
Abstract
Background
The prevalence of Alzheimer's disease (AD) is increasing, and with it comes the demand for specialized services. Current information on the institutionalization of patients with AD is limited.
Objective
To determine the level of institutionalization among AD patients in the facilities of the Czech Republic and the Slovak Republic.
Methods
A survey of the rate of institutionalization in facilities in the Czech Republic and Slovak Republic. The survey collects data on the institutionalization of patients suffering from AD in relation to the capacity of the facilities and the prevalence of the disease. Data were collected by representative quantitative survey, during years 2019–2021.
Results
Patients with AD occupy approximately 25% of the total capacities of institutions in the Czech and Slovak Republics. The rate of institutionalization of patients with AD is estimated at 20.5% in the Czech Republic and 24% in the Slovak Republic. This is more than the estimated worldwide rate of institutionalization of people with AD (16%) but less than the estimated rate of institutionalization of these patients in high-income countries (31%).
Conclusions
As the prevalence of AD increases, so do the demands for care. If there is no increase in institutional capacity, this growth will put more pressure on home care. In order to provide specialized care to as many patients as possible, emphasis must be placed on increasing the capacity of institutions.
Introduction
Alzheimer's disease (AD) is a progressive, neurodegenerative, brain disease that worsens over time. Its origin is unknown, with genetic factors explaining early onset. 1 The first symptoms are almost imperceptible but worsens to include memory loss, cognitive deterioration, reading and writing problems, loss of orientation, personality changes, and self-care challenges. In the final (so-called severe) phase, advanced symptoms of dementia appear, and require continuous care. 2
AD affected some 55 million people globally in 2019, with an estimated cost of US$1.3 trillion annually. By 2050, experts estimate that this disease will affect 139 million individuals worldwide. 3 As of 2018, the Czech Republic has over 149,000 individuals living with AD, accounting for 1.14 percent of the country's total population. By 2025, that number is predicted to rise to over 181,000. In Slovakia, the number of individuals with AD was over 62,000 in 2018, accounting for over 1.15 percent of the country's total population. By 2025, that number is predicted to rise to over 74,000. 4
AD symptoms, affecting the patient's daily activities, often require the assistance of another person. The difficulty of caring for people with AD gradually increases with the progression of the disease's symptoms, often leading to the inability of informal caregivers to provide required care hence the need to institutionalize the patient. The term ‘institutionalization’ in this article covers specialized inpatient care provided by professionals. It includes both medical and non-medical care settings. The time of institutionalization of a person with AD is unique to each individual but some factors may predict the need for early institutionalization. Lower cognitive and functional abilities at the onset of the disease, a faster decline in these abilities, or an increase in the frequency or severity of neuropsychiatric symptoms predict earlier institutionalization of AD patients. 5 Another reason for early institutionalization of patients is patient agitation. Patient agitation, which occurs in approximately 76% of AD patients, makes it difficult for informal caregivers to care for patients and leads them to seek specialized care. According to Jones et al. the rate of institutionalization of agitated patients is more than three times higher than that of non-agitated patients. 6
There are currently no studies or statistics available that provide information on the overall rate of institutionalization of patients with AD in the Czech and Slovak Republics. This paper aims to provide unique data on estimates of the overall rate of institutionalization of patients with AD in the Czech and Slovak Republics. The paper will enhance understanding of the institutionalization rate of AD patients in relation to the overall capabilities of the facilities and the prevalence of AD in the countries studied. This can serve as a basis for the creation of policies and action plans for the given countries in relation to AD patient care provision.
