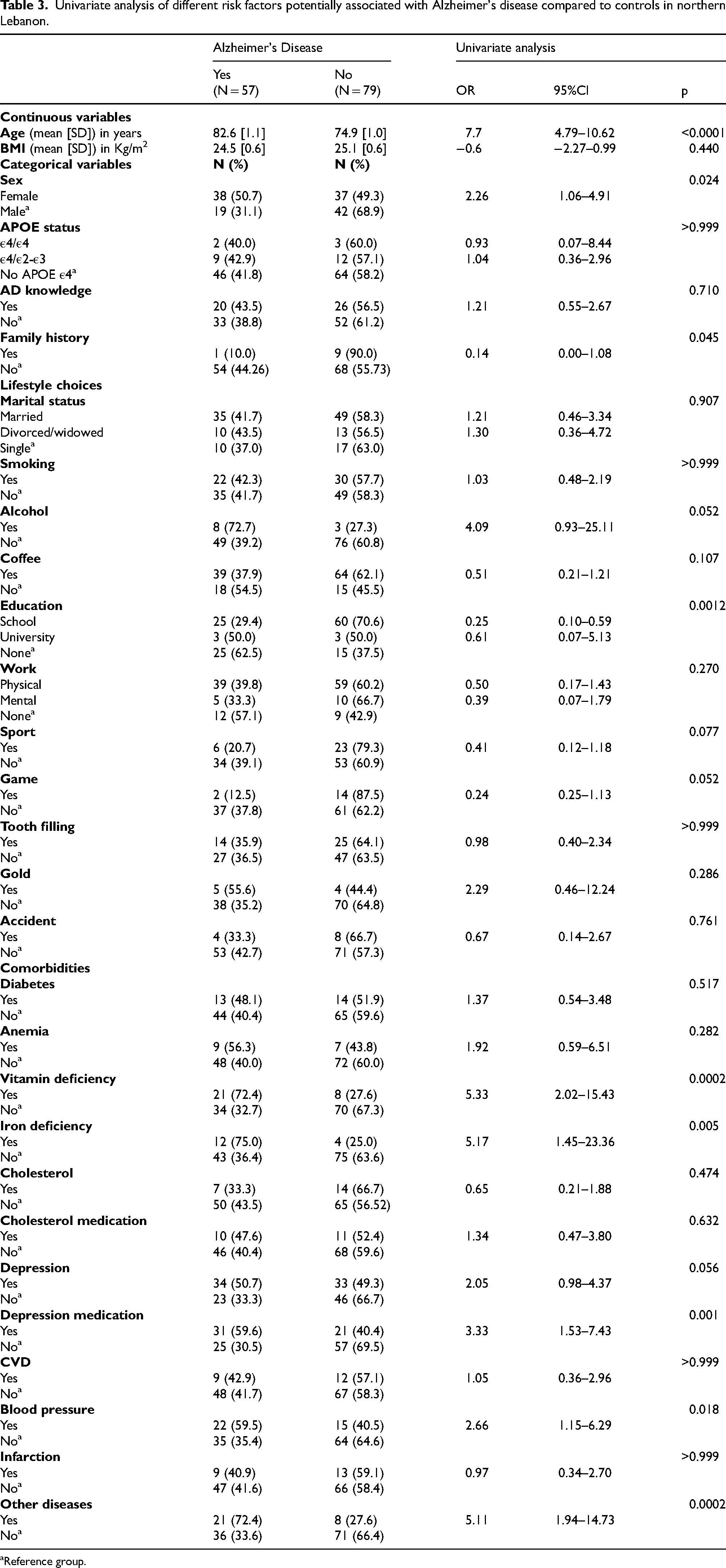
aReference group.
Before and after MMSE score adjustment, out of 29 considered factors, only nine factors were statistically significant (p ≤ 0.05). Age was highly significant in both analyses (p < 0.0001) with AD patients being significantly older than controls with a mean difference of 7.7 years before MMSE correction and a mean difference of 10.25 years after adjustment. Although sex showed statistical significance (p = 0.024) before MMSE selection, it ended up being insignificant but still close to the significance level after filtering (p = 0.055). When significant, the OR for being a female is 2.26 with a 95%CI (1.06–4.91), showing that the risk of AD is potentially higher for females compared to males.
Nevertheless, family history was significant before (p = 0.045) and after MMSE20 correction (p = 0.008). Although the former is statistically significant, the 95%CI (0.00–1.08) carried the probability of this factor being the same for both AD patients and controls with known family history compared to the unexposed group. However, after correction, the OR = 0.09 with a 95%CI (0.00- 0.72) proves that family history knowledge is beneficial for individuals as it constitutes a protective factor for them.
Among the lifestyle choices, education was significant for all data analysis (p = 0.0012) and after MMSE20 adjustment (p < 0.0001). However, the influential group was at the school level and not at the university level compared to the uneducated reference group. Compared to the latter, the ORs of schooling are 0.25 with 95%CI (0.10–0.59) and 0.13 with 95%CI (0.04–0.39) before and after correction respectively. Accordingly, these findings revealed education at the school level as a crucial protective factor against AD. Gaming is also a significant protective factor after MMSE cut- off (p = 0.02). The OR = 0.16 within a 95%CI (0.17–0.80) indicated that gaming that stimulates brain activity is correlated to a reduced risk of AD compared to those who do not indulge in such activities.
