
Abstract
Background
Alzheimer's disease (AD) is a progressive neurodegenerative disorder characterized by significant cognitive and behavioral impairments. Near-infrared (NIR) light treatment has shown potential in cognitive improvement in previous studies. However, clinical trials of NIR for AD remain limited.
Objective
This study investigated the safety and effects of whole-head 810 nm NIR therapy in AD patients, including long-term efficacy.
Methods
An open-label pilot study on whole-head NIR treatment for AD patients was conducted. Nine AD patients completed 4-month treatment (810 nm, 100 mW/cm², 30 min/session, 6 sessions weekly). Safety and efficacy were evaluated at baseline, months 2 and 4, and 2-month post-treatment.
Results
After four months of whole-head NIR treatment, mean changes from baseline on the Mini-Mental State Examination were 3.2 (p = 0.02). Mean changes from baseline on the Alzheimer's Disease Assessment Scale-Cognitive were −5.0 (p = 0.05), mean changes from baseline on the Montreal Cognitive Assessment were 1.9 (p = 0.12). Mean changes from baseline on the Neuropsychiatric Inventory were −4.2 (p = 0.47). These benefits were sustained two months at least. With no device-related adverse effects were reported.
Conclusions
Whole-head 810 nm NIR light is safe and offers promising benefits for AD patients. To fully confirm its efficacy, durability, and underlying mechanisms, further large-scale randomized controlled trials are necessary.
Keywords
Introduction
Alzheimer's disease (AD), the most prevalent form of dementia, accounting for 60–80% of dementia cases, is characterized by cognitive impairment and functional decline. 1 Approximately 50 million people worldwide are affected, and this number is steadily increasing. 2 AD not only severely impacts the patients but also imposes significant burdens on their families and society. Currently, therapeutic methods, mainly including medications, 3 can alleviate some symptoms. 4 However, studies have shown they caused various side effects, such as nausea, vomiting, and headache. 5 Therefore, there is an urgent need to explore alternative or adjunct therapies for AD treatment.
Photobiomodulation (PBM) is a non-invasive, innovative neurostimulation method using red or near-infrared light (600 to 1100 nm) to target the brain.3,6 Among the PBM method, near-infrared (NIR) light has been highlighted for its safety, low cost, and convenience. It has been shown to enhance mitochondrial activity by targeting photoreceptor molecules such as cytochrome c oxidase (CCO) in neuronal mitochondria, thereby reducing amyloid-beta (Aβ) deposition and toxicity. Many animal studies have indicated the potential benefits of NIR for AD.7–9 However, fewer than 10 clinical studies have reported the effectiveness of NIR in improving cognitive function and quality of life in patients with AD or dementia, with most focusing on localized irradiation. 10 For example, Saltmarshes et al. applied 810 nm NIR to the default mode network (DMN) of five dementia patients, cognitive function was improved after treatment. 11 Similarly, Chao et al. using 810 nm NIR light targeting DMN nodes, found cognitive and neuropsychiatric symptoms improvement after three months of intervention. 12
The pathogenesis of AD involves multiple brain regions, Aβ plaques initially manifest in the neocortex and amygdala, while tau protein neurofibrillary tangles first appear in the brainstem and other subcortical area, eventually involving the entorhinal cortex and hippocampus. 13 As AD progresses, systematic degeneration of various brain structures and functions occurs. 14 However, NIR light must penetrate several barriers, including bone tissue and so on, to effectively stimulate brain tissue. 15 Model-based dosimetry studies emphasized the importance of covering multiple brain regions with NIR to achieve uniform photon energy distribution. 16 Given the widespread brain atrophy and loss of network connections in AD patients, 10 localized NIR light may be insufficient for effective neuromodulation. Therefore, investigating the safety and benefits of whole-head NIR treatment is essential. A recent study provides preliminary evidence supporting the potential values of whole-head NIR. Nizamutdinov et al. used a 1060–1080 nm NIR helmet in an eight-week intervention for dementia patients and observed cognitive improvements without any reported adverse effects.17,18 Despite this positive result, the safety and efficacy of whole-head 810 nm NIR in AD patients require further investigation, and the duration of improvements remains unclear.
In the present study, we aimed to determine the safety and potential benefits of whole-head 810 nm NIR light in AD patients, including the durability of improvements.
Methods
Participants
Ten participants were recruited from a senior cognitive care center (Figure 1). The inclusion criteria were: (1) meeting the core criteria for probable AD as defined by the National Institute of Aging Alzheimer's Association (NIA-AA criteria);19,20 (2) a Mini-Mental State Examination (MMSE) score < 26, (3) craniocerebral magnetic resonance imaging (MRI) examination (within 6 months) findings that supported the AD diagnosis; (4) age over 65 years; (5) both genders, predominantly right-handed; (6) receiving stable doses of drugs for at least three months prior to treatment until the follow-up was completed.