Methods
Data source
It was a study of data from the Czech and Slovak Republics on the prevalence of AD patients institutionalized in these nations’ inpatient institutions. The findings of real-world surveys conducted in inpatient facilities served as the main source of information on hospitals, sanatoriums for long-term diseased, retirement homes, and retirement homes with a special regime.7–9 The public database ÚZIS was the additional source of hospital data. 10
Institution specification
Institutions providing inpatient care to persons with AD in the Czech and Slovak Republics are governed by the Act on Municipalities, the Act on Social Services, and the Act on Health Services.11,12 Official health and social care facilities in these countries that provide inpatient care for people with AD were included consisting of. Hospitals (general and psychiatric hospitals), sanatoriums for long-term diseased, and retirement homes with a special régime were included. Retirement homes, according to the Social Services Act, are officially not allowed to accept persons suffering from AD, but in reality, AD patients are often found, and therefore they are also included.
Data collection and analysis
To determine the prevalence of the institutionalized population with AD, data were obtained from studies that used a uniform data collection methodology.7–9 Data on the prevalence of AD patients in the given institutions were collected in the form of a questionnaires which were distributed by e-mail and telephone communication. Table 1 lists the sources and years of data collection.
Summary of main data sources.
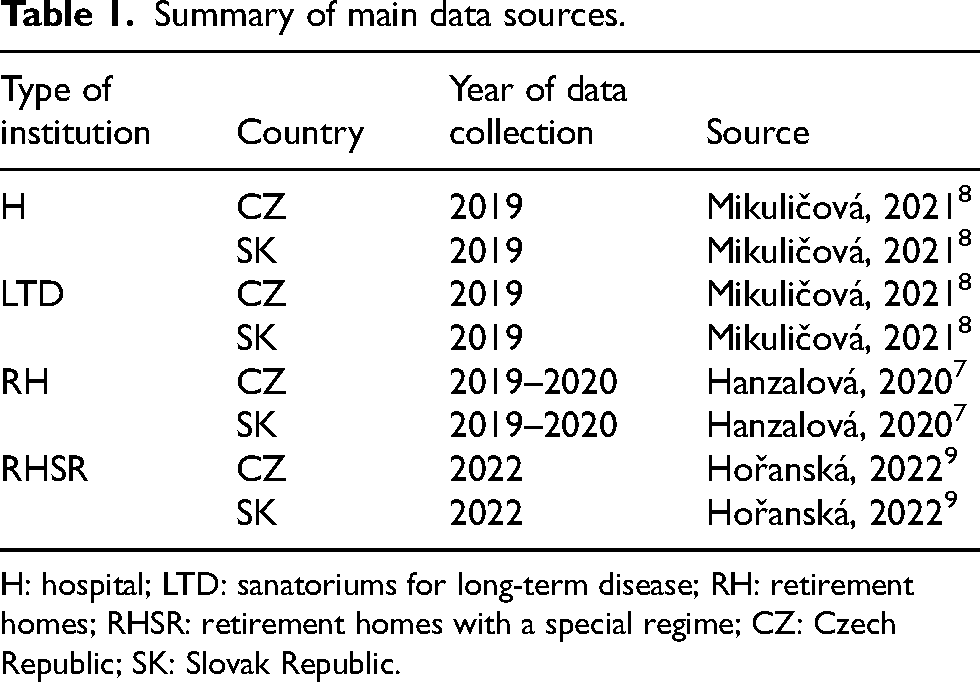
H: hospital; LTD: sanatoriums for long-term disease; RH: retirement homes; RHSR: retirement homes with a special regime; CZ: Czech Republic; SK: Slovak Republic.
Data collection was performed by trained individuals under the supervision of the authors of this article. The facility director or the head of the direct care department, which had an overview of the patients’ diagnoses, received the questionnaire survey. Respondents were asked a short set of questions, including a question about the region in which the facility is located, the type of facility, the type of facility from the point of view of ownership, the total capacity of the facility, and the proportion of patients with AD. The collected data were evaluated in Excel software.
Table 2 summarizes the extent of individual facilities’ involvement in research. The minimum involvement of institutions was set at 10% to ensure the results’ applicability to the entire analyzed area. 13 All listed facilities in both countries met this condition. The participants were selected randomly within the regions. In each region of both countries, it was necessary to meet the minimum involvement of institutions set at 10%.