Among comorbidities, vitamin deficiency (p = 0.0002), iron deficiency (p = 0.005), depression medication (p = 0.001), and blood pressure (p = 0.018) were significant prior to any MMSE exclusions. After excluding controls with possible cognitive decline, the same factors remained significant with the following p-values in the same order: 0.001, 0.024, 0.001, and 0.022. These factors were proved to be potent risk factors, increasing the odds of the disease. Factually, based on Table 3, vitamin and iron deficiency had ORs = 6.07 with 95%CI (1.98–22.67) and 4.77 with 95%CI (1.18–28.02) respectively. Despite the large confidence interval range, vitamin deficiency includes at least an increase in the odds of developing AD by two times compared to the unexposed group. Similar interpretation applies for iron deficiency, but at minimum, it is correlated with 1.18 times increased odds of AD compared to the unexposed group. On the other hand, blood pressure with OR = 3.95 and 95%CI (1.65–9.89) and depression medication with OR = 2.8 and 95%CI (1.10–7.55) showed relatively more reasonable confidence interval ranges. However, similar to other comorbidities, these factors are related to an increase in the odds of developing AD compared to the unexposed group. Also, some other disease problems including eczema, urinary tract infections, osteoporosis, arthritis, and paralysis, showed statistical significance in both analyses with p = 0.001 after MMSE correction. This is correlated with an increased risk of AD since the OR = 5.74 with a 95%CI (1.88–21.36). Although the wide range reflects big data variability, there is at least an increase in the odds of developing AD by 1.88 times compared to the unexposed group.
Note that some other lifestyle and comorbidity factors are close to the significance level, such as sports (p = 0.057) and depression (p = 0.058), but the analysis showed these factors including the probability of the exposure group having the same odds of AD occurrence compared to the unexposed group. Some important lifestyle and comorbidities factors are displayed in Figures 2 and 3 below.
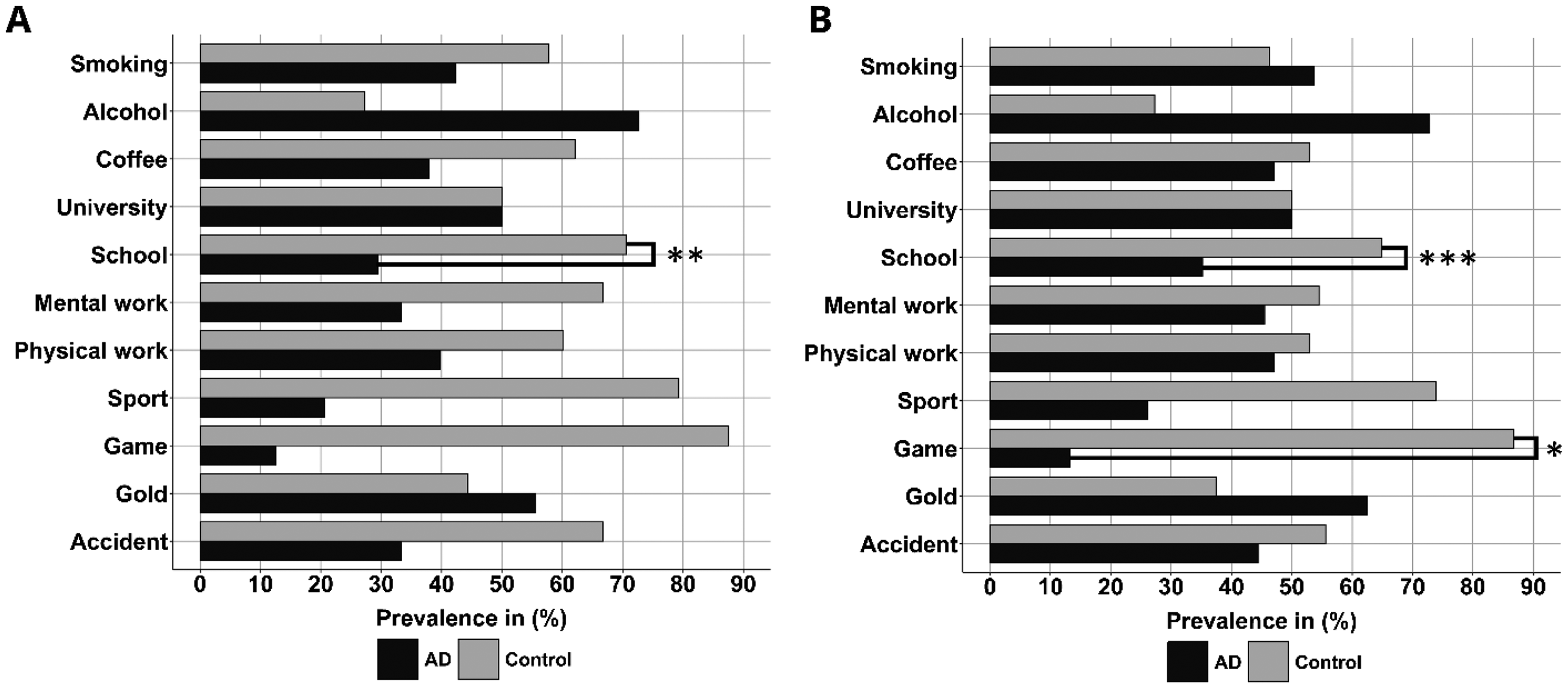
Distribution of AD patients and controls across important lifestyle risk factors. (A) Before MMSE correction; (B) Adjusted for MMSE score ≥ 20; Significance levels: *p < 0.05, **p < 0.01, ***p < 0.001, ****p < 0.0001.