The exclusion criteria were: (1) contraindications for MRI, such as metal implants or claustrophobia; (2) other types of dementia or other psychiatric or neurological disorders, such as depression or Parkinson's disease; (3) history of stroke or seizures; (4) photosensitivity to sunlight or visible light, or increased skin sensitivity in the treatment area; (5) severe vision or hearing impairments; (6) had an alcohol or drug addiction; and (7) any other unsuitable for participation in this study.
This study was approved by the Ethics Committee of Rehabilitation Hospital Affiliated to National Rehabilitation Assistive Devices Research Center, Beijing, China (20211207). Written informed consent was obtained from all participants or their guardians prior to participation. This study is registered with Clinical Trial Registry (http://www.clinicaltrials.gov) with the registration number: NCT06008639.
Procedures
Each participant received 30 min each session, six times weekly, for four months. Neuropsychological assessment was conducted at months 2 and 4, as well as 2-months post-treatment (The timeline diagram is presented in Figure 2). The whole-head NIR treatment was administered using helmet device, it equipped with 80 light-emitting diode (LED) modules, emitting NIR light at 810 nm, with a pulse frequency of 10 Hz. The average power at about 1 cm from the LED modules was 90–100 mW/cm². Prior to each session, participants were seated comfortably and equipped with protective eyewear and a treatment cap. To ensure consistent lighting, researchers added a chin rest to minimize head movement and closely monitored each treatment. The effectiveness of each session was ensured by checking each device before and after each treatment.
Neuropsychological assessment
We used the MMSE, 21 the Montreal Cognitive Assessment (MoCA), 22 and the Alzheimer's Disease Assessment Scale-Cognitive subscale 12-item (ADAS-cog12) 23 to assess cognitive function. The MMSE is widely used to measure cognitive function, with below 26 indicating potential impairment. Compared to the MMSE, the MoCA emphasizes the assessment of cognitive functions related to executive function and attention. The ADAS-cog is commonly used for observing cognitive function changes in AD and evaluating the efficacy of AD treatments. Generally, higher scores on the MMSE and MoCA, and lower scores on the ADAS-cog, indicate better cognitive performance.
Dementia-related behaviors were assessed using the Neuropsychiatric Inventory (NPI), 24 a caregiver-based questionnaire that evaluates 12 common behavioral domains in dementia, including frequency, severity. The NPI frequency severity total score (NPI-FS) was used as a summary measure. Basic Activity of Daily Living (ADL) were evaluated using the Barthel Index (BI), 25 The BI consists of 10 subitems, each assigned varying weights. Scores are given in increments of 5 points, with a maximum possible score of 100. Higher scores indicate greater levels of functional independence. All assessments were conducted by a professional, neutral neuropsychological assessor who was blind to the intervention protocols to ensure impartial evaluation.
Statistical analysis
Neuropsychological assessment scores were used in this study as the endpoint to evaluate the effects of whole-head NIR treatment. Data analysis was performed using Origin2021 software (https://www.originlab.com). Initially, the data underwent normality testing. For normally distributed data, a one-way repeated measures (ANOVA) and paired t-tests were used. For non-normal data, the Kruskal–Walli's and Mann-Whitney U test were employed, with the significance level set at p < 0.05 (two-tailed).
Results
Participant characterization
In this study, we included a cohort of 9 individuals with AD, consisting of eight females and one male. Of these participants, 5 were receiving stable doses of concomitant medications, including dementia medication or other medications (details provided in Table 1). Table 1 also presents the participants’ characteristics and baseline neuropsychological assessment scores. Additionally, caregivers confirmed that none of the participants had a family history of AD.
The demographics and baseline characteristics of the participants.