The extent of individual facilities’ involvement in research.
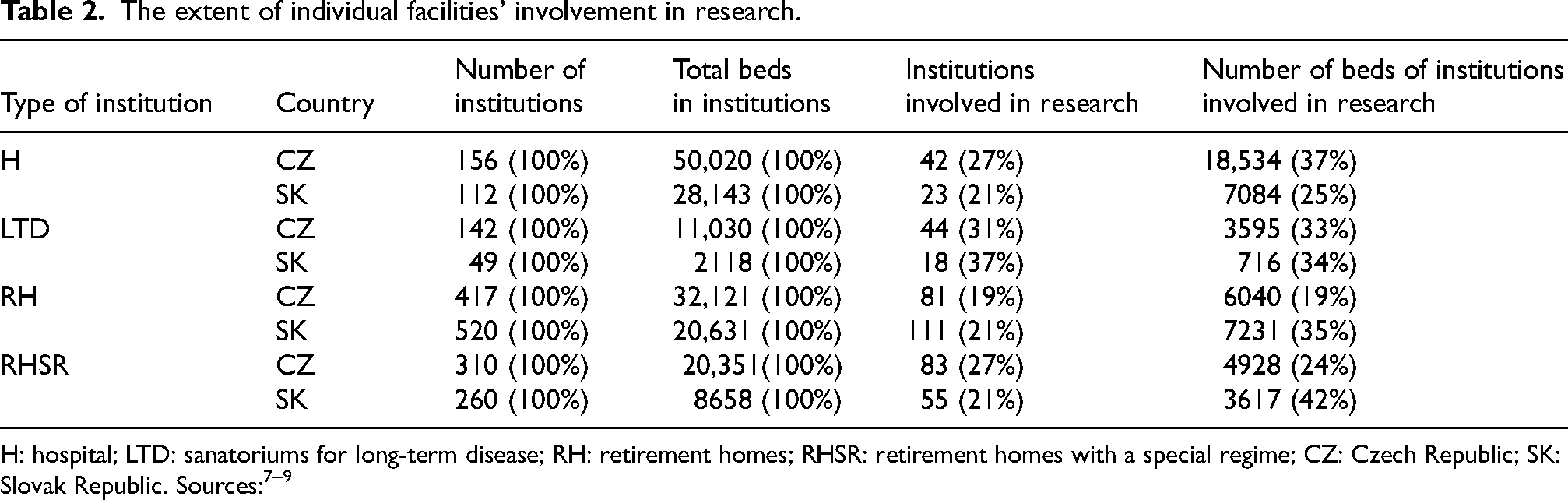
The source of CZ hospitals data only brings data for general hospitals. This paper supplements the data with the number of patients in psychiatric hospitals. Data on the number of patients in psychiatric hospitals were found in the freely available public database of the Czech Republic, and in the results of this paper, the capacity of hospitalizations for general hospitals in the Czech Republic is supplemented by another 8618 hospitalizations for psychiatric hospitals, of which 1680 patients with AD. 10
The data obtained were grouped to determine the overall level of institutionalization in inpatient care facilities in the Czech and Slovak Republics. The data were expressed in relation to facility capacities and in relation to the prevalence of AD.
Results
The institutionalization of persons with AD in inpatient care facilities in the Czech and Slovak Republics varied depending on the type of facility. Persons with AD were found in short-term and long-term care facilities, including hospitals, sanatoriums for long-term diseased, retirement homes, and retirement homes with a special regime. Hospitals primarily cater to short-term patients, frequently treating other medical conditions in which AD is only a comorbidity. Sanatoriums for long-term diseased provide care most often in the order of weeks to months. According to the National Palliative Care Database, in 2014, 14 the average length of residence in sanatoriums for long-term diseased was 45 days, the median was 30 days. Long-term inpatient care is the intended use of retirement homes and retirement homes with special regimes.