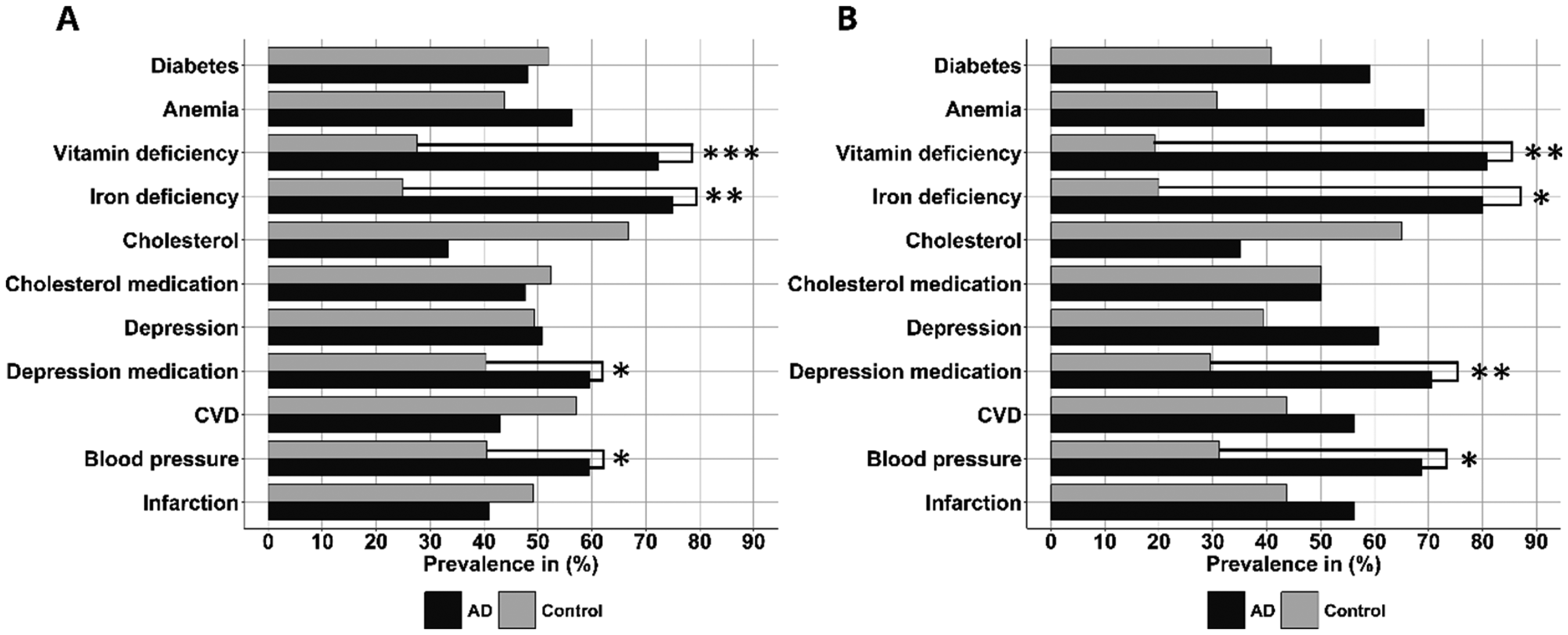
Distribution of AD patients and controls across important comorbidities. (A) Before MMSE correction; (B) Adjusted for MMSE score ≥ 20; Significance levels: *p < 0.05, **p < 0.01, ***p < 0.001, ****p < 0.0001.
The prevalence of E4 allele across the different risk factors shown significant based on Fisher's exact test is shown in Figure 4. There is a noticeable difference between AD patients and controls in several factors including age, sex, blood pressure, vitamin deficiency, iron deficiency, cholesterol, and other diseases. To further assess this possible relation, a multivariable analysis is required.
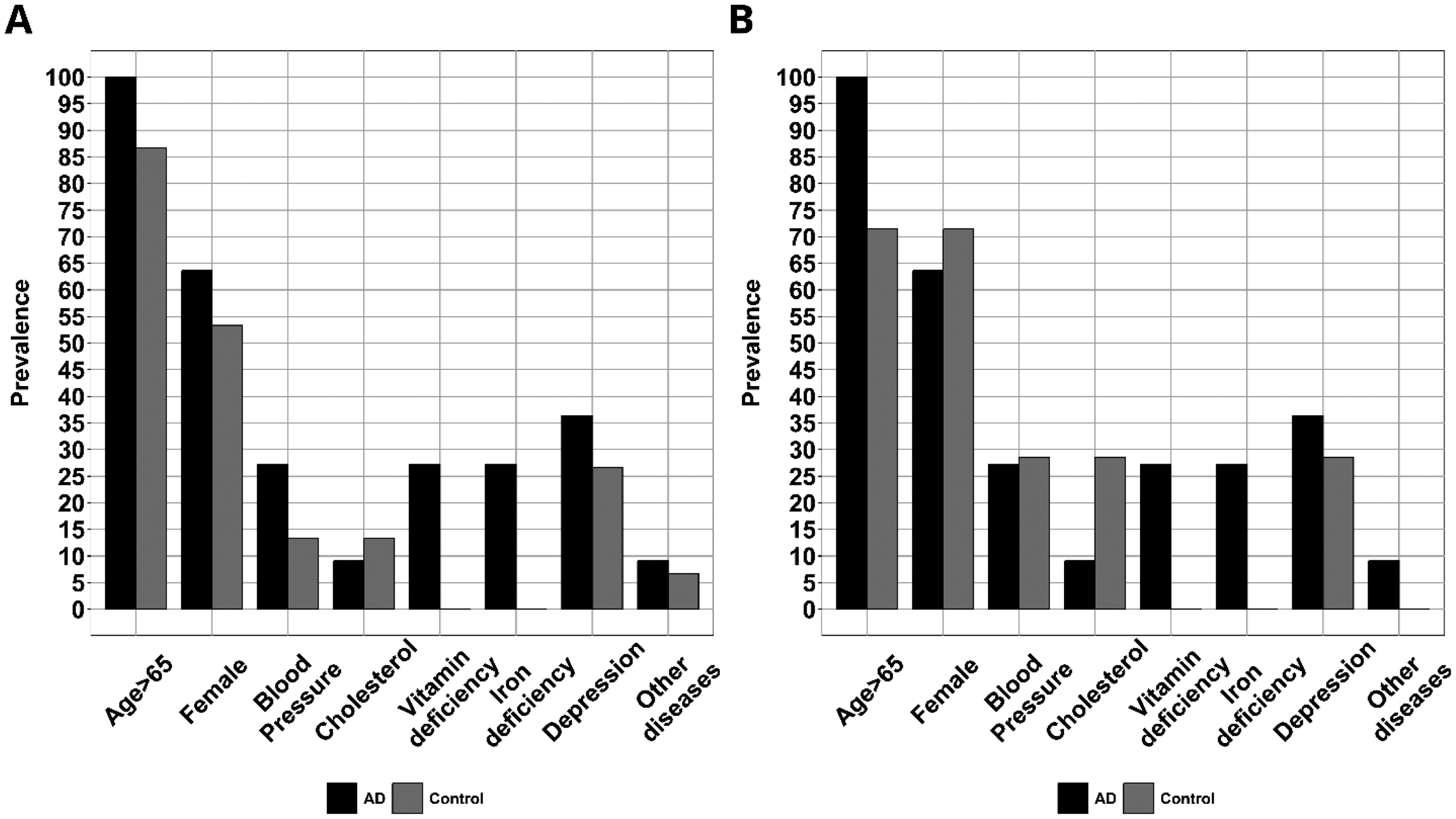
Distribution of AD patients and controls carriers of APOE ε4 allele across different risk factors. (A) Before MMSE correction; (B) Adjusted for MMSE score ≥ 20.