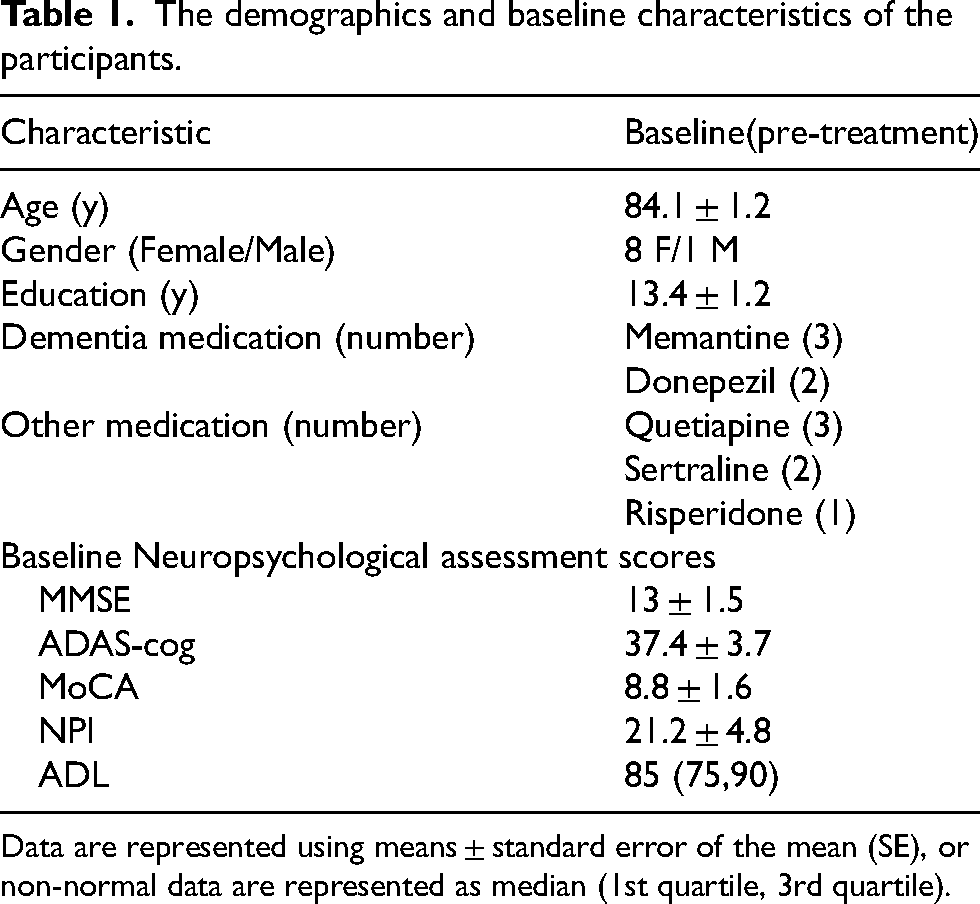
Data are represented using means ± standard error of the mean (SE), or non-normal data are represented as median (1st quartile, 3rd quartile).
Whole-head NIR treatment improved cognitive function
The assessment of cognitive function (Figure 3) demonstrated significant cognition improvement in AD patients after a 4-month treatment. There was significant increase in the mean change from baseline on MMSE (3.2, p = 0.02), with eight of participants (88.9%) showing increased, and 4 individuals rising by 5 or more