Primarily, retirement homes with a special regime are intended for the long-term residence of persons with AD, which are able to provide services for specific AD patients needs.11,12 Retirement homes with a special regime not only cater to AD patients, but also welcome patients with other diagnoses. However, the capacities of homes with a special regime are significantly insufficient, and even if only persons diagnosed with AD were admitted to this type of facility, their capacity would not cover even a quarter of people with an official diagnosis of AD (see Table 3).
Capacity of retirement homes with a special regime compared to prevalence of Alzheimer's disease.
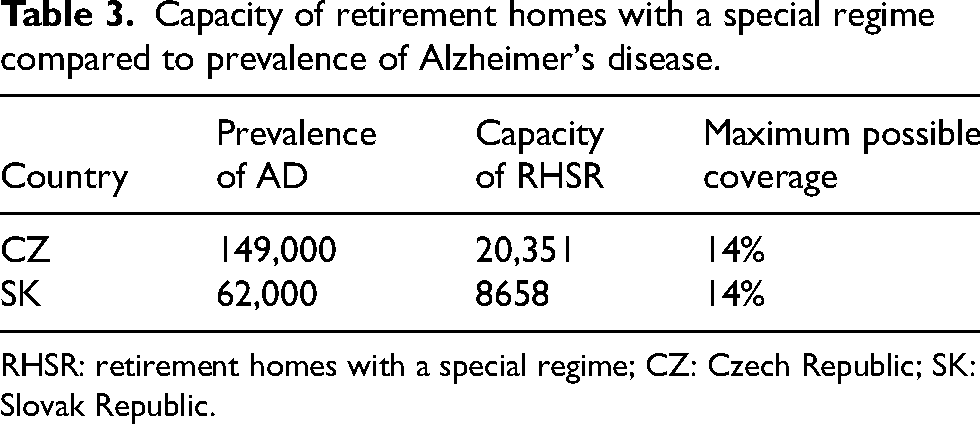
RHSR: retirement homes with a special regime; CZ: Czech Republic; SK: Slovak Republic.
Table 4 summarizes the rate of institutionalization of patients with AD in facilities in the Czech Republic. Retirement homes with a special regime have the highest number and share of AD patients (compared to these facilities’ total capacity). The second highest number of AD patients was identified in hospitals, but the proportion of AD patients to the total capacity of the facilities was the smallest there. Together, all institutions had a total capacity of 122,140 beds, with 29,960 beds occupied by AD patients. This represents almost 25% of the total capacity of all institutions.
Estimation of the prevalence of people with AD to the total capacities of the Czech facilities.
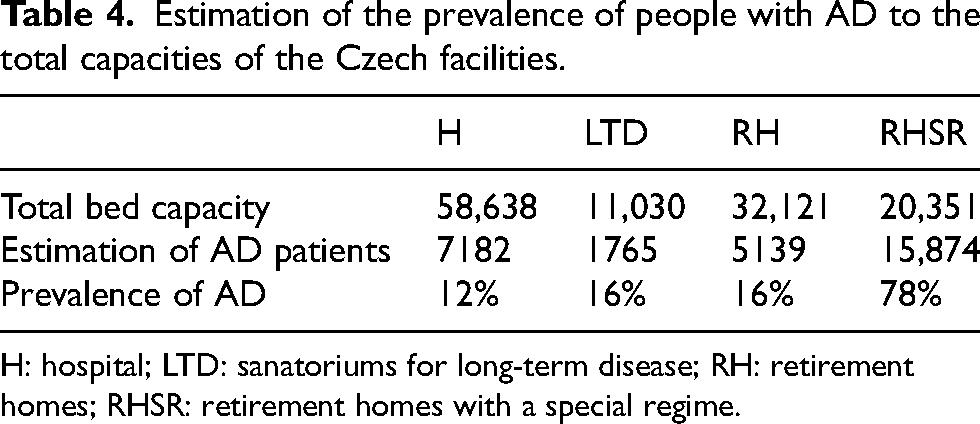
H: hospital; LTD: sanatoriums for long-term disease; RH: retirement homes; RHSR: retirement homes with a special regime.