Multivariable analysis
A logistic regression analysis was performed in order to study the contribution of each of the considered factors in the appearance of cognitive decline. Factors with a p-value less than 0.2 from the univariate analysis were included in model 1. Then in model 2, a stepwise backward logistic regression was used to remove noncontributing factors in order to obtain the best model. The analysis was done for all the sample first, as shown in Table 4, and then controls were selected based on their MMSE score to avoid any misclassification bias (Tables 5 and 6).
Univariate analysis of different risk factors potentially associated with Alzheimer's disease compared to cognitively normal individuals with MMSE score ≥ 20 in northern Lebanon.
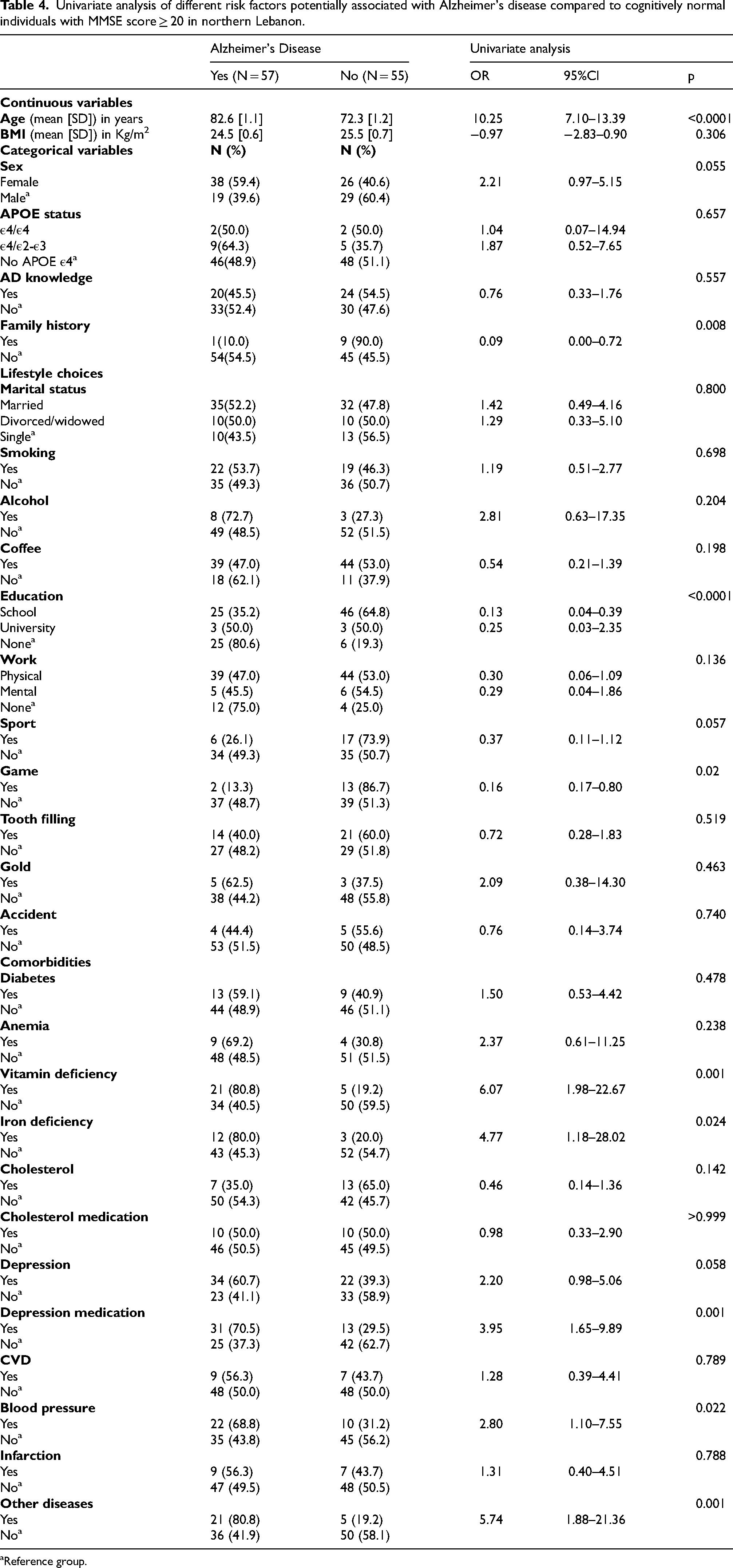
aReference group.