points. After 4-month treatment, the average ADAS-cog showed a reduction of 5.0 points from baseline (p = 0.05). Approximately 66.7% of participants exhibited a reduction in ADAS-cog, with nearly half experiencing a drop of about 10 points. Additionally, the average MoCA score improved by 1.9 points compared to baseline (p = 0.12). Of the 9 participants, 7 showed an increased, with 5 increasing by more than 3 points.
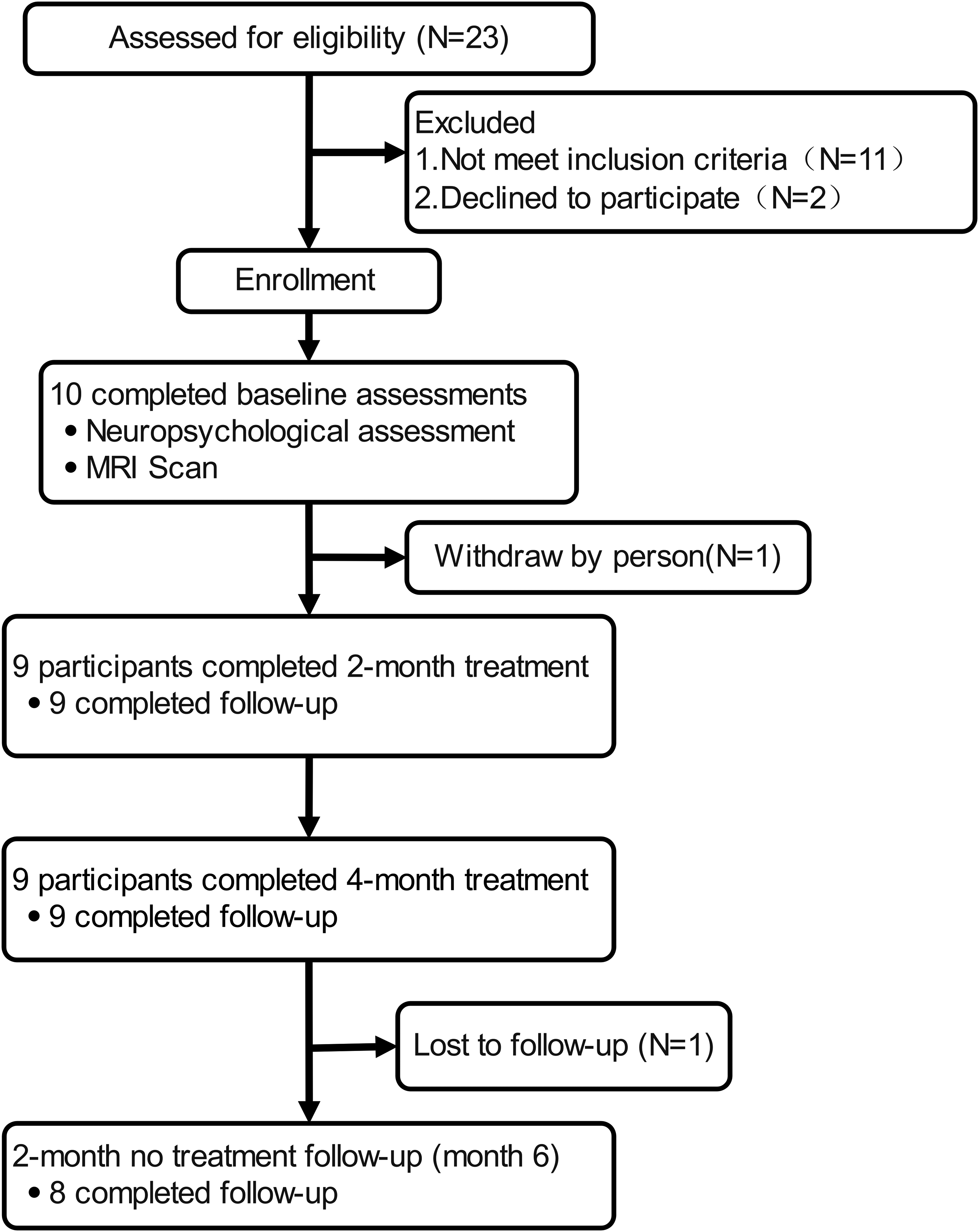
Experimental flowchart.
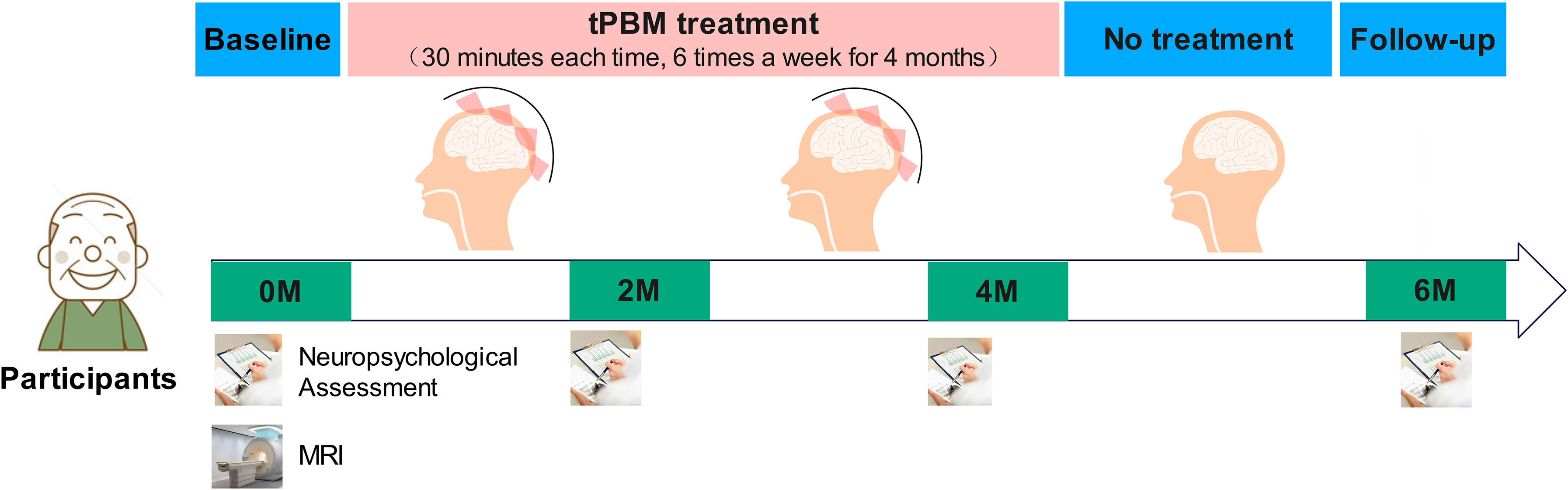
The diagrammatic of timeline.