Similarly, retirement homes with a special regime dominate the prevalence of institutionalized AD patients in the Slovak Republic's facilities, both in terms of the number of patients and in relation to the facility's total capacity. The particular prevalence rate of institutionalized persons with AD can be seen in Table 5. Also similar to the Czech Republic, Slovakia hosts AD patients in retirement homes, despite the current legislation prohibiting their stay in such facilities. The number of people with AD in retirement homes was estimated at approximately 4538 people. This represents 22% (6% higher than in the Czech Republic) of the total capacity of this type of facility. Overall, in all types of institutions, AD sufferers accounted for 14,857 cases out of a total of 59,550 beds, which represents almost 25% of the total capacities.
Estimation of the prevalence of people with AD to the total capacities of the Slovak facilities.
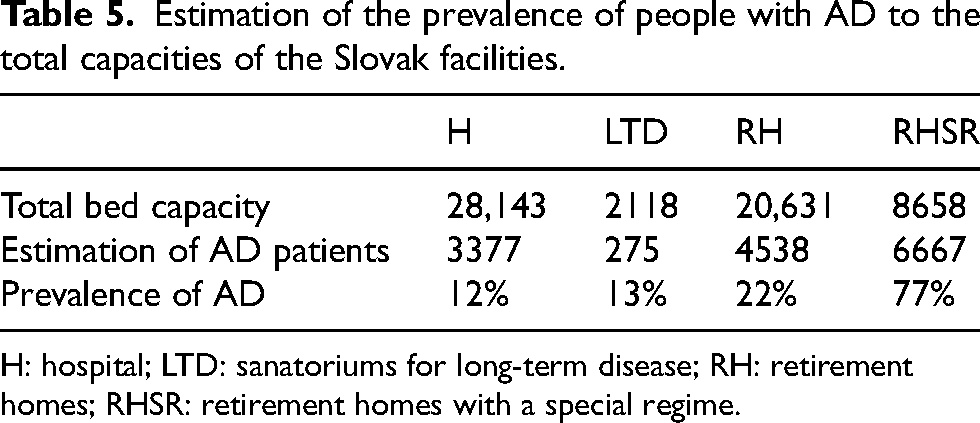
H: hospital; LTD: sanatoriums for long-term disease; RH: retirement homes; RHSR: retirement homes with a special regime.
Table 6 shows the rate of institutionalization of AD patients compared to the total official prevalence of AD in the given countries. Approximately 20% of the AD population was institutionalized in the Czech Republic while approximately 24% of the AD population was institutionalized in the Slovak Republic in health and social inpatient care facilities. This indicates that a significant portion of the population, specifically 79.9% in the Czech Republic and 76% in the Slovak Republic, live predominantly in their homes under the care of a formal or informal caregiver and do not use institutions allowing inpatient care. People with AD who are not institutionalized in inpatient care facilities can use specialized outpatient services, such as day care centers, and specialized health outpatient services.
Estimation of the institutionalization of persons with AD to the prevalence of the disease.