Multivariable analysis of significant risk factors potentially associated with Alzheimer's disease compared to normal individuals.
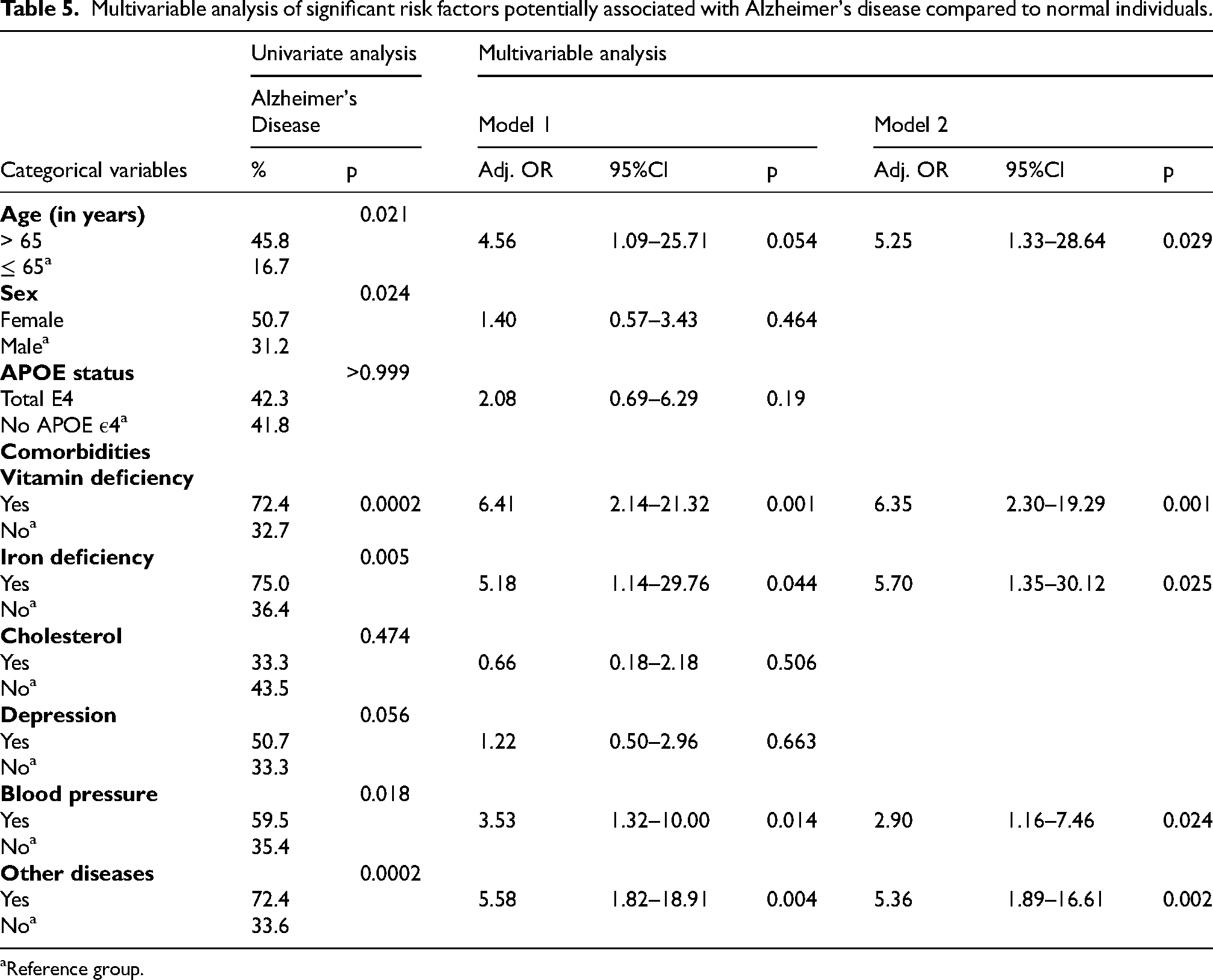
aReference group.
Multivariate analysis of significant risk factors potentially associated with Alzheimer's disease compared to cognitively normal individuals with MMSE score ≥20 studied.