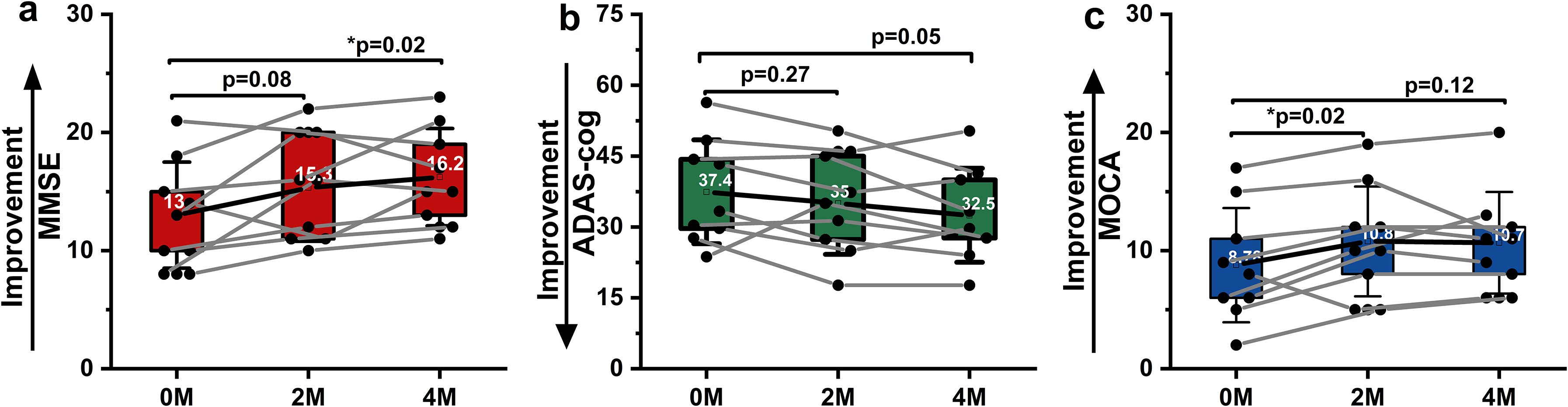
The results of the cognitive function scores, (a) MMSE, (b) ADAS-cog, and (c) MoCA, displayed as mean (marked), with boxes indicating first and third quartiles, error bars representing standard deviation (SD), black dots are individual scores. Black lines represent the overall trend, grey lines show individual trends. ‘p’ statistical results, with * indicating p < 0.05.
Whole-head NIR treatment alleviated neuropsychiatric symptoms
After a 4-month treatment, the NPI-FS showed an improvement trend (p = 0.47), with an average change from baseline of −4.2 points (Figure 4(a)). Although not statistically significant, item scores in the NPI (Figure 4(b)) indicated improvements in symptoms such as delusions, hallucinations, depression, anxiety, apathy, and sleep/nighttime behavior (p > 0.05), most of the abnormal behaviors were relieved. In treatment interview records, caregivers indicated that most participants showed an increased willingness to engage in group activities, suggesting improved social interaction. Participants also proactively reported improvements in sleep quality and daily memory.
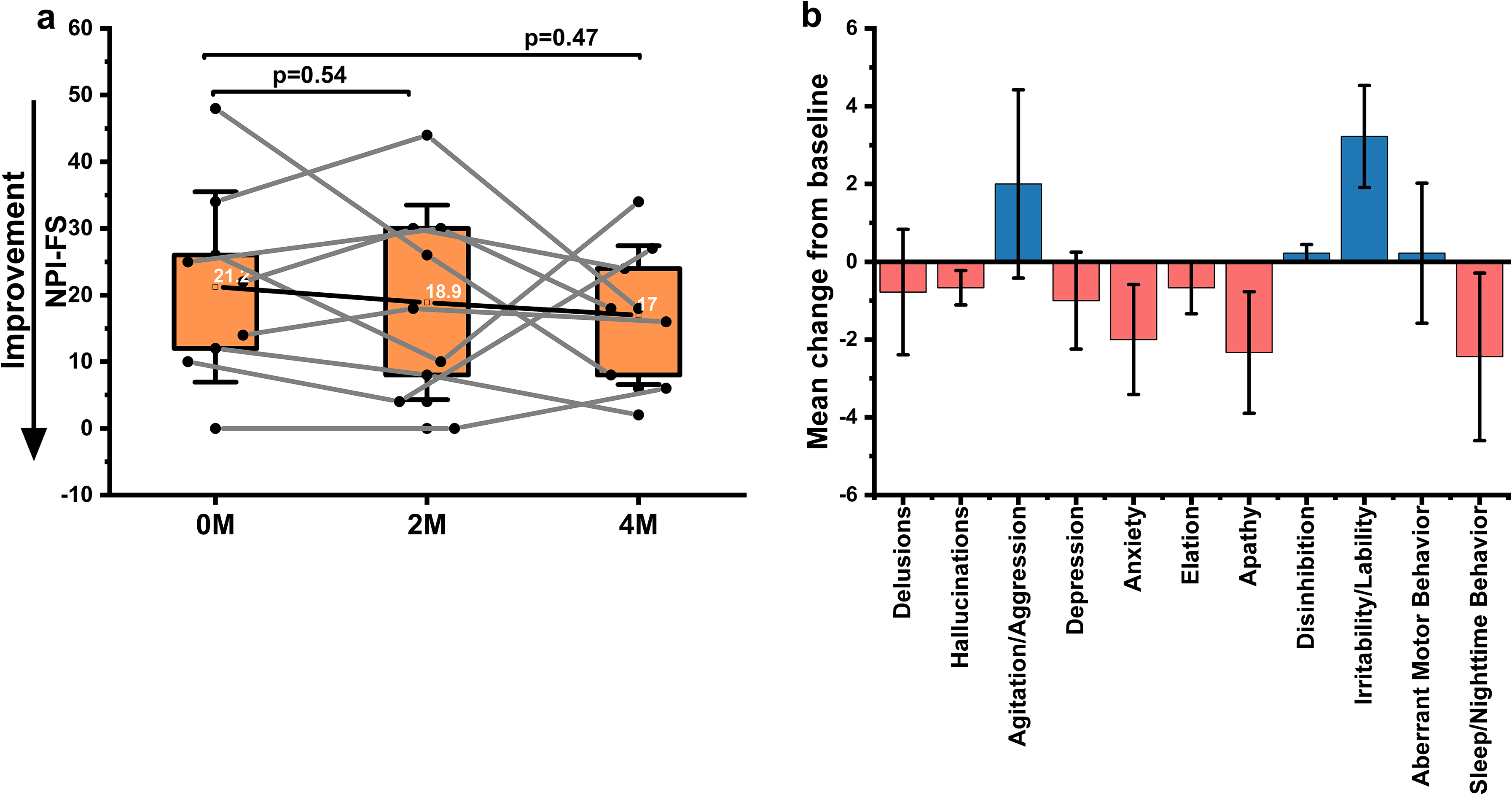
The results of the NPI scores, (a) NPI-FS, displayed as mean (marked), with boxes indicating first and third quartiles, error bars representing SD, black dots are individual scores. Black line represents the overall trend, while the grey lines show individual trends, ‘p’ statistical results. (b) Mean change from baseline in NPI-FS item scores, presented as mean ± SE.
Long-term efficacy of whole-head NIR in AD patients