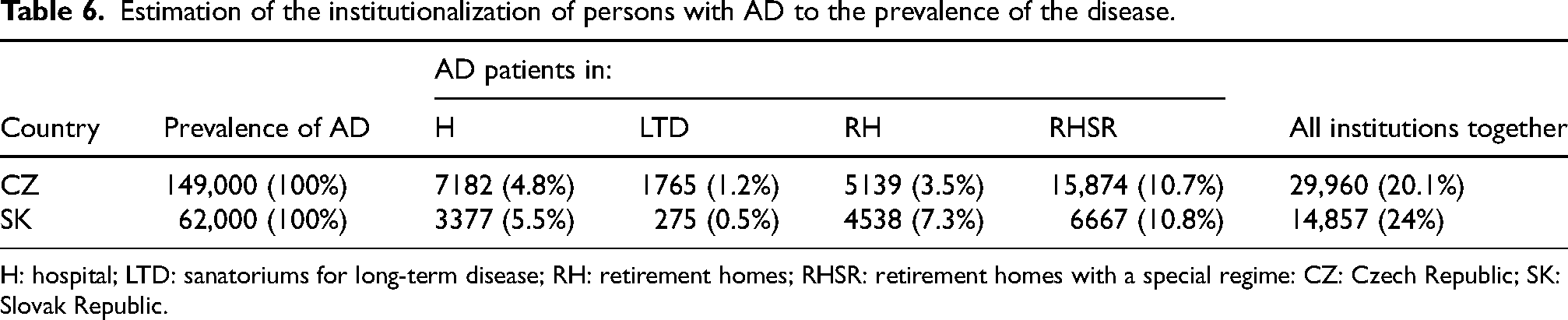
H: hospital; LTD: sanatoriums for long-term disease; RH: retirement homes; RHSR: retirement homes with a special regime: CZ: Czech Republic; SK: Slovak Republic.
When focusing only on retirement homes with a special regime, which are primarily intended for long-term inpatient stays for patients with AD, the rate of institutionalization of patients with AD would be approximately 10.7% in the Czech Republic and 10.8% in the Slovak Republic.
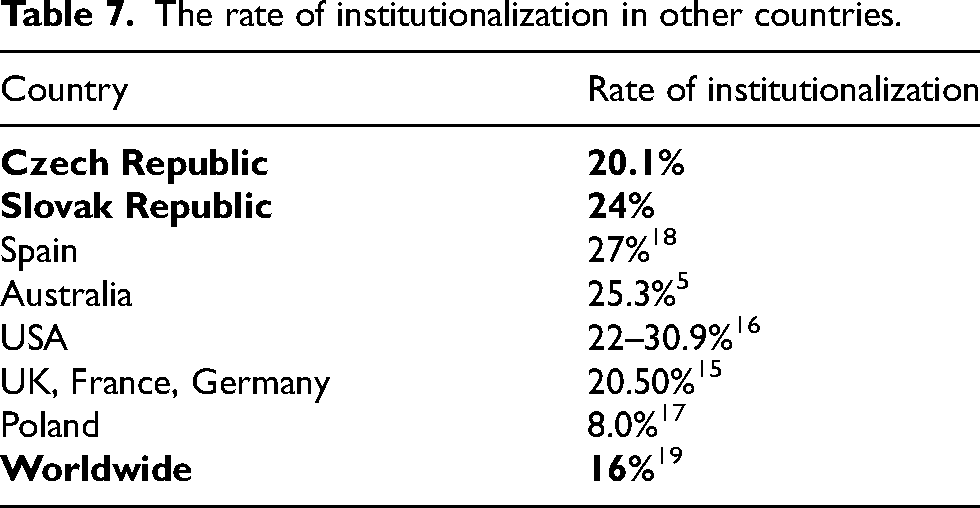
Table 7 presents a comparison of the results with institutionalization rates in other countries. Belger et al. (2017) reported in their study that during the 36-month duration of the study on patients from the UK, France, and Germany, 20.5% of respondents were institutionalized. 15 Brodaty et al. (2014) report the rate of institutionalization of AD patients in Australia at 25.3%. 5 Khandker et al. (2023) reported, based on a 4-year study in the US, that the rate of institutionalization of AD patients was 30.9% in patients with behavioral symptoms and 22% in patients without these symptoms. 16 Rusowicz et al. (2021) report that approximately 92% of people with dementia in Poland live at home. As a result, the rate of institutionalization of people with dementia in Poland is only around 8%. 17 Mar et al. (2019) It puts the institutionalization rate of people with dementia at 27%, based on a study done in Spain. 18 Alzheimer's Disease International (2018) reports that the global rate of home care for people with dementia is approximately 84%, with only 16% institutionalized. There is a difference in the degree of institutionalization in relation to the amount of income, where in low-income countries, the degree of institutionalization is 4%, while in high-income countries, the degree of institutionalization is estimated at 31%. 19
The rate of institutionalization in other countries.