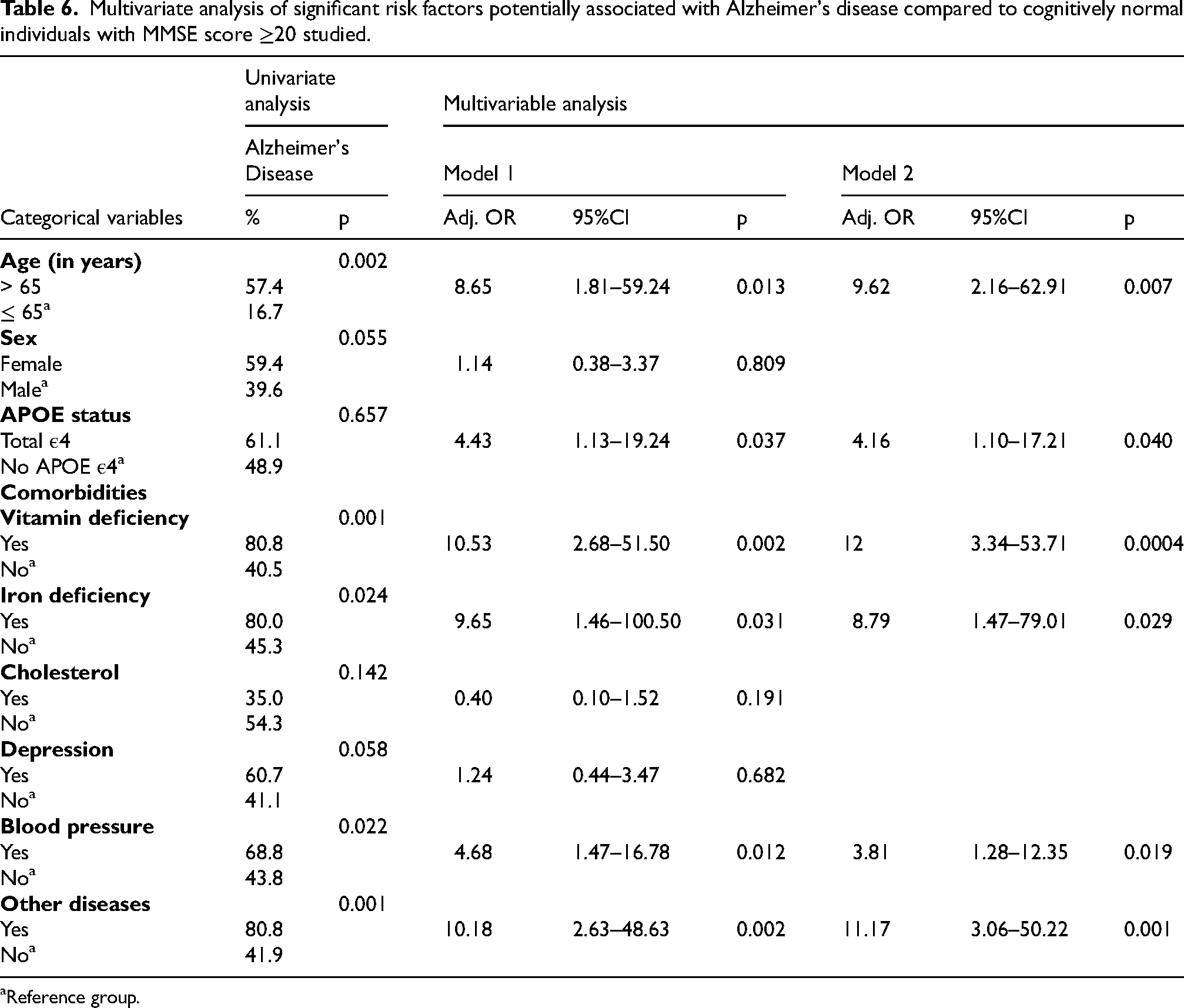
aReference group.
Based on the logistic regression test, before MMSE score adjustment, the presence of APOE ε4 did not show significant associations, but after MMSE cut-off, the presence of APOE ε4 became significant in model 1 (p = 0.0373) and model 2 (p = 0.040). In model 1, age was not significant but close to the significance level (p = 0.0542) including all the data, but then after correction, it became significant (p = 0.0132) with an OR of 8.65, concluding that age increases the odds of developing AD. Sex was not significant before (p = 0.4646) and after (p = 0.8087) correction. Among comorbidities, cholesterol, and depression were not significant before (p = 0.5055, p = 0.6631 respectively) and after correction (p = 0.1907, p = 0.689 respectively). These findings revealed that cholesterol and depression are not correlated with AD at least within this analysis. Vitamin deficiency, iron deficiency, blood pressure, and other diseases showed statistical significance in both analyses with p = 0.0014, p = 0.0437, p = 0.0138, p = 0.0037 respectively before correction and p = 0.0016, p = 0.0313, p = 0.0121, p = 0.0016, respectively, after correction. Their OR were all > 1 which means that these factors are associated with an increase of the risk of AD. Note that other diseases include only chronic diseases that do not affect cognition directly (i.e., eczema, urinary tract infections, osteoporosis, arthritis, etc.).
In model 2, a backward stepwise logistic regression algorithm was used to remove factors that do not affect the model while keeping those significant and other confounding factors. Specifically, age, vitamin deficiency, iron deficiency, blood pressure, and other diseases were significant before (p = 0.029, p = 0.001, p = 0.025, p = 0.024, p = 0.002, respectively) and after correction (p = 0.007, p = 0.0004, p = 0.029, p = 0.019, p = 0.001, respectively). Their OR were all > 1 which indicates that these factors are associated with an increased risk of AD.
AD symptoms in North Lebanon
The results indicate that patients’ diagnosis was remarkably tardy in our sample reaching around 79.5 ± 1.1 years with 95%CI (77.2–81.8). Additionally, a detailed description of the major symptoms affecting AD patients face is vital due to the fact that only a minority of the patients (24.6%) are getting medical treatment and health support. The most prominent AD manifestation in North Lebanon is directly related to a decline in cognitive functions. As shown in Figure 5, these symptoms include: Time problems (75.4%), followed by numerical problems (61.4%), and language problems (45.6%). Also, regarding behavioral and psychological manifestations, AD patients mostly suffer from sleep disturbances (68.4%), sundowning issues (47.4%), anorexia (43.9%), and aggression (35.1%). Clearly, physical symptoms are the least prevalent ones, including trembling (22.8%) and sclerosis (19.3%).