Two months after the treatment ended (6M); one participant withdraw due to personal reasons. Eight participants completed the follow-up assessments. Although the extent of improvement slightly decreased compared to 4M, cognitive function still show improvement relative to baseline (0M), NPI-FS also keep improvement compared to baseline. Specifically, MMSE showed an increase of 1.9 points (Figure 5(a)), MoCA increased by 1.4 points (Figure 5(c)), and the average changes in ADAS-cog (Figure 5(b)) and NPI (Figure 5(d)) were −3.0 and −2.0 points, respectively. The results are noteworthy as they reveal the potential long-term benefits of whole-head NIR in AD patients, suggesting its effects can endure for at least 2 months or longer.
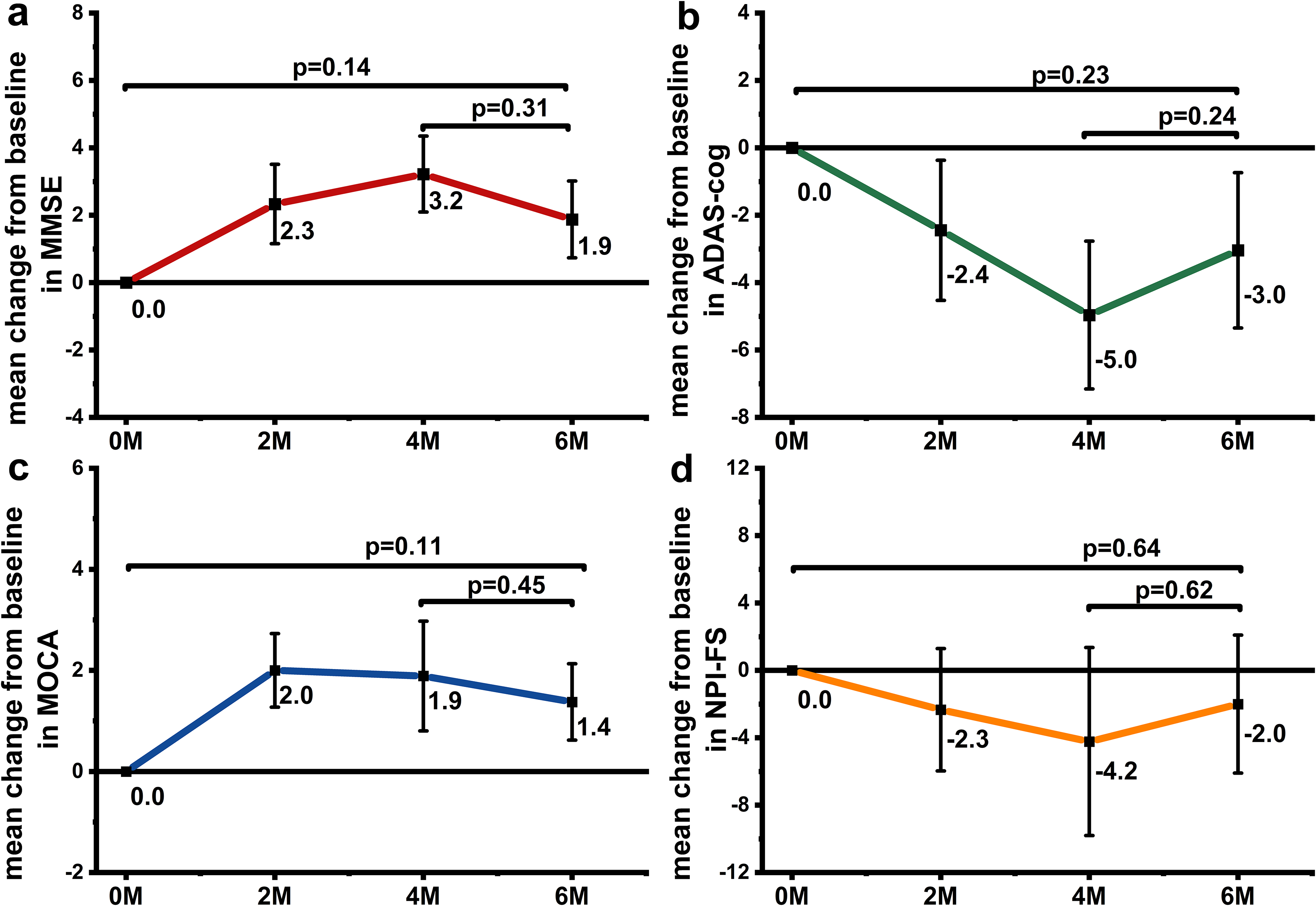
The mean change from baseline in scores: (a) MMSE, (b) ADAS-Cog, (c) MoCA, and (d) NPI-FS. Data are presented as mean ± SE. The sample size was 9 participants at 0 M, 2 M, and 4 M, and reduced to 8 participants at 6 M due to one withdraw.
Safety
In this study, 5 participants experienced adverse events (AEs), including one participant whose previous leg wound became inflamed during treatment. After medication, the participant recovered and completed treatment. However, during the two-month without treatment, the patient was hospitalized for another leg surgery and could not complete the follow-up. Another reported slight physical discomfort after a treatment at the three-month mark. Symptoms subsided after one week, and the participant continued treatment and completed the evaluation. In addition, three participants were infected with the Corona Virus Disease 2019 (COVID-19), during the no-treatment period after four-month treatment and evaluation. After receiving treatment, their symptoms improved, and they completed the six-month evaluation. These AEs were either associated to the participants’ previous surgical history, or the participants’ older age or other diseases. Most of the adverse events (60%) were due to the impact of the COVID-19. Routine vital sign assessments indicated no additional discomfort reported by the participants or their caregivers. Overall, no serious adverse events (SAEs) occurred in the participants. In addition, no device-related AEs, SAEs, or device defects were reported.