Discussion
AD is a chronic, neurodegenerative disease whose prevalence is constantly increasing. This article presented the first estimates of the rate of institutionalization of patients with AD in inpatient facilities in the Czech and Slovak Republics. Patients with AD occupy approximately 25% of the total capacity of facilities in the Czech Republic. The institutionalization rate of AD patients in the Czech Republic is estimated at 20.5%. In the Slovak Republic, AD patients occupy approximately 25% of the total bed capacity. The Slovak Republic institutionalizes an estimated 24% of AD patients. As a result, for both countries examined, the total rate of home care is more than three quarters (79.9% in the Czech Republic, 76% in the Slovak Republic).
A direct comparison of the results of this paper with the results of other studies is not possible, as it is a unique data set that has not been, thus far, published. This paper is the first to provide information on the level of institutionalization in inpatient facilities in the Czech and Slovak Republics. As a result, it is only possible to compare the paper's results for the Czech and Slovak Republics with the rate of institutionalization in other countries (Table 7). The level of institutionalization in the Czech Republic and the Slovak Republic is above the global average, but below the average for high-income countries. 19 In comparison with data from European countries, the degree of institutionalization is similar in the Czech Republic and higher in the Slovak Republic than reported for the UK, France, and Germany. 15 The level of institutionalization in Poland is lower than in the Czech and Slovak Republics. 17
The research limitations of this study include the different times of data collection for individual institution types, which range from 2019 to 2022. The results of the individual studies that provided the input data for this paper may have been influenced by the facilities’ unwillingness to respond to the questionnaire and their reluctance to share real data (particularly in the case of retirement homes where the law prohibits AD patients from being present). However, based on the results of this input research and the detailed examination of the input data, we think that this aspect will have a minimal impact on the outcomes of our paper.
As to co-morbidities, Physicians frequently neglect to document secondary diagnoses that did not initiate the patient's stay, potentially influencing the results in hospital institutions.
A factor that could have influenced the results is the high rate of underdiagnosis of AD in the Czech and Slovak Republic and the fact that many specialists still confuse the terms “dementia” and “Alzheimer's disease”, which makes it challenging to the clear identification of the prevalence of the institutionalized population with AD.7–9
It is also necessary to keep in mind that institutions differ in the length of stay for patients. While in a hospital it can be a stay of a few days or weeks, sanatoriums for long-term diseased provide care for several months on average. Retirement homes and retirement homes with a special regime are intended for the long-term stay of the diseased. Due to the lack of public data, the severity of the illness of institutionalized patients was not identified in the study.
Conclusion
In the Czech and Slovak Republics, less than a quarter of people suffering from AD are institutionalized. The rate of institutionalization of persons with AD is estimated at 20.5% in the Czech Republic and 24% in the Slovak Republic. Due to the increasing prevalence of AD, there is a need to emphasize increasing the capacity of specialized care facilities, especially long-term inpatient care. The current capacities of retirement homes with a special regime would not be able to accept even a quarter of patients with AD. Unless there is a significant increase in facility capacities, this trend will continue to deepen, and specialized care will be available to an even smaller proportion of patients than currently. This survey collects data on the institutionalization of people with AD, which provides a basis of information for better management of care for people with AD. The identification of the level of institutionalization of this population group will allow to evaluate the capacities and employment of the facilities in recent years and a determination of trends on which future need might be bases.
Footnotes
Acknowledgments
The authors have no acknowledgments to report.
Author contributions
Kristina Randlová (Conceptualization; Formal analysis; Methodology; Writing – original draft); Peter Pažitný (Conceptualization; Methodology; Writing – original draft); Daniela Kandilaki (Conceptualization; Methodology; Writing – original draft).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The data supporting the findings of this study are available within the articles listed in the sources of this paper.