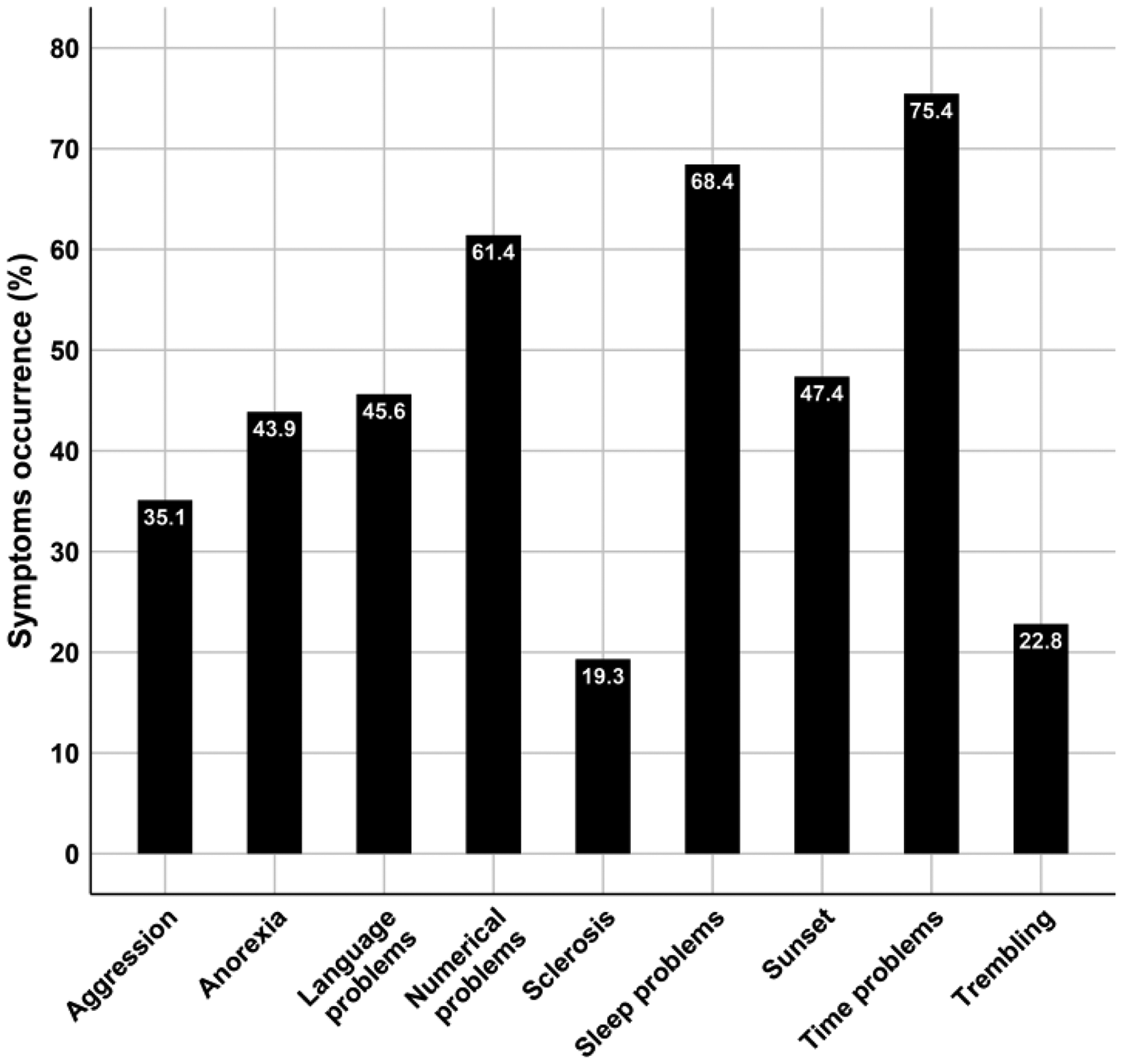
The occurrence of late-stage Alzheimer's disease symptoms in North Lebanon.
Discussion
In the present study, the distribution of APOE ε4 among the total sample, including 136 individuals (19.1%) is in line with a previous study done by Shamieh et al. in 2019. 24 Factually, the latter study showed that the distribution of APOE ε4 in the general Lebanese population (12%), based on a 1000 genomes populations comparison, is close to some ethnic groups in some Asian countries, including India (17%), Bangladesh (16%), Pakistan (16%), the Hai Chinese of Beijing (20%), and Japan (15%). Furthermore, it is essential to mention the surprisingly higher prevalence of APOE ε4 in Europeans reaching around 33% of their total population. 24 APOE is proved to have a pivotal role in the appearance of AD as its predisposition at its ε4 allele is correlated with a drastic increase in the disease pathology. 25 Based on Fisher's exact test, the APOE ε4 allele had no significant correlation with AD when taken alone (p = 0.657). However, the varying impact of this gene on the disease across different ethnic groups may be attributed to differences in lifestyle factors, as well as gene-gene and gene-environment interactions, which require further investigations.
According to Table 3, it is evident that age is a highly significant risk factor for AD (p < 0.0001). The large mean difference between AD and Normal subjects could be explained by the tardy diagnosis reaching around 80 years old. This staggering situation explains the extensively poor management of the disease, reaching only 24.6% of the considered AD patients. For the most part, these patients were suffering from a remarkable decline in their cognitive functions which indicates a tardive stage of the disease (Figure 5).