Discussion
A substantial body of evidence from cellular and animal studies supports the potential of NIR treatment for AD. However, clinical studies of NIR for AD are limited, and multiple of those studies have focused on localized regions. This limitation maybe due to photon scattering, which hampers the delivery of light to deeper brain tissues. 16 Whole-head coverage may be more suitable for AD, a disease that affects multiple brain regions. However, the effect and persistency of whole-head NIR treatment on AD patients remain unclear.
First of all, this open-label pilot study provides evidence of the benefits of whole-head NIR in AD patients. Our results indicate that whole-head NIR treatment significantly improves cognitive function in AD, which aligns with prior studies using NIR in AD patients.18,26 The expected annual decline in MMSE score described previously was 2–4 points in untreated patients with AD27–29 and 2.2 points in placebo-treatment patients, 30 In the present study, the mean increase in MMSE score from baseline was 3.2 points (Figure 3(a)), after 4-month treatment. Moreover, while untreated AD patients experience an 8-point increase in the ADAS-cog score over one year,31,32 our study observed a decrease of 5.0 points (Figure 3(b)). These changes in both ADAS-cog and MMSE scores suggest that the treatment is beneficial for AD. Comparatively, pharmacological studies such as Jia et al. have reported that 151 patients with mild to moderate AD who received a 4-month treatment of rivastigmine, the MMSE score increased by 0.3 points and ADAS-cog score reduced by 2-point compare to baseline. 33 Collectively, these findings highlight the potential of whole-head NIR in treatment of AD.