The biological sex was shown nearly significant (p = 0.055), indicating that females would be more susceptible to experiencing the disease which validates previous findings. This disparity is not due to age differences between both sexes, since the average age of females or males among AD patients and control were similar ≈82.6 and ≈74.6 years respectively.13,26 Heavy menstrual bleeding could explain this increased risk of AD in females. Also, the progression of AD may have a bioenergetic origin that is related to hormonal changes in women. Indeed, estrogen plays a crucial role in the regulation of several metabolic processes in the brain, particularly glycolysis. However, during menopause, a major drop in sex hormones, estrogen, and progesterone, will result in an alteration in the modulation of these metabolisms. As a result, during the post-menopause stage, there will be a reduction in glucose metabolism that will be considerably compensated by the activation of fatty acid metabolism. 27
Our result is consistent with previously performed clinical studies where iron and vitamin deficiencies (namely vitamins D3 and C) were found to be essential risk factors for AD. This could be explained by the periodic excessive blood loss making females more vulnerable to such shortfalls.28–30 We speculate that iron deficiency could carry a high risk of developing AD due to the lack of rich oxygenation to the brain. In fact, such deficiency could disrupt oxygen transport through hemoglobin molecules, resulting in a systemically poor oxygenation in the body as well as in the brain. 31 This stimulates the accumulation of free radicals, which promotes a progressive membranal decay that renders the neurons’ physiological functions and disrupts synaptic communications, leading to cellular apoptosis.32,33
Both educational level (p < 0.0001) and brain-stimulating games (p = 0.02) were significantly important protective factors against AD. This has been reported by many other intervention studies, as a noticeable enhancement in cognitive functions including visuospatial abilities and cognitive workload is seen in cognitively normal elders. 34 Additionally, depression medication emerged as a significant risk factor correlated with an increased risk of AD. In fact, the number of patients treated with such medications reflects the number of patients suffering from clinical depression who require medical intervention following a specific diagnostic protocol. Surprisingly, family history of AD was also another protective factor against cognitive decline (p = 0.008). This could possibly be explained by the fact that these individuals adopt specific and healthy lifestyle choices trying to delay the early onset of the disease.
While no significant correlation between tooth fillings and AD was found in the present work, it is recommended to consider gum disease (i.e., periodontitis), in further studies as it may contribute to AD through chronic inflammation, which can promote Aβ deposition and neuroinflammation. 35
The multivariable analysis conducted in the study provides a clearer understanding of the correlation between the most prominent factors and the emergence of AD. Based on Table 5, six out of the nine considered factors were shown to be significant. Taken together with the other factors, APOE ε4 predisposition is a remarkably influential risk factor, leading to a higher risk of developing the disease. These results are in line with the recent findings performed on a large scale by Fortea et al. (2024). 36 Model 2 validates the impact of age > 65 years on the incidence of the disease as mentioned previously. Similar to the univariable analysis, vitamin deficiency, iron deficiency, blood pressure, and other chronic diseases (i.e., eczema, urinary tract infections, osteoporosis, arthritis, and paralysis) were correlated with an increased risk of AD. However, gender, cholesterol, and depression were excluded due to their insignificant correlation with AD and the other considered factors within the model. The latter suggests that there is an interplay between genetics, some environmental risk factors, and co-morbidities.
This study faced some limitations that should be addressed in future research projects. The limited sample size and the lack of information (i.e., NA values) about some individuals included in the study affected the accuracy of our analyses. In addition, while the MMSE test was the reference to classify and remove the false negative cases from the study (exclusive criteria), it still can be influenced by the psychological state of individuals, which might diminish the specificity of the test. Also, it is important to mention that biochemical tests (e.g., lipid profile, sugar levels, vitamin deficiencies, C-reactive protein, etc.) were not performed due to the lack of funding.
Conclusion
APOE ε4, a major gene involved in the appearance of AD, is an influential risk factor when studied with other environmental factors. However, a thorough statistical assessment of its impact in North Lebanon is still required. Our results highlight the association of several other factors with an increased risk of AD, specifically; vitamin deficiency, iron deficiency, blood pressure, and other chronic diseases based on which some preventative measures could be adopted against the disease. Even though the sample size is small, these results show the importance of studying APOE ε4 with other environmental factors as a diagnostic tool for AD. Results also highlight other factors, such as education and mental games which might delay the onset of the disease. Finally, an essential point is to avoid late diagnosis in Lebanon; we hope to establish a diagnostic protocol before or at an early stage of the AD to be able to implement an effective treatment and management. In addition, it is advisable to conduct further studies with a larger sample size in order to reach more decisive and conclusive outcomes. Furthermore, it is recommended to investigate the possible role of other genes along with the influence of each environmental factor in correlation with genetic factors, including APOE ε4. All of these suggestions may lead to a better understanding of the disease's mechanism.
Footnotes
Author contributions
Mohamed Khaled (Conceptualization; Project administration; Supervision; Validation; Visualization; Writing – original draft; Writing – review & editing); Hadi Al-Jamal (Conceptualization; Data curation; Formal analysis; Investigation; Software; Validation; Visualization; Writing – original draft; Writing – review & editing); Dana Matar (Formal analysis; Investigation; Software; Writing – original draft; Writing – review & editing); Antonia Ibrahim (Formal analysis; Investigation; Software; Writing – original draft; Writing – review & editing)
Layla Tajer, M.Sc in Microbiology (Investigation; Writing – original draft; Writing – review & editing); Nicole Issa (Investigation; Writing – original draft; Writing – review & editing); Reem El-mir (Investigation; Methodology; Writing – original draft; Writing – review & editing); Joudi Hantour (Investigation; Methodology; Writing – original draft; Writing – review & editing)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restriction.