Referring to previous studies, the efficacy of whole-head NIR treatment for AD may be partly attributed to its potential to enhance neuroplasticity and functional connectivity (FC). This view is supported by PBM studies, which suggest that PBM can improve cognitive function by enhancing FC of DMN. 12 Additionally, PBM has been shown to alter the FC of large-scale brain networks, particularly in the frontal and parietal cortical regions that are integral to memory, thereby contributing to improved cognitive function.34–36 This perspective is further supported by studies on other neuromodulation methods. For instance, Meinzer found that 20 min of transcranial direct current stimulation (tDCS) can reverse age-related cognitive decline in healthy elderly and establish a cortical connectivity pattern more similar to that of the young. 37 Therefore, it is reasonable to speculate that whole-head NIR treatment may affect the FC of cognition-related regions, thereby potentially promoting cognitive function improvement in AD patients. However, it remains unclear how whole-head NIR influences neuroplasticity and FC to benefit AD patients.
Secondly, two months post-treatment, the improvements from whole-head NIR in AD patients persisted. This persistency may be attributed to the lasting effects of PBM, consistent with previous studies.11,38 Although, MMSE score declined by 1.3 points and ADAS-cog score increased by 2 points at 6M (Figure 5). Overall improvements relative to baseline were maintained, with MMSE score improved by 1.9 points and ADAS-cog score decreased by 3.0 points. Notably, the sustained effects in this study surpass those reported in previous studies on localized PBM, where MMSE score decreased by 1.6 points and ADAS-cog score increased by 2 points 1-month post-treatment. Studies using helmet-based PBM have yet evaluated the long-term effects after the treatment ends.26,39 Our findings suggest that the effects of whole-head NIR may be more enduring, possibly because the whole-head NIR covers a broader brain region, positively impacting more brain networks, and potentially inducing adaptive FC reorganization, 40 which helps maintain these improvements. However, as the follow-up in this study was only two months, future research will extend the follow-up period to explore the longer-term effects.
Overall, whole-head NIR therapy shows potential in the treatment of AD. Although its efficacy and durability are influenced by various factors, such as frequency, power and disease stage, the potential of whole-head NIR in AD treatment should not be underestimated. While the results of this study are promising, there are several limitations. First, the COVID-19 pandemic significantly increased recruitment difficulties, and the long phase of study resulted in a small sample size. Future studies will increase the sample size to further validate these findings. Additionally, this study's single-arm design without a placebo-controlled group limits the objective evaluation of the intervention effect. To address this limitation, we are currently conducting a randomized double-blind controlled trial to minimize the placebo effects and enhance the rigor of the efficacy. This trial includes various imaging biomarkers, such as positron emission tomography, MRI, electroencephalography, and functional near-infrared spectroscopy, to more accurately evaluate efficacy and explore mechanisms. The combination of multimodal approaches is expected to establish more robust scientific evidence for whole-head NIR therapy in AD treatment.
This study revealed the potential benefits of whole-head 810 nm NIR treatment in AD patients, improving cognitive function and neuropsychiatric symptoms, with improvement persisting for at least two months. These results encouraged us to conduct a large-sample double-blind clinical trial to validate the efficacy and safety of whole-head NIR treatment in AD patients.
Footnotes
Acknowledgments
We thank the Director Li Dongmei of the senior cognitive care center for her supports. We express appreciation to HuiChuang Company for providing all devices.
Author contributions
Rong Guo (Conceptualization; Investigation; Methodology; Visualization; Writing – original draft; Writing – review & editing); Deyu Li (Conceptualization; Data curation; Visualization; Writing – review & editing); Fang Li (Investigation; Methodology); Linna Ji (Investigation; Methodology); Hongying Liu (Investigation; Methodology); Huiting Qiao (Writing – review & editing); Zeping Lv (Conceptualization; Supervision); Yi Tang (Methodology; Supervision; Writing – review & editing); Daifa Wang (Conceptualization; Supervision).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by grants from the National Key Research & Development Program of China (Grant No. 2022YFC3601200). horizontal project from Danyang Huichuang Medical Equipment Co., Ltd (Funding Number: KH54480701, KH54392701). The funder had no role in the design, data collection, data analysis, and reporting of this study.
Declaration of conflicting interests
The authors declare that they have no conflict of interest. Prof. Wang (the corresponding author) holds shares in Jiangsu Danyang Huichuang Medical Equipment Co., Ltd, but there are no conflicts of interest in connection with this article